
Harnessing Digital Health Technologies to Remotely Manage Diabetic Foot Syndrome: A Narrative Review



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
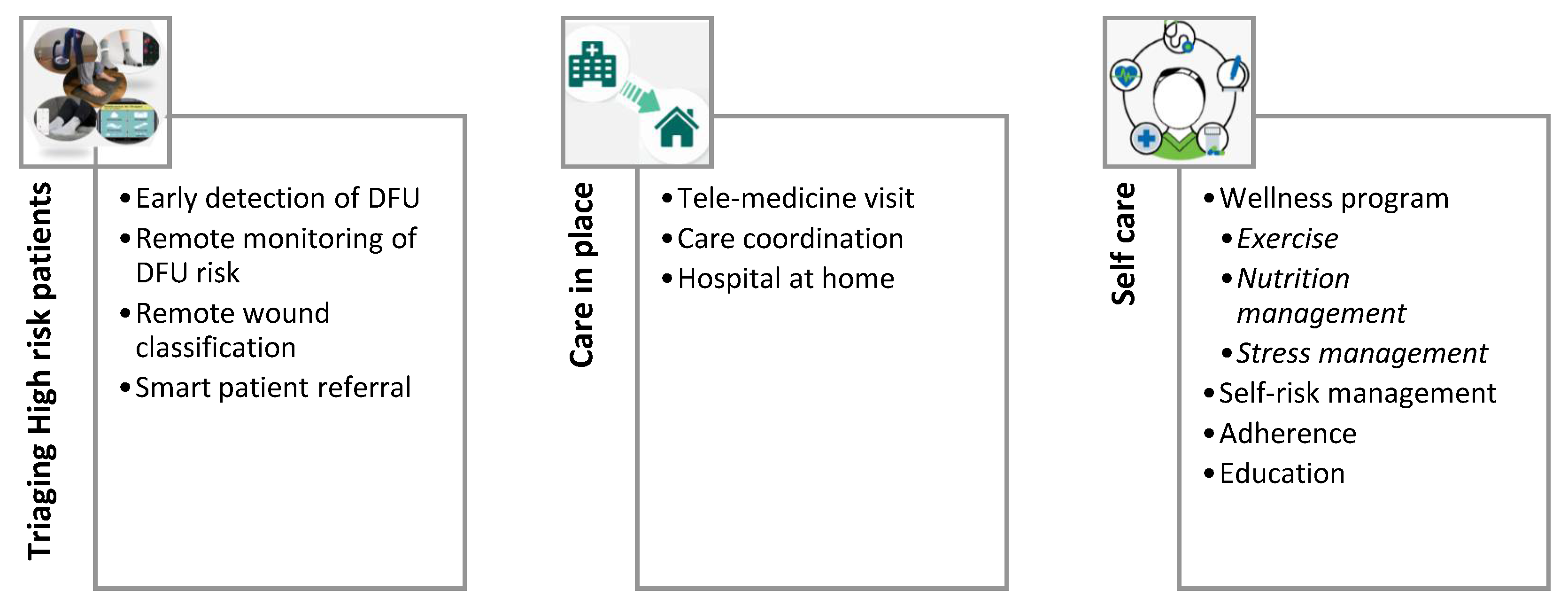
2. Triaging High-Risk Patients
2.1. Early Detection of DFU
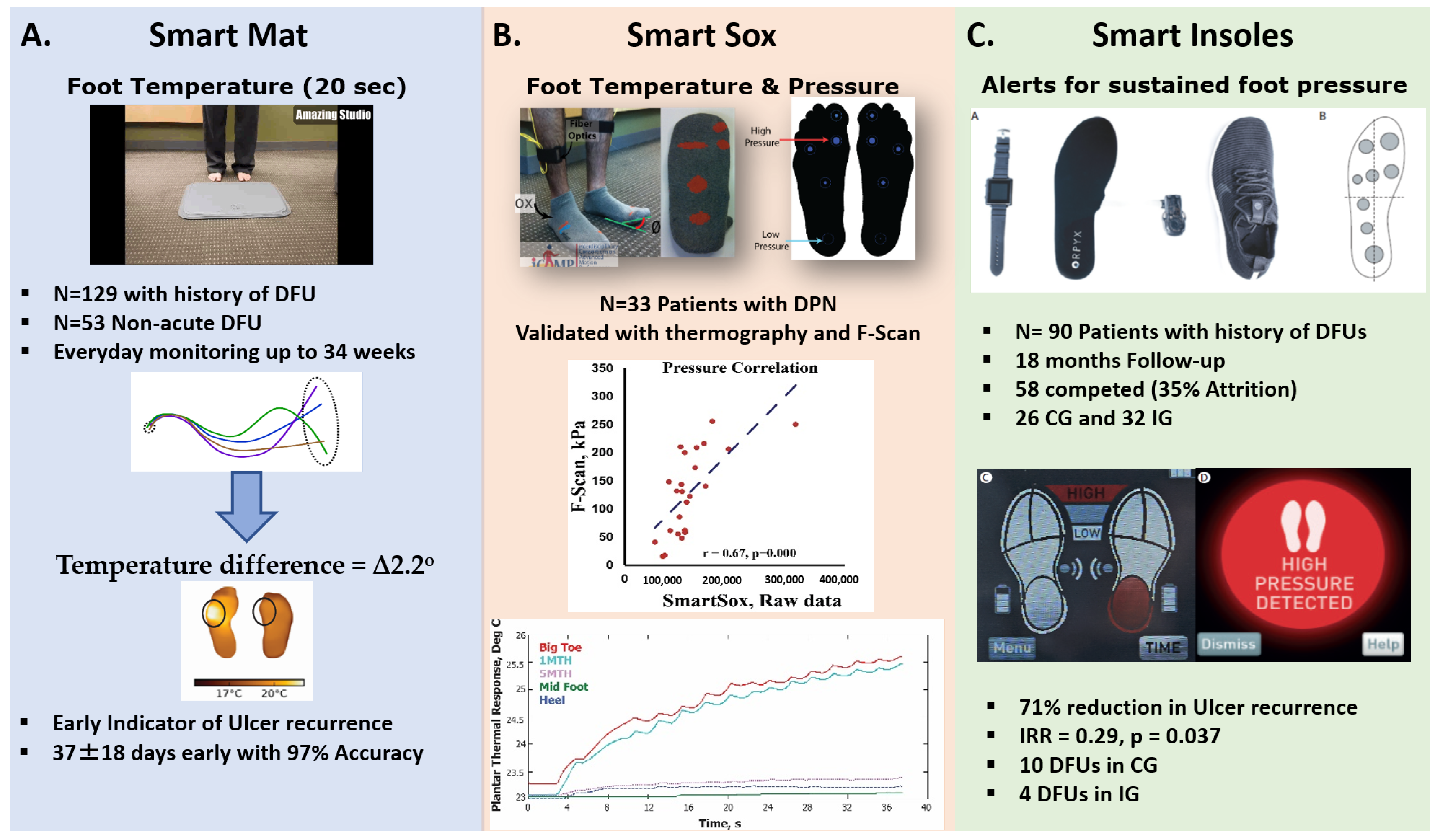
2.2. Remote Monitoring of DFU Risk
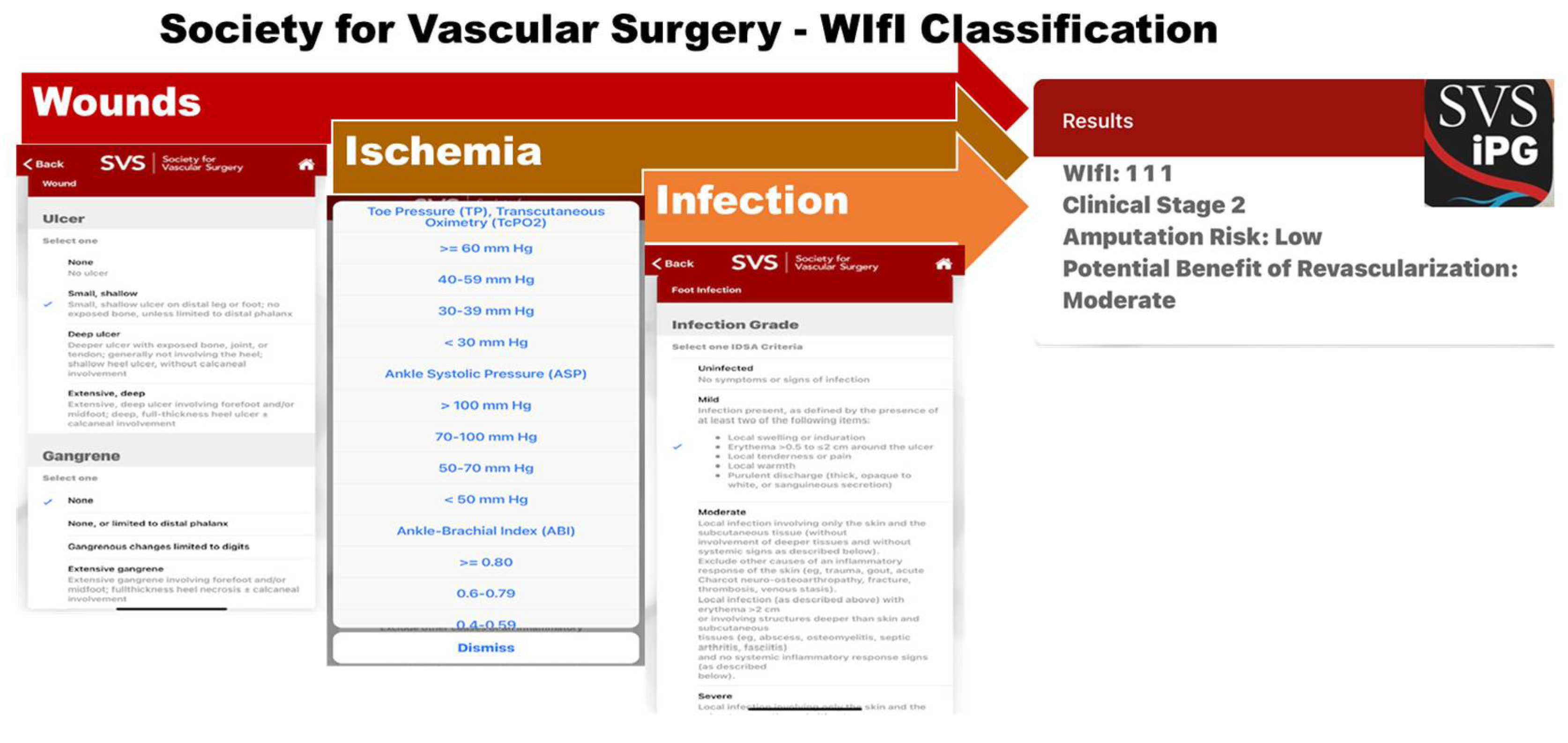
2.3. Remote Monitoring of Wound Characteristics
2.4. Smart Patient Referral
- The proposed binary classification Ensemble CNN method detected one class at a time, which cannot detect the co-occurrence of infection and ischemia;
- The dataset is small and cannot be generalized; and
- The recognition rate of infection is 73%, which requires substantial work to improve the accuracy. Despite these efforts on still in infancy, we anticipate that with advances in artificial intelligence (AI) and advanced analytical approaches, a more accurate computerized method would be emerged to smartly automate the DFU pathology recognition using mobile apps and by non-wound care specialists. Such development could facilitate smart triaging of patients with DFU who could benefit from hospital referral for revascularization or advanced wound care management.
3. Care in Place
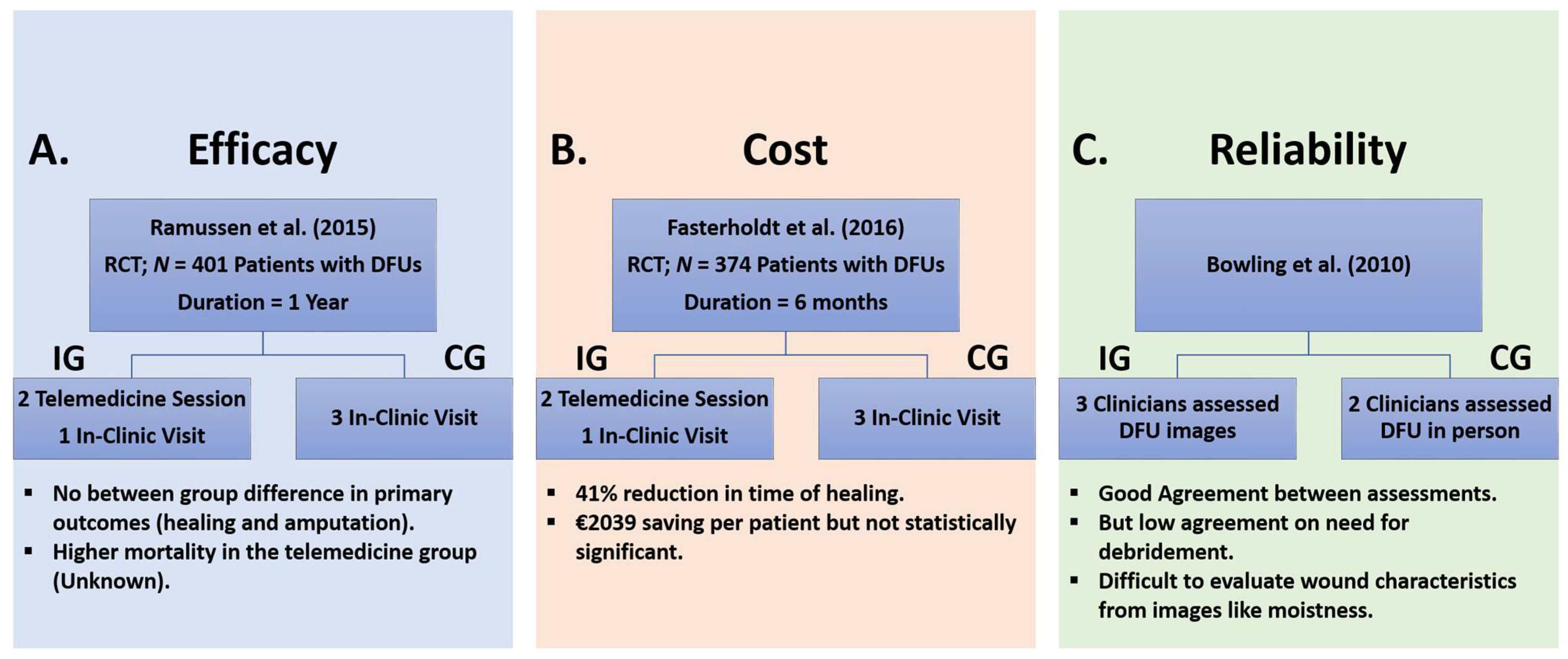
3.1. Telemedicine Visits
3.2. Care Coordination
3.3. Hospital at Home
4. Technologies to Empower Self-Care
4.1. Wellness Program
4.1.1. Exercise
4.1.2. Nutrition Management
4.1.3. Stress Management
4.2. Technologies to Promote Self-Risk Management
4.3. Technologies to Reinforce Adherence to Offloading
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barshes, N.R.; Sigireddi, M.; Wrobel, J.S.; Mahankali, A.; Robbins, J.M.; Kougias, P.; Armstrong, D.G. The system of care for the diabetic foot: Objectives, outcomes, and opportunities. Diabet. Foot Ankle 2013, 4, 21847. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lazzarini, P.A.; McPhail, S.M.; van Netten, J.J.; Armstrong, D.G.; Pacella, R.E. Global Disability Burdens of Diabetes-Related Lower-Extremity Complications in 1990 and 2016. Diabetes Care 2020, 43, 964–974. [Google Scholar] [CrossRef]
- Skrepnek, G.H.; Mills, J.L., Sr.; Armstrong, D.G. A Diabetic Emergency One Million Feet Long: Disparities and Burdens of Illness among Diabetic Foot Ulcer Cases within Emergency Departments in the United States, 2006–2010. PLoS ONE 2015, 10, e0134914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collaboration, N.R.F. Worldwide trends in diabetes since 1980: A pooled analysis of 751 population-based studies with 4.4 million participants. Lancet 2016, 387, 1513–1530. [Google Scholar] [CrossRef] [Green Version]
- Allen, L.; Powell-Cope, G.; Mbah, A.; Bulat, T.; Njoh, E. A Retrospective Review of Adverse Events Related to Diabetic Foot Ulcers. Ostomy Wound Manag. 2017, 63, 30–33. [Google Scholar]
- Najafi, B.; Grewal, G.S.; Bharara, M.; Menzies, R.; Talal, T.K.; Armstrong, D.G. Can’t Stand the Pressure: The Association Between Unprotected Standing, Walking, and Wound Healing in People with Diabetes. J. Diabetes Sci. Technol. 2017, 11, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Toosizadeh, N.; Mohler, J.; Lei, H.; Parvaneh, S.; Sherman, S.; Najafi, B. Motor Performance Assessment in Parkinson’s Disease: Association between Objective In-Clinic, Objective In-Home, and Subjective/Semi-Objective Measures. PLoS ONE 2015, 10, e0124763. [Google Scholar] [CrossRef] [Green Version]
- Lavery, L.A.; Hunt, N.A.; Ndip, A.; Lavery, D.C.; Van Houtum, W.; Boulton, A.J. Impact of chronic kidney disease on survival after amputation in individuals with diabetes. Diabetes Care 2010, 33, 2365–2369. [Google Scholar] [CrossRef] [Green Version]
- Rogers, L.C.; Andros, G.; Caporusso, J.; Harkless, L.B.; Mills, J.L., Sr.; Armstrong, D.G. Toe and flow: Essential components and structure of the amputation prevention team. J. Vasc. Surg. 2010, 52, 23S–27S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golledge, J.; Fernando, M.; Lazzarini, P.; Najafi, B.; G Armstrong, D. The Potential Role of Sensors, Wearables and Telehealth in the Remote Management of Diabetes-Related Foot Disease. Sensors 2020, 20, 4527. [Google Scholar] [CrossRef] [PubMed]
- van Netten, J.J.; Raspovic, A.; Lavery, L.A.; Monteiro-Soares, M.; Rasmussen, A.; Sacco, I.C.N.; Bus, S.A. Prevention of foot ulcers in the at-risk patient with diabetes: A systematic review. Diabetes Metab. Res. Rev. 2020, 36 (Suppl. 1), e3270. [Google Scholar] [CrossRef] [Green Version]
