
Permissible Outcomes of Lobe-Specific Lymph Node Dissection for Elevated Carcinoembryonic Antigen in Non-Small Cell Lung Cancer

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
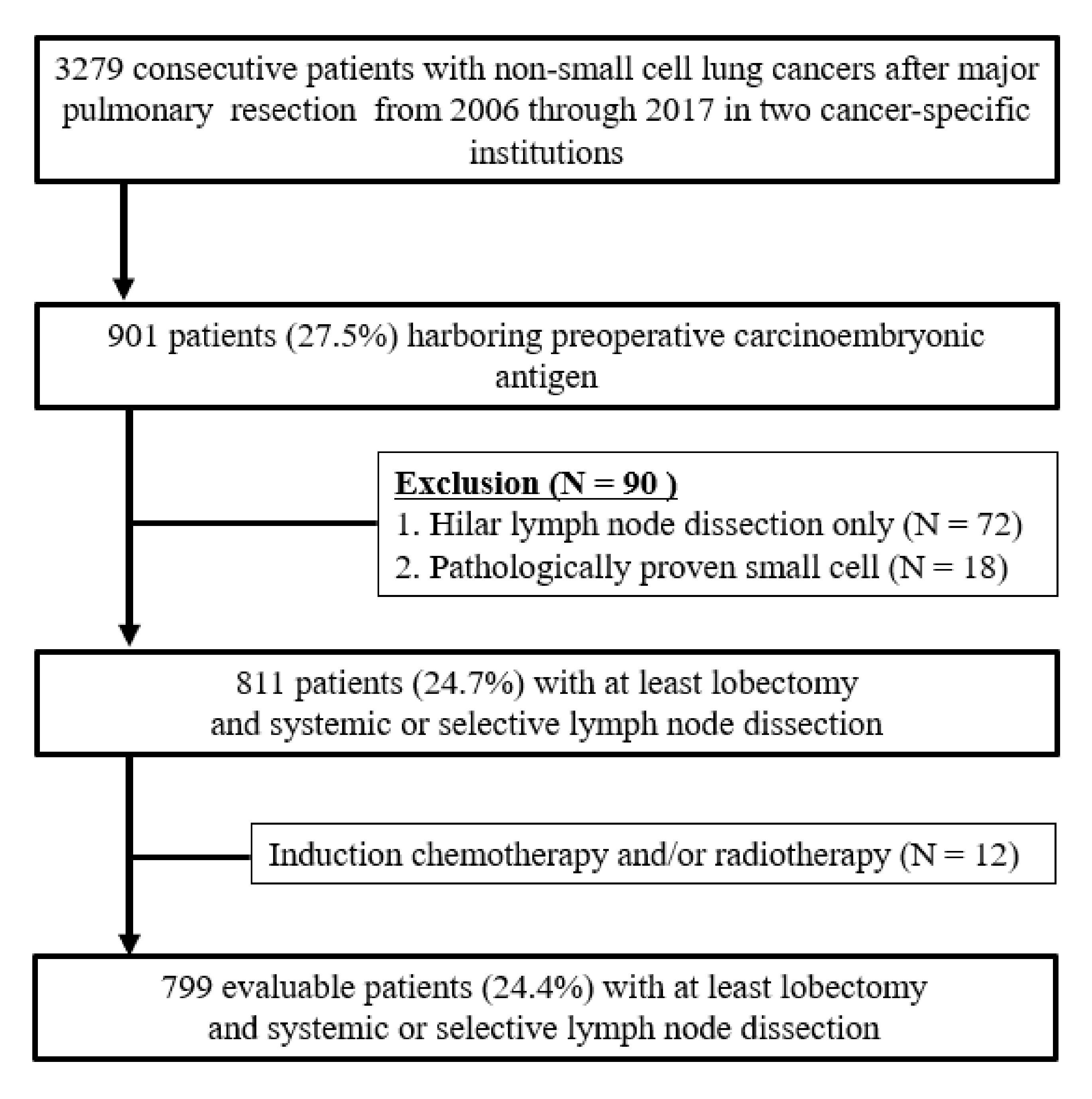
2.1. Study Population
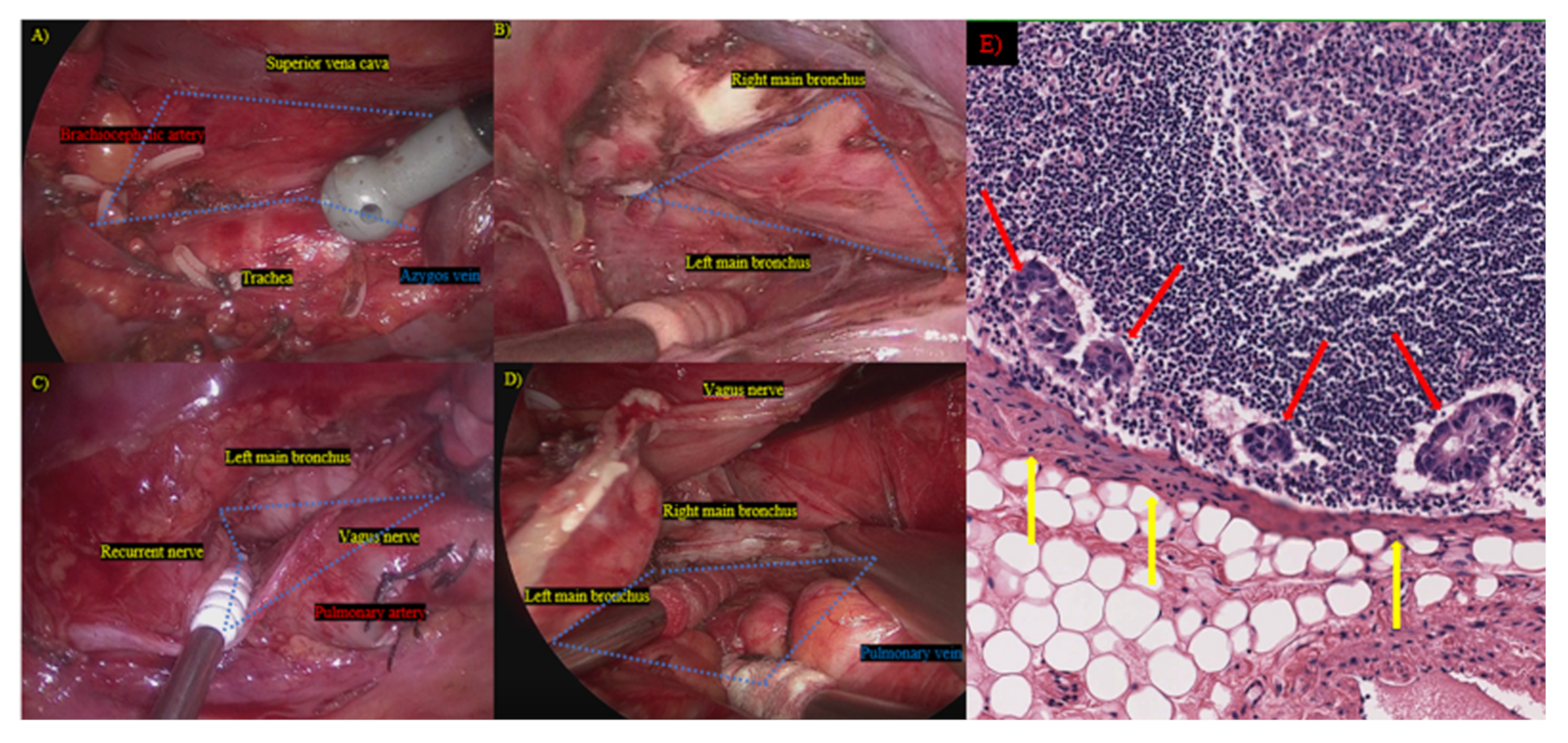
2.2. Surgical Procedure and Outcome Measures
2.3. Statistical Analyses
3. Results
3.1. Unadjusted Baseline Characteristics
3.2. Surgical Procedure, Approach, and Hazard Ratios for Overall Survival in Patients with CEA Abnormality
3.3. Clinicopathological Factors Associated with Systemic Lymph Node Dissection
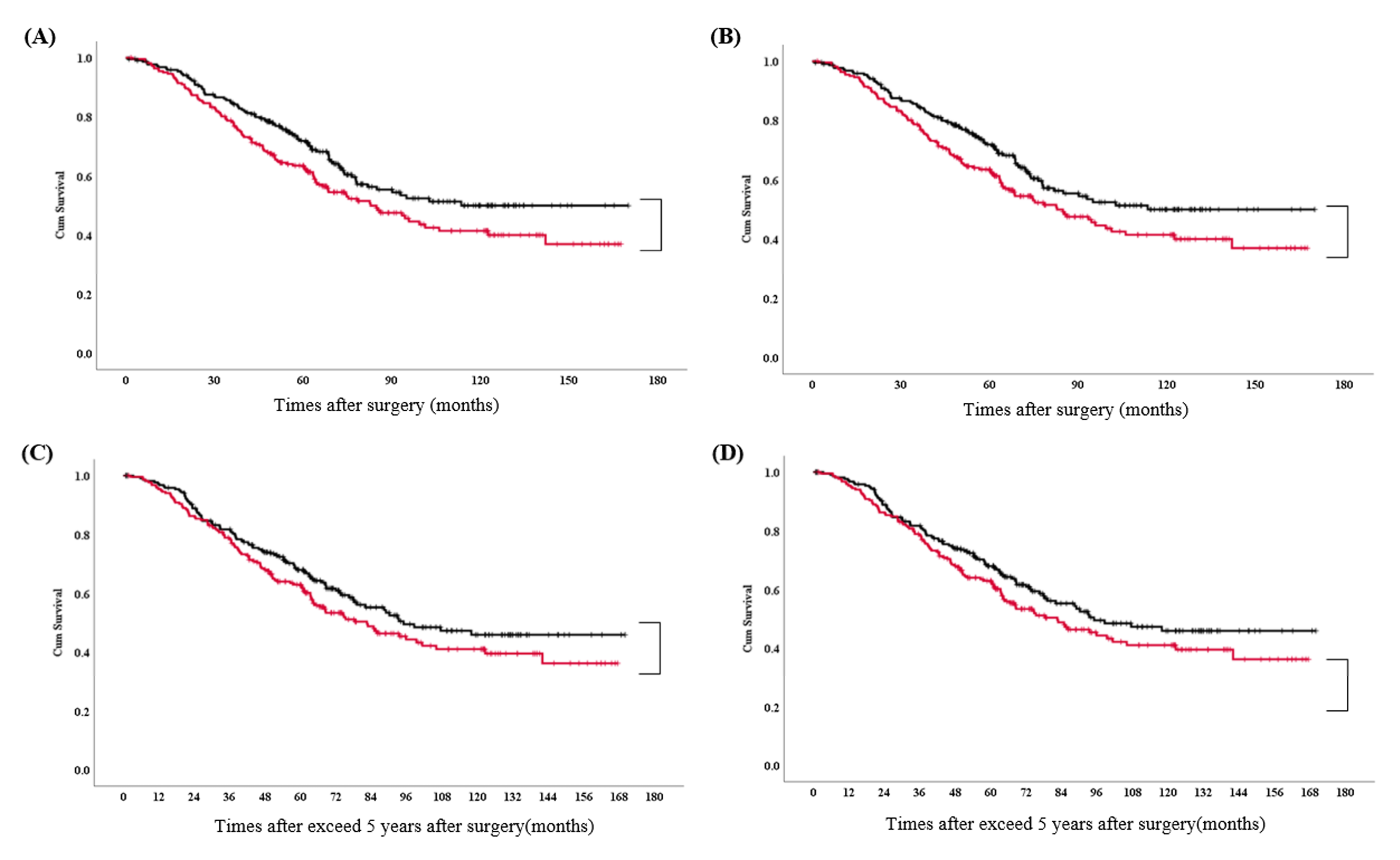
3.4. Surgical Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mountain, C.F.; Dresler, C.M. Regional lymph node classification for lung cancer staging. Chest 1997, 111, 1718–1723. [Google Scholar] [CrossRef] [PubMed]
- Fibla, J.J.; Cassivi, S.D.; Decker, P.A.; Allen, M.S.; Darling, G.E.; Landreneau, R.J.; McKenna, R.J.; Putnam, J.B.; ACOSOG Z0030 Study Group. Validation of the lung cancer staging system revisions using a large prospective clinical trial database (ACOSOG Z0030). Eur. J. Cardio-Thorac. Surg. 2013, 43, 911–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Mao, Y.; He, J.; Gao, S.; Zhang, Z.; Ding, N.; Xue, Q.; Gao, Y.; Wang, D.; Zhao, J.; et al. Lobe-specific Lymph Node Dissection in Clinical Stage IA Solid-dominant non-small-cell Lung Cancer: A Propensity Score Matching Study. Clin. Lung Cancer 2021, 122, e201–e210. [Google Scholar] [CrossRef] [PubMed]
- Aokage, K.; Yoshida, J.; Ishii, G.; Hishida, T.; Nishimura, M.; Nagai, K. Subcarinal lymph node in upper lobe non-small cell lung cancer patients: Is selective lymph node dissection valid? Lung Cancer 2010, 70, 163–167. [Google Scholar] [CrossRef]
- Meng, S.; Liu, G.; Wang, S.; Yang, F.; Wang, J. Nodal Involvement Pattern in Clinical Stage IA Non-Small Cell Lung Cancer According to Tumor Location. Cancer Manag. Res. 2020, 12, 7875–7880. [Google Scholar] [CrossRef]
