
The Fertility Indicator Equation Using Serum Progesterone and Urinary Pregnanediol-3-Glucuronide for Assessment of Ovulatory to Luteal Phase Transition



Abstract
:1. Introduction
2. Methods
2.1. Fertility Indicator Equation Analysis
2.2. Day-Specific Serum Progesterone and Urinary Pregnanediol-3-Glucuronide Levels
2.3. Computations and Graphics
3. Results
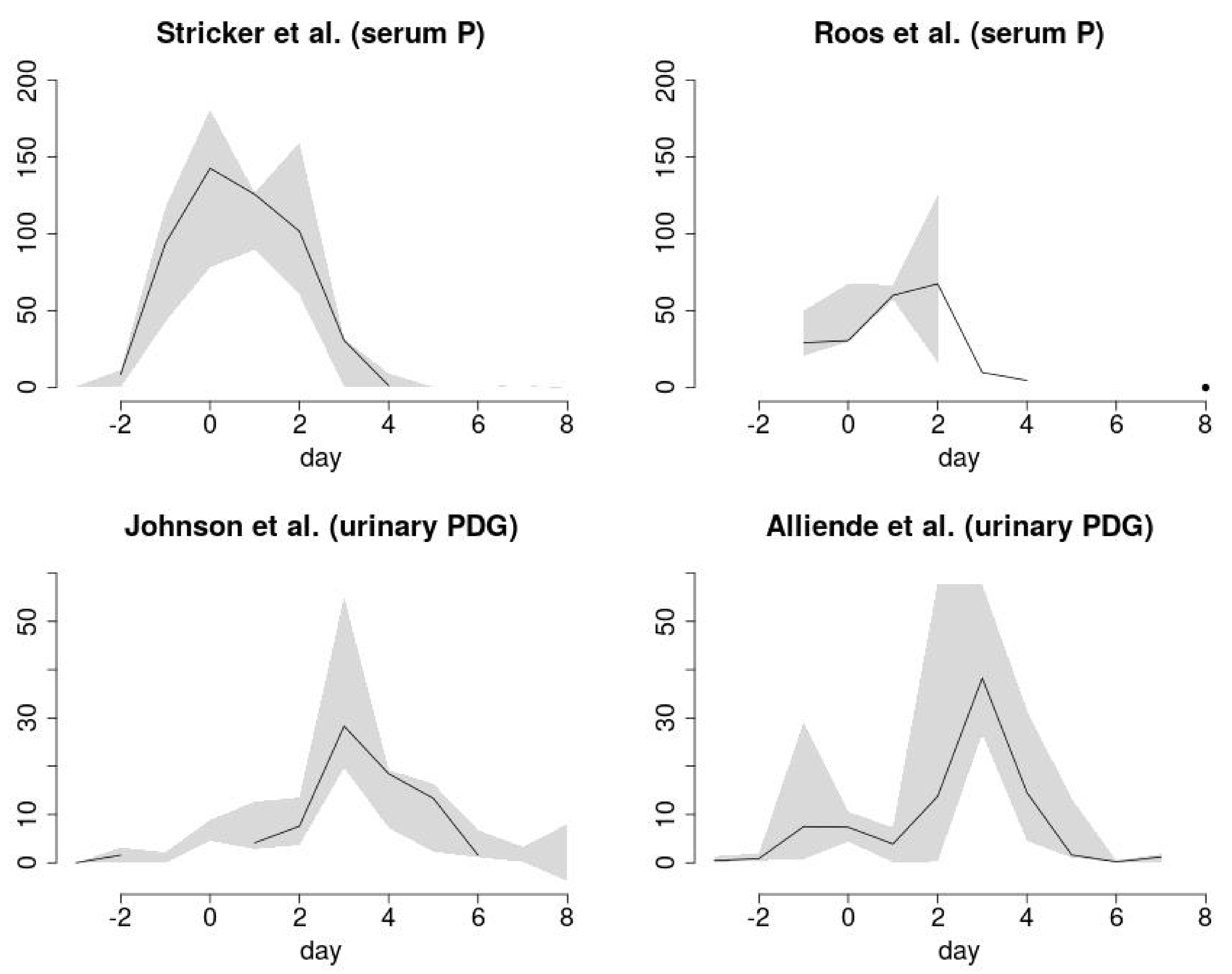
3.1. FIE Analysis of Day-Specific Serum Progesterone Provides a Luteal Phase Signature

{kind=link}
{kind=link}
| Day of Cycle (Day 0, day of ovulation) a | FIE b Stricker P (mean) | FIE Stricker P (5th PCTL) | FIE Stricker P (95th PCTL) | FIE Roos P (median) | FIE Roos P (10th PCTL) | FIE Roos P (90th PCTL) |
|---|---|---|---|---|---|---|
| −16 | -- | -- | -- | -- | -- | -- |
| −15 | -- | -- | -- | -- | -- | -- |
| −14 | −4.62 | 0 | −11.35 | −9.88 | ind | ind |
| −13 | −3.85 | ind | ind | ind | ind | ind |
| −12 | −1.91 | 0 | ind | 18.75 | 11.11 | ind |
| −11 | ind | 0 | ind | ind | ind | 0 |
| −10 | ind | 0 | ind | 0 | ind | ind |
| −9 | −1.62 | 0 | ind | ind | ind | ind |
| −8 | ind | 0 | ind | −1.9 | ind | 1 |
| −7 | ind | 0 | −4.44 | −5.71 | 8.33 | ind |
| −6 | ind | 0 | ind | ind | 0 | ind |
| −5 | 0.41 | 0 | ind | 4.8 | 0 | ind |
| −4 | ind | 0 | ind | ind | ind | ind |
| −3 | ind | 0 | 0.65 | ind | ind | ind |
| −2 | 11.43 | 0 | 8.52 | 20.51 | 16.66 | ind |
| −1 | 117.18 | 93.75 | 42.69 | 29.14 | 50 | 20.59 |
| 0 | 142.65 | 78.22 | 180.82 | 30.56 | 67.5 | 29.68 |
| 1 | 125.65 | 89.55 | 126.74 | 59.95 | 66.72 | 57.17 |
| 2 | 101.7 | 159.4 | 60.38 | 125.11 | 16.47 | 67.45 |
| 3 | 30.66 | 0.49 | 31.5 | 9.75 | ind | ind |
| 4 | 9.1 | 0.38 | 1.18 | 4.55 | ind | ind |
| 5 | 0.25 | ind | 0.07 | ind | ind | ind |
| 6 | 0.12 | ind | 0.46 | ind | ind | ind |
| 7 | ind | ind | 1.42 | ind | ind | ind |
| 8 | −0.24 | −0.96 | ind | ind | ind | −0.12 |
| 9 | ind | −0.75 | ind | 0.02 | −0.36 | ind |
| 10 | ind | −1.73 | ind | ind | −7.16 | ind |
| 11 | −3.41 | −28.24 | ind | −7.02 | −3.89 | −9.48 |
| 12 | −2.68 | −18.86 | ind | |||
| 13 | −4.18 | −4.62 | ind | |||
| 14 | ||||||
