
Serological Parameters and Vascular Investigation for a Better Assessment in DVT during Pregnancy—A Systematic Review

Abstract
:1. Introduction
- -
- in more than 88% of cases, it affects the left lower limb as a result of the compression on the left common iliac vein accentuated by the growth of the uterus [6]
- -
- it occurs most commonly in the third pregnancy trimester on the ilio-femoral vein
- -
- localization above the groin is much more common compared with other non-pregnant DVT patients
- -
- it frequently occurs, postpartum, in the first six weeks after birth
2. The Research Was Performed as Follows
3. Epidemiology
4. Laboratory Assessment of DVT
5. Clinical Vascular Evaluation of DVT
- -
- the examination of the lower limbs should be performed on both the whole limb and on segments, for patients with suspicion/risk of DVT (according to current literature recommendations [30].
- -
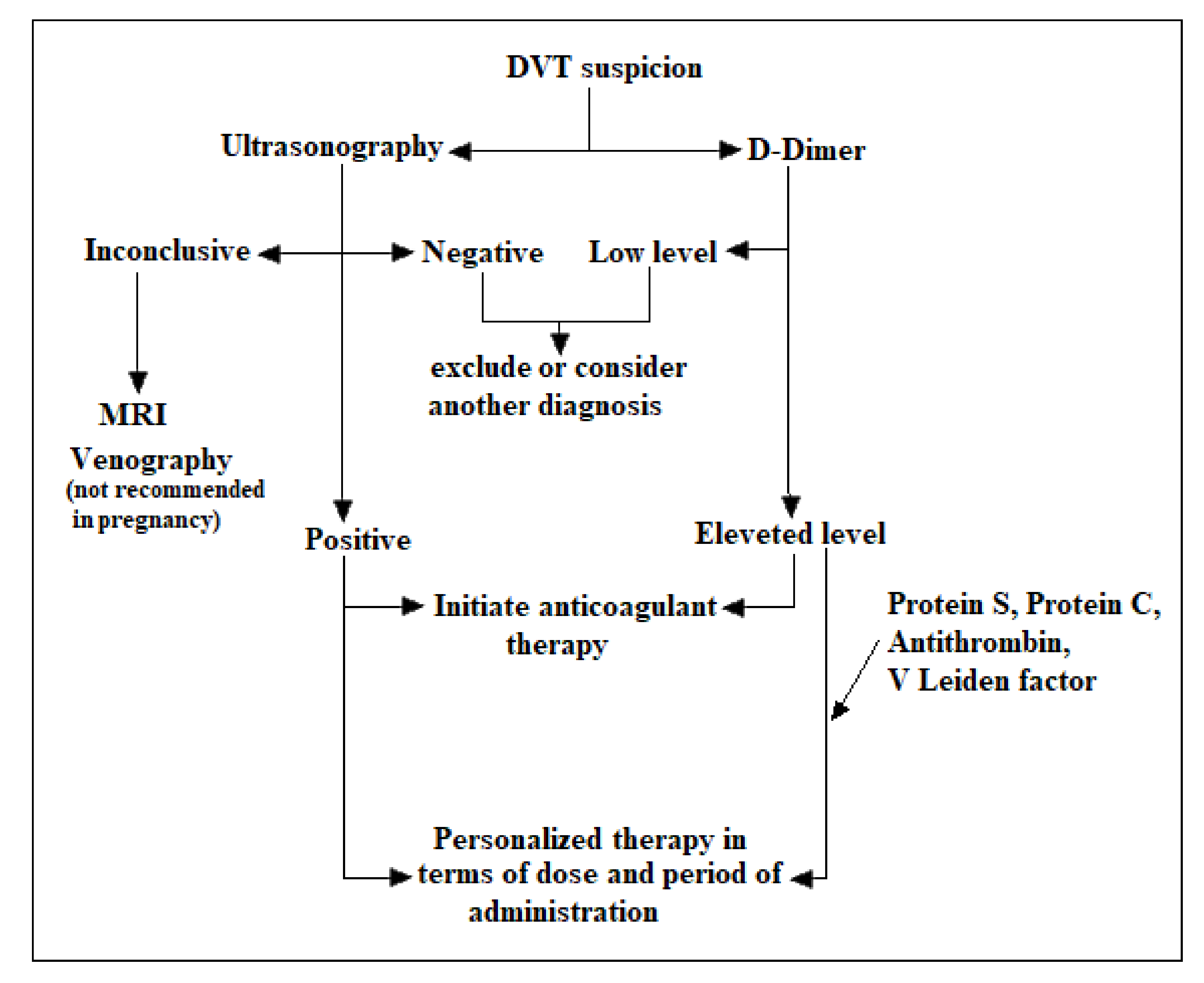
- examination by ultrasonography as the first line of investigation in DVT due to lack of risks. It is less sensitive than venography but it is an affordable and available tool. Even so, it has low accuracy in pelvic vein thrombosis. Although ultrasonography is the main DVT method of determination, magnetic resonance imaging (MRI) is recommended when ultrasound is inconclusive and the clinical symptoms persist. A high-quality study [31] shows that the prevalence of venography over ultrasonography in DVT identification in asymptomatic patients is about 22%. Even so, the study concluded that particularly for the proximal veins, ultrasound is accurate in diagnosing DVT in asymptomatic patients having a 95% confidence. For the distal vein, the ultrasound accuracy in DVT detection is inconclusive due to anatomical particularities.
- -
- examination of venography only where other investigations are inconclusive. Venography is generally accepted as the gold standard in detecting DVT. Its limitation comes from the invasive method of investigation, and thus non-invasive diagnostic tests like ultrasound replace venography in routine screening for DVT, particularly in pregnant patients. In conclusion, the ultrasound investigation is the gold standard in particular cases of pregnancy.
6. Diagnosis and Therapeutic Steps
7. Therapeutic Steps during Pregnancy
8. Antithrombotic Treatment
9. General Guidelines in DVT and PE
10. General Guidelines in Thrombophilia before and after Childbirth