- De Leyn, P.; Lardinois, D.; Van Schil, P.; Rami-Porta, R.; Passlick, B.; Zielinski, M.; Waller, D.; Lerut, T.; Weder, W. ESTS European trends in preoperative and intraoperative nodal staging: ESTS guidelines. J. Thorac. Oncol. 2007, 2, 357–361. [Google Scholar] [CrossRef]
- Ettinger, D.S.; Wood, D.E.; Aggarwal, C.; Aisner, D.L.; Akerley, W.; Bauman, J.R.; Bharat, A.; Bruno, D.S.; Chang, J.Y.; Chirieac, L.R.; et al. NCCN Guidelines Insights: Non-Small Cell Lung Cancer, Version 1.2020. Natl. Compr. Cancer Netw. 2019, 17, 1464–1472. [Google Scholar] [CrossRef] [Green Version]
- Broderick, S.R. Adjuvant and Neoadjuvant Immunotherapy in Non-small Cell Lung Cancer. Thorac. Surg. Clin. 2020, 30, 215–220. [Google Scholar] [CrossRef]
- Lee, P.C.; Nasar, A.; Port, J.L.; Paul, S.; Stiles, B.; Chiu, Y.L.; Andrews, W.G.; Altorki, N.K. Long-term survival after lobectomy for non-small cell lung cancer by videoassisted thoracic surgery versus thoracotomy. Ann. Thorac. Surg. 2013, 96, 951–960, discussion 960–961. [Google Scholar] [CrossRef]
- Fang, L.; Xu, J.; Ye, B.; Yu, G.; Chen, G.; Yang, J. Is lobe specific lymph node dissection adequate for cN0-1 non-small cell lung cancer? J. Cardiothorac. Surg. 2020, 15, 46. [Google Scholar] [CrossRef]
- Kuroda, H.; Mori, S.; Tanaka, H.; Yoshida, T.; Mizuno, T.; Sakakura, N.; Yatabe, Y.; Iwata, H.; Sakao, Y. Prognostic significance of combined radiologic imaging modalities for prognosis of clinical IA adenocarcinomas. Oncotarget 2018, 9, 10745–10753. [Google Scholar] [CrossRef] [Green Version]
- Kuroda, H.; Nakada, T.; Oya, Y.; Takahashi, Y.; Matsusita, H.; Sakakura, N. Clinical adjustability of radiological tools in patients with surgically resected cT1N0-staged non-small-cell lung cancer from the long-term survival evaluation. J. Thorac. Dis. 2020, 12, 6655–6662. [Google Scholar] [CrossRef]