| 15 | ||||||
| 16 |
3.2. FIE Analysis of Day-Specific Urinary Pregnanediol-3-Glucuronide Displays a Similar Periovulatory Cluster
| Day of Cycle (Day 0, Day of Ovulation) a | FIE Johnson PDG (Median) | FIE Johnson PDG (10th PCTL) | FIE Johnson PDG (90th PCTL) | FIE Alliende PDG (Mean) | FIE Alliende PDG (Median) | FIE Alliende PDG (5th PCTL) | FIE Alliende PDG (95th PCTL) | FIE Alliende PDG (10th PCTL) | FIE Alliende PDG (90th PCTL) |
|---|---|---|---|---|---|---|---|---|---|
| −16 | -- | -- | -- | -- | -- | -- | -- | -- | -- |
| −15 | ind | ind | ind | -- | -- | -- | -- | -- | -- |
| −14 | ind | ind | ind | ind | ind | ind | ind | ind | ind |
| −13 | −0.5 | 0 | −0.85 | ind | 1.37 | ind | ind | ind | 4.1 |
| −12 | −0.86 | ind | ind | −0.23 | ind | ind | ind | −0.07 | ind |
| −11 | ind | ind | ind | ind | ind | 0.23 | 0.29 | ind | ind |
| −10 | ind | 0 | ind | ind | ind | ind | ind | ind | ind |
| −9 | ind | ind | ind | −0.78 | −0.09 | ind | −2.58 | ind | −3.18 |
| −8 | 0 | ind | ind | ind | ind | 1.47 | ind | 3.75 | ind |
| −7 | ind | ind | ind | ind | ind | ind | 1.57 | ind | 0.13 |
| −6 | ind | ind | ind | −0.26 | ind | ind | ind | ind | ind |
| −5 | 0 | 1.78 | ind | −0.58 | ind | ind | −3.78 | ind | −1.32 |
| −4 | 0 | 0 | −1.9 | ind | ind | −0.15 | ind | ind | −0.42 |
| −3 | 0 | 0 | ind | 0.43 | 0.10 | ind | 1.36 | ind | ind |
| −2 | 1.57 | 0 | 3.14 | 0.45 | 0.51 | 0.47 | 1.6 | ind | 1.95 |
| −1 | ind | 0 | 2.16 | 2.42 | 0.76 | 29.13 | 3.14 | 21.53 | 2.91 |
| 0 | ind | 4.54 | 8.88 | 7.91 | 4.87 | 4.36 | 9.28 | ind | 10.52 |
| 1 | 12.65 | 2.84 | 4.15 | 4.89 | 5.02 | 1.77 | 7.37 | ind | 0.1 |
| 2 | 13.54 | 3.67 | 7.57 | 15.51 | 13.73 | 13.42 | 12.37 | 57.85 | 0.24 |
| 3 | 19.67 | 28.32 | 55.07 | 32.56 | 30.50 | 55.06 | 35.05 | 26.71 | 57.64 |
| 4 | 19.23 | 7.22 | 18.43 | 15.79 | 22.38 | 7.64 | 31.58 | 12.3 | 4.5 |
| 5 | 13.33 | 2.28 | 16.35 | 1.77 | 1.06 | 13.24 | 1.46 | ||
| 6 | 1.55 | 1.14 | 6.74 | 0.48 | 0.19 | 0.09 | ind | ||
| 7 | 0.19 | 3.31 | ind | 1.79 | 1.18 | 0.01 | ind | ||
| 8 | ind | 8.02 | −3.79 | ind | ind | ind | ind | ||
| 9 | ind | ind | ind | ind | ind | ind | ind | ||
