
A Randomized Controlled Trial on the Effectiveness of Epidermal Growth Factor-Containing Ointment on the Treatment of Solar Lentigines as Adjuvant Therapy

 , , , , and
, , , , and
Abstract
:1. Introduction
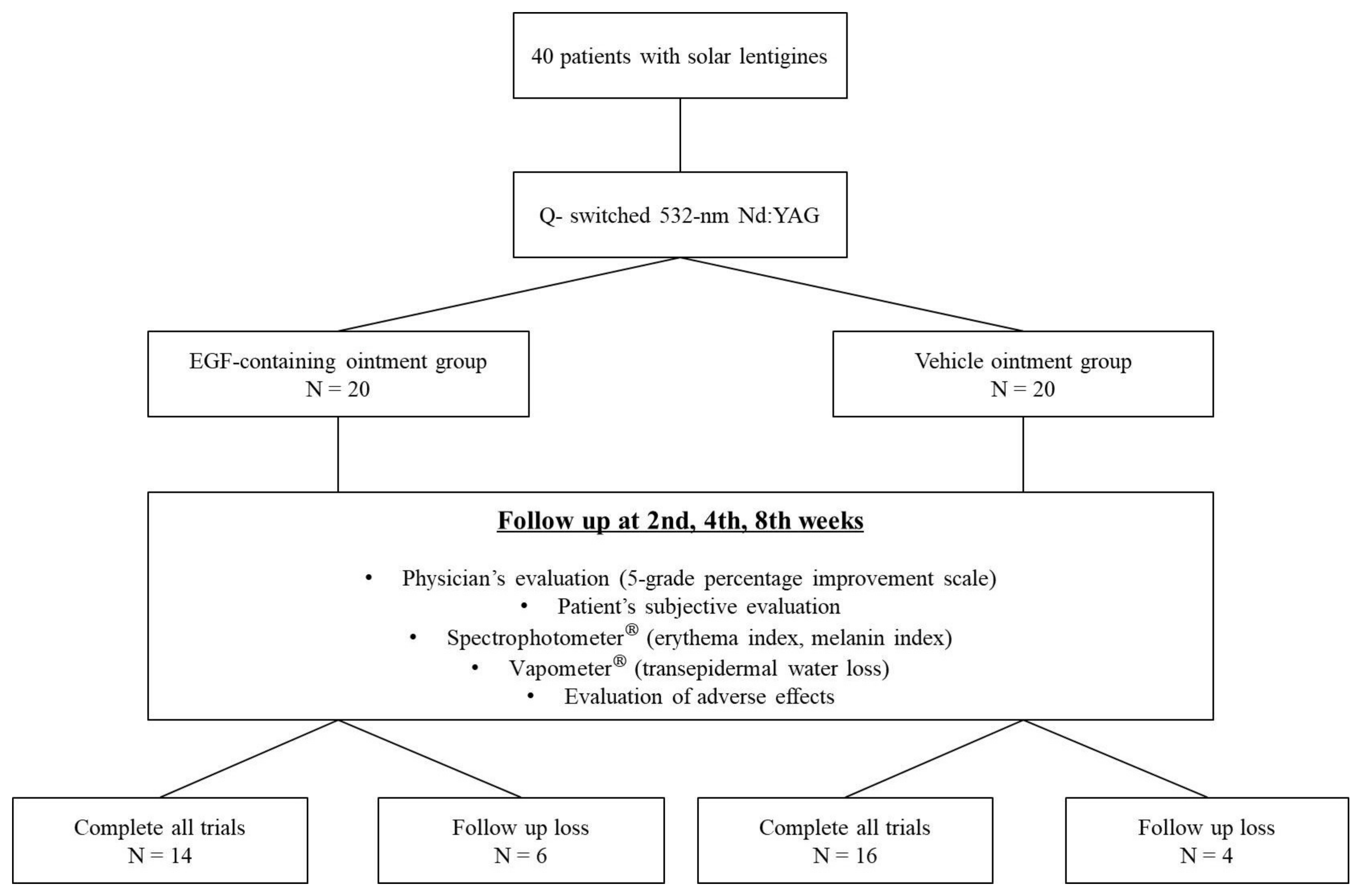
2. Materials and Methods
2.1. Subjects
2.2. Study Design
2.3. Outcome Measurement
2.3.1. Physician’s Evaluation
2.3.2. Objective Evaluation of Melanin Index, Erythema Index, and Transepidermal Water Loss
2.3.3. The Patient’s Subjective Evaluation
2.3.4. PIH Measurement
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Subjects
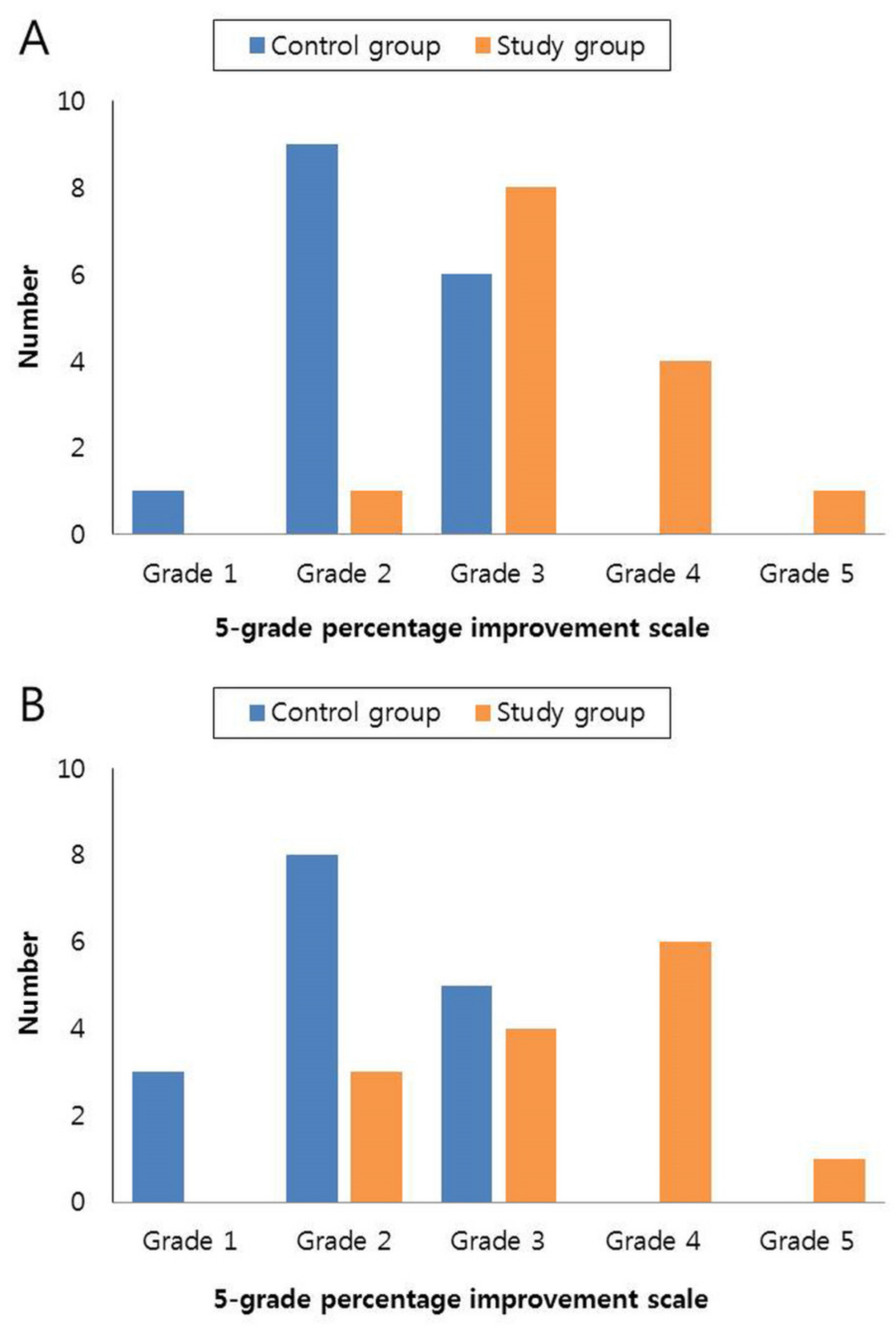
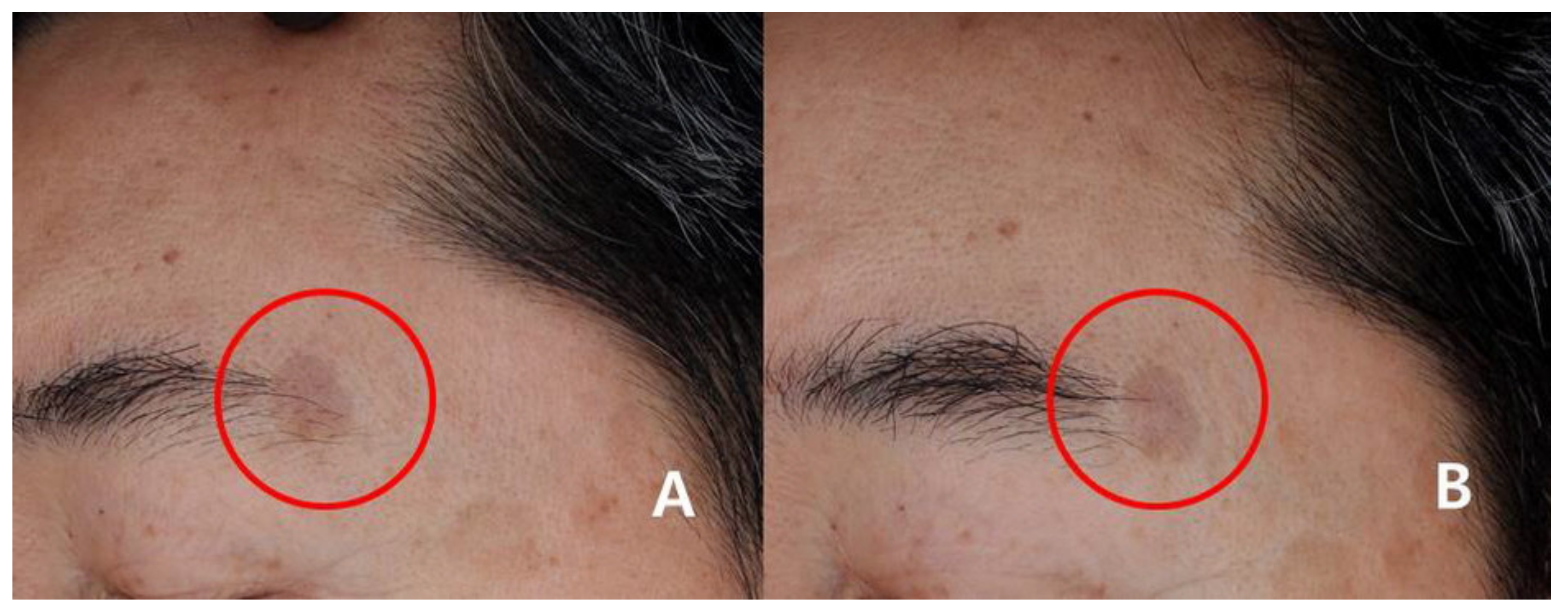
3.2. Physician’s Assessment
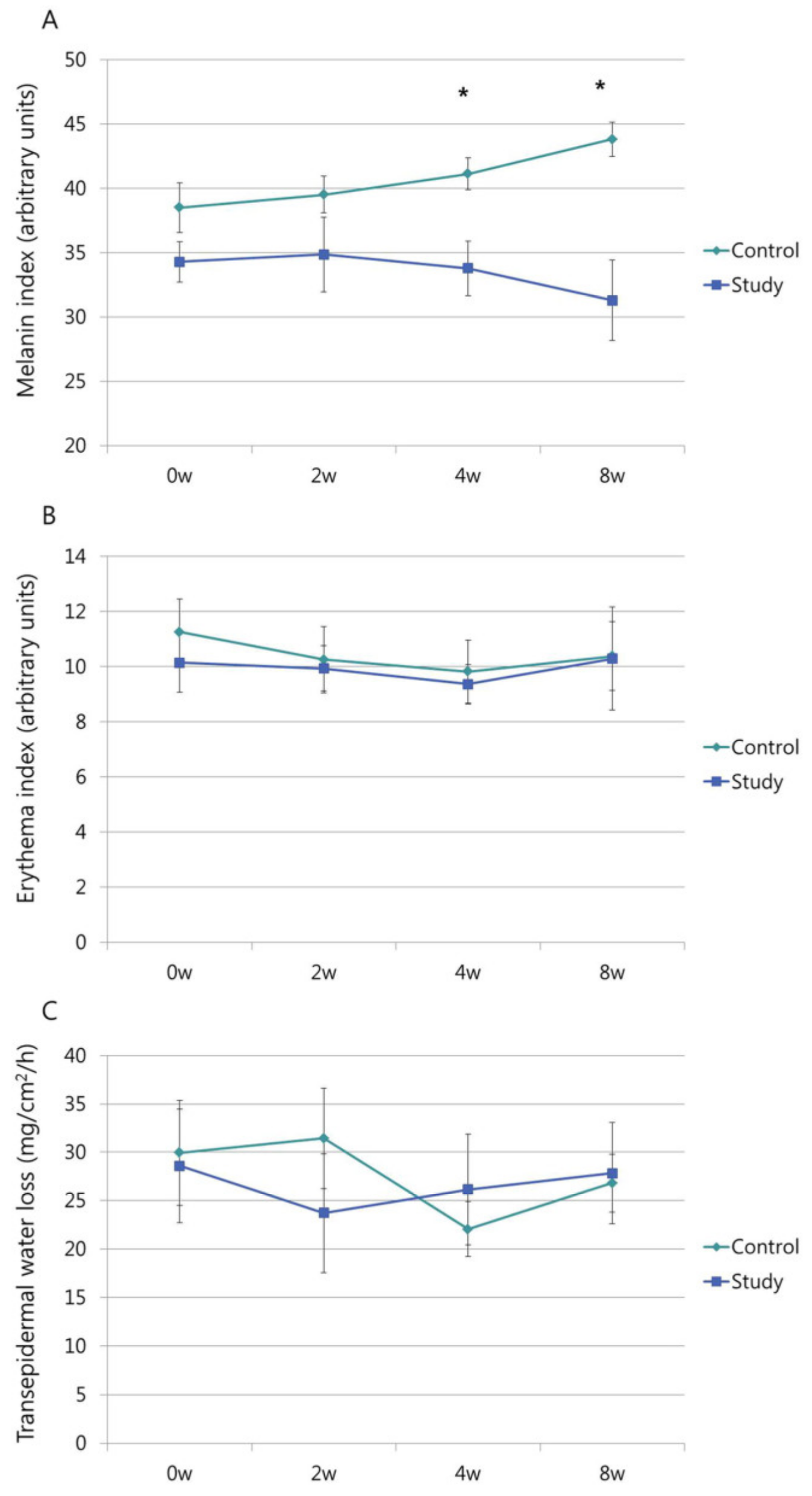
3.3. MI, EI, and TEWL
3.4. Patient’s Satisfaction
3.5. Incidence of PIH and Other Adverse Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ortonne, J.P.; Pandya, A.G.; Lui, H.; Hexsel, D. Treatment of solar lentigines. J. Am. Acad. Dermatol. 2006, 54, S262–S271. [Google Scholar] [CrossRef]
- Ortonne, J.P. Pigmentary changes of the ageing skin. Br. J. Dermatol. 1990, 122 (Suppl. 35), 21–28. [Google Scholar] [CrossRef]
- Hüls, A.; Vierkötter, A.; Gao, W.; Krämer, U.; Yang, Y.; Ding, A.; Stolz, S.; Matsui, M.; Kan, H.; Wang, S.; et al. Traffic-Related Air Pollution Contributes to Development of Facial Lentigines: Further Epidemiological Evidence from Caucasians and Asians. J. Invest. Dermatol. 2016, 136, 1053–1056. [Google Scholar] [CrossRef] [Green Version]