- Sakao, Y.; Kuroda, H.; Mun, M.; Uehara, H.; Motoi, N.; Ishikawa, Y.; Nakagawa, K.; Okumura, S. Prognostic significance of tumor size of small lung adenocarcinomas evaluated with mediastinal window settings on comuputed tomography. PLoS ONE 2014, 9, e110305. [Google Scholar] [CrossRef]
- Moro, D.; Villemain, D.; Vuillez, J.P.; Delord, C.A.; Brambilla, C. CEA, CYFRA21–1 and SCC in non-small cell lung cancer. Lung Cancer 1995, 13, 169–176. [Google Scholar] [CrossRef]
- Nasralla, A.; Lee, J.; Dang, J.; Turner, S. Elevated preoperative CEA is associated with subclinical nodal involvement and worse survival in stage I non-small cell lung cancer: A systematic review and meta-analysis. J. Cardiothorac. Surg. 2020, 15, 318. [Google Scholar] [CrossRef]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V.; et al. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef] [Green Version]
- Kuroda, H.; Nakada, T.; Oya, Y.; Takahashi, Y.; Shirai, S.; Matsui, T.; Nakanishi, K.; Matsushita, H.; Sakakura, N. Computed tomography and positron emission tomography-staged cN0 non-small cell lung cancer. Video-Assist Thorac. Surg. 2020, 5, 14. [Google Scholar] [CrossRef]
- Thomas, P.A. Intraoperative lymph-node assessment during NSCLC surgery: The need for standardisation and quality evaluation. Lancet Oncol. 2019, 20, 23–25. [Google Scholar] [CrossRef]
- Shapiro, M.; Mhango, G.; Kates, M.; Weiser, T.S.; Chin, C.; Swanson, S.J.; Wisnivesky, J.P. Extent of lymph node resection does not increase perioperative morbidity and mortality after surgery for stage I lung cancer in the elderly. Eur. J. Surg. Oncol. 2012, 38, 516–522. [Google Scholar] [CrossRef] [Green Version]
- Naruke, T.; Suemasu, K.; Ishikawa, S. Lymph node mapping and curability at various levels of metastasis in resected lung cancer. J. Thorac. Cardiovasc. Surg. 1978, 76, 832–839. [Google Scholar] [CrossRef]
