
Impact of Lactate Clearance on Early Outcomes in Pediatric ECMO Patients

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jenks, C.L.; Raman, L.; Dalton, H.J. Pediatric Extracorporeal Membrane Oxygenation. Crit. Care Clin. 2017, 33, 825–841. [Google Scholar] [CrossRef]
- O’Halloran, C.P.; Andren, K.G.; Mecklosky, J.; Larsen, S.; Brediger, S.; Vitali, S.; Zalieckas, J.M.; Fynn-Thompson, F.; Thiagarajan, R.R.; Alexander, P.M.A. Mortality and Factors Associated with Hemorrhage During Pediatric Extracorporeal Membrane Oxygenation. Pediatr. Crit. Care Med. 2020, 21, 75–81. [Google Scholar] [CrossRef]
- Slottosch, I.; Liakopoulos, O.; Kuhn, E.; Scherner, M.; Deppe, A.-C.; Sabashnikov, A.; Mader, N.; Choi, Y.-H.; Wippermann, J.; Wahlers, T. Lactate and lactate clearance as valuable tool to evaluate ECMO therapy in cardiogenic shock. J. Crit. Care 2017, 42, 35–41. [Google Scholar] [CrossRef]
- Khorsandi, M.; Dougherty, S.; Bouamra, O.; Pai, V.; Curry, P.; Tsui, S.; Clark, S.; Westaby, S.; Al-Attar, N.; Zamvar, V. Extra-corporeal membrane oxygenation for refractory cardiogenic shock after adult cardiac surgery: A systematic review and meta-analysis. J. Cardiothorac. Surg. 2017, 12, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Lazzeri, C.; Bonizzoli, M.; Cianchi, G.; Batacchi, S.; Terenzi, P.; Cozzolino, M.; Bernardo, P.; Peris, A. Lactate and Echocardiography Before Veno-Venous Extracorporeal Membrane Oxygenation Support. Heart Lung Circ. 2018, 27, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Mungan, I.; Kazancı, D.; Bektaş, Ş.; Ademoglu, D.; Turan, S. Does lactate clearance prognosticates outcomes in ECMO therapy: A retrospective observational study. BMC Anesthesiol. 