
Treatment Outcomes of Langerhans Cell Histiocytosis: A Retrospective Study

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fletcher, C.D.; Lazar, A.J. WHO classification of tumors of soft tissue and bone. In Soft Tissue and Bone Tumours, 5th ed.; IARC Publications: Lyon, France, 2020; pp. 492–494. [Google Scholar]
- Krooks, J.; Minkov, M.; Weatherall, A.G. Langerhans cell histiocytosis in children: History, classification, pathobiology, clinical manifestations, and prognosis. J. Am. Acad. Dermatol. 2018, 78, 1035–1044. [Google Scholar] [CrossRef] [PubMed]
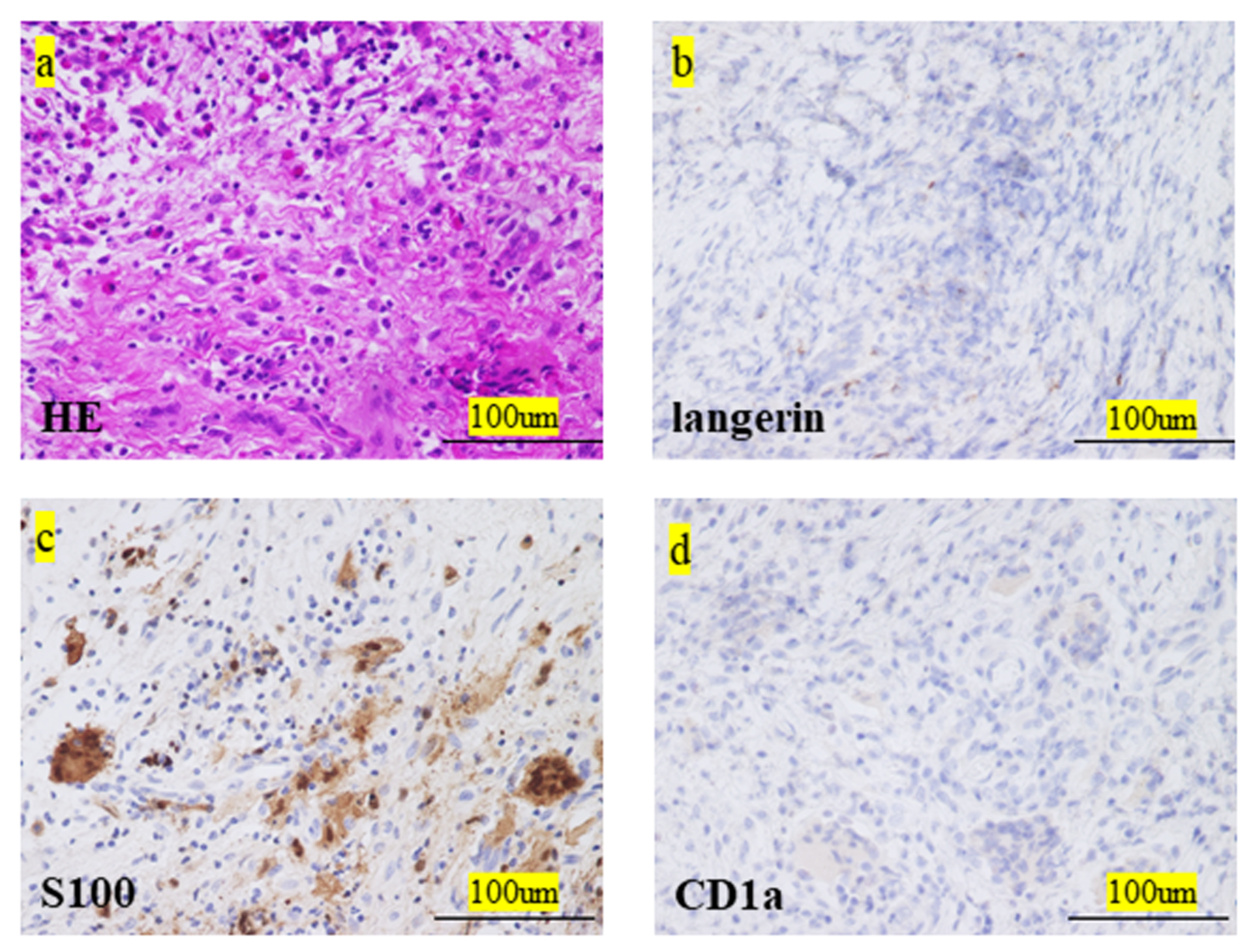
- Kim, H.K.; Park, C.J.; Jang, S.; Cho, Y.U.; Park, S.H.; Koh, K.N.; Im, H.J.; Seo, J.J. Bone marrow involvement of Langerhans cell histiocytosis: Immunohistochemical evaluation of bone marrow for CD1a, langerin, and S100 expression. Histopathology 2014, 65, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Islinger, R.B.; Kuklo, T.R.; Owens, B.D.; Horan, P.J.; Choma, T.J.; Murphey, M.D.; Temple, H. Langerhans’ cell histiocytosis in patients older than 21 years. Clin. Orthop. Relat. Res. 2000, 379, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Ando, S.; Kawamata, T.; Makiyama, J.; Yokoyama, K.; Imai, Y.; Tojo, A. Clinical features and outcomes of adult Langerhans cell histiocytosis: A single-center experience. Int. J. Hematol. 2020, 112, 185–192. [Google Scholar] [CrossRef]
- Minkov, M. Multisystem Langerhans cell histiocytosis in children: Current treatment and future directions. Pediatr. Drugs 2011, 13, 75–86. [Google Scholar] [CrossRef]