- Hattori, H.; Kawashima, M.; Ichikawa, Y.; Imokawa, G. The epidermal stem cell factor is over-expressed in lentigo senilis: Implication for the mechanism of hyperpigmentation. J. Investig. Dermatol. 2004, 122, 1256–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkar, R.; Arora, P.; Garg, K.V. Cosmeceuticals for Hyperpigmentation: What is Available? J. Cutan. Aesthet. Surg. 2013, 6, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Bukvić Mokos, Z.; Lipozenčić, J.; Ceović, R.; Stulhofer Buzina, D.; Kostović, K. Laser therapy of pigmented lesions: Pro and contra. Acta Dermatol. Croat. 2010, 18, 185–189. [Google Scholar]
- Cameli, N.; Abril, E.; Agozzino, M.; Mariano, M. Clinical and instrumental evaluation of the efficacy of a new depigmenting agent containing a combination of a retinoid, a phenolic agent and an antioxidant for the treatment of solar lentigines. Dermatology 2015, 230, 360–366. [Google Scholar] [CrossRef]
- Farris, P.K. Combination therapy for solar lentigines. J. Drugs Dermatol. 2004, 3, S23–S26. [Google Scholar]
- Negishi, K.; Akita, H.; Tanaka, S.; Yokoyama, Y.; Wakamatsu, S.; Matsunaga, K. Comparative study of treatment efficacy and the incidence of post-inflammatory hyperpigmentation with different degrees of irradiation using two different quality-switched lasers for removing solar lentigines on Asian skin. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 307–312. [Google Scholar] [CrossRef]
- Anderson, R.R.; Margolis, R.J.; Watenabe, S.; Flotte, T.; Hruza, G.J.; Dover, J.S. Selective photothermolysis of cutaneous pigmentation by Q-switched Nd: YAG laser pulses at 1064, 532, and 355 nm. J. Investig. Dermatol. 1989, 93, 28–32. [Google Scholar] [CrossRef] [Green Version]
- Sadighha, A.; Saatee, S.; Muhaghegh-Zahed, G. Efficacy and adverse effects of Q-switched ruby laser on solar lentigines: A prospective study of 91 patients with Fitzpatrick skin type II, III, and IV. Dermatol. Surg. 2008, 34, 1465–1468. [Google Scholar] [CrossRef] [PubMed]