| 10 | ind | ind | ind | ind | ind | ind | |||
| 11 | −5.47 | ind | −4.1 | −5.71 | −3.79 | ind | |||
| 12 | −2.04 | ind | −5.89 | −4.57 | −7.05 | ind | |||
| 13 | −1.06 | ind | −2.18 | −2.51 | −0.24 | −9.42 | |||
| 14 | |||||||||
| 15 | |||||||||
| 16 |
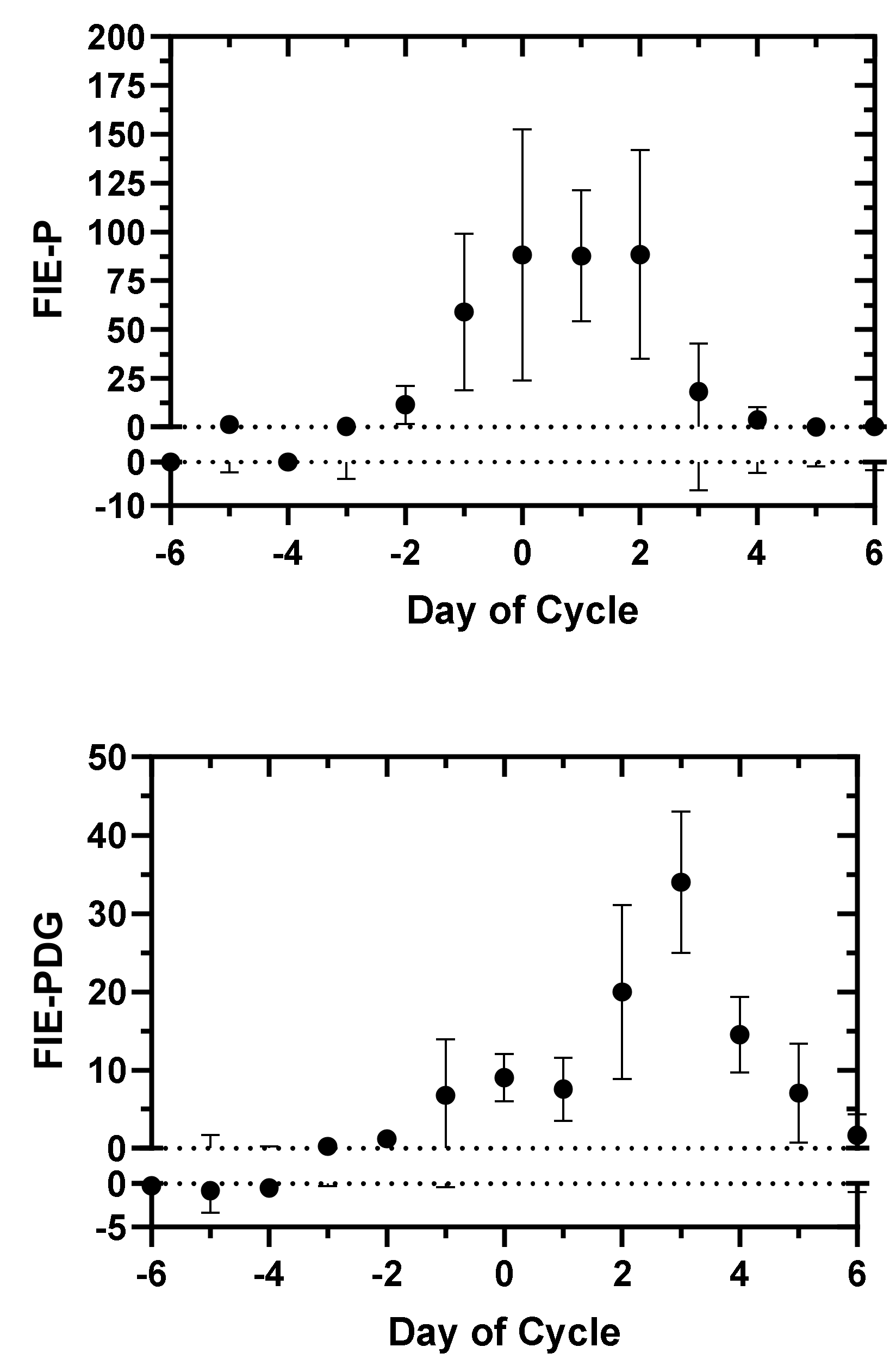
3.3. Characteristics and Comparison of FIE-P and FIE-PDG Clusters


4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gabbe, S.G. Classic pages from the American Journal of Obstetrics and Gynecology. Am. J. Obstet. Gynecol. 1997, 176, 491. [Google Scholar]
- Israel, R.; Mishell, D.R., Jr.; Stone, S.C.; Thorneycroft, I.H.; Moyer, D.L. Single luteal phase serum progesterone assay as an indicator of ovulation. Am. J. Obstet. Gynecol. 1972, 112, 1043–1046. [Google Scholar] [CrossRef]
- Leiva, R.; Bouchard, T.; Boehringer, H.; Abulla, S.; Ecochard, R. Random serum progesterone threshold to confirm ovulation. Steroids 2015, 101, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Carmina, E.; Stanczyk, F.Z.; Lobo, R.A. Laboratory assessment. In Reproductive Endocrinology, 7th ed.; Strauss, J.F., III, Barbieri, R.L., Eds.; Elsevier Saunders: Philadelphia, PA, USA, 2013; pp. 822–851. [Google Scholar]
- O’Connor, K.A.; Brindle, E.; Holman, D.J.; Klein, N.A.; Soules, M.R.; Campbell, K.L.; Fortune, K.; Munro, C.J.; Shofer, J.B.; Lasley, B.L.; et al. Urinary estrone conjugate and pregnanediol-3-glucuronide enzyme immunoassays for population research. Clin. Chem. 2003, 49, 1139–1148. [Google Scholar] [CrossRef] [Green Version]
- Takaya, Y.; Matsubayashi, H.; Kitaya, K.; Nishiyama, R.; Yamaguchi, K.; Takeuchi, T.; Tomomoto, I. Minimum values for midluteal plasma progesterone and estradiol concentrations in patients who achieved pregnancy with timed intercourse or intrauterine insemination without a human menopausal gonadotropin. BMC Res. Notes 2018, 11, 61. [Google Scholar] [CrossRef]
- Edelman, A.; Stouffer, R.; Zava, D.T.; Jensen, J.T. A comparison of blood spot vs. plasma analysis of gonadotropin and ovarian steroid hormone levels in reproductive-age women. Fertil. Steril. 2007, 88, 1404–1407. [Google Scholar] [CrossRef] [Green Version]