- Radzikowska, E. Pulmonary Langerhans’ cell histiocytosis in adults. Adv. Respir. Med. 2017, 85, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Kilpatrick, S.E.; Wenger, D.E.; Gilchrist, G.S.; Shives, T.C.; Wollan, P.C.; Unni, K.K. Langerhans’ cell histiocytosis (histiocytosis X) of bone. A clinicopathologic analysis of 263 pediatric and adult cases. Cancer 1995, 76, 2471–2484. [Google Scholar] [CrossRef]
- Howarth, D.M.; Gilchrist, G.S.; Mullan, B.P.; Wiseman, G.A.; Edmonson, J.H.; Schomberg, P.J. Langerhans cell histiocytosis: Diagnosis, natural history, management, and outcome. Cancer 1999, 85, 2278–2290. [Google Scholar] [CrossRef]
- Kim, B.E.; Koh, K.N.; Suh, J.K.; Im, H.J.; Song, J.S.; Lee, J.W.; Kang, H.J.; Park, K.D.; Shin, H.Y.; Choi, H.S.; et al. Korea Histiocytosis Working Party. Clinical features and treatment outcomes of Langerhans cell histiocytosis: A nationwide survey from Korea Histiocytosis Working Party. J. Pediatr. Hematol. Oncol. 2014, 36, 125–133. [Google Scholar] [CrossRef]
- Weitzman, S.; Egeler, R.M. Langerhans cell histiocytosis: Update for the pediatrician. Curr. Opin. Pediatr. 2008, 20, 23–29. [Google Scholar] [CrossRef]
- Van Nieuwenhuyse, J.P.; Clapuyt, P.; Malghem, J.; Everarts, P.; Melin, J.; Pauwels, S.; Brichard, B.; Ninane, J.; Vermylen, C.; Cornu, G. Radiographic skeletal survey and radionuclide bone scan in Langerhans cell histiocytosis of bone. Pediatr. Radiol. 1996, 26, 734–738. [Google Scholar] [CrossRef]
- Azouz, E.M.; Saigal, G.; Rodriguez, M.M.; Podda, A. Langerhans’ cell histiocytosis: Pathology, imaging and treatment of skeletal involvement. Pediatr. Radiol. 2005, 35, 103–115. [Google Scholar] [CrossRef] [PubMed]