- Lazzarini, P.A.; Crews, R.T.; van Netten, J.J.; Bus, S.A.; Fernando, M.E.; Chadwick, P.J.; Najafi, B. Measuring Plantar Tissue Stress in People with Diabetic Peripheral Neuropathy: A Critical Concept in Diabetic Foot Management. J. Diabetes Sci. Technol. 2019, 13, 869–880. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Reeves, N.D.; Armstrong, D.G. Leveraging smart technologies to improve the management of diabetic foot ulcers and extend ulcer-free days in remission. Diabetes Metab. Res. Rev. 2020, 36 (Suppl. 1), e3239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, D.G.; Boulton, A.J.M.; Bus, S.A. Diabetic Foot Ulcers and Their Recurrence. N. Engl. J. Med. 2017, 376, 2367–2375. [Google Scholar] [CrossRef]
- Gordon, I.L.; Rothenberg, G.M.; Lepow, B.D.; Petersen, B.J.; Linders, D.R.; Bloom, J.D.; Armstrong, D.G. Accuracy of a foot temperature monitoring mat for predicting diabetic foot ulcers in patients with recent wounds or partial foot amputation. Diabetes Res. Clin. Pract. 2020, 161, 108074. [Google Scholar] [CrossRef] [Green Version]
- Najafi, R.G.; Gordon, I.L.; Reyzelman, A.M.; Cazzell, S.M.; Fitzgerald, R.H.; Rothenberg, G.M.; Bloom, J.D.; Petersen, B.J.; Linders, D.R.; Nouvong, A.; et al. Feasibility and Efficacy of a Smart Mat Technology to Predict Development of Diabetic Plantar Ulcers. Diabetes Care 2017, 40, 973–980. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, D.G.; Lavery, L.A. Predicting neuropathic ulceration with infrared dermal thermometry. J. Am. Podiatr. Med. Assoc. 1997, 87, 336–337. [Google Scholar] [CrossRef]
- Lavery, L.A.; Petersen, B.J.; Linders, D.R.; Bloom, J.D.; Rothenberg, G.M.; Armstrong, D.G. Unilateral remote temperature monitoring to predict future ulceration for the diabetic foot in remission. BMJ Open Diabetes Res. Care 2019, 7, e000696. [Google Scholar] [CrossRef] [Green Version]
- Isaac, A.L.; Swartz, T.D.; Miller, M.L.; Short, D.J.; Wilson, E.A.; Chaffo, J.L.; Watson, E.S.; Hu, H.; Petersen, B.J.; Bloom, J.D. Lower resource utilization for patients with healed diabetic foot ulcers during participation in a prevention program with foot temperature monitoring. BMJ Open Diabetes Res. Care 2020, 8, e001440. [Google Scholar] [CrossRef] [PubMed]
- Bus, S.; Van Netten, S.; Lavery, L.; Monteiro-Soares, M.; Rasmussen, A.; Jubiz, Y.; Price, P. IWGDF guidance on the prevention of foot ulcers in at-risk patients with diabetes. Diabetes Metab. Res. Rev. 2016, 32, 16–24. [Google Scholar] [CrossRef] [Green Version]
- Frykberg, R.G.; Zgonis, T.; Armstrong, D.G.; Driver, V.R.; Giurini, J.M.; Kravitz, S.R.; Landsman, A.S.; Lavery, L.A.; Moore, J.C.; Schuberth, J.M. Diabetic foot disorders: A clinical practice guideline (2006 revision). J. Foot Ankle Surg. 2006, 45, S1–S66. [Google Scholar] [CrossRef]
- Lavery, L.A.; Davis, K.E.; Berriman, S.J.; Braun, L.; Nichols, A.; Kim, P.J.; Margolis, D.; Peters, E.J.; Attinger, C. WHS guidelines update: Diabetic foot ulcer treatment guidelines. Wound Repair Regen. Off. Publ. Wound Heal. Soc. Eur. Tissue Repair Soc. 2016, 24, 112–126. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.G.; Holtz-Neiderer, K.; Wendel, C.; Mohler, M.J.; Kimbriel, H.R.; Lavery, L.A. Skin temperature monitoring reduces the risk for diabetic foot ulceration in high-risk patients. Am. J. Med. 2007, 120, 1042–1046. [Google Scholar] [CrossRef]
- Lavery, L.A.; Higgins, K.R.; Lanctot, D.R.; Constantinides, G.P.; Zamorano, R.G.; Armstrong, D.G.; Athanasiou, K.A.; Agrawal, C.M. Home monitoring of foot skin temperatures to prevent ulceration. Diabetes Care 2004, 27, 2642–2647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavery, L.A.; Higgins, K.R.; Lanctot, D.R.; Constantinides, G.P.; Zamorano, R.G.; Athanasiou, K.A.; Armstrong, D.G.; Agrawal, C.M. Preventing diabetic foot ulcer recurrence in high-risk patients: Use of temperature monitoring as a self-assessment tool. Diabetes Care 2007, 30, 14–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skafjeld, A.; Iversen, M.M.; Holme, I.; Ribu, L.; Hvaal, K.; Kilhovd, B.K. A pilot study testing the feasibility of skin temperature monitoring to reduce recurrent foot ulcers in patients with diabetes–a randomized controlled trial. BMC Endocr. Disord. 2015, 15, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Mohseni, H.; Grewal, G.S.; Talal, T.K.; Menzies, R.A.; Armstrong, D.G. An Optical-Fiber-Based Smart Textile (Smart Socks) to Manage Biomechanical Risk Factors Associated with Diabetic Foot Amputation. J. Diabetes Sci. Technol. 2017, 11, 668–677. [Google Scholar] [CrossRef] [Green Version]