- Park, G.H.; do Rhee, Y.; Moon, H.R.; Won, C.H.; Lee, M.W.; Choi, J.H.; Moon, K.C.; Chang, S.E. Effect of an epidermal growth factor-containing cream on postinflammatory hyperpigmentation after Q-switched 532-nm neodymium-doped yttrium aluminum garnet laser treatment. Dermatol. Surg. 2015, 41, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Yun, W.J.; Bang, S.H.; Min, K.H.; Kim, S.W.; Lee, M.W.; Chang, S.E. Epidermal growth factor and epidermal growth factor signaling attenuate laser-induced melanogenesis. Dermatol. Surg. 2013, 39, 1903–1911. [Google Scholar] [CrossRef] [PubMed]
- Williams, F.N.; Herndon, D.N. Metabolic and Endocrine Considerations After Burn Injury. Clin. Plast Surg. 2017, 44, 541–553. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela-Silva, C.M.; Tuero-Iglesias, Á.D.; García-Iglesias, E.; González-Díaz, O.; Del Río-Martín, A.; Yera Alos, I.B.; Fernández-Montequín, J.I.; López-Saura, P.A. Granulation response and partial wound closure predict healing in clinical trials on advanced diabetes foot ulcers treated with recombinant human epidermal growth factor. Diabetes Care 2013, 36, 210–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Ojalvo, A.; Berlanga Acosta, J.; Figueroa-Martínez, A.; Béquet-Romero, M.; Mendoza-Marí, Y.; Fernández-Mayola, M.; Fabelo-Martínez, A.; Guillén-Nieto, G. Systemic translation of locally infiltrated epidermal growth factor in diabetic lower extremity wounds. Int. Wound J. 2019, 16, 1294–1303. [Google Scholar] [CrossRef]
- Savory, S.A.; Agim, N.G.; Mao, R.; Peter, S.; Wang, C.; Maldonado, G.; Bearden Dietert, J.; Lieu, T.J.; Wang, C.; Pretzlaff, K.; et al. Reliability assessment and validation of the postacne hyperpigmentation index (PAHPI), a new instrument to measure postinflammatory hyperpigmentation from acne vulgaris. J. Am. Acad. Dermatol. 2014, 70, 108–114. [Google Scholar] [CrossRef]
