
Central Serous Chorioretinopathy and Personality Characteristics: A Systematic Review of Scientific Evidence over the Last 10 Years (2010 to 2020)

 , ,
, ,  ,
,  ,
,
Abstract
:1. Introduction
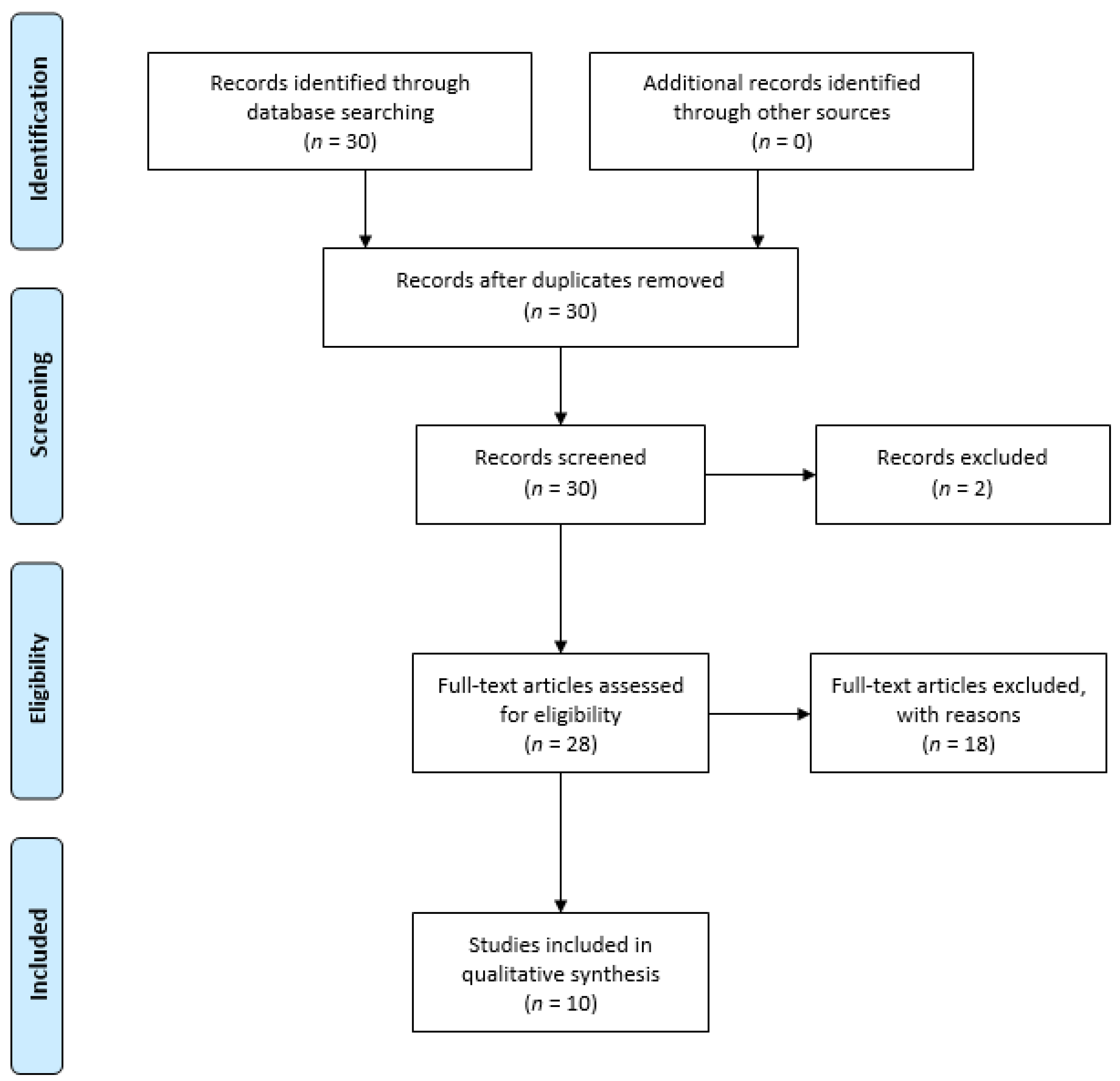
2. Materials and Methods
2.1. Search Processes
2.2. Study Selection
2.3. Data Extraction
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Number | Search Term |
|---|---|
| 1 | “Central serous chorioretinopathy” |
| 2 | “Mental disorder” |
| 3 | “personality” |
| 4 | “temperament” |
| 5 | “character” |
| 6 | “psychiatr*” |
| 7 | 1 AND 2 OR 3 OR 4 OR 5 OR 6 |
| 8 | English OR Italian [Language] |
| 9 | From 1 January 2010 to 31 December 2020 |
References
- Borooah, S.; Sim, P.Y.; Phatak, S.; Moraes, G.; Wu, C.Y.; Cheung, C.M.G.; Pal, B.; Bujarborua, D. Pachychoroid spectrum disease. Acta Ophthalmol. 2020. [Google Scholar] [CrossRef]
- Liew, G.; Quin, G.; Gillies, M.; Fraser-Bell, S. Central serous chorioretinopathy: A review of epidemiology and pathophysiology. Clin. Exp. Ophthalmol. 2013, 41, 201–214. [Google Scholar] [CrossRef]
- Gülkaş, S.; Şahin, Ö. Current Therapeutic Approaches to Chronic Central Serous Chorioretinopathy. Turk. J. Ophthalmol. 2019, 49, 30–39. [Google Scholar] [CrossRef]
- Karska-Basta, I.; Pociej-Marciak, W.; Chrząszcz, M.; Kubicka-Trząska, A.; Dębicka-Kumela, M.; Gawęcki, M.; Romanowska-Dixon, B.; Sanak, M. Imbalance in the Levels of Angiogenic Factors in Patients with Acute and Chronic Central Serous Chorioretinopathy. J. Clin. Med. 2021, 10, 1087. [Google Scholar] [CrossRef] [PubMed]
- Karska-Basta, I.; Pociej-Marciak, W.; Chrzaszcz, M.; Wilanska, J.; Jager, M.J.; Markiewicz, A.; Romanowska-Dixon, B.; Sanak, M.; Kubicka-Trzaska, A. Differences in anti-endothelial and anti-retinal antibody titers: Implications for the pathohysiology of acute and chronic central serous chorioretinopathy. J. Physiol. Pharmacol. 2020, 71, 235–242. [Google Scholar]
- Scarinci, F.; Ghiciuc, C.M.; Patacchioli, F.R.; Palmery, M.; Parravano, M. Investigating the Hypothesis of Stress System Dysregulation as a Risk Factor for Central Serous Chorioretinopathy: A Literature Mini-Review. Curr. Eye Res. 2019, 44, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Haimovici, R.; Rumelt, S.; Melby, J. Endocrine abnormalities in patients with central serous chorioretinopathy. Ophthalmology 2003, 110, 698–703. [Google Scholar] [CrossRef]
- Brand, S.; Bazzazi, N.; Ahmadpanah, M.; Seifrabie, M.A.; Holsboer-Trachsler, E.; Akbarzadeh, S. In patients suffering from idiopathic central serous chorioretinopathy, anxiety scores are higher than in healthy controls, but do not vary according to sex or repeated central serous chorioretinopathy. Neuropsychiatr. Dis. Treat. 2015, 11, 1131–1136. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-Y.; Huang, L.-Y.; Liao, W.-L.; Chou, P. Association between Central Serous Chorioretinopathy and Risk of Depression: A Population-Based Cohort Study. J. Ophthalmol. 2019, 2019, 2749296. [Google Scholar] [CrossRef]
- Ji, Y.; Li, M.; Zhang, X.; Peng, Y.; Wen, F. Poor Sleep Quality Is the Risk Factor for Central Serous Chorioretinopathy. J. Ophthalmol. 2018, 2018, 1–6. [Google Scholar] [CrossRef]