- Najafi, B.; Swerdlow, M.; Murphy, G.A.; Armstrong, D.G. The Promise and Hurdles of Telemedicine in Diabetes Foot Care Delivery. In Telemedicine, Telehealth and Telepresence; Springer International Publishing: Cham, Switzerland, 2021; pp. 455–470. [Google Scholar]
- Wrobel, J.S.; Ammanath, P.; Le, T.; Luring, C.; Wensman, J.; Grewal, G.S.; Najafi, B.; Pop-Busui, R. A novel shear reduction insole effect on the thermal response to walking stress, balance, and gait. J. Diabetes Sci. Technol. 2014, 8, 1151–1156. [Google Scholar] [CrossRef] [Green Version]
- Rahemi, H.; Armstrong, D.G.; Enriquez, A.; Owl, J.; Talal, T.K.; Najafi, B. Lace Up for Healthy Feet: The Impact of Shoe Closure on Plantar Stress Response. J. Diabetes Sci. Technol. 2017, 11, 678–684. [Google Scholar] [CrossRef] [Green Version]
- Najafi, B.; Wrobel, J.S.; Grewal, G.; Menzies, R.A.; Talal, T.K.; Zirie, M.; Armstrong, D.G. Plantar Temperature Response to Walking in Diabetes with and without Acute Charcot: The Charcot Activity Response Test. J. Aging Res. 2012, 2012, 140968. [Google Scholar] [CrossRef] [Green Version]
- Reyzelman, A.M.; Koelewyn, K.; Murphy, M.; Shen, X.; Yu, E.; Pillai, R.; Fu, J.; Scholten, H.J.; Ma, R. Continuous temperature-monitoring socks for home use in patients with diabetes: Observational study. J. Med. Internet Res. 2018, 20, e12460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernando, M.E.; Crowther, R.G.; Pappas, E.; Lazzarini, P.A.; Cunningham, M.; Sangla, K.S.; Buttner, P.; Golledge, J. Plantar pressure in diabetic peripheral neuropathy patients with active foot ulceration, previous ulceration and no history of ulceration: A meta-analysis of observational studies. PLoS ONE 2014, 9, e99050. [Google Scholar] [CrossRef] [Green Version]
- Hessert, M.J.; Vyas, M.; Leach, J.; Hu, K.; Lipsitz, L.A.; Novak, V. Foot pressure distribution during walking in young and old adults. BMC Geriatr. 2005, 5, 8. [Google Scholar] [CrossRef] [Green Version]
- Miller, J.D.; Najafi, B.; Armstrong, D.G. Current Standards and Advances in Diabetic Ulcer Prevention and Elderly Fall Prevention Using Wearable Technology. Curr. Geriatr. Rep. 2015, 4, 249–256. [Google Scholar] [CrossRef]
- Shu, L.; Hua, T.; Wang, Y.; Li, Q.; Feng, D.D.; Tao, X. In-shoe plantar pressure measurement and analysis system based on fabric pressure sensing array. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 767–775. [Google Scholar] [CrossRef] [Green Version]
- Crea, S.; Donati, M.; De Rossi, S.M.M.; Maria Oddo, C.; Vitiello, N. A wireless flexible sensorized insole for gait analysis. Sensors 2014, 14, 1073–1093. [Google Scholar] [CrossRef] [Green Version]
- Abbott, C.A.; Chatwin, K.E.; Foden, P.; Hasan, A.N.; Sange, C.; Rajbhandari, S.M.; Reddy, P.N.; Vileikyte, L.; Bowling, F.L.; Boulton, A.J.M.; et al. Innovative intelligent insole system reduces diabetic foot ulcer recurrence at plantar sites: A prospective, randomised, proof-of-concept study. Lancet Digit. Health 2019, 1, e308–e318. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Pedersen, P.C.; Strong, D.M.; Tulu, B.; Agu, E.; Ignotz, R. Smartphone-based wound assessment system for patients with diabetes. IEEE Trans. Biomed. Eng. 2015, 62, 477–488. [Google Scholar] [CrossRef] [PubMed]
- Mammas, C.S.; Geropoulos, S.; Markou, G.; Saatsakis, G.; Lemonidou, C.; Tentolouris, N. Mobile Tele-Medicine Systems in the multidisciplinary approach of diabetes management: The remote prevention of diabetes complications. Stud. Health Technol. Inform. 2014, 202, 307–310. [Google Scholar] [PubMed]
- Van Netten, J.J.; Clark, D.; Lazzarini, P.A.; Janda, M.; Reed, L.F. The validity and reliability of remote diabetic foot ulcer assessment using mobile phone images. Sci. Rep. 2017, 7, 1–10. [Google Scholar] [CrossRef]
- Hayward, R.A.; Hofer, T.P.; Kerr, E.A.; Krein, S.L. Quality improvement initiatives: Issues in moving from diabetes guidelines to policy. Diabetes Care 2004, 27 (Suppl. 2), B54–B60. [Google Scholar] [CrossRef] [Green Version]