- Burke, E.E.; Beqaj, S.; Douglas, N.C.; Luo, R. Concordance of Fingerstick and Venipuncture Sampling for Fertility Hormones. Obstet. Gynecol. 2019, 133, 343–348. [Google Scholar] [CrossRef]
- Blackwell, L.F.; Cooke, D.G.; Brown, S. The Use of Estrone-3-Glucuronide and Pregnanediol-3-Glucuronide Excretion Rates to Navigate the Continuum of Ovarian Activity. Front. Public Health 2018, 6, 153–165. [Google Scholar] [CrossRef]
- Blackwell, L.F.; Vigil, P.; Gross, B.; d’Arcangues, C.; Cooke, D.G.; Brown, J.B. Monitoring of ovarian activity by measurement of urinary excretion rates of estrone glucuronide and pregnanediol glucuronide using the Ovarian Monitor, Part II: Reliability of home testing. Hum. Reprod. 2011, 27, 550–557. [Google Scholar] [CrossRef]
- Blackwell, L.F.; Vigil, P.; Cooke, D.G.; d’Arcangues, C.; Brown, J.B. Monitoring of ovarian activity by daily measurement of urinary excretion rates of oestrone glucuronide and pregnanediol glucuronide using the Ovarian Monitor, Part III: Variability of normal menstrual cycle profiles. Hum. Reprod. 2013, 28, 3306–3315. [Google Scholar] [CrossRef] [Green Version]
- Blackwell, L.F.; Vigil, P.; Alliende, M.E.; Brown, S.; Festin, M.; Cooke, D.G. Monitoring of ovarian activity by measurement of urinary excretion rates using the Ovarian Monitor, Part IV: The relationship of the pregnanediol glucuronide threshold to basal body temperature and cervical mucus as markers for the beginning of the post-ovulatory infertile period. Hum. Reprod. 2016, 31, 445–453. [Google Scholar] [PubMed] [Green Version]
- Ecochard, R.; Leiva, R.; Bouchard, T.; Boehringer, H.; Direito, A.; Mariani, A.; Fehring, R. Use of urinary pregnanediol 3-glucuronide to confirm ovulation. Steroids 2013, 78, 1035–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alliende, M.E.; Arraztoa, J.A.; Guajardo, U.; Mellado, F. Towards the Clinical Evaluation of the Luteal Phase in Fertile Women: A Preliminary Study of Normative Urinary Hormone Profiles. Front. Public Health 2018, 6, 147. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, T.P.; Fehring, R.J.; Schneider, M. Pilot Evaluation of a New Urine Progesterone Test to Confirm Ovulation in Women Using a Fertility Monitor. Front. Public Health 2018, 7, 184. [Google Scholar] [CrossRef] [PubMed]