- Liu, B.; Deng, T.; Zhang, J. Risk Factors for Central Serous Chorioretinopathy. Retina 2016, 36, 9–19. [Google Scholar] [CrossRef] [Green Version]
- Tsai, D.-C.; Chen, S.-J.; Huang, C.-C.; Chou, P.; Chung, C.-M.; Huang, P.-H.; Lin, S.-J.; Chen, J.-W.; Chen, T.-J.; Leu, H.-B.; et al. Epidemiology of Idiopathic Central Serous Chorioretinopathy in Taiwan, 2001–2006: A Population-based Study. PLoS ONE 2013, 8, e66858. [Google Scholar] [CrossRef] [Green Version]
- Nicholson, B.P.; Atchison, E.; Idris, A.A.; Bakri, S.J. Central serous chorioretinopathy and glucocorticoids: An update on evidence for association. Surv. Ophthalmol. 2018, 63, 1–8. [Google Scholar] [CrossRef]
- Dunlop, B.W.; Wong, A. The hypothalamic-pituitary-adrenal axis in PTSD: Pathophysiology and treatment interventions. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 89, 361–379. [Google Scholar] [CrossRef]
- Keller, J.; Gomez, R.; Williams, G.; Lembke, A.; Lazzeroni, L.; Murphy, G.M.; Schatzberg, A.F. HPA axis in major depression: Cortisol, clinical symptomatology and genetic variation predict cognition. Mol. Psychiatry 2017, 22, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, B.P.; Idris, A.M.A.; Bakri, S.J. Central Serous Chorioretinopathy: Clinical Characteristics Associated with Visual Outcomes. Semin. Ophthalmol. 2018, 33, 804–807. [Google Scholar] [CrossRef]
- Yannuzzi, L.A. Type-A Behavior and Central Serous Chorioretinopathy. Retina 1987, 7, 111–131. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatic Association. Diagnostic and Statistical Manual of Mental Disorders, 3rd ed.; APA Press: Washington, DC, USA, 1980. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlingon, VA, USA, 2013. [Google Scholar]
- Karska-Basta, I.; Pociej-Marciak, W.; Chrząszcz, M.; Żuber-Łaskawiec, K.; Sanak, M.; Romanowska-Dixon, B. Quality of life of patients with central serous chorioretinopathy—A major cause of vision threat among middle-aged individuals. Arch. Med. Sci. 2021, 17, 724–730. [Google Scholar] [CrossRef] [PubMed]
- Türkcü, F.M.; Şahin, A.; Bez, Y.; Yuksel, H.; Çinar, Y.; Cingü, A.K.; Çaça, I. Vision-Related Quality of Life in Patients with Chronic Central Serous Chorioretinopathy. Semin. Ophthalmol. 2013, 30, 272–275. [Google Scholar] [CrossRef]
- Yu, J.; Xu, G.; Chang, Q.; Ye, X.; Li, L.; Jiang, C.; Zhao, Q. Risk Factors for Persistent or Recurrent Central Serous Chorioretinopathy. J. Ophthalmol. 2019, 2019, 5970659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matet, A.; Daruich, A.; Zola, M.; Behar-Cohen, F. Risk Factors for Recurrences of Central Serous Chorioretinopathy. Retina 2018, 38, 1403–1414. [Google Scholar] [CrossRef] [PubMed]