- Kuroda, H.; Sakao, Y.; Mun, M.; Uehara, H.; Nakao, M.; Matsuura, Y.; Mizuno, T.; Sakakura, N.; Motoi, N.; Ishikawa, Y.; et al. Lymph Node Metastases and Prognosis in Left Upper Division Non-Small Cell Lung Cancers: The Impact of Interlobar Lymph Node Metastasis. PLoS ONE 2015, 10, e0134674. [Google Scholar] [CrossRef]
- Karush, J.M. Are Lobe-Specific Mediastinal Lymph Node Dissections Reasonable for Peripheral Stage Ia Non-small Cell Lung Cancer? Ann. Surg. Oncol. 2020, 27, 331–332. [Google Scholar] [CrossRef]
- Ichinose, J.; Murakawa, T.; Hino, H.; Konoeda, C.; Inoue, Y.; Kitano, K.; Nagayama, K.; Nitadori, J.; Anraku, M.; Nakajima, J. Prognostic impact of the current Japanese nodal classification on outcomes in resected non-small cell lung cancer. Chest 2014, 146, 644–649. [Google Scholar] [CrossRef]
- Gorai, A.; Sakao, Y.; Kuroda, H.; Uehara, H.; Mun, M.; Ishikawa, Y.; Nakagawa, K.; Masuda, M.; Okumura, S. The clinicopathological features associated with skip N2 metastases in patients with clinical stage IA non-small-cell lung cancer. Eur. J. Cardiothorac. Surg. 2015, 47, 653–658. [Google Scholar] [CrossRef]
- Wang, X.B.; Li, J.; Han, Y. Prognostic significance of preoperative serum carcinoembryonic antigen in non-small cell lung cancer: A meta-analysis. Tumour Biol. 2014, 35, 10105–10110. [Google Scholar] [CrossRef]
- Arriagada, R.; Bergman, B.; Dunant, A.; Le Chevalier, T.; Pignon, J.P.; Vansteenkiste, J.; International Adjuvant Lung Cancer Trial Collaborative Group. Cisplatin-based adjuvant chemotherapy in patients with completely resected non-small-cell lung cancer. N. Engl. J. Med. 2004, 350, 351–360. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Systemic Lymph Node Dissection | Lobe-Specific Lymph Node Dissection | p |
|---|---|---|---|
| n = 265 | n = 534 | ||
| Age (years old), | 66 | 68 | <0.01 |
| median (IQR) | (63–74) | (60–71) | |
| Sex, male (%) | 157 (59.2%) | 328 (61.4%) | 0.55 |
