
Obesity May Not Be Associated with 28-Day Mortality, Duration of Invasive Mechanical Ventilation and Length of Intensive Care Unit and Hospital Stay in Critically Ill Patients with Severe Acute Respiratory Syndrome Coronavirus-2: A Retrospective Cohort Study



Abstract
:1. Introduction
2. Materials and Methods
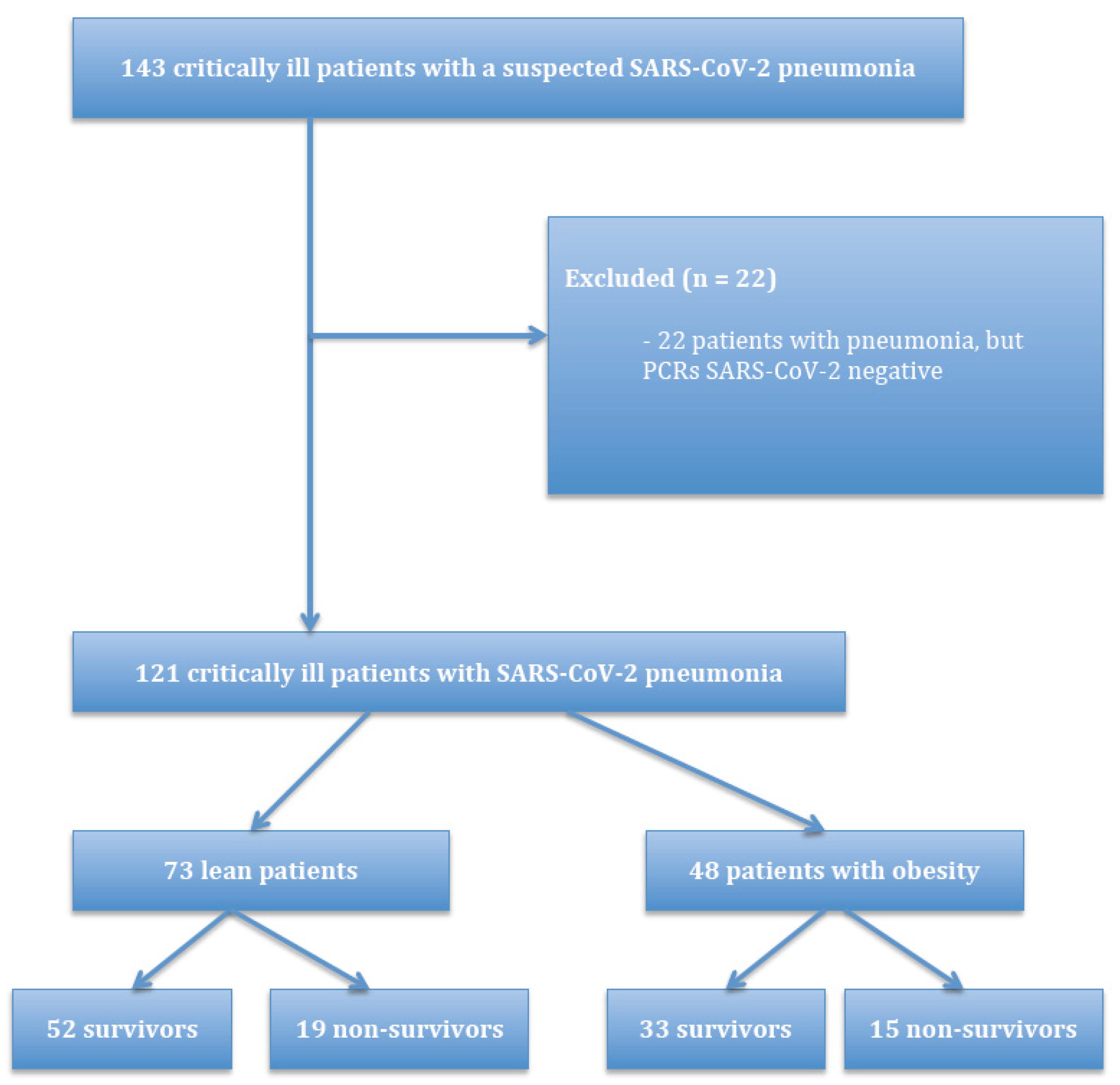
2.1. Study Design and Patient Enrolment
2.2. Outcomes
2.3. Data Collection and Statistical Analysis
3. Results
3.1. Descriptive Characteristics of the Patients