- Fok, A.C.; Chan, P.P.; Lam, D.S.; Lai, T.Y. Risk Factors for Recurrence of Serous Macular Detachment in Untreated Patients with Central Serous Chorioretinopathy. Ophthalmic Res. 2011, 46, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Tien, P.-T.; Lai, C.-Y.; Lin, C.-J.; Chen, W.-L.; Lin, P.-K.; Muo, C.-H.; Tsai, Y.-Y.; Wan, L.; Ho, W.-C.; Lin, H.-J. Increased Risk of Central Serous Chorioretinopathy among Patients with Nonorganic Sleep Disturbance. J. Ophthalmol. 2020, 2020, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Provencher, T.; Lemyre, A.; Vallières, A.; Bastien, C.H. Insomnia in personality disorders and substance use disorders. Curr. Opin. Psychol. 2020, 34, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Mylona, I.; Dermenoudi, M.; Tsinopoulos, I.; Floros, G. Personality of patients with central serous chorioretinopathy. Eur. J. Ophthalmol. 2020, 5. [Google Scholar] [CrossRef]
- Romano, M.R.; Parolini, B.; Allegrini, D.; Michalewska, Z.; Adelman, R.; Bonovas, S.; Bopp, S.; Citirik, M.; Tekin, K.; Fiser, I.; et al. An international collaborative evaluation of central serous chorioretinopathy: Different therapeutic approaches and review of literature. The European Vitreoretinal Society central serous chorioretinopathy study. Acta Ophthalmol. 2019, 98. [Google Scholar] [CrossRef]
- Van Haalen, F.M.; Van Dijk, E.H.; Andela, C.D.; Dijkman, G.; Biermasz, N.R.; Pereira, A.M.; Boon, C.J. Maladaptive personality traits, psychological morbidity and coping strategies in chronic central serous chorioretinopathy. Acta Ophthalmol. 2019, 97, e572–e579. [Google Scholar] [CrossRef]
- Mansour, A.M.; Koaik, M.; Lima, L.H.; Casella, A.M.B.; Uwaydat, S.H.; Shahin, M.; Tamim, H.; Sanchez-Ruiz, M.-J.; Mansour, H.A.; Dodwell, D. Physiologic and Psychologic Risk Factors in Central Serous Chorioretinopathy. Ophthalmol. Retin. 2017, 1, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Chatziralli, I.; Kabanarou, S.A.; Parikakis, E.; Chatzirallis, A.; Xirou, T.; Mitropoulos, P. Risk Factors for Central Serous Chorioretinopathy: Multivariate Approach in a Case-Control Study. Curr. Eye Res. 2017, 42, 1069–1073. [Google Scholar] [CrossRef]
- Islam, Q.U.; Hanif, M.K.; Tareen, S. Frequency of Systemic Risk Factors in Central Serous Chorioretinopathy. J. Coll. Physicians Surg. Pak. 2016, 26, 692–695. [Google Scholar] [PubMed]
- Lahousen, T.; Painold, A.; Luxenberger, W.; Schienle, A.; Kapfhammer, H.-P.; Ille, R. Psychological factors associated with acute and chronic central serous chorioretinopathy. Nord. J. Psychiatry 2015, 70, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Carlesimo, S.C.; Piazzi, G.; Leone, C.; Di Santo, L.; Coccanari dè Fornari, M.A. Masuda’s Central Serous Chorioretinopathy (C.S.C.R.) and its somatic investment in Narcissism: Our observations on new psychiatric nosography. Clin. Ter. 2014, 165, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Piskunowicz, M.; Jaracz, M.; Lesiewska, H.; Malukiewicz, G.; Brożek-Pestka, M.; Borkowska, A. Temperament Profile in Patients with Central Serous Chorioretinopathy: A Case-Control Study. Eur. J. Ophthalmol. 2014, 24, 392–395. [Google Scholar] [CrossRef] [PubMed]
- Conrad, R.; Geiser, F.; Kleiman, A.; Zur, B.; Karpawitz-Godt, A. Temperament and Character Personality Profile and Illness-Related Stress in Central Serous Chorioretinopathy. Sci. World J. 2014, 2014, 1–7. [Google Scholar] [CrossRef]
- Yannuzzi, L.A. Type A behavior and central serous chorioretinopathy. Trans. Am. Ophthalmol. Soc. 1986, 84, 799–845. [Google Scholar]