| Smoking history, | 30.0 | 33.9 | 0.68 |
| pack-year (median, IQR) | (0–51.0) | (0–50.0) | |
| Carcinoembryonic antigen (ng/mL) | 9.4 | 8.3 | 0.11 |
| median, IQR | (6.2–18.4) | (6.3–14.5) | |
| Clinical stage n (number, %) | <0.01 | ||
| cN0 | 164 (61.9%) | 407 (76.2%) | |
| cN1-2 | 101 (38.1%) | 127 (23.8%) | |
| Histology (number, %) | 0.29 | ||
| Adenocarcinoma | 183 (69.1%) | 388 (72.7%) | |
| Squamous | 48 (18.1%) | 86 (16.1%) | |
| Others | 34 (12.8%) | 60 (11.2%) | |
| Surgical approach (number, %) | <0.01 | ||
| Thoracoscopy | 25 (9.4%) | 127 (23.8%) | |
| Thoracotomy | 240 (90.6%) | 407 (76.2%) | |
| Type of procedures (number, %) | <0.01 | ||
| Lobectomy | 235 (88.7%) | 529 (99.1%) | |
| Pneumonectomy/Bilobectomy | 30 (11.3%) | 5 (0.9%) | |
| Adjuvant chemotherapy ± Radiotherapy | <0.01 | ||
| (yes, %) | 139 (52.5%) | 117 (21.9%) | |
| Pathological stage | <0.01 | ||
| IA1/IA2/IA3/IB | 5/19/16/35 | 13/79/47/133 | |
| IIA/IIB | 8/60 | 28/90 | |
| IIIA/IIIB | 101/21 | 115/19 | |
| Mutation status | <0.01 | ||
| EGFR or ALK positive | 106 | 148 | |
| No mutations or uninformative | 159 | 386 |
| Characteristics | Systemic Nodal Dissection | Lobe-Specific Nodal Dissection | p |
|---|---|---|---|
| n = 219 | n = 219 | ||
| Age (years old), | 67 | 66 | 0.69 |
| Median, IQR | (61–72) | (61–72) | |
| Sex, male (%) | 131 (59.8%) | 132 (60.3%) | 0.92 |
| Smoking history, | 30.0 | 35.0 | 0.64 |
| pack-year (median, IQR) | (0–52.0) | (0–51.0) | |
| Carcinoembryonic antigen (ng/mL) | 8.9 | 8.3 | 0.82 |
| median, IQR | (6.2–19.2) | (6.5–17.0) | |
| Clinical stage n (number, %) | 0.83 | ||
| cN0 | 154 (70.3%) | 156 (71.2%) | |
| cN1-2 | 65 (29.7%) | 63 (28.8%) | |
| Histology (number, %) | 0.36 | ||
| Adenocarcinoma | 153 (69.9%) | 162 (74.0%) | |
| Squamous | 39 (17.8%) | 33 (15.1%) | |
| Others | 27 (12.3%) | 24 (10.9%) | |
| Surgical approach (number, %) | 0.64 | ||
| Thoracoscopy | 25 (9.4%) | 22 (10.0%) | |