- Lavery, L.A.; Wunderlich, R.P.; Tredwell, J.L. Disease management for the diabetic foot: Effectiveness of a diabetic foot prevention program to reduce amputations and hospitalizations. Diabetes Res. Clin. Pract. 2005, 70, 31–37. [Google Scholar] [CrossRef]
- Mills, J.L., Sr.; Conte, M.S.; Armstrong, D.G.; Pomposelli, F.B.; Schanzer, A.; Sidawy, A.N.; Andros, G.; Society for Vascular Surgery Lower Extremity Guidelines Committee. The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: Risk stratification based on wound, ischemia, and foot infection (WIfI). J. Vasc. Surg. 2014, 59, 220–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prompers, L.; Huijberts, M.; Apelqvist, J.; Jude, E.; Piaggesi, A.; Bakker, K.; Edmonds, M.; Holstein, P.; Jirkovska, A.; Mauricio, D.; et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia 2007, 50, 18–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipsky, B.A.; Berendt, A.R.; Cornia, P.B.; Pile, J.C.; Peters, E.J.; Armstrong, D.G.; Deery, H.G.; Embil, J.M.; Joseph, W.S.; Karchmer, A.W.; et al. 2012 infectious diseases society of america clinical practice guideline for the diagnosis and treatment of diabetic foot infections. J. Am. Podiatr. Med. Assoc. 2013, 103, 2–7. [Google Scholar] [CrossRef]
- Skrepnek, G.H.; Mills, J.L., Sr.; Lavery, L.A.; Armstrong, D.G. Health Care Service and Outcomes Among an Estimated 6.7 Million Ambulatory Care Diabetic Foot Cases in the U.S. Diabetes Care 2017, 40, 936–942. [Google Scholar] [CrossRef] [Green Version]
- Zhan, L.X.; Branco, B.C.; Armstrong, D.G.; Mills, J.L., Sr. The Society for Vascular Surgery lower extremity threatened limb classification system based on Wound, Ischemia, and foot Infection (WIfI) correlates with risk of major amputation and time to wound healing. J. Vasc. Surg. 2015, 61, 939–944. [Google Scholar] [CrossRef] [Green Version]
- Goyal, M.; Reeves, N.D.; Rajbhandari, S.; Ahmad, N.; Wang, C.; Yap, M.H. Recognition of ischaemia and infection in diabetic foot ulcers: Dataset and techniques. Comput. Biol. Med. 2020, 117, 103616. [Google Scholar] [CrossRef]
- The Future of Home Health Care: Workshop Summary; National Academies Press: Washington, DC, USA, 2015.
- Leff, B.; Burton, L.; Mader, S.L.; Naughton, B.; Burl, J.; Inouye, S.K.; Greenough, W.B., 3rd; Guido, S.; Langston, C.; Frick, K.D.; et al. Hospital at home: Feasibility and outcomes of a program to provide hospital-level care at home for acutely ill older patients. Ann. Intern. Med. 2005, 143, 798–808. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B. Post the Pandemic: How will COVID-19 Transform Diabetic Foot Disease Management? J. Diabetes Sci. Technol. 2020, 14, 764–766. [Google Scholar] [CrossRef] [PubMed]
- Ivanova, D.; Wallenburg, I.; Bal, R. Care in place: A case study of assembling a carescape. Sociol. Health Illn. 2016, 38, 1336–1349. [Google Scholar] [CrossRef]
- Bus, S.A.; Lavery, L.A.; Monteiro-Soares, M.; Rasmussen, A.; Raspovic, A.; Sacco, I.C.N.; van Netten, J.J.; International Working Group on the Diabetic Foot. Guideline on the Prevention of Foot Ulcers in Persons with Diabetes. Diabetes/Metab. Res. Rev. 2020, 36, e3269. [Google Scholar]
- Tchero, H.; Noubou, L.; Becsangele, B.; Mukisi-Mukaza, M.; Retali, G.R.; Rusch, E. Telemedicine in Diabetic Foot Care: A Systematic Literature Review of Interventions and Meta-analysis of Controlled Trials. Int. J. Low. Extrem. Wounds 2017, 16, 274–283. [Google Scholar] [CrossRef]
- Najafi, B.; Swerdlow, M.; Murphy, G.A.; Armstrong, D.G. Digital foot care—Leveraging digital health to extend ulcer-free days in remission. In Diabetes Digital Health; Elsevier: Amsterdam, The Netherlands, 2020; pp. 179–194. [Google Scholar]
- Rasmussen, B.S.B.; Froekjaer, J.; Bjerregaard, M.R.; Lauritsen, J.; Hangaard, J.; Henriksen, C.W.; Halekoh, U.; Yderstraede, K.B. A randomized controlled trial comparing telemedical and standard outpatient monitoring of diabetic foot ulcers. Diabetes Care 2015, 38, 1723–1729. [Google Scholar] [CrossRef] [Green Version]
- Kobza, L.; Scheurich, A. The impact of telemedicine on outcomes of chronic wounds in the home care setting. Ostomy Wound Manag. 2000, 46, 48–53. [Google Scholar]
- Wilbright, W.A.; Birke, J.A.; Patout, C.A.; Varnado, M.; Horswell, R. The use of telemedicine in the management of diabetes-related foot ulceration: A pilot study. Adv. Skin Wound Care 2004, 17, 232–238. [Google Scholar] [CrossRef]