- Akram, U.; McCarty, K.; Akram, A.; Gardani, M.; Tan, A.; Villarreal, D.; Bilsborough, E.; Dooher, G.; Gibbs, G.; Hudson, J.L.; et al. The relationship between Type D personality and insomnia. Sleep Health 2018, 4, 360–363. [Google Scholar] [CrossRef] [Green Version]
- Cloninger, C.R. A Practical Way to Diagnosis Personality Disorder: A Proposal. J. Pers. Disord. 2000, 14, 99–108. [Google Scholar] [CrossRef]
- Penas, S.; Castro, P.; Pereira, G.; Oliveira, A.M.; Carneiro, Â.M.; Rocha-Sousa, A.; Azevedo, E.; Falcão-Reis, F.M. Cerebral Neurovascular Coupling Impairment in Central Serous Chorioretinopathy. Ophthalmic Res. 2020. [Google Scholar] [CrossRef]
- DeSoto, M.C.; Salinas, M. Neuroticism and cortisol: The importance of checking for sex differences. Psychoneuroendocrinology 2015, 62, 174–179. [Google Scholar] [CrossRef]
- Kitzmann, A.S.; Pulido, J.S.; Diehl, N.N.; Hodge, D.O.; Burke, J.P. The Incidence of Central Serous Chorioretinopathy in Olmsted County, Minnesota, 1980–2002. Psychoneuroendocrinology 2008, 115, 169–173. [Google Scholar] [CrossRef]
- Waugh, M.H.; Hopwood, C.J.; Krueger, R.F.; Morey, L.C.; Pincus, A.L.; Wright, A.G.C. Psychological assessment with the DSM–5 Alternative Model for Personality Disorders: Tradition and innovation. Prof. Psychol. Res. Pract. 2017, 48, 79–89. [Google Scholar] [CrossRef] [PubMed]


| Reference | Subjects | Assessment | Main Findings |
|---|---|---|---|
| Mylona I. et al. (2020) [28] | 100 CSC patients (79 male), 200 healthy control (HC), 200 non-CSC patients. | The Zuckerman–Kuhlman personality questionnaire (ZKPQ) | CSC patients, compared to the other groups, scored significantly higher on neuroticism/anxiety, aggression/hostility, and activity; they scored significantly lower in impulsivity compared to non-CSC patients. |
| Romano M.R. et al. (2019) [29] | 1719 CSC patients (1326 male, 77.1%) | The questionnaire asked patients about whether they were considered to have a high-stress personality | A total of 33.2% of patients recognised contributing factors (60.1% unknown and 6.7% missing); 96.8% of that 33.2% reported having a type-A personality |
| van Haalen F.M. et al. (2019) [30] | 86 chronic CSC patients (77 male, 90%) | Dimensional assessment of personality pathology short form (DAPPsf); The apathy scale (AS); the irritability scale (IS); The Utrecht coping scale (UCS) | Patients with CSC did not report more apathy or irritability compared with the general population at the AS and IS. The authors did not find a higher prevalence of maladaptive personality traits in patients with CSC compared with the general population. |
| Mansour A.M. et al. (2017) [31] | 86 CSC patients (67 male, 80.7%) and 86 non-CSC patients. | They administered an interview composed of different tests in a short form. | CSC group compared to controls showed higher obsessive-compulsive and aggressive behaviors, and higher type-A personality traits |
| Chatziralli I. et al. (2017) [32] | 183 first episode CSC patients (131 male, 71.6%); 183 HC. | Jenkins activity survey | Type-A personality and stress were associated with CSC. |