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Devis, P.; Knuttinen, M.G. Deep venous thrombosis in pregnancy: Incidence, pathogenesis and endovascular management. Cardivasc. Diagn. Ther. 2017, 7 (Suppl. S3), S309–S319. [Google Scholar] [CrossRef]
- Conklin, P.; Soares, G.M.; Dubel, G.J.; Ahn, S.H.; Murphy, T.P. Acute deep vein thrombosis (DVT); Evolving treatment strategies and endovascular therapy. Rhode Isl. Med. Health 2009, 92, 394–397. [Google Scholar]
- Kesieme, E.; Kesieme, C.; Jebbin, N.; Irekpita, E.; Dongo, A. Deep vein thrombosis: A clinical review. J. Blood Med. 2011, 2, 59–69. [Google Scholar] [CrossRef] [Green Version]
- Chan, W.S.; Spencer, F.A.; Ginsbergm, J.S. Anatomic distribution of deep vein thrombosis in pregnancy. CMAJ 2010, 182, 657–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinelli, I.; Bucciarelli, P.; Mannucci, P.M. Thrombotic risk factors: Basic pathophysiology. Crit. Care Med. 2010, 38 (Suppl. S2), S3–S9. [Google Scholar] [CrossRef] [PubMed]
- De Jong, P.G.; Coppens, M.; Middeldorp, S. Duration of anticoagulant therapy for venous thromboembolism: Balancing benefits and harms on the long term. Br. J. Haematol. 2012, 158, 433–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marik, P.E.; Plante, L.A. Venous thromboembolic disease and pregnancy. N. Engl. J. Med. 2008, 359, 2025–2033. [Google Scholar] [CrossRef]
- Margeti, S. Laboratory investigation of thrombophilia. J. Med. Biochem. 2014, 33, 28–46. [Google Scholar] [CrossRef] [Green Version]
- Lindhoff-Last, E.; Luxembourg, B. Evidence-based indications for thrombophilia screening. Vasa 2008, 37, 19–30. [Google Scholar] [CrossRef]
- Lussana, F.; Dentali, F.; Abbate, R.; d’Aloja, E.; D’Angelo, A.; De Stefano, V.; Faioni, E.M.; Grandone, E.; Legnani, C.; Martinelli, I. Screening for thrombophilia and antithrombotic prophylaxis in pregnancy: Guidelines of the Italian Society for Haemostasis and Thrombosis(SISET). Thromb. Res. 2009, 124, 19–25. [Google Scholar] [CrossRef] [Green Version]
- Margetic, S. Diagnostic algorithm for thrombophilia screening. Clin. Chem. Lab. Med. 2010, 48 (Suppl. S1), S27–S39. [Google Scholar] [CrossRef] [PubMed]
- Wee-Shian, C. Diagnosis of venous thromboembolism in pregnancy. Thromb. Res. 2018, 163, 221–228. [Google Scholar]
- Ercan, Ş.; Özkan, S.; Yücel, N.; Orçun, A. Establishing reference intervals for D-dimers to trimesters. J. Mater. Fetal Neonatal Med. 2015, 28, 983–987. [Google Scholar] [CrossRef] [PubMed]