- Summerhayes, C.; Mcgee, J.A.; Cooper, R.J.; Ghauri, A.S.K.; Ranaboldo, C.J. Introducing leg ulcer telemedicine into rural general practice. Wounds UK 2012, 8, 28–36. [Google Scholar]
- Fasterholdt, I.; Gerstrøm, M.; Rasmussen, B.S.B.; Yderstræde, K.B.; Kidholm, K.; Pedersen, K.M. Cost-effectiveness of telemonitoring of diabetic foot ulcer patients. Health Inform. J. 2018, 24, 245–258. [Google Scholar] [CrossRef]
- Bowling, F.L.; King, L.; Paterson, J.A.; Hu, J.; Lipsky, B.A.; Matthews, D.R.; Boulton, A.J.M. Remote assessment of diabetic foot ulcers using a novel wound imaging system. Wound Repair Regen. 2011, 19, 25–30. [Google Scholar] [CrossRef]
- Farrow, M.J.; Hunter, I.S.; Connolly, P. Developing a real time sensing system to monitor bacteria in wound dressings. Biosensors 2012, 2, 171–188. [Google Scholar] [CrossRef] [PubMed]
- Mehmood, N.; Hariz, A.; Templeton, S.; Voelcker, N.H. A flexible and low power telemetric sensing and monitoring system for chronic wound diagnostics. Biomed. Eng. Online 2015, 14, 17. [Google Scholar] [CrossRef] [Green Version]
- Sharp, D. Printed composite electrodes for in-situ wound pH monitoring. Biosens. Bioelectron. 2013, 50, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Razjouyan, J.; Grewal, G.S.; Talal, T.K.; Armstrong, D.G.; Mills, J.L.; Najafi, B. Does Physiological Stress Slow Down Wound Healing in Patients with Diabetes? J. Diabetes Sci. Technol. 2017, 11, 685–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bettencourt-Silva, R.; Aguiar, B.; Sá-Araújo, V.; Barreira, R.; Guedes, V.; Marques Ribeiro, M.J.; Carvalho, D.; Östlundh, L.; Paulo, M.S. Diabetes-related symptoms, acute complications and management of diabetes mellitus of patients who are receiving palliative care: A protocol for a systematic review. BMJ Open 2019, 9, e028604. [Google Scholar] [CrossRef] [Green Version]
- Samal, L.; Dykes, P.C.; Greenberg, J.O.; Hasan, O.; Venkatesh, A.K.; Volk, L.A.; Bates, D.W. Care coordination gaps due to lack of interoperability in the United States: A qualitative study and literature review. BMC Health Serv. Res. 2016, 16, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maeng, D.D.; Martsolf, G.R.; Scanlon, D.P.; Christianson, J.B. Care coordination for the chronically ill: Understanding the patient’s perspective. Health Serv. Res. 2012, 47, 1960–1979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, S. Inpatient Care Coordination for Patients with Diabetes. Diabetes Spectr. 2008, 21, 272–275. [Google Scholar] [CrossRef] [Green Version]
- Weeks, D.L.; Polello, J.M.; Hansen, D.T.; Keeney, B.J.; Conrad, D.A. Measuring primary care organizational capacity for diabetes care coordination: The Diabetes Care Coordination Readiness Assessment. J. Gen. Intern. Med. 2014, 29, 98–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.C.; Cheng, S.H. Care Continuity and Care Coordination: A Preliminary Examination of Their Effects on Hospitalization. Med. Care Res. Rev. 2020, 1077558720903882. [Google Scholar] [CrossRef]
- Schultz, E.M.; Pineda, N.; Lonhart, J.; Davies, S.M.; McDonald, K.M. A systematic review of the care coordination measurement landscape. BMC Health Serv. Res. 2013, 13, 119. [Google Scholar] [CrossRef] [Green Version]
- Patel, V.; Reed, M.E.; Grant, R.W. Electronic health records and the evolution of diabetes care: A narrative review. J. Diabetes Sci. Technol. 2015, 9, 676–680. [Google Scholar] [CrossRef] [Green Version]
- Reed, M.; Huang, J.; Graetz, I.; Brand, R.; Hsu, J.; Fireman, B.; Jaffe, M. Outpatient electronic health records and the clinical care and outcomes of patients with diabetes mellitus. Ann. Intern. Med. 2012, 157, 482–489. [Google Scholar] [CrossRef]
- Reed, M.; Huang, J.; Brand, R.; Graetz, I.; Neugebauer, R.; Fireman, B.; Jaffe, M.; Ballard, D.W.; Hsu, J. Implementation of an outpatient electronic health record and emergency department visits, hospitalizations, and office visits among patients with diabetes. JAMA 2013, 310, 1060–1065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charles, D.; Gabriel, M.; Furukawa, M.F. Adoption of electronic health record systems among US non-federal acute care hospitals: 2008–2012. ONC Data Brief 2013, 9, 1–9. [Google Scholar]
- Richesson, R.L. Data standards in diabetes patient registries. J. Diabetes Sci. Technol. 2011, 5, 476–485. [Google Scholar] [CrossRef] [Green Version]
