
Effect of Blue Light Filtering Intraocular Lenses on Visual Perception

 ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
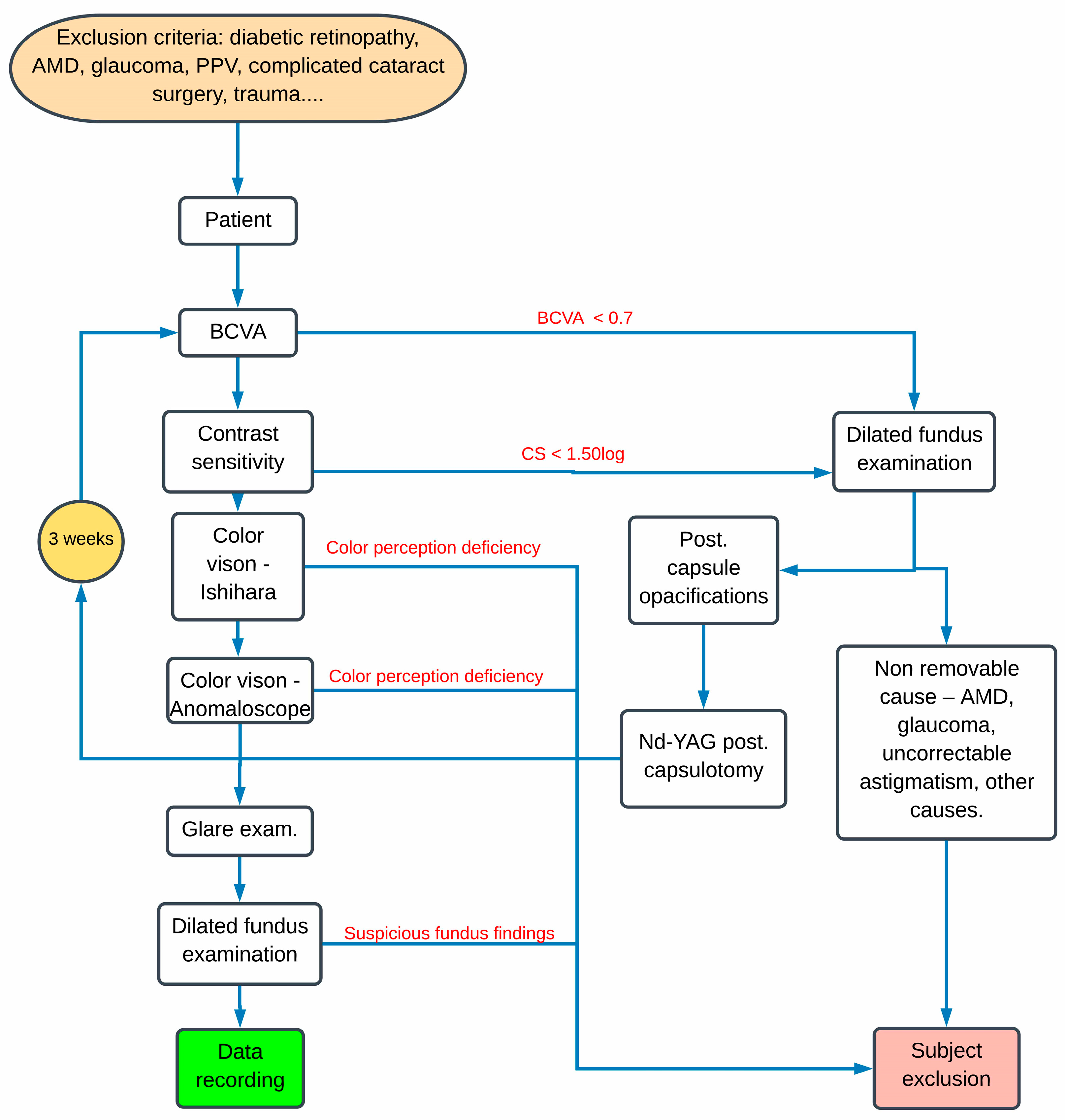
2.1. Examination Protocol and Data Collection
2.2. Statistical Analysis
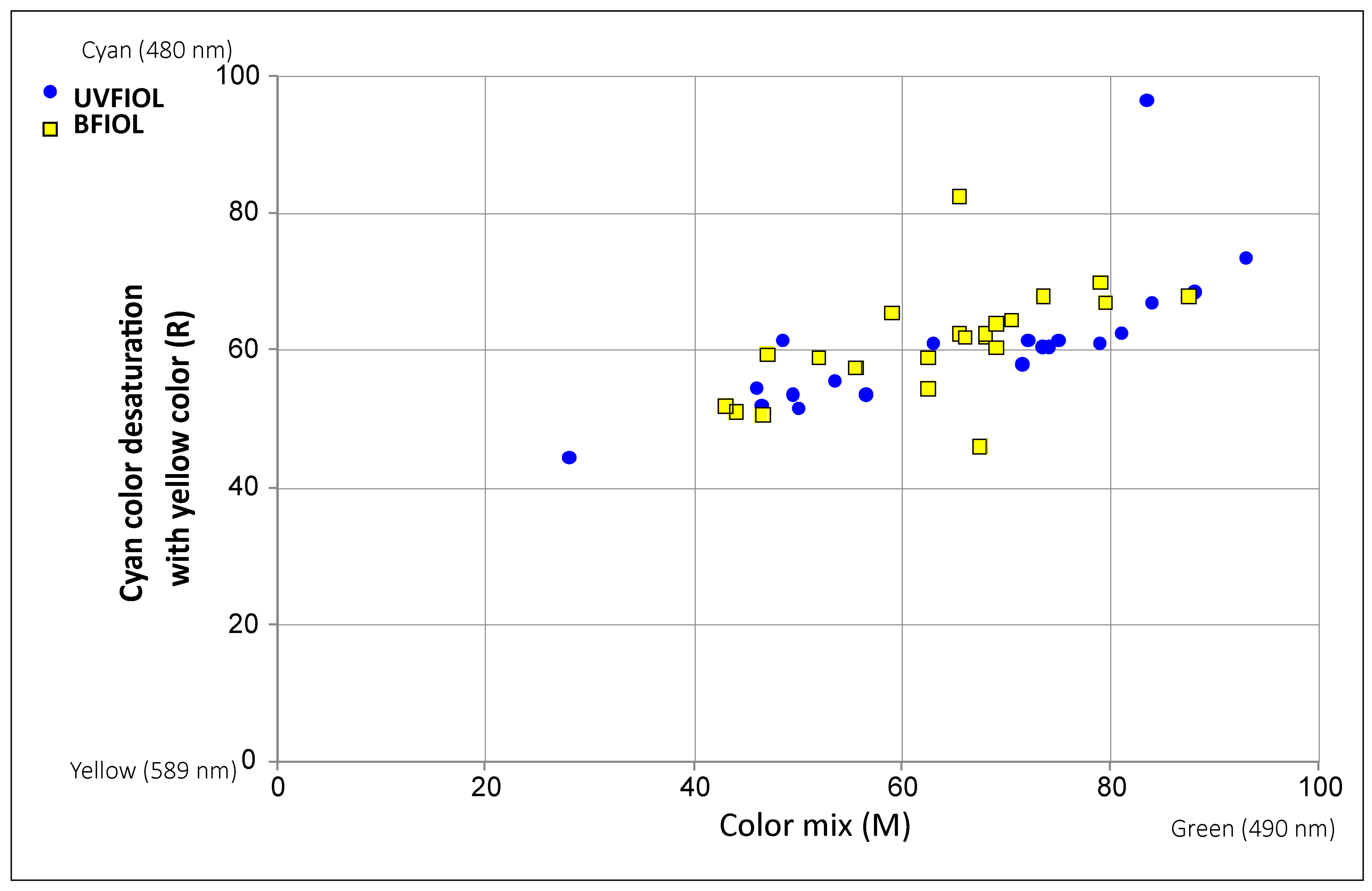
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cuthbertson, F.M.; Peirson, S.N.; Wulff, K.; Foster, R.G.; Downes, S.M. Blue light-filtering intraocular lenses: Review of potential ben-efits and side effects. J. Cataract Refract. Surg. 2009, 35, 1281–1297. [Google Scholar] [CrossRef]
- van Norren, D.; van de Kraats, J. Spectral transmission of intraocular lenses expressed as a virtual age. Br. J. Ophthalmol. 2007, 91, 1374–1375. [Google Scholar] [CrossRef] [Green Version]
- Ham, W.T., Jr.; Mueller, H.A.; Sliney, D.H. Retinal sensitivity to damage from short wavelength light. Nature 1976, 260, 153–155. [Google Scholar] [CrossRef]
- Taylor, H.R.; West, S.; Muñoz, B.; Rosenthal, F.S.; Bressler, S.B.; Bressler, N.M. The Long-term Effects of Visible Light on the Eye. Arch. Ophthalmol. 1992, 110, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Youssef, P.N.; Sheibani, N.; Albert, D.M. Retinal light toxicity. Eye 2010, 25, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Afshari, N.A. The yellow intraocular lens and the natural ageing lens. Curr. Opin. Ophthalmol. 2014, 25, 40–43. [Google Scholar] [CrossRef]
- Schwiegerling, J. Blue light–filtering intraocular lenses and scotopic sensitivity. J. Cataract Refract. Surg. 2009, 35, 2032. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Z.; Reinach, P.; Yuan, J. Contrast sensitivity and color vision with a yellow intraocular len. Am. J. Ophthalmol. 2004, 138, 138–140. [Google Scholar] [CrossRef] [PubMed]
- Mainster, M.A.; Turner, P.L. Blue-blocking IOLs Decrease Photoreception without Providing Significant Photoprotection. Surv. Ophthalmol. 2010, 55, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, S.; Saha, M.; Chakrabarti, A.; Sinha, A. Effect on contrast sensitivity after clear, yellow and orange intraocular lens implantation. Int. Ophthalmol. 2016, 36, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Tomany, S.C.; Cruickshanks, K.J.; Klein, R.; Klein, B.E.; Knudtson, M.D. Sunlight and the 10-year incidence of age-related macu-lopathy: The Beaver Dam Eye Study. Arch. Ophthalmol. 2004, 122, 750–757. [Google Scholar] [CrossRef] [Green Version]