- Haupt, R.; Minkov, M.; Astigarraga, I.; Schäfer, E.; Nanduri, V.; Jubran, R.; Egeler, R.M.; Janka, G.; Micic, D.; Rodriguez-Galindo, C.; et al. Langerhans cell histiocytosis (LCH): Guidelines for diagnosis, clinical work-up, and treatment for patients till the age of 18 years. Pediatr. Blood Cancer 2013, 60, 175–184. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.R.; Yoon, H.M.; Jung, A.Y.; Cho, Y.A.; Seo, J.J.; Lee, J.S. Comparison of whole-body MRI, bone scan, and radiographic skeletal survey for lesion detection and risk stratification of Langerhans cell histiocytosis. Sci. Rep. 2019, 9, 317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, M.; Allen, C.; Gerson, P.; McClain, K. Comparison of FDG-PET scans to conventional radiography and bone scans in management of Langerhans cell histiocytosis. Pediatr. Blood Cancer 2009, 52, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Binkovitz, L.A.; Olshefski, R.S.; Adler, B.H. Coincidence FDG-PET in the evaluation of Langerhans’ cell histiocytosis: Preliminary findings. Pediatr. Radiol. 2003, 33, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Kaste, S.C.; Rodriguez-Galindo, C.; McCarville, M.E.; Shulkin, B.L. PET-CT in pediatric Langerhans cell histiocytosis. Pediatr. Radiol. 2007, 37, 615–622. [Google Scholar] [CrossRef]
- Khung, S.; Budzik, J.F.; Amzallag-Bellenger, E.; Lambilliote, A.; Soto Ares, G.; Cotten, A.; Boutry, N. Skeletal involvement in Langerhans cell histiocytosis. Insights Imaging 2013, 4, 569–579. [Google Scholar] [CrossRef] [Green Version]
- Oh, B.; Lee, S.; Ke, Y.; Kimpo, M.; Yeoh, A.; Quah, T.C. A “wait-and-see” approach to quiescent single-system Langerhans cell histiocytosis to spare children from chemotherapy. Front. Pediatr. 2020, 8, 466. [Google Scholar] [CrossRef]