- Grant, R.W.; Cagliero, E.; Sullivan, C.M.; Dubey, A.K.; Estey, G.A.; Weil, E.M.; Gesmundo, J.; Nathan, D.M.; Singer, D.E.; Chueh, H.C.; et al. A controlled trial of population management: Diabetes mellitus: Putting evidence into practice (DM-PEP). Diabetes Care 2004, 27, 2299–2305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, H.H.; Eisert, S.L.; Durfee, M.J.; Moore, S.L.; Steele, A.W.; McCullen, K.; Anderson, K.; Penny, L.; Mackenzie, T.D. The impact of tailored diabetes registry report cards on measures of disease control: A nested randomized trial. BMC Med. Inform. Decis. Mak. 2011, 11, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joret, M.O.; Osman, K.; Dean, A.; Cao, C.; van der Werf, B.; Bhamidipaty, V. Multidisciplinary clinics reduce treatment costs and improve patient outcomes in diabetic foot disease. J. Vasc. Surg. 2019, 70, 806–814. [Google Scholar] [CrossRef]
- Coughlin, S.S.; Williams, L.B.; Hatzigeorgiou, C. A systematic review of studies of web portals for patients with diabetes mellitus. Mhealth 2017, 3, 23. [Google Scholar] [CrossRef] [Green Version]
- Ralston, J.D.; Hirsch, I.B.; Hoath, J.; Mullen, M.; Cheadle, A.; Goldberg, H.I. Web-based collaborative care for type 2 diabetes: A pilot randomized trial. Diabetes Care 2009, 32, 234–239. [Google Scholar] [CrossRef] [Green Version]
- Irizarry, T.; Dabbs, A.D.; Curran, C.R. Patient portals and patient engagement: A state of the science review. J. Med. Internet Res. 2015, 17, e148. [Google Scholar] [CrossRef] [Green Version]
- Coughlin, S.S.; Prochaska, J.J.; Williams, L.B.; Besenyi, G.M.; Heboyan, V.; Goggans, D.S.; Yoo, W.; De Leo, G. Patient web portals, disease management, and primary prevention. Risk Manag. Healthc. Policy 2017, 10, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkar, U.; Karter, A.J.; Liu, J.Y.; Adler, N.E.; Nguyen, R.; Lopez, A.; Schillinger, D. The literacy divide: Health literacy and the use of an internet-based patient portal in an integrated health system—Results from the Diabetes Study of Northern California (DISTANCE). J. Health Commun. 2010, 15, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Dash, S.; Acharya, B.R.; Mittal, M.; Abraham, A.; Kelemen, A.G. Deep Learning Techniques for Biomedical and Health Informatics; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Makino, M.; Yoshimoto, R.; Ono, M.; Itoko, T.; Katsuki, T.; Koseki, A.; Kudo, M.; Haida, K.; Kuroda, J.; Yanagiya, R. Artificial intelligence predicts the progression of diabetic kidney disease using big data machine learning. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kagawa, R.; Kawazoe, Y.; Ida, Y.; Shinohara, E.; Tanaka, K.; Imai, T.; Ohe, K. Development of Type 2 Diabetes Mellitus Phenotyping Framework Using Expert Knowledge and Machine Learning Approach. J. Diabetes Sci. Technol. 2017, 11, 791–799. [Google Scholar] [CrossRef]
- Anderson, J.P.; Parikh, J.R.; Shenfeld, D.K.; Ivanov, V.; Marks, C.; Church, B.W.; Laramie, J.M.; Mardekian, J.; Piper, B.A.; Willke, R.J.; et al. Reverse Engineering and Evaluation of Prediction Models for Progression to Type 2 Diabetes: An Application of Machine Learning Using Electronic Health Records. J. Diabetes Sci. Technol. 2015, 10, 6–18. [Google Scholar] [CrossRef] [Green Version]
- Sudharsan, B.; Peeples, M.; Shomali, M. Hypoglycemia prediction using machine learning models for patients with type 2 diabetes. J. Diabetes Sci. Technol. 2015, 9, 86–90. [Google Scholar] [CrossRef]
- Wang, L.; Pedersen, P.C.; Strong, D.M.; Tulu, B.; Agu, E.; Ignotz, R.; He, Q. An automatic assessment system of diabetic foot ulcers based on wound area determination, color segmentation, and healing score evaluation. J. Diabetes Sci. Technol. 2016, 10, 421–428. [Google Scholar] [CrossRef]
- Davenport, T.H.; Hongsermeier, T.; Mc Cord, K.A. Using AI to improve electronic health records. Harv. Bus. Rev. 2018, 12, 1–6. [Google Scholar]
- Holbrook, A.; Thabane, L.; Keshavjee, K.; Dolovich, L.; Bernstein, B.; Chan, D.; Troyan, S.; Foster, G.; Gerstein, H. Individualized electronic decision support and reminders to improve diabetes care in the community: COMPETE II randomized trial. CMAJ 2009, 181, 37–44. [Google Scholar] [CrossRef] [Green Version]
- Williams, Y.; Johnson, K.; Jones, S. Increasing Healthcare Provider Compliance in Performing Foot Examinations in Diabetic Patients. Available online: https://search.proquest.com/openview/747b6c2148963033a1323c0148a08cc2/1?pq-origsite=gscholar&cbl=2034896 (accessed on 13 April 2021).