- Sotoodian, B.; Maibach, H.I. Noninvasive test methods for epidermal barrier function. Clin. Dermatol. 2012, 30, 301–310. [Google Scholar] [CrossRef]
- Roskos, K.V.; Guy, R.H. Assessment of skin barrier function using transepidermal water loss: Effect of age. Pharm. Res. 1989, 6, 949–953. [Google Scholar] [CrossRef]
- Praetorius, C.; Sturm, R.A.; Steingrimsson, E. Sun-induced freckling: Ephelides and solar lentigines. Pigment. Cell Melanoma Res. 2014, 27, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Schallreuter, K.U.; Kothari, S.; Chavan, B.; Spencer, J.D. Regulation of melanogenesis—Controversies and new concepts. Exp. Dermatol. 2008, 17, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Imokawa, G. Autocrine and paracrine regulation of melanocytes in human skin and in pigmentary disorders. Pigment. Cell Res. 2004, 17, 96–110. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, D.; Cardinali, G.; Aspite, N.; Cota, C.; Luzi, F.; Bellei, B.; Briganti, S.; Amantea, A.; Torrisi, M.R.; Picardo, M. Role of fibroblast-derived growth factors in regulating hyperpigmentation of solar lentigo. Br. J. Dermatol. 2010, 163, 1020–1027. [Google Scholar] [CrossRef]
- Lin, C.B.; Hu, Y.; Rossetti, D.; Chen, N.; David, C.; Slominski, A.; Seiberg, M. Immuno-histochemical evaluation of solar lentigines: The association of KGF/KGFR and other factors with lesion development. J. Dermatol. Sci 2010, 59, 91–97. [Google Scholar] [CrossRef]
- Chen, N.; Hu, Y.; Li, W.H.; Eisinger, M.; Seiberg, M.; Lin, C.B. The role of keratinocyte growth factor in melanogenesis: A possible mechanism for the initiation of solar lentigines. Exp. Dermatol. 2010, 19, 865–872. [Google Scholar] [CrossRef]