- Hedengran, K.K.; Andersen, M.R.; Stender, S.; Szecsi, P.B. Large D-Dimer fluctuation in normal pregnancy: A longitudinal cohort study of 4117 samples from 714 healthy Danish women. Obstet. Gynecol. Int. 2016, 2016, 3561675. [Google Scholar] [CrossRef] [Green Version]
- Kline, J.A.; Richardson, D.M.; Than, M.P.; Penaloza, A.; Roy, P.M. Systematic Review and Meta-analysis of Pregnant Patients Investigated for Suspected Pulmonary Embolism in the Emergency Department. Acad. Emerg. Med. 2014, 21, 949–959. [Google Scholar] [CrossRef] [Green Version]
- Morse, M. Establishing a normal range for D-Dimer levels through pregnancy to aid in the diagnosis of pulmonary embolism and deep vein thrombosis. Thromb. Haemost. 2004, 2, 1202–1204. [Google Scholar] [CrossRef]
- Edward, H.S. Thromboembolism in Pregnancy Workup. Available online: https://emedicine.medscape.com/article/2056380-workup (accessed on 10 February 2021).
- Ducloy-Bouthors, A.S.; Duhamel, A.; Kipnis, E.; Tournoys, A.; Prado-Dupont, A.; Elkalioubie, A.; Jeanpierre, E.; Debize, G.; Peynaud-Debayle, E.; DeProst, D.; et al. Post-partum haemorrage related early increase in D-Dimers is inhibited by tranexamic acid: Haemostasis parameters of a randomized controlled open labelled trial. Br. J. Anesth. 2016, 116, 641–648. [Google Scholar] [CrossRef] [Green Version]
- Middeldorp, S. Thrombophilia and pregnancy complications:cause or association? J. Thromb. Haemost. 2007, 5 (Suppl. S1), 276–282. [Google Scholar] [CrossRef]
- Dalen, J.E. Should patients with venous thromboembolism be screened for thrombophilia? Am. J. Med. 2008, 121, 458–463. [Google Scholar] [CrossRef]
- Cohn, D.M.; Vansenne, F.; Kaptein, A.A.; De Borgie, C.A.; Middeldorp, S. The psychological impact of testing for thrombophilia: A systematic review. J. Thromb. Haemost. 2008, 6, 1099–1104. [Google Scholar] [CrossRef] [PubMed]
- Bates, S.M.; Greer, I.A.; Middeldorp, S. Venous Thromboembolism, thrombophilia, antithrombotic therapy and pregnancy: Antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence- based clinical practice guidelines. Chest 2012, 141, 691s–736s. [Google Scholar] [CrossRef] [Green Version]
- Den Heijer, M.; Koster, T.; Blom, H.J.; Bos, G.M.; Briët, E.; Reitsma, P.H.; Vandenbroucke, J.P.; Rosendaal, F.R. Hyperhomocysteinemia as a risk factor for deep-vein thrombosis. N. Engl. J. Med. 1996, 334, 759–762. [Google Scholar] [CrossRef] [Green Version]