| Islam Q.U. et al. (2016) [33] | 42 acute CSC (38 male, 90.47%). | NA | A total of 35.71% of CSC patients suffer from emotional stress or psychiatric disorder; 26.19% have in a type-A personality. |
| Lahousen T. et al. (2016) [34] | 95 CSC patients (37 acute, 49 chronic; 71 male, 74.7%); 75 other ophthalmic patients. | The questionnaire to critical life events; Stressverarbeitungsfragebogen (SVF 120); Freiburg personality inventory (FPI-R). | Patients with CSC reported higher results then controls in psychosomatic symptoms, rumination, and several personality traits. The chronic CSC group showed higher scores in aggressiveness than the acute CSC subtype. |
| Carlesimo S.C. et al. (2014) [35] | One Male | Minnesota multiphasic personality inventory (MMPI) | A narcissistic personality disorder was diagnosed after CSC onset. The MMPI showed a tendency towards somatization. |
| Piskunowicz M. et al. (2014) [36] | 32 acute CSC (27 male, 84%), 30 HC | The temperament and character inventory (TCI) | CSC patients showed higher scores than controls in harm avoidance and reward dependence but lower scores in subscale sentimentality, as well as lower scores in novelty seeking but higher score in subscale disorderliness. |
| Conrad R. et al. (2014) [37] | 57 CSC patients (45 male, 78.9%) 57 HC | The Symptom Checklist 90-Revised (SCL-90-R); the TCI; the global severity index (GSI) | The CSC group compared to HC showed significantly higher results on GSI and SCL-90-R. CSC group was associated with a significantly lower score than controls on cooperativeness and reward dependence. Both these TCI dimensions and the subjective assessment of severity of illness correlates with illness-related work stress. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Genovese, G.; Meduri, A.; Muscatello, M.R.A.; Gangemi, S.; Cedro, C.; Bruno, A.; Aragona, P.; Pandolfo, G. Central Serous Chorioretinopathy and Personality Characteristics: A Systematic Review of Scientific Evidence over the Last 10 Years (2010 to 2020). Medicina 2021, 57, 628. https://doi.org/10.3390/medicina57060628
Genovese G, Meduri A, Muscatello MRA, Gangemi S, Cedro C, Bruno A, Aragona P, Pandolfo G. Central Serous Chorioretinopathy and Personality Characteristics: A Systematic Review of Scientific Evidence over the Last 10 Years (2010 to 2020). Medicina. 2021; 57(6):628. https://doi.org/10.3390/medicina57060628
Chicago/Turabian StyleGenovese, Giovanni, Alessandro Meduri, Maria Rosaria Anna Muscatello, Sebastiano Gangemi, Clemente Cedro, Antonio Bruno, Pasquale Aragona, and Gianluca Pandolfo. 2021. "Central Serous Chorioretinopathy and Personality Characteristics: A Systematic Review of Scientific Evidence over the Last 10 Years (2010 to 2020)" Medicina 57, no. 6: 628. https://doi.org/10.3390/medicina57060628
APA StyleGenovese, G., Meduri, A., Muscatello, M. R. A., Gangemi, S., Cedro, C., Bruno, A., Aragona, P., & Pandolfo, G. (2021). Central Serous Chorioretinopathy and Personality Characteristics: A Systematic Review of Scientific Evidence over the Last 10 Years (2010 to 2020). Medicina, 57(6), 628. https://doi.org/10.3390/medicina57060628