- Ishikawa, Y.; Niwano, T.; Hirano, S.; Numano, K.; Takasima, K.; Imokawa, G. Whitening effect of L-ascorbate-2-phosphate trisodium salt on solar lentigos. Arch. Dermatol. Res. 2019, 311, 183–191. [Google Scholar] [CrossRef]
- Draelos, Z.D. The combination of 2% 4-hydroxyanisole (mequinol) and 0.01% tretinoin effectively improves the appearance of solar lentigines in ethnic groups. J. Cosmet. Dermatol. 2006, 5, 239–244. [Google Scholar] [CrossRef]
- Grippaudo, F.R.; Di Russo, P.P. Effects of topical application of B-Resorcinol and Glycyrrhetinic acid monotherapy and in combination with fractional CO(2) laser treatment for benign hand hyperpigmentation treatment. J. Cosmet. Dermatol. 2016, 15, 413–419. [Google Scholar] [CrossRef] [PubMed]
- Campanati, A.; Giannoni, M.; Scalise, A.; De Blasio, S.; Giuliano, A.; Giuliodori, K.; Ganzetti, G.; Bolletta, E.; Di Benedetto, G.; Offidani, A. Efficacy and Safety of Topical Pidobenzone 4% as Adjuvant Treatment for Solar Lentigines: Result of a Randomized, Controlled, Clinical Trial. Dermatology 2016, 232, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Tokumaru, S.; Higashiyama, S.; Endo, T.; Nakagawa, T.; Miyagawa, J.I.; Yamamori, K.; Hanakawa, Y.; Ohmoto, H.; Yoshino, K.; Shirakata, Y.; et al. Ectodomain shedding of epidermal growth factor receptor ligands is required for keratinocyte migration in cutaneous wound healing. J. Cell Biol. 2000, 151, 209–220. [Google Scholar] [CrossRef] [Green Version]
- Dogan, S.; Demirer, S.; Kepenekci, I.; Erkek, B.; Kiziltay, A.; Hasirci, N.; Müftüoglu, S.; Nazikoglu, A.; Renda, N.; Dincer, U.D.; et al. Epidermal growth factor-containing wound closure enhances wound healing in non-diabetic and diabetic rats. Int. Wound J. 2009, 6, 107–115. [Google Scholar] [CrossRef]