| Thoracotomy | 194 (90.6%) | 197 (90.0%) | |
| Type of procedure (number, %) | 0.76 | ||
| Lobectomy | 213 (97.3%) | 214 (97.7%) | |
| Pneumonectomy/bilobectomy | 6 (2.7%) | 5 (2.3%) | |
| Adjuvant chemotherapy ± Radiotherapy (yes, %) | 88 (40.2%) | 86 (39.3%) | 0.85 |
| Pathological stage | 0.29 | ||
| IA1/IA2/IA3/IB | 5/19/14/34 | 3/21/11/46 | |
| IIA/IIB | 8/49 | 12/47 | |
| IIIA/IIIB | 75/15 | 69/10 | |
| Mutation status | 0.77 | ||
| EGFR or ALK positive | 83 (37.9%) | 86 (39.3%) | |
| No mutations or uninformative | 136 (62.1%) | 133 (60.7%) |
| Variables | Univariate | Multivariate | |
|---|---|---|---|
| p | Hazard Ratio (95% CI) | p | |
| Patient characteristics | |||
| Age | <0.01 * | 1.02 (1.01–1.04) | 0.17 |
| Male | 0.55 | ||
| Pack-year | 0.77 | ||
| Carcinoembryonic antigen | |||
| Level | 0.76 | ||
| Clinical N stage | |||
| N1-2 | <0.01 * | 0.53 (0.36–0.79) | <0.01 * |
| Histology | |||
| Adenocarcinoma or SQCC | 0.32 | ||
| Procedures | |||
| More than lobectomy | <0.01 * | 0.11 (0.04–0.30) | <0.01 * |
| Approach | |||
| Thoracotomy | <0.01 * | 1.87 (1.13–3.05) | 0.01 * |
| Adjuvant | |||
| Chemotherapy and/or radiotherapy | <0.01 * | 0.60 (0.42–0.86) | <0.01 * |
| Pathological stage | |||
| More advanced | <0.01 * | 1.14 (1.04–1.26) | <0.01 * |
| Mutation status | |||
| EGFR or ALK positive | <0.01 * | 0.53 (0.38–0.75) | <0.01 * |
| Variables | Univariate | Multivariate | |
|---|---|---|---|
| p | Hazard Ratio (95%CI) | p | |
| Patient characteristics | |||
| Age | <0.01 * | 1.04 (1.03–1.05) | <0.01 * |
| Female (vs. male) | <0.01 * | 0.82 (0.62–1.09) | 0.16 |
| Pack-year | <0.01 * | 1.04 (1.03–1.05) | 0.14 |
| Carcinoembryonic antigen | |||
| Value | 0.58 | ||
| Clinical N stage | |||
| N0 (vs. cN1-2) | <0.01 * | 0.53 (0.36–0.79) | 0.07 |
| Histology | |||
| Adenocarcinoma or SQCC | <0.01 * | 0.48 | |
| Procedures | |||
| More than lobectomy | <0.01 * | 0.92 (0.58–1.48) | 0.74 |