2018, 18, 152. [Google Scholar] [CrossRef] [PubMed]
- Sabashnikov, A.; Djordjevic, I.; Deppe, A.-C.; Kuhn, E.W.; Merkle, J.; Weber, C.; Sindhu, D.; Eghbalzadeh, K.; Zeriouh, M.; Liakopoulos, O.J.; et al. Managing Traps and Pitfalls During Initial Steps of an ECMO Retrieval Program Using a Miniaturized Portable System: What Have We Learned From the First Two Years? Artif. Organs 2018, 42, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Merkle, J.; Azizov, F.; Fatullayev, J.; Weber, C.; Maier, J.; Eghbalzadeh, K.; Sabashnikov, A.; Pfister, R.; Wahlers, T.; Michels, G. Monitoring of adult patient on venoarterial extracorporeal membrane oxygenation in intensive care medicine. J. Thorac. Dis. 2019, 11 (Suppl. 6), S946–S956. [Google Scholar] [CrossRef]
- Azizov, F.; Merkle, J.; Fatullayev, J.; Eghbalzadeh, K.; Djordjevic, I.; Weber, C.; Saenko, S.; Kroener, A.; Zeriouh, M.; Sabashnikov, A.; et al. Outcomes and factors associated with early mortality in pediatric and neonatal patients requiring ex-tracorporeal membrane oxygenation for heart and lung failure. J. Thorac. Dis. 2019, 11 (Suppl. 6), S871–S888. [Google Scholar] [CrossRef]