- Leiva, R.; McNamara-Kilian, M.; Niezgoda, H.; Ecochard, R.; Bouchard, T. Pilot observational prospective cohort study on the use of a novel home-based urinary pregnanediol 3-glucuronide (PDG) test to confirm ovulation when used as adjunct to fertility awareness methods (FAMs) stage 1. BMJ Open 2018, 9, e028496. [Google Scholar] [CrossRef]
- Usala, S.J.; Trindade, A.A. A Novel Fertility Indicator Equation Using Estradiol Levels for Assessment of Phase of the Menstrual Cycle. Medicina 2020, 56, 555. [Google Scholar] [CrossRef]
- Stricker, R.; Eberhart, R.; Chevailler, M.C.; Quinn, F.A.; Bischof, P.; Stricker, R. Establishment of detailed reference values for luteinizing hormone, follicle stimulating hormone, estradiol, and progesterone during different phases of the menstrual cycle on the Abbott ARCHITECT analyzer. Clin. Chem. Lab. Med. 2006, 44, 883–887. [Google Scholar] [CrossRef]
- Roos, J.; Johnson, S.; Weddell, S.; Godehardt, E.; Schiffner, J.; Freundl, G.; Gnoth, C. Monitoring the menstrual cycle: Comparison of urinary and serum reproductive hormones referenced to true ovulation. Eur. J. Contracept. Reprod. Health Care 2015, 20, 438–450. [Google Scholar] [CrossRef]
- Johnson, S.; Weddell, S.; Godbert, S.; Freundl, G.; Roos, J.; Gnoth, C. Development of the first urinary reproductive hormone ranges referenced to independently determined ovulation day. Clin. Chem. Lab. Med. 2015, 53, 1099–1108. [Google Scholar] [CrossRef]
- Direito, A.; Bailly, S.; Mariani, A.; Ecochard, R. Relationships between the luteinizing hormone surge and other characteristics of the menstrual cycle in normally ovulating women. Fertil. Steril. 2013, 99, 279–285. [Google Scholar] [CrossRef]