- Cugati, S.; Mitchell, P.; Rochtchina, E.; Tan, A.G.; Smith, W.; Wang, J.J. Cataract surgery and the 10-year incidence of age-related maculopathy: The Blue Mountains Eye Study. Ophthalmology 2006, 113, 2020–2025. [Google Scholar] [CrossRef]
- Niwa, K.; Yoshino, Y.; Okuyama, F.; Tokoro, T. Effects of tinted intraocular lens on contrast sensitivity. Ophthalmic Physiol. Opt. 1996, 16, 297–302. [Google Scholar] [CrossRef]
- Bhattacharjee, H.; Bhattacharjee, K.; Medhi, J. Visual performance: Comparison of foldable intraocular lenses. J. Cataract. Refract. Surg. 2006, 32, 451–455. [Google Scholar] [CrossRef]
- Zhu, X.-F.; Zou, H.-D.; Yu, Y.-F.; Sun, Q.; Zhao, N.-Q. Comparison of Blue Light-Filtering IOLs and UV Light-Filtering IOLs for Cataract Surgery: A Meta-Analysis. PLoS ONE 2012, 7, e33013. [Google Scholar] [CrossRef] [PubMed]
- Mester, U.; Holz, F.; Kohnen, T.; Lohmann, C.; Tetz, M. Intraindividual comparison of a blue-light filter on visual function: AF-1 (UY) versus AF-1 (UV) intraocular lens. J. Cataract Refract. Surg. 2008, 34, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Pierre, A.; Wittich, W.; Faubert, J.; Overbury, O. Luminance contrast with clear and yellow-tinted intraocular lenses. J. Cataract Refract. Surg. 2007, 33, 1248–1252. [Google Scholar] [CrossRef]
- Turner, P.L.; Mainster, M.A. Circadian photoreception: Ageing and the eye’s important role in systemic health. Br. J. Ophthalmol. 2008, 92, 1439–1444. [Google Scholar] [CrossRef]
- Mainster, M.A. Violet and blue light blocking intraocular lenses: Photoprotection versus photoreception. Br. J. Ophthalmol. 2006, 90, 784–792. [Google Scholar] [CrossRef] [Green Version]