- Merkle, J.; Azizov, F.; Sabashnikov, A.; Weixler, V.; Weber, C.; Djordjevic, I.; Eghbalzadeh, K.; Kröner, A.; Zeriouh, M.; Wahlers, T.; et al. Pediatric patients requiring extracorporeal membrane oxygenation in heart failure: 30-day outcomes; mid- and long-term survival. A single center experience. Artif. Organs 2019, 43, 966–975. [Google Scholar] [CrossRef] [PubMed]
- Sabashnikov, A.; Merkle, J.; Azizov, F.; Djordjevic, I.; Eghbalzadeh, K.; Tunggal, I.; Weber, C.; Weixler, V.; Rustenbach, C.; Zeriouh, M.; et al. Early and long-term outcomes comparing neonates, infants, and preadolescents requiring ex-tracorporeal membrane oxygenation for heart failure. Perfusion 2019, 35, 323–330. [Google Scholar] [CrossRef]
- Li, C.-L.; Wang, H.; Jia, M.; Ma, N.; Meng, X.; Hou, X.-T. The early dynamic behavior of lactate is linked to mortality in postcardiotomy patients with extracorporeal membrane oxygenation support: A retrospective observational study. J. Thorac. Cardiovasc. Surg. 2015, 149, 1445–1450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Napp, L.C.; Kühn, C.; Bauersachs, J. ECMO in cardiac arrest and cardiogenic shock. Herz 2017, 42, 27–44. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.P.; Chauhan, S.; Bisoi, A.K.; Sahoo, M. Lactate clearance for initiating and weaning off extracorporeal membrane oxygenation in a child with regressed left ventricle after arterial switch operation. Ann. Card. Anaesth. 