- Ecochard, R.; Bouchard, T.; Leiva, R.; Abdulla, S.; Dupuis, O.; Duterque, O.; Garmier Billard, M.; Boehringer, H.; Genolini, C. Characterization of hormonal profiles during the luteal phase in regularly menstruating women. Fertil. Steril. 2017, 108, 175–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouchard, T.P.; Genuis, S.J. Personal fertility monitors for contraception. Can. Med. Assoc. J. 2010, 183, 73–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fehring, R.J.; Schneider, M.; Barron, M.L. Efficacy of the Marquette Method of natural family planning. MCN Am. J. Matern. Nurs. 2008, 33, 348–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilgers, T.W.; Stanford, J.B. Creighton Model NaProEducation Technology for avoiding pregnancy. Use effectiveness. J. Reprod. Med. 1998, 43, 495–502. [Google Scholar] [PubMed]
- Blackwell, L.; Cooke, D.; Brown, S. Self-monitoring of fertility hormones: A new era for natural family planning? Linacre Q. 2018, 85, 26–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fehring, R.J.; Bouchard, T.; Schneider, M. Comparison of Abstinence and Coital Frequency Between Two Natural Methods of Family Planning; Marquette University: Milwaukee, WI, USA, 2013. [Google Scholar]
- Simmons, R.G.; Jennings, V. Fertility awareness-based methods of family planning. Best Prac. Res. Clin. Obstet. Gynaecol. 2020, 66, 68–82. [Google Scholar] [CrossRef] [PubMed]
- Freundl, G.; Godehardt, E.; Kern, P.A.; Frank-Herrmann, P.; Koubenec, H.J.; Gnoth, C. Estimated maximum failure rates of cycle monitors using daily conception probabilites in the menstrual cycle. Hum. Reprod. 2003, 18, 2628–2633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alliende, M.E.; Cabezón, C.; Figueroa, H.; Kottmann, C. Cervicovaginal fluid changes to detect ovulation accurately. Am. J. Obstet Gynecol. 2005, 193, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Dunson, D.B.; Baird, D.D.; Wilcox, A.J.; Weinberg, C.R. Day-specific probabilities of clinical pregnancy based on two studies with imperfect measures of ovulation. Hum. Reprod. 1999, 14, 1835–1839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanford, J.B.; White, G.L.; Hatasaka, H. Timing intercourse to achieve pregnancy: Current evidence. Obstet Gynecol. 2002, 100, 1333–1341. [Google Scholar] [CrossRef]