- Kondo, S.; Kuroyanagi, Y. Development of a wound dressing composed of hyaluronic acid and collagen sponge with epidermal growth factor. J. Biomater. Sci. Polym. Ed. 2012, 23, 629–643. [Google Scholar] [CrossRef] [PubMed]
- Raja, S.K.; Garcia, M.S.; Isseroff, R.R. Wound re-epithelialization: Modulating keratinocyte migration in wound healing. Front. Biosci. 2007, 12, 2849–2868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Starner, R.J.; McClelland, L.; Abdel-Malek, Z.; Fricke, A.; Scott, G. PGE(2) is a UVR-inducible autocrine factor for human melanocytes that stimulates tyrosinase activation. Exp. Dermatol. 2010, 19, 682–684. [Google Scholar] [CrossRef] [Green Version]
- Roméro-Graillet, C.; Aberdam, E.; Biagoli, N.; Massabni, W.; Ortonne, J.P.; Ballotti, R. Ultraviolet B radiation acts through the nitric oxide and cGMP signal transduction pathway to stimulate melanogenesis in human melanocytes. J. Biol. Chem. 1996, 271, 28052–28056. [Google Scholar] [CrossRef] [Green Version]
- Vachiramon, V.; Iamsumang, W.; Triyangkulsri, K. Q-switched double frequency Nd:YAG 532-nm nanosecond laser vs. double frequency Nd:YAG 532-nm picosecond laser for the treatment of solar lentigines in Asians. Lasers Med. Sci. 2018, 33, 1941–1947. [Google Scholar] [CrossRef]
- Stratigos, A.J.; Dover, J.S.; Arndt, K.A. Laser treatment of pigmented lesions--2000: How far have we gone? Arch. Dermatol. 2000, 136, 915–921. [Google Scholar] [CrossRef]
- Ho, S.G.; Chan, N.P.; Yeung, C.K.; Shek, S.Y.; Kono, T.; Chan, H.H. A retrospective analysis of the management of freckles and lentigines using four different pigment lasers on Asian skin. J. Cosmet. Laser 2012, 14, 74–80. [Google Scholar] [CrossRef]