| Approach | |||
| Thoracotomy (vs. Thoracoscopy) | <0.01 * | 1.56 (1.03–2.37) | 0.04 * |
| Lymph node dissection | |||
| L-SND (vs. SND) | <0.01 | 0.78 (0.61–0.99) | 0.04 * |
| Adjuvant | |||
| Chemotherapy and/or radiotherapy (vs. No) | 0.37 | ||
| Pathological stage | |||
| More advanced | <0.01 * | 1.32 (1.22–1.43) | <0.01 * |
| Mutation status | |||
| EGFR or ALK positive (vs. negative) | <0.01 * | 1.20 (0.90–1.60) | 0.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuroda, H.; Ichinose, J.; Masago, K.; Takahashi, Y.; Nakada, T.; Nakao, M.; Okumura, S.; Hashimoto, K.; Matsuura, Y.; Sakakura, N.; et al. Permissible Outcomes of Lobe-Specific Lymph Node Dissection for Elevated Carcinoembryonic Antigen in Non-Small Cell Lung Cancer. Medicina 2021, 57, 1365. https://doi.org/10.3390/medicina57121365
Kuroda H, Ichinose J, Masago K, Takahashi Y, Nakada T, Nakao M, Okumura S, Hashimoto K, Matsuura Y, Sakakura N, et al. Permissible Outcomes of Lobe-Specific Lymph Node Dissection for Elevated Carcinoembryonic Antigen in Non-Small Cell Lung Cancer. Medicina. 2021; 57(12):1365. https://doi.org/10.3390/medicina57121365
Chicago/Turabian StyleKuroda, Hiroaki, Junji Ichinose, Katsuhiro Masago, Yusuke Takahashi, Takeo Nakada, Masayuki Nakao, Sakae Okumura, Kohei Hashimoto, Yosuke Matsuura, Noriaki Sakakura, and et al. 2021. "Permissible Outcomes of Lobe-Specific Lymph Node Dissection for Elevated Carcinoembryonic Antigen in Non-Small Cell Lung Cancer" Medicina 57, no. 12: 1365. https://doi.org/10.3390/medicina57121365
APA StyleKuroda, H., Ichinose, J., Masago, K., Takahashi, Y., Nakada, T., Nakao, M., Okumura, S., Hashimoto, K., Matsuura, Y., Sakakura, N., Matsushita, H., & Mun, M. (2021). Permissible Outcomes of Lobe-Specific Lymph Node Dissection for Elevated Carcinoembryonic Antigen in Non-Small Cell Lung Cancer. Medicina, 57(12), 1365. https://doi.org/10.3390/medicina57121365