2016, 19, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Attanà, P.; Lazzeri, C.; Picariello, C.; Dini, C.S.; Gensini, G.F.; Valente, S. Lactate and lactate clearance in acute cardiac care patients. Eur. Heart J. Acute Cardiovasc. Care. 2012, 1, 115–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yanase, S.; Yasuda, K.; Ishii, N. Small-Scale Colorimetric Assays of Intracellular Lactate and Pyruvate in the Nematode Caenorhabditis elegans. J. Vis. Exp. 2018, 16, e57807. [Google Scholar] [CrossRef] [Green Version]
- Zang, Z.; Xu, H.; Dong, L.; Gao, F.; Yan, J. Prognostic significance of early lactate clearance rate for severe acute respiratory failure patients on extracorporeal membrane oxygenation. Chin. J. Tuberc. Respir. Dis. 2014, 37, 197–201. [Google Scholar]
- Schwartz, S.; Floh, A.A. Is glucose metabolism important for patients on extracorporeal membrane oxygenation? Pediatr. Crit. Care Med. 2015, 16, 296–297. [Google Scholar] [CrossRef] [PubMed]
- Jean-St-Michel, E.; Chetan, D.; Schwartz, S.M.; van Arsdell, G.S.; Floh, A.A.; Honjo, O.; Conway, J. Outcomes in Patients with Persistent Ventricular Dysfunction After Stage I Palliation for Hy-poplastic Left Heart Syndrome. Pediatr. Cardiol. 2016, 37, 239–247. [Google Scholar] [CrossRef]
- Luo, Y.; Fritz, C.; Hammache, N.; Grandmougin, D.; Kimmoun, A.; Orlowski, S.; Tran, N.; Albuisson, E.; Levy, B. Low versus standard-blood-flow reperfusion strategy in a pig model of refractory cardiac arrest resuscitated with Extra Corporeal Membrane Oxygenation. Resuscitation 2018, 133, 12–17. [Google Scholar] [CrossRef]