- Kang, H.J.; Na, J.I.; Lee, J.H.; Roh, M.R.; Ko, J.Y.; Chang, S.E. Postinflammatory hyperpigmentation associated with treatment of solar lentigines using a Q-Switched 532-nm Nd: YAG laser: A multicenter survey. J. Dermatol. Treat. 2017, 28, 447–451. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.C.; Sue, Y.M.; Yang, C.H.; Chen, C.K. A comparison of Q-switched alexandrite laser and intense pulsed light for the treatment of freckles and lentigines in Asian persons: A randomized, physician-blinded, split-face comparative trial. J. Am. Acad. Dermatol. 2006, 54, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Rutnin, S.; Pruettivorawongse, D.; Thadanipon, K.; Vachiramon, V. A Prospective Randomized Controlled Study of Oral Tranexamic Acid for the Prevention of Postinflammatory Hyperpigmentation After Q-Switched 532-nm Nd:YAG Laser for Solar Lentigines. Lasers Surg Med. 2019, 51, 850–858. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Kim, H.; Kim, H.S. Topical Brimonidine Tartrate 0.33% Gel on Postlaser Erythema: Our Experience and Review of the Literature. Dermatol. Surg. 2018, 44, 144–147. [Google Scholar] [CrossRef] [PubMed]
- West, T.B.; Alster, T.S. Effect of pretreatment on the incidence of hyperpigmentation following cutaneous CO2 laser resurfacing. Dermatol. Surg. 1999, 25, 15–17. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group | Study Group | p-Value | |
|---|---|---|---|
| Number | 16 | 14 | |
| Sex (M/F) | 5/11 | 3/11 | |
| Age (years) | 58.63 ± 2.53 | 56.71 ± 2.62 | 0.605 |
| MI | 38.5 ± 1.95 | 34.29 ± 1.57 | 0.109 |
| EI | 11.25 ± 1.20 | 10.14 ± 4.06 | 0.504 |
| TEWL | 29.94 ± 5.44 | 28.59 ± 5.90 | 0.867 |