- Brøndsted, A.E.; Sander, B.; Haargaard, B.; Lund-Andersen, H.; Jennum, P.; Gammeltoft, S.; Kessel, L. The Effect of Cataract Surgery on Circadian Photoentrainment: A Randomized Trial of Blue-Blocking versus Neutral Intraocular Lenses. Ophthalmology 2015, 122, 2115–2124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brøndsted, A.E.; Haargaard, B.; Sander, B.; Lund-Andersen, H.; Jennum, P.; Kessel, L. The effect of blue-blocking and neutral intra-ocular lenses on circadian photoentrainment and sleep one year after cataract surgery. Acta Ophthalmol. 2017, 95, 344–351. [Google Scholar] [CrossRef] [Green Version]
- García-Domene, M.C.; Pérez-Vives, C.; Peris-Martínez, C.; Artigas, J.M. Comparison of the Ultraviolet Light Filtering across Dif-ferent Intraocular Lenses. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2018, 95, 1129–1134. [Google Scholar] [CrossRef]
- Downie, L.E.; Busija, L.; Keller, P.R. Blue-light filtering intraocular lenses (IOLs) for protecting macular health. Cochrane Database Syst. Rev. 2018, 22, CD011977. [Google Scholar] [CrossRef] [PubMed]
- Downie, L.E.; Wormald, R.; Evans, J.; Virgili, G.; Keller, P.R.; Lawrenson, J.G.; Li, T. Analysis of a Systematic Review About Blue Light–Filtering Intraocular Lenses for Retinal Protection: Understanding the Limitations of the Evidence. JAMA Ophthalmol. 2019, 137, 694–697. [Google Scholar] [CrossRef]
- Wirtitsch, M.G.; Schmidinger, G.; Prskavec, M.; Rubey, M.; Skorpik, F.; Heinze, G.; Findl, O.; Karnik, N. Influence of Blue-Light-Filtering Intraocular Lenses on Color Perception and Contrast Acuity. Ophthalmology 2009, 116, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Muftuoglu, O.; Karel, F.; Duman, R. Effect of a yellow intraocular lens on scotopic vision, glare disability, and blue color perception. J. Cataract Refract. Surg. 2007, 33, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Khokhar, S.K.; Jindal, A.; Agarwal, T.; Panda, A. Comparison of color perception after tinted blue light-filtering and clear ultravi-olet-filtering intraocular lens implantation. J. Cataract Refract. Surg. 2011, 37, 1598–1604. [Google Scholar] [CrossRef]