- Gadner, H.; Minkov, M.; Grois, N.; Pötschger, U.; Thiem, E.; Aricò, M.; Astigarraga, I.; Braier, J.; Donadieu, J.; Henter, J.I.; et al. Histiocyte Society. Therapy prolongation improves outcome in multi-system Langerhans cell histiocytosis. Blood 2013, 121, 5006–5014. [Google Scholar] [CrossRef]
- Morimoto, A.; Shimazaki, C.; Takahashi, S.; Yoshikawa, K.; Nishimura, R.; Wakita, H.; Kobayashi, Y.; Kanegane, H.; Tojo, A.; Imamura, T.; et al. Therapeutic outcome of multifocal Langerhans cell histiocytosis in adults treated with the Special C regimen formulated by the Japan LCH Study Group. Int. J. Hematol. 2013, 97, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Donadieu, J.; Bernard, F.; van Noesel, M.; Barkaoui, M.; Bardet, O.; Mura, R.; Arico, M.; Piguet, C.; Gandemer, V.; Armari Alla, C.; et al. Cladribine and cytarabine in refractory multi-system Langerhans cell histiocytosis: Results of an international phase 2 study. Blood 2015, 126, 1415–1423. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Patient No. | Age (Years) | Sex | Site | Imaging Tool for Diagnosis | Symptom | Comorbidity | Biopsy Site | Treatment | Outcome | Follow-Up Period (Months) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 24 | F | Rt tibia, left seventh rib | Radiography, scintigraphy, PET-CT | Pain and swelling | None | Tibia | Spontaneous regression | CDF | 13 |
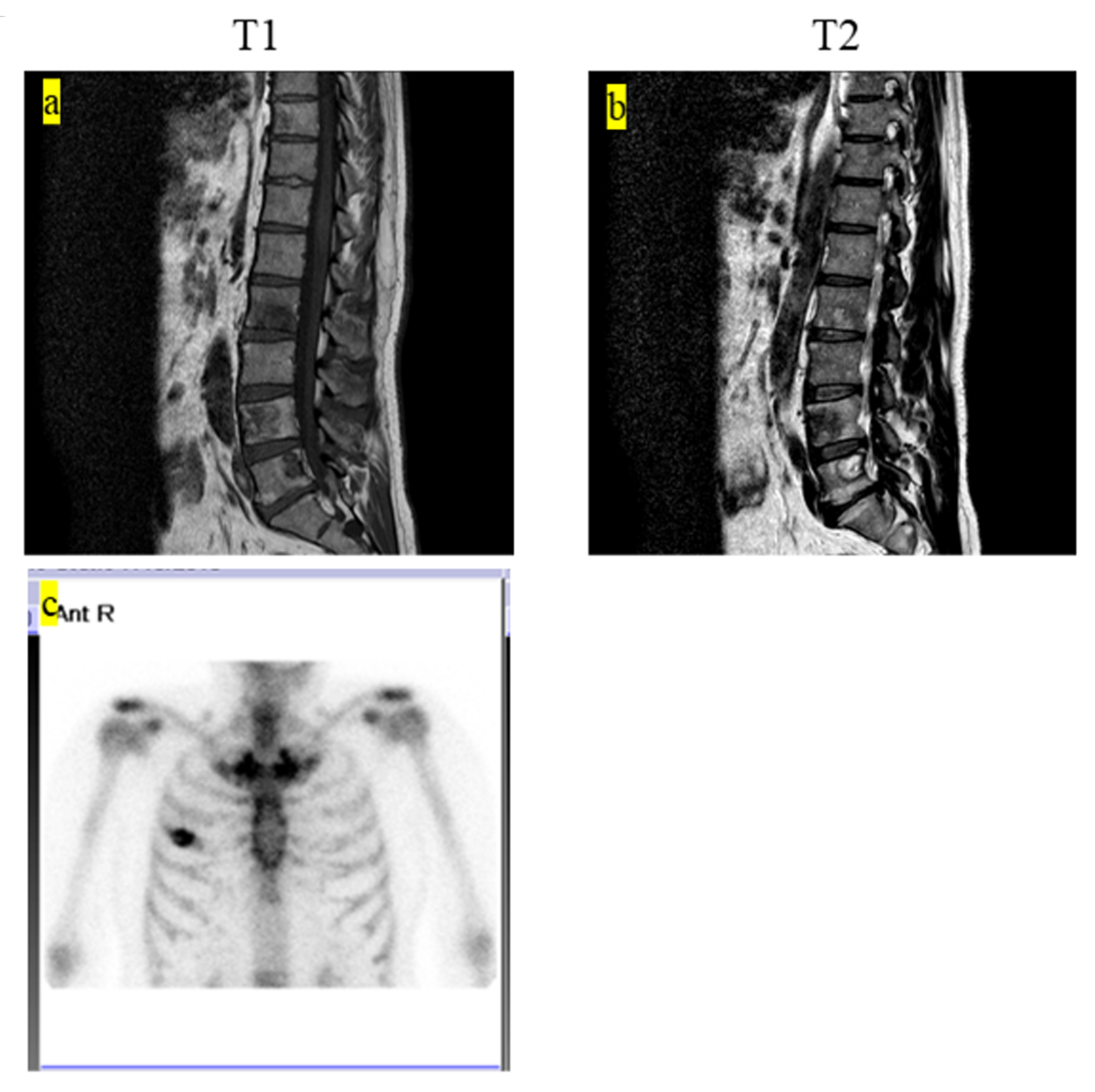
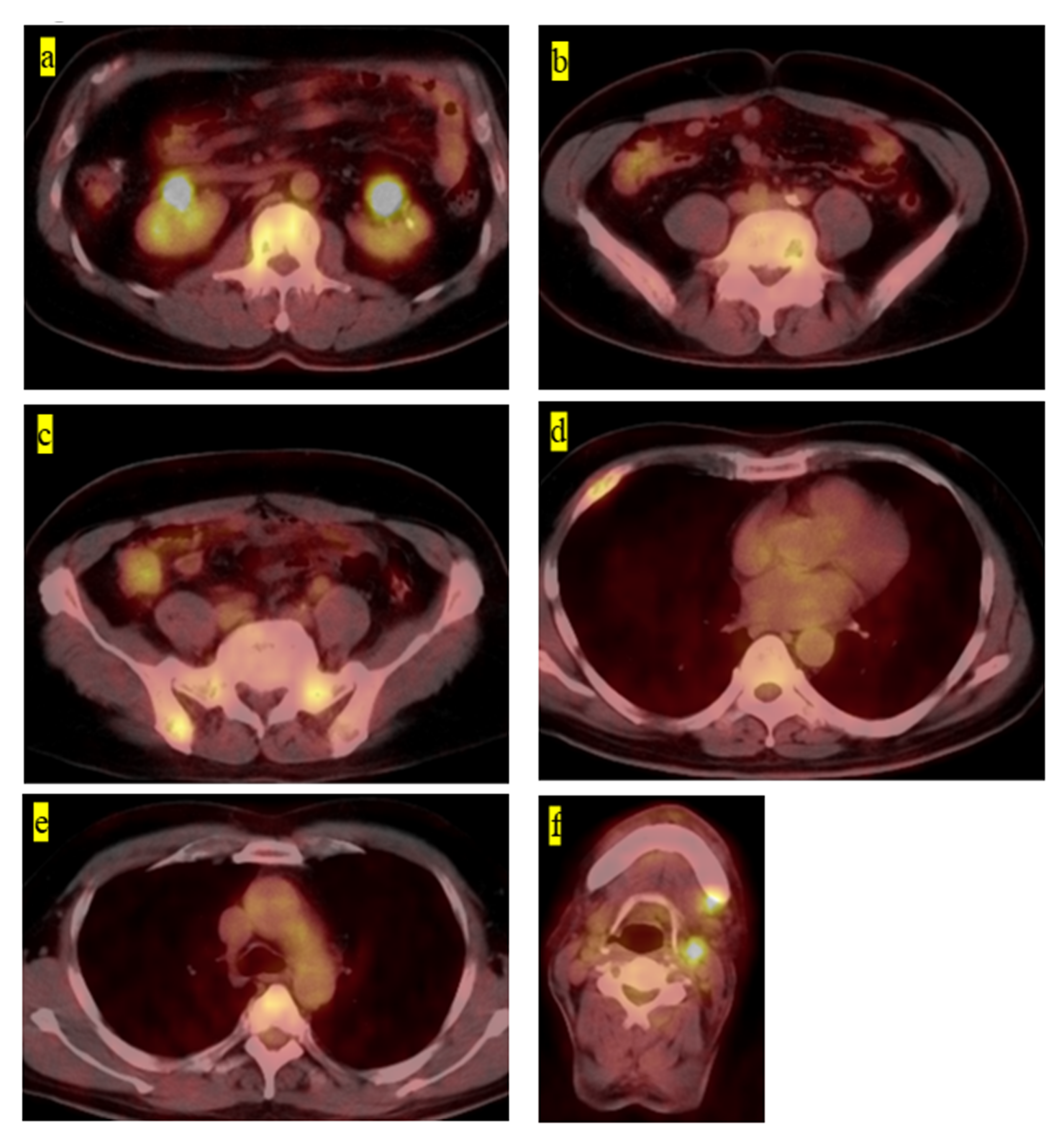
| 2 | 60 | M | Second, third, fourth, fifth lumbar, Th10, rt fourth rib, sacrum, pelvic | Radiography, MRI, PET-CT | Without symptoms | Hepatitis B | Fifth lumbar | Chemotherapy (6-mercaptopurine 110 mg, MTX 2.5 mg, PSL 5 mg) | CDF | 63 |