| 4 Weeks | 8 Weeks | |||
|---|---|---|---|---|
| Control Group | Study Group | Control Group | Study Group | |
| Worse | 1 (6.25%) | 0 | 3 (18.75%) | 0 |
| No change | 9 (56.25%) | 1 (7.14%) | 8 (50%) | 3 (21.43%) |
| Improved | 6 (37.5%) | 8 (57.14%) | 5 (31.25%) | 4 (28.57%) |
| Much improved | 0 | 4 (28.57%) | 0 | 6 (42.86%) |
| Very much improved | 0 | 1 (7.14%) | 0 | 1 (7.14%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.O.; Kim, H.R.; Kim, J.C.; Kang, S.Y.; Jung, M.J.; Chang, S.E.; Park, C.W.; Chung, B.Y. A Randomized Controlled Trial on the Effectiveness of Epidermal Growth Factor-Containing Ointment on the Treatment of Solar Lentigines as Adjuvant Therapy. Medicina 2021, 57, 166. https://doi.org/10.3390/medicina57020166
Kim HO, Kim HR, Kim JC, Kang SY, Jung MJ, Chang SE, Park CW, Chung BY. A Randomized Controlled Trial on the Effectiveness of Epidermal Growth Factor-Containing Ointment on the Treatment of Solar Lentigines as Adjuvant Therapy. Medicina. 2021; 57(2):166. https://doi.org/10.3390/medicina57020166
Chicago/Turabian StyleKim, Hye One, Hye Ran Kim, Jin Cheol Kim, Seok Young Kang, Min Je Jung, Sung Eun Chang, Chun Wook Park, and Bo Young Chung. 2021. "A Randomized Controlled Trial on the Effectiveness of Epidermal Growth Factor-Containing Ointment on the Treatment of Solar Lentigines as Adjuvant Therapy" Medicina 57, no. 2: 166. https://doi.org/10.3390/medicina57020166
APA StyleKim, H. O., Kim, H. R., Kim, J. C., Kang, S. Y., Jung, M. J., Chang, S. E., Park, C. W., & Chung, B. Y. (2021). A Randomized Controlled Trial on the Effectiveness of Epidermal Growth Factor-Containing Ointment on the Treatment of Solar Lentigines as Adjuvant Therapy. Medicina, 57(2), 166. https://doi.org/10.3390/medicina57020166