- Kumar, A.; Carmichael, K. Diabetic foot ulcers: Managing a common and costly complication. Consultant 2020, 60, 85–86. [Google Scholar] [CrossRef]
- Pocuis, J.; Li, S.M.-H.; Janci, M.M.; Thompson, H.J. Exploring diabetic foot exam performance in a specialty clinic. Clin. Nurs. Res. 2017, 26, 82–92. [Google Scholar] [CrossRef] [PubMed]
- Quach, T.V.; Goldschmidt, M.H. Evaluating a Program Process Change to Improve Completion of Foot Exams and Amputation Risk Assessments for Veterans with Diabetes. Fed. Pract. 2019, 36, S10–S15. [Google Scholar]
- Caplan, G.A.; Sulaiman, N.S.; Mangin, D.A.; Aimonino Ricauda, N.; Wilson, A.D.; Barclay, L. A meta—Analysis of “hospital in the home”. Med. J. Aust. 2012, 197, 512–519. [Google Scholar] [CrossRef]
- Federman, A.D.; Soones, T.; DeCherrie, L.V.; Leff, B.; Siu, A.L. Association of a bundled hospital-at-home and 30-day postacute transitional care program with clinical outcomes and patient experiences. JAMA Intern. Med. 2018, 178, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Council, N.R. Health Care Comes Home: The Human Factors; National Academies Press: Washington, DC, USA, 2011. [Google Scholar]
- Basatneh, R.; Najafi, B.; Armstrong, D.G. Health Sensors, Smart Home Devices, and the Internet of Medical Things: An Opportunity for Dramatic Improvement in Care for the Lower Extremity Complications of Diabetes. J. Diabetes Sci. Technol. 2018, 12, 577–586. [Google Scholar] [CrossRef]
- Binning, J.; Woodburn, J.; Bus, S.A.; Barn, R. Motivational interviewing to improve adherence behaviours for the prevention of diabetic foot ulceration. Diabetes Metab. Res. Rev. 2019, 35, e3105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Netten, J.J.; Woodburn, J.; Bus, S.A. The future of prevention of diabetic foot ulcer: A paradigm shift from stratified healthcare towards personalized medicine. Diabetes Metab. Res. Rev. 2020, 36, e3234. [Google Scholar] [CrossRef]
- Martos-Cabrera, M.B.; Membrive-Jiménez, M.J.; Suleiman-Martos, N.; Mota-Romero, E.; Gómez-Urquiza, J.L.; Albendín-García, L. Games and Health Education for Diabetes Control: A Systematic Review with Meta-Analysis. Healthcare 2020, 8, 399. [Google Scholar] [CrossRef]
- Olive, J.L.; DeVan, A.E.; McCully, K.K. The effects of aging and activity on muscle blood flow. Dyn. Med. 2002, 1, 1–7. [Google Scholar] [CrossRef]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical activity/exercise and diabetes: A position statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. National Diabetes Statistics Report; Centers for Disease Control and Prevention, US Department of Health and Human Services: Atlanta, GA, USA, 2020; pp. 12–15.
- Höchsmann, C.; Walz, S.P.; Schäfer, J.; Holopainen, J.; Hanssen, H.; Schmidt-Trucksäss, A. Mobile Exergaming for Health—Effects of a serious game application for smartphones on physical activity and exercise adherence in type 2 diabetes mellitus—study protocol for a randomized controlled trial. Trials 2017, 18, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Höchsmann, C.; Müller, O.; Ambühl, M.; Klenk, C.; Königstein, K.; Infanger, D.; Walz, S.P.; Schmidt-Trucksäss, A. Novel smartphone game improves physical activity behavior in type 2 diabetes. Am. J. Prev. Med. 2019, 57, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Kempf, K.; Martin, S. Autonomous exercise game use improves metabolic control and quality of life in type 2 diabetes patients-a randomized controlled trial. BMC Endocr. Disord. 2013, 13, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, H.; Al-Ali, F.; Kang, G.E.; Hamad, A.I.; Ibrahim, R.A.; Talal, T.K.; Najafi, B. Application of Wearables to Facilitate Virtually Supervised Intradialytic Exercise for Reducing Depression Symptoms. Sensors 2020, 20, 1571. [Google Scholar] [CrossRef] [Green Version]
- Iraj, B.; Khorvash, F.; Ebneshahidi, A.; Askari, G. Prevention of diabetic foot ulcer. Int. J. Prev. Med. 2013, 4, 373. [Google Scholar]
- Centers for Disease Control and Prevention. Centers for Disease Control and Prevention Diabetes Prevention Recognition Program. 2015. Available online: https://www.cdc.gov/diabetes/prevention/index.html (accessed on 13 April 2021).