- Park, S.J.; Kim, S.-P.; Kim, J.B.; Jung, S.-H.; Choo, S.J.; Chung, C.H.; Lee, J.W. Blood lactate level during extracorporeal life support as a surrogate marker for survival. J. Thorac. Cardiovasc. Surg. 2014, 148, 714–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buijs, E.A.; Houmes, R.J.; Rizopoulos, D.; Wildschut, E.D.; Reiss, I.K.; Ince, C.; Tibboel, D. Arterial lactate for predicting mortality in children requiring extracorporeal membrane oxygenation. Minerva Anestesiol. 2014, 80, 1282–1293. [Google Scholar] [PubMed]
- Scolari, F.L.; Schneider, D.; Fogazzi, D.V.; Gus, M.; Rover, M.M.; Bonatto, M.G.; De Araújo, G.N.; Zimerman, A.; Sganzerla, D.; Goldraich, L.A.; et al. Association between serum lactate levels and mortality in patients with cardiogenic shock receiving mechanical circulatory support: A multicenter retrospective cohort study. BMC Cardiovasc. Disord. 2020, 20, 496. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall | Survivors | Non-Survivors | p-Value | |
|---|---|---|---|---|
| Age (days) | 98(12;653) | 128(16;188) | 84(9;5722) | 0.77 |
| Gender (m/f) | 24/17 | 18/9 | 6/8 | 0.19 |
| Weight (gram) | 5040(3247;11,000) | 5200(3230;9000) | 4600(3050;68,000) | 0.44 |
| Length (cm) | 58(51;84) | 58(51;70) | 90(51;180) | 0.38 |
| MAP (mmHg) | 37(26;43) | 35(23;50) | 40(27;43) | 0.74 |
| Heart rate (min−1) | 147(131;177) | 145(135;180) | 160(65;177) | 0.95 |
| Blood sugar (mg/dL) | 200 ± 86 | 196 ± 75 | 209 ± 108 | 0.97 |
| HCO3−1 (mEq/L) | 20.2 ± 6.1 | 22.4 ± 5.3 | 16.8 ± 6.1 | 0.03 |
| Body temperature (°C) | 35.6(34.1;36) | 35.8(35.4;36.3) | 34(32;36) | 0.13 |