- Debreceni, L. Homocysteine—A risk factor for atherosclerosis. Orv. Hetil. 2001, 142, 1439–1444. [Google Scholar]
- Milosevic-Tosic, M.; Borota, J. Hyperhomocysteinemia—A risk factor for development of occlusive vascular diseases. Med. Pregl. 2002, 55, 385–391. [Google Scholar] [CrossRef] [Green Version]
- Falcon, C.R.; Cattaneo, M.; Panzeri, D.; Martinelli, I.; Mannucci, P.M. High prevalence of hyperhomocysteinemia in patients with juvenile venous thrombosis. Arterioscler. Thromb. 2000, 14, 1080–1083. [Google Scholar] [CrossRef] [Green Version]
- Badulescu, O.V.; Ciocoiu, M.; Filip, N.; Veringa, V. The Efficiency of Substitutive Treatment with Moroctocog Alfa in Managing Hemostasis in Patients with Hemophilia A Without Inhibitors With Total Knee Arthroplasties. Rev. Chim. 2019, 69, 3702. [Google Scholar] [CrossRef]
- Badulescu, O.V.; Filip, N.; Sirbu, P.D.; Bararu-bojan, I.; Vladeanu, M.; Bojan, A.; Ciocoiu, M. Current practices in haemophilic patients undergoing orthopedic surgery a systematic review. Exp. Ther. Med. 2020, 20, 1. [Google Scholar] [CrossRef]
- Dargaud, Y.; Rugeri, L.; Fleury, C.; Battie, C.; Gaucherand, P.; Huissoud, C.; Rudigoz, R.C.; Desmurs-Clavel, H.; Ninet, J.; Trzeciak, M.C. Personalized thromboprophylaxis using a risk score for the management of pregnancies with high risk of thrombosis: A prospective clinical study. J. Thromb. Haemost. 2017, 15, 897–906. [Google Scholar] [CrossRef] [Green Version]
- De Maeseneer, M.G.; Bochanen, N.; van Rooijen, G.; Neglén, P. Analysis of 1338 patients with acute limn deep venous thrombosis (DVT) supports the inadequacy of the term “proximal DVT”. Eur. J. Vasc. Endovasc. Surg. 2016, 51, 415–420. [Google Scholar] [CrossRef] [Green Version]
- Kassaï, B.; Boissel, J.P.; Cucherat, M.; Sonie, S.; Shah, N.R.; Leizorovicz, A. A systematic review of the accuracy of ultrasound in the diagnosis of deep venous thrombosis in asymptomatic patients. Thromb. Haemost. 2004, 91, 655–666. [Google Scholar]
- Dua, A.; Thondapu, V.; Rosovsky, R.; Hunt, D.; Latz, C.; Waller, H.D.; Manchester, S.; Patell, R.; Romero, J.; Ghoshhajra, B.; et al. Deep Vein Thrombosis Protocol Optimization to Minimize Healthcare Worker Exposure in Coronavirus Disease-2019. Available online: https://www.jvsvenous.org/article/S2213-333X(20)30438-8/fulltext (accessed on 8 February 2021).