- Grock, S.; Ku, J.-H.; Kim, J.; Moin, T. A review of technology-assisted interventions for diabetes prevention. Curr. Diabetes Rep. 2017, 17, 1–12. [Google Scholar] [CrossRef]
- Quinn, C.C.; Shardell, M.D.; Terrin, M.L.; Barr, E.A.; Ballew, S.H.; Gruber-Baldini, A.L. Cluster-randomized trial of a mobile phone personalized behavioral intervention for blood glucose control. Diabetes Care 2011, 34, 1934–1942. [Google Scholar] [CrossRef] [Green Version]
- Fischer, H.H.; Fischer, I.P.; Pereira, R.I.; Furniss, A.L.; Rozwadowski, J.M.; Moore, S.L.; Durfee, M.J.; Raghunath, S.G.; Tsai, A.G.; Havranek, E.P. Text message support for weight loss in patients with prediabetes: A randomized clinical trial. Diabetes Care 2016, 39, 1364–1370. [Google Scholar] [CrossRef] [Green Version]
- Lin, M.; Mahmooth, Z.; Dedhia, N.; Frutchey, R.; Mercado, C.E.; Epstein, D.H.; Preston, K.L.; Gibbons, M.C.; Bowie, J.V.; Labrique, A.B. Tailored, interactive text messages for enhancing weight loss among African American adults: The TRIMM randomized controlled trial. Am. J. Med. 2015, 128, 896–904. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, J.R.; Koro, T.; Doran, N.; Thompson, S.; Sallis, J.F.; Calfas, K.; Patrick, K. Text4Diet: A randomized controlled study using text messaging for weight loss behaviors. Prev. Med. 2012, 55, 412–417. [Google Scholar] [CrossRef]
- Michaelides, A.; Raby, C.; Wood, M.; Farr, K.; Toro-Ramos, T. Weight loss efficacy of a novel mobile Diabetes Prevention Program delivery platform with human coaching. BMJ Open Diabetes Res. Care 2016, 4, e000264. [Google Scholar] [CrossRef] [Green Version]
- Sepah, S.C.; Jiang, L.; Peters, A.L. Long-term outcomes of a Web-based diabetes prevention program: 2-year results of a single-arm longitudinal study. J. Med. Internet Res. 2015, 17, e92. [Google Scholar] [CrossRef]
- Castro Sweet, C.M.; Chiguluri, V.; Gumpina, R.; Abbott, P.; Madero, E.N.; Payne, M.; Happe, L.; Matanich, R.; Renda, A.; Prewitt, T. Outcomes of a digital health program with human coaching for diabetes risk reduction in a Medicare population. J. Aging Health 2018, 30, 692–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravana, S.D.; Rahman, S.A.; Chan, H. Web-based diet information system with case-based reasoning capabilities. Int. J. Web Inf. Syst. 2006. [Google Scholar] [CrossRef]
- Holt, R.I.; De Groot, M.; Golden, S.H. Diabetes and depression. Curr. Diabetes Rep. 2014, 14, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Katon, W.J.; Rutter, C.; Simon, G.; Lin, E.H.; Ludman, E.; Ciechanowski, P.; Kinder, L.; Young, B.; Von Korff, M. The association of comorbid depression with mortality in patients with type 2 diabetes. Diabetes Care 2005, 28, 2668–2672. [Google Scholar] [CrossRef] [Green Version]
- Bassi, G.; Gabrielli, S.; Donisi, V.; Carbone, S.; Forti, S.; Salcuni, S. Assessment of Psychological Distress in Adults With Type 2 Diabetes Mellitus Through Technologies: Literature Review. J. Med. Internet Res. 2021, 23, e17740. [Google Scholar] [CrossRef]
- Lin, E.H.B.; Katon, W.; Von Korff, M.; Rutter, C.; Simon, G.E.; Oliver, M.; Ciechanowski, P.; Ludman, E.J.; Bush, T.; Young, B. Relationship of depression and diabetes self-care, medication adherence, and preventive care. Diabetes Care 2004, 27, 2154–2160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.W.B.; Ho, R.C.M.; Loh, A.; Wing, T.; Wynne, O.; Chan, S.W.C.; Car, J.; Fung, D.S.S. Current status of postnatal depression smartphone applications available on application stores: An information quality analysis. BMJ Open 2017, 7, e015655. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.W.B.; Ho, C.S.H.; Cheok, C.C.S.; Ho, R.C.M. Smartphone apps in mental healthcare: The state of the art and potential developments. BJPsych Adv. 2015, 21, 354–358. [Google Scholar] [CrossRef] [Green Version]
- Dobson, R.; Carter, K.; Cutfield, R.; Hulme, A.; Hulme, R.; McNamara, C.; Maddison, R.; Murphy, R.; Shepherd, M.; Strydom, J.; et al. Diabetes text-message self-management support program (SMS4BG): A pilot study. JMIR mHealth uHealth 2015, 3, e32. [Google Scholar] [CrossRef] [Green Version]
- Holland-Carter, L.; Tuerk, P.W.; Wadden, T.A.; Fujioka, K.N.; Becker, L.E.; Miller-Kovach, K.; Hollander, P.L.; Garvey, W.T.; Weiss, D.; Rubino, D.M.; et al. Impact on psychosocial outcomes of a nationally available weight management program tailored for individuals with type 2 diabetes: Results of a randomized controlled trial. J. Diabetes Complicat. 2017, 31, 891–897. [Google Scholar] [CrossRef]
- Wayne, N.; Perez, D.F.; Kaplan, D.M.; Ritvo, P. Health coaching reduces hba1c in type 2 diabetic patients from a lower-socioeconomic status community: A randomized controlled trial. J. Med. Internet Res. 2015, 17, e224. [Google Scholar] [CrossRef]
- Hay, J.W.; Lee, P.J.; Jin, H.; Guterman, J.J.; Gross-Schulman, S.; Ell, K.; Wu, S. Cost-Effectiveness of a Technology-Facilitated Depression Care Management Adoption Model in Safety-Net Primary Care Patients with Type 2 Diabetes. Value Health 2018, 21, 561–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramirez, M.; Wu, S.; Jin, H.; Ell, K.; Gross-Schulman, S.; Myerchin Sklaroff, L.; Guterman, J. Automated Remote Monitoring of Depression: Acceptance Among Low-Income Patients in Diabetes Disease Management. JMIR Ment. Health 2016, 3, e6. [Google Scholar] [CrossRef]
- Vidyanti, I.; Wu, B.; Wu, S. Low-income minority patient engagement with automated telephonic depression assessment and impact on health outcomes. Qual. Life Res. 2015, 24, 1119–1129. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.; Ell, K.; Gross-Schulman, S.G.; Sklaroff, L.M.; Katon, W.J.; Nezu, A.M.; Lee, P.J.; Vidyanti, I.; Chou, C.P.; Guterman, J.J. Technology-facilitated depression care management among predominantly Latino diabetes patients within a public safety net care system: Comparative effectiveness trial design. Contemp. Clin. Trials 2014, 37, 342–354. [Google Scholar] [CrossRef]
- Parvaneh, S.; Grewal, G.S.; Grewal, E.; Menzies, R.A.; Talal, T.K.; Armstrong, D.G.; Sternberg, E.; Najafi, B. Stressing the dressing: Assessing stress during wound care in real-time using wearable sensors. Wound Med. 2014, 4, 21–26. [Google Scholar] [CrossRef]
- Solowiej, K.; Mason, V.; Upton, D. Psychological stress and pain in wound care, part 2: A review of pain and stress assessment tools. J. Wound Care 2010, 19, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Najafi, B.; Ron, E.; Enriquez, A.; Marin, I.; Razjouyan, J.; Armstrong, D.G. Smarter Sole Survival: Will Neuropathic Patients at High Risk for Ulceration Use a Smart Insole-Based Foot Protection System? J. Diabetes Sci. Technol. 2017, 11, 702–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dugas, M.; Crowley, K.; Gao, G.G.; Xu, T.; Agarwal, R.; Kruglanski, A.W.; Steinle, N. Individual differences in regulatory mode moderate the effectiveness of a pilot mHealth trial for diabetes management among older veterans. PLoS ONE 2018, 13, e0192807. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Najafi, B.; Mishra, R. Harnessing Digital Health Technologies to Remotely Manage Diabetic Foot Syndrome: A Narrative Review. Medicina 2021, 57, 377. https://doi.org/10.3390/medicina57040377
Najafi B, Mishra R. Harnessing Digital Health Technologies to Remotely Manage Diabetic Foot Syndrome: A Narrative Review. Medicina. 2021; 57(4):377. https://doi.org/10.3390/medicina57040377
Chicago/Turabian StyleNajafi, Bijan, and Ramkinker Mishra. 2021. "Harnessing Digital Health Technologies to Remotely Manage Diabetic Foot Syndrome: A Narrative Review" Medicina 57, no. 4: 377. https://doi.org/10.3390/medicina57040377
APA StyleNajafi, B., & Mishra, R. (2021). Harnessing Digital Health Technologies to Remotely Manage Diabetic Foot Syndrome: A Narrative Review. Medicina, 57(4), 377. https://doi.org/10.3390/medicina57040377