- Greenstein, V.C.; Chiosi, F.; Baker, P.; Seiple, W.; Holopigian, K.; Braunstein, R.E.; Sparrow, J.R. Scotopic sensitivity and color vision with a blue-light-absorbing intraocular lens. J. Cataract Refract. Surg. 2007, 33, 667–672. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, K.; Hayashi, H. Visual function in patients with yellow tinted intraocular lenses compared with vision in patients with non-tinted intraocular lenses. Br. J. Ophthalmol. 2006, 90, 1019–1023. [Google Scholar] [CrossRef] [Green Version]
- Derefeldt, G.; Lennerstrand, G.; Lundh, B. Age variations in normal human contrast sensitivity. Acta Ophthalmol. 1979, 57, 679–690. [Google Scholar] [CrossRef]
- Khan, K.N.; Mahroo, O.A.; Khan, R.S.; Mohamed, M.D.; McKibbin, M.; Bird, A.; Michaelides, M.; Tufail, A.; Moore, A.T. Differentiating drusen: Drusen and drusen-like appearances associated with ageing, age-related macular degeneration, inherited eye disease and other pathological processes. Prog. Retin. Eye Res. 2016, 53, 70–106. [Google Scholar] [CrossRef] [Green Version]
- da Costa, M.F.; Júnior, A.P.; Lottenberg, C.L.; Castro, L.C.; Ventura, D.F. Psychophysical Measurements of Luminance Contrast Sen-sitivity and Color Discrimination with Transparent and Blue-Light Filter Intraocular Lenses. Ophthalmol. Ther. 2017, 6, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Vuori, M.L.; Mantyjarvi, M. Colour vision and retinal nerve fibre layer photography in patients with an Acrysof Natural intra-ocular lens. Acta Ophthalmol. Scand. 2006, 84, 92–94. [Google Scholar] [CrossRef] [PubMed]
- Neumaier-Ammerer, B.; Felke, S.; Hagen, S.; Haas, P.; Zeiler, F.; Mauler, H.; Binder, S. Comparison of visual performance with blue light–filtering and ultraviolet light–filtering intraocular lenses. J. Cataract Refract. Surg. 2010, 36, 2073–2079. [Google Scholar] [CrossRef] [PubMed]
- Gray, R.; Perkins, S.A.; Suryakumar, R.; Neuman, B.; Maxwell, W.A. Reduced effect of glare disability on driving performance in patients with blue light–filtering intraocular lenses. J. Cataract Refract. Surg. 2011, 37, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Gray, R.; Hill, W.; Neuman, B.; Houtman, D.; Potvin, R. Effects of a blue light–filtering intraocular lens on driving safety in glare conditions. J. Cataract Refract. Surg. 2012, 38, 816–822. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Age (Years) | BCVA | CS (logCS) | Anomaloscope M | Anomaloscope R | Glare− | Glare + | ||