| Lactate (mmol/L) | 11 ± 5.8 | 9.8 ± 5.3 | 13.5 ± 6.1 | 0.07 |
| Arterial blood pH | 7.220(7.075;7.304) | 7.273(7.108;7.355) | 7.105(6.815;7.265) | 0.08 |
| Base excess (mEq/L) | −5.6(−14.7;3.1) | −3.1(−5.6;4.0) | −15(−17;−9) | 0.01 |
| paO2 (mmHg) | 41(32;58) | 43(37;57) | 41(26;70) | 0.50 |
| paCO2 (mmHg) | 46(35;64) | 45(36;61) | 50(31;94) | 0.55 |
| Overall | Survivors | Non-Survivors | p-Value | |
|---|---|---|---|---|
| Peak lactate level in the first 24 h of ECMO support (mmol/L) | 11.8 ± 6.8 | 10.4 ± 6.0 | 14.7 ± 7.1 | 0.07 |
| Lactate (mmol/L) | ||||
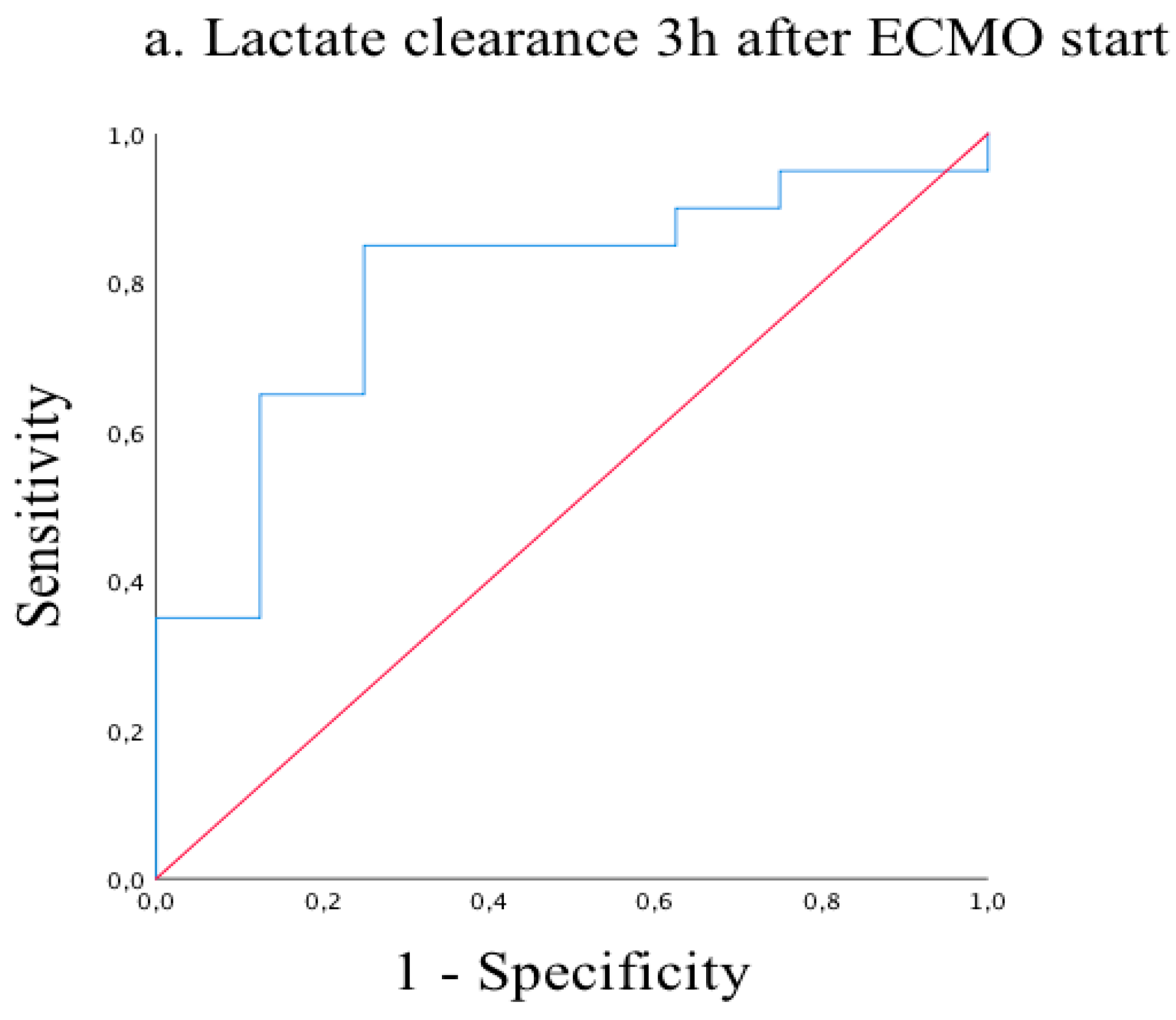
| 3 h after ECMO start | 8.5 ± 5.5 | 6.9 ± 5.0 | 10.1 ± 7.3 | 0.059 |
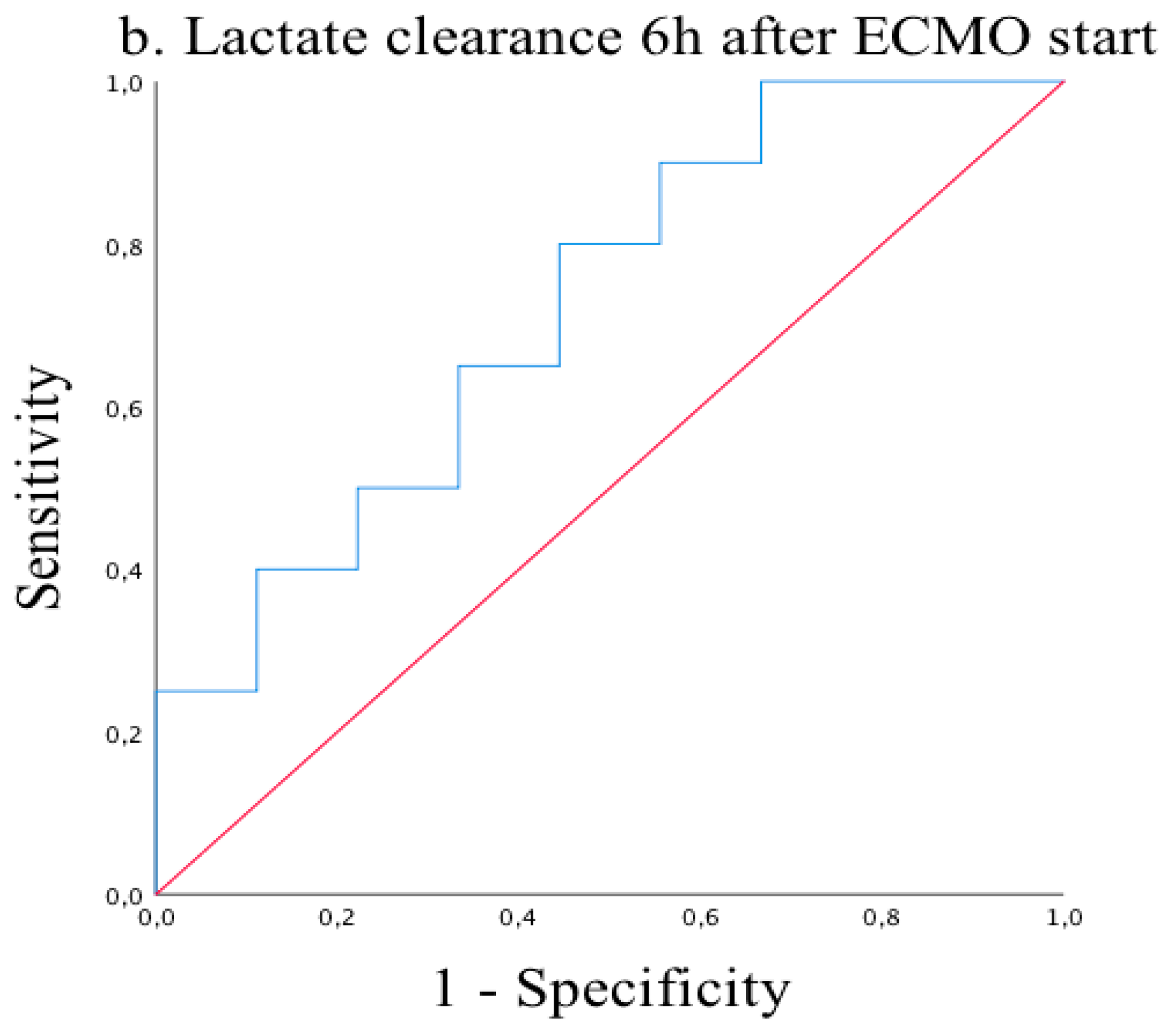
| 6 h after ECMO start | 5.3 ± 4.9 | 3.8 ± 2.7 | 6.7 ± 6.0 | 0.015 |
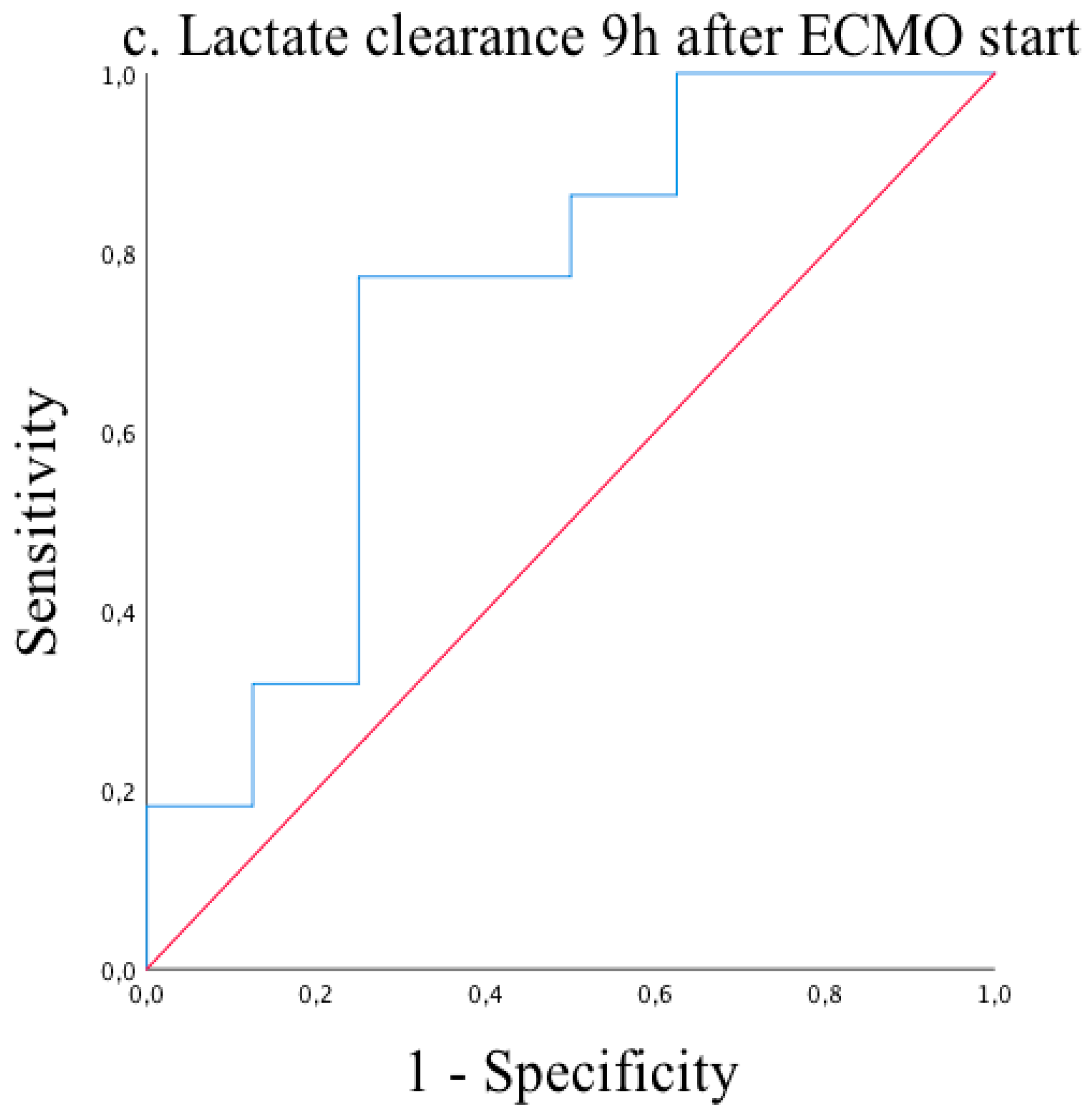
| 9 h after ECMO start | 4.2 ± 3.0 | 3.3 ± 2.0 | 4.4 ± 2.4 | 0.075 |
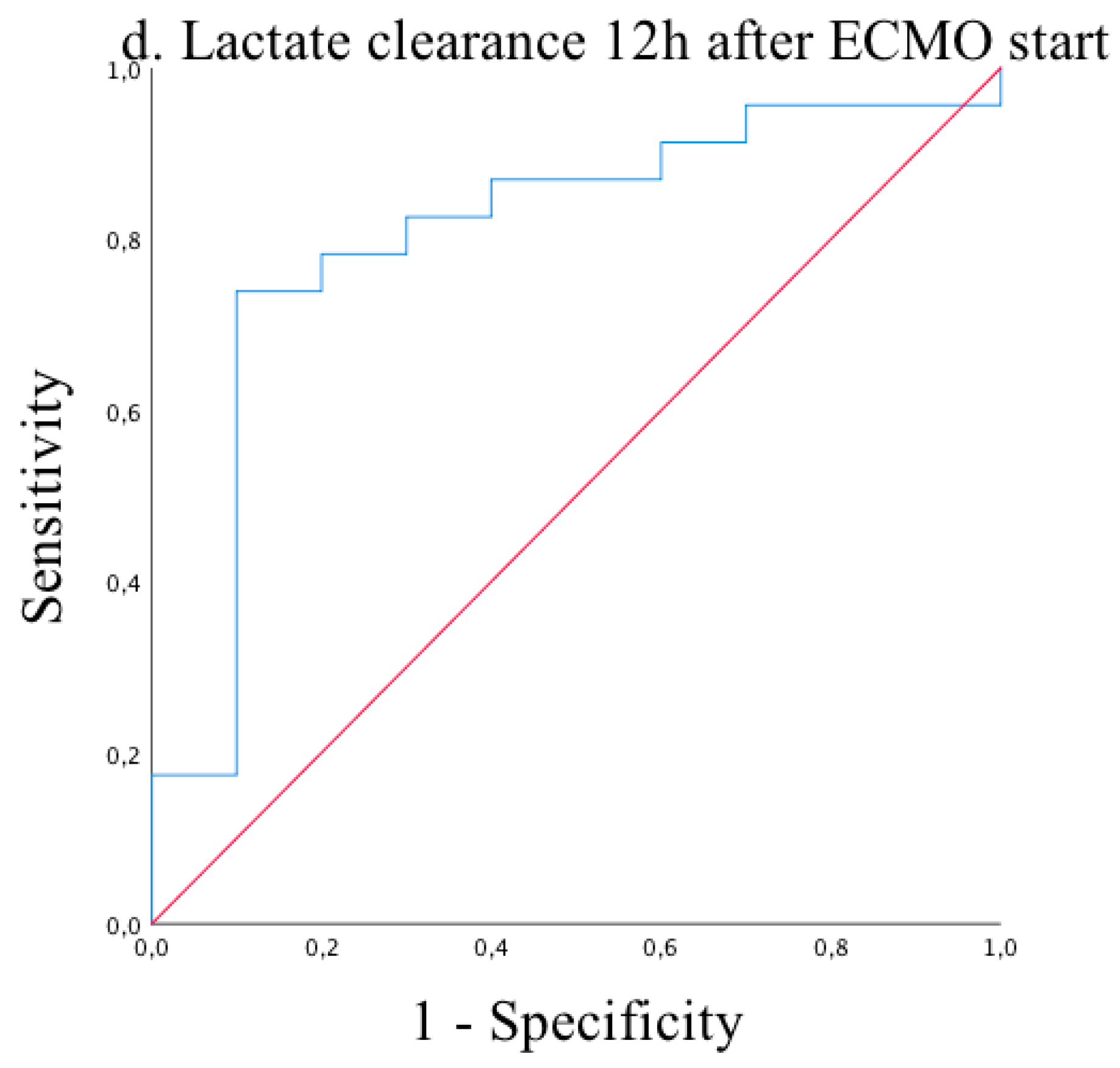
| 12 h after ECMO start | 4.1 ± 3.1 | 2.9 ± 1.5 | 4.3 ± 2.2 | 0.022 |
| ECMO duration (d) | 4(2;6) | 4(3;7) | 1.5(1;3.7) | 0.01 |
| Duration of mechanical ventilation (h) | 205(78;545) | 354(195;665) | 55(32;123) | <0.001 |
| eCPR | 16(39%) | 8(29.6%) | 8(57.1%) | 0.10 |
| pre-ECMO | 1st Day | 2nd Day | 3rd Day | |
|---|---|---|---|---|
| Creatine kinase | 0.72 | 0.25 | 0.004 | 0.001 |
| Creatine kinase MB | 0.71 | 0.01 | 0.001 | <0.001 |
| hsTnT | 0.61 | 0.007 | 0.001 | 0.002 |
| INR | 0.80 | 0.63 | 0.48 | 0.98 |
| AST (GOT) | 0.35 | 0.17 | 0.004 | 0.002 |