| 3 | 30 | F | Rt fourth rib | Radiography, scintigraphy, CT, MRI, contrast-enhanced MRI | Pain | None | Rt fourth rib | Natural observation | AWD | 4 |
| 4 | 2 | F | Femur, eighth thoracic vertebra | Radiography, MRI | Pain and claudication | None | Femur | Spontaneous regression | CDF | 27 |
| 5 | 2 | M | Femur, temporal bone, anterior mediastinum | Radiography, scintigraphy | Pain and claudication | Autism | Femur | Chemotherapy (cladribine 5 mg/m2 and cytarabine 500 mg/m2) | CDF | 55 |
| 6 | 3 | M | Elbow | Radiography, Scintigraphy | Pain | None | Radius | Spontaneous regression | CDF | 73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hashimoto, K.; Nishimura, S.; Sakata, N.; Inoue, M.; Sawada, A.; Akagi, M. Treatment Outcomes of Langerhans Cell Histiocytosis: A Retrospective Study. Medicina 2021, 57, 356. https://doi.org/10.3390/medicina57040356
Hashimoto K, Nishimura S, Sakata N, Inoue M, Sawada A, Akagi M. Treatment Outcomes of Langerhans Cell Histiocytosis: A Retrospective Study. Medicina. 2021; 57(4):356. https://doi.org/10.3390/medicina57040356
Chicago/Turabian StyleHashimoto, Kazuhiko, Shunji Nishimura, Naoki Sakata, Masami Inoue, Akihisa Sawada, and Masao Akagi. 2021. "Treatment Outcomes of Langerhans Cell Histiocytosis: A Retrospective Study" Medicina 57, no. 4: 356. https://doi.org/10.3390/medicina57040356
APA StyleHashimoto, K., Nishimura, S., Sakata, N., Inoue, M., Sawada, A., & Akagi, M. (2021). Treatment Outcomes of Langerhans Cell Histiocytosis: A Retrospective Study. Medicina, 57(4), 356. https://doi.org/10.3390/medicina57040356