| Data Set, Serum P or Urinary PDG | Start Day of FIE-P or FIE-PDG Cluster | End Day of FIE-P or FIE-PDG Cluster | Day of Maximum FIE-P or FIE-PDG | FIE-P or FIE-PDG Max Value |
|---|---|---|---|---|
| Stricker (P) mean | −2 | 6 | 0 | 142.65 |
| Stricker( P) 5th PCTL | −1 | 4 | 2 | 159.4 |
| Stricker (P) 95th PCTL | −3 | 7 | 0 | 180.82 |
| Roos (P) median | −2 | 4 | 2 | 125.11 |
| Roos (P) 10th PCTL | −2 | 2 | 0 | 67.5 |
| Roos (P) 90th PCTL | −1 | 2 | 2 | 67.45 |
| Johnson (PDG) median | 1 | 7 | 3 | 19.67 |
| Johnson (PDG) 10th PCTL | 0 | 8 | 3 | 28.32 |
| Johnson (PDG) 90th PCTL | −2 | 6 | 3 | 55.07 |
| Alliende (PDG) mean | −3 | 7 | 3 | 32.56 |
| Alliende (PDG) median | −3 | 7 | 3 | 30.50 |
| Alliende (PDG) 5th PCTL | −2 | 4 | 3 | 55.06 |
| Alliende (PDG) 10th PCTL | 2 | 7 | 2 | 57.85 |
| Alliende(PDG) 90th PCTL | −2 | 5 | 3 | 57.64 |
| Alliende(PDG) 95th PCTL | -3 | 4 | 3 | 35.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Usala, S.J.; Alliende, M.E.; Trindade, A.A. The Fertility Indicator Equation Using Serum Progesterone and Urinary Pregnanediol-3-Glucuronide for Assessment of Ovulatory to Luteal Phase Transition. Medicina 2021, 57, 134. https://doi.org/10.3390/medicina57020134
Usala SJ, Alliende ME, Trindade AA. The Fertility Indicator Equation Using Serum Progesterone and Urinary Pregnanediol-3-Glucuronide for Assessment of Ovulatory to Luteal Phase Transition. Medicina. 2021; 57(2):134. https://doi.org/10.3390/medicina57020134
Chicago/Turabian StyleUsala, Stephen J., María Elena Alliende, and A. Alexandre Trindade. 2021. "The Fertility Indicator Equation Using Serum Progesterone and Urinary Pregnanediol-3-Glucuronide for Assessment of Ovulatory to Luteal Phase Transition" Medicina 57, no. 2: 134. https://doi.org/10.3390/medicina57020134
APA StyleUsala, S. J., Alliende, M. E., & Trindade, A. A. (2021). The Fertility Indicator Equation Using Serum Progesterone and Urinary Pregnanediol-3-Glucuronide for Assessment of Ovulatory to Luteal Phase Transition. Medicina, 57(2), 134. https://doi.org/10.3390/medicina57020134