| ALT (GPT) | 0.49 | 0.46 | 0.057 | 0.068 |
| Bilirubine | 0.069 | 0.63 | 0.33 | 0.45 |
| Creatinine | 0.38 | 0.055 | 0.007 | 0.002 |
| Creatinine | 0.38 | 0.055 | 0.007 | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merkle-Storms, J.; Djordjevic, I.; Weber, C.; Avgeridou, S.; Krasivskyi, I.; Gaisendrees, C.; Mader, N.; Kuhn-Régnier, F.; Kröner, A.; Bennink, G.; et al. Impact of Lactate Clearance on Early Outcomes in Pediatric ECMO Patients. Medicina 2021, 57, 284. https://doi.org/10.3390/medicina57030284
Merkle-Storms J, Djordjevic I, Weber C, Avgeridou S, Krasivskyi I, Gaisendrees C, Mader N, Kuhn-Régnier F, Kröner A, Bennink G, et al. Impact of Lactate Clearance on Early Outcomes in Pediatric ECMO Patients. Medicina. 2021; 57(3):284. https://doi.org/10.3390/medicina57030284
Chicago/Turabian StyleMerkle-Storms, Julia, Ilija Djordjevic, Carolyn Weber, Soi Avgeridou, Ihor Krasivskyi, Christopher Gaisendrees, Navid Mader, Ferdinand Kuhn-Régnier, Axel Kröner, Gerardus Bennink, and et al. 2021. "Impact of Lactate Clearance on Early Outcomes in Pediatric ECMO Patients" Medicina 57, no. 3: 284. https://doi.org/10.3390/medicina57030284
APA StyleMerkle-Storms, J., Djordjevic, I., Weber, C., Avgeridou, S., Krasivskyi, I., Gaisendrees, C., Mader, N., Kuhn-Régnier, F., Kröner, A., Bennink, G., Sabashnikov, A., Trieschmann, U., Wahlers, T., & Menzel, C. (2021). Impact of Lactate Clearance on Early Outcomes in Pediatric ECMO Patients. Medicina, 57(3), 284. https://doi.org/10.3390/medicina57030284