- Varaki, E.S.; Gargiulo, G.D.; Penkala, S.; Breen, P.P. Peripheral vascular disease assessmentin the lower limb: A review of current and emerging non-invasive diagnostic methods. Biomed. Eng. Online 2018, 17, 1–27. [Google Scholar]
- Laurence, N.; John, J.; Cronan, M.P.; Lilly, G.J.; Merli, S.A.; Barbara, S.; Hertzberg, M.; Robert DeJong, R.D.M.S.; Michael, B.; Streiff, M.H. Ultrasound for Lower Extremity Deep Venous ThrombosisCirculation. Meissner 2018, 137, 1505–1515. [Google Scholar]
- Zitek, J.A.; Baydoun, J.; Baird, J. Tools for the Clinician: The Essentials of Bedside (ED or ICU) Ultrasound for Deep Vein Thrombosis. Curr. Emerg. Hosp. Med. Rep. 2013, 1, 65–70. [Google Scholar] [CrossRef] [Green Version]
- Sucker, C. Prophylaxis and Therapy of Venous Thrombotic Events (VTE) in Pregnancy and the Postpartum Period. Geburtshilfe Frauenheilkd. 2020, 80, 48–59. [Google Scholar] [CrossRef] [Green Version]
- Alsheef, M.A.; Alabbad, A.M.; Albassam, R.A.; Alarfaj, R.M.; Zaidi, A.R.Z.; Al-Arfaj, O.; Abu-Shaheen, A. Pregnancy and Venous Thromboembolism: Risk Factors, Trends, Management, and Mortality. Biomed. Res. Int. 2020, 2020, 4071892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, W.; Eikelboom, J.W.; Ginsberg, J.S. Inherited thrombophilia and pregnancy associated venous thromboembolism. BMJ 2007, 334, 1318–1321. [Google Scholar] [CrossRef] [Green Version]
- Voicu, D.I.; Munteanu, O.; Gherghiceanu, F.; Arsene, L.V.; Bohiltea, R.E.; Gradinaru, D.M.; Cirstoiu, M.M. Maternal inherited thrombophilia and pregnancy outcomes. Exp. Ther. Med. 2020, 20, 2411–2414. [Google Scholar] [CrossRef]
- James, A.H.; Rhee, E.; Thames, B.; Philipp, C.S. Characterization of antithrombin levels in pregnancy. Thromb. Res. 2014, 134, 648–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khare, M.; Nelson-Piercy, C. Acquired thrombophilias and pregnancy. Best Pract. Res. Clin. Obstet. Gynaecol. 2003, 17, 491–507. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Key Summary | References |
|---|---|
| Clinical vascular assessment | [2,30,31,33,34,35] |
| Serological assessment | [8,9,11,13,14,16,17,18,20,23,24,25,26] |
| Management and therapy in DVT-pregnancy | [6,22,27,28,29,36,39,40] |
| Review and protocols | [1,3,4,5,7,10,12,15,19,21,32,37,38,41] |
| Symptoms and Signs of Deep Venous Thrombosis |
|---|
|
|
|
|
|
| Blood and Serum Modification in Deep Venous Thrombosis |
|---|
|
|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Filip, C.; Socolov, D.G.; Albu, E.; Filip, C.; Serban, R.; Popa, R.F. Serological Parameters and Vascular Investigation for a Better Assessment in DVT during Pregnancy—A Systematic Review. Medicina 2021, 57, 160. https://doi.org/10.3390/medicina57020160
Filip C, Socolov DG, Albu E, Filip C, Serban R, Popa RF. Serological Parameters and Vascular Investigation for a Better Assessment in DVT during Pregnancy—A Systematic Review. Medicina. 2021; 57(2):160. https://doi.org/10.3390/medicina57020160
Chicago/Turabian StyleFilip, Catalina, Demetra Gabriela Socolov, Elena Albu, Cristiana Filip, Roxana Serban, and Radu Florin Popa. 2021. "Serological Parameters and Vascular Investigation for a Better Assessment in DVT during Pregnancy—A Systematic Review" Medicina 57, no. 2: 160. https://doi.org/10.3390/medicina57020160
APA StyleFilip, C., Socolov, D. G., Albu, E., Filip, C., Serban, R., & Popa, R. F. (2021). Serological Parameters and Vascular Investigation for a Better Assessment in DVT during Pregnancy—A Systematic Review. Medicina, 57(2), 160. https://doi.org/10.3390/medicina57020160