|---|---|---|---|---|---|---|---|---|
| Total | n | 60 | 60 | 59 | 48 | 48 | 51 | 50 |
| Mean | 75.62 | 0.94 | 1.78 | 64.55 | 60.39 | 3.96 | 2.66 | |
| SD | 5.48 | 0.12 | 0.13 | 14.27 | 8.97 | 0.20 | 1.51 | |
| Range | 63–87 | 0.70–1.2 | 1.50–2.0 | 13–93 | 44.5–96.5 | 3–4 | 0–4 | |
| UVIOL | n | 28 | 28 | 28 | 21 | 21 | 25 | 24 |
| Mean | 76.21 | 0.93 | 1.79 | 65.38 | 60.79 | 3.92 | 2.79 | |
| SD | 5.53 | 0.14 | 0.13 | 17.14 | 10.39 | 0.28 | 1.53 | |
| Range | 63–87 | 0.70–1.2 | 1.50–2.0 | 28–93 | 44.5–96.5 | 3–4 | 0–4 | |
| BFIOL | n | 32 | 32 | 31 | 27 | 27 | 26 | 26 |
| Mean | 75.09 | 0.96 | 1.78 | 63.91 | 60.07 | 4.00 | 2.54 | |
| SD | 5.47 | 0.09 | 0.12 | 11.88 | 7.89 | 0.00 | 1.50 | |
| Range | 67–86 | 0.70–1.2 | 1.5–2.0 | 43–87.5 | 46–82.5 | 4–4 | 0–4 | |
| UVIOL vs. BFIOL | p value | 0.434 | 0.379 | 0.645 | 0.738 | 0.788 | 0.235 | 0.549 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popov, I.; Jurenova, D.; Valaskova, J.; Sanchez-Chicharro, D.; Stefanickova, J.; Waczulikova, I.; Krasnik, V. Effect of Blue Light Filtering Intraocular Lenses on Visual Perception. Medicina 2021, 57, 559. https://doi.org/10.3390/medicina57060559
Popov I, Jurenova D, Valaskova J, Sanchez-Chicharro D, Stefanickova J, Waczulikova I, Krasnik V. Effect of Blue Light Filtering Intraocular Lenses on Visual Perception. Medicina. 2021; 57(6):559. https://doi.org/10.3390/medicina57060559
Chicago/Turabian StylePopov, Ivajlo, Denisa Jurenova, Jela Valaskova, Diego Sanchez-Chicharro, Jana Stefanickova, Iveta Waczulikova, and Vladimir Krasnik. 2021. "Effect of Blue Light Filtering Intraocular Lenses on Visual Perception" Medicina 57, no. 6: 559. https://doi.org/10.3390/medicina57060559
APA StylePopov, I., Jurenova, D., Valaskova, J., Sanchez-Chicharro, D., Stefanickova, J., Waczulikova, I., & Krasnik, V. (2021). Effect of Blue Light Filtering Intraocular Lenses on Visual Perception. Medicina, 57(6), 559. https://doi.org/10.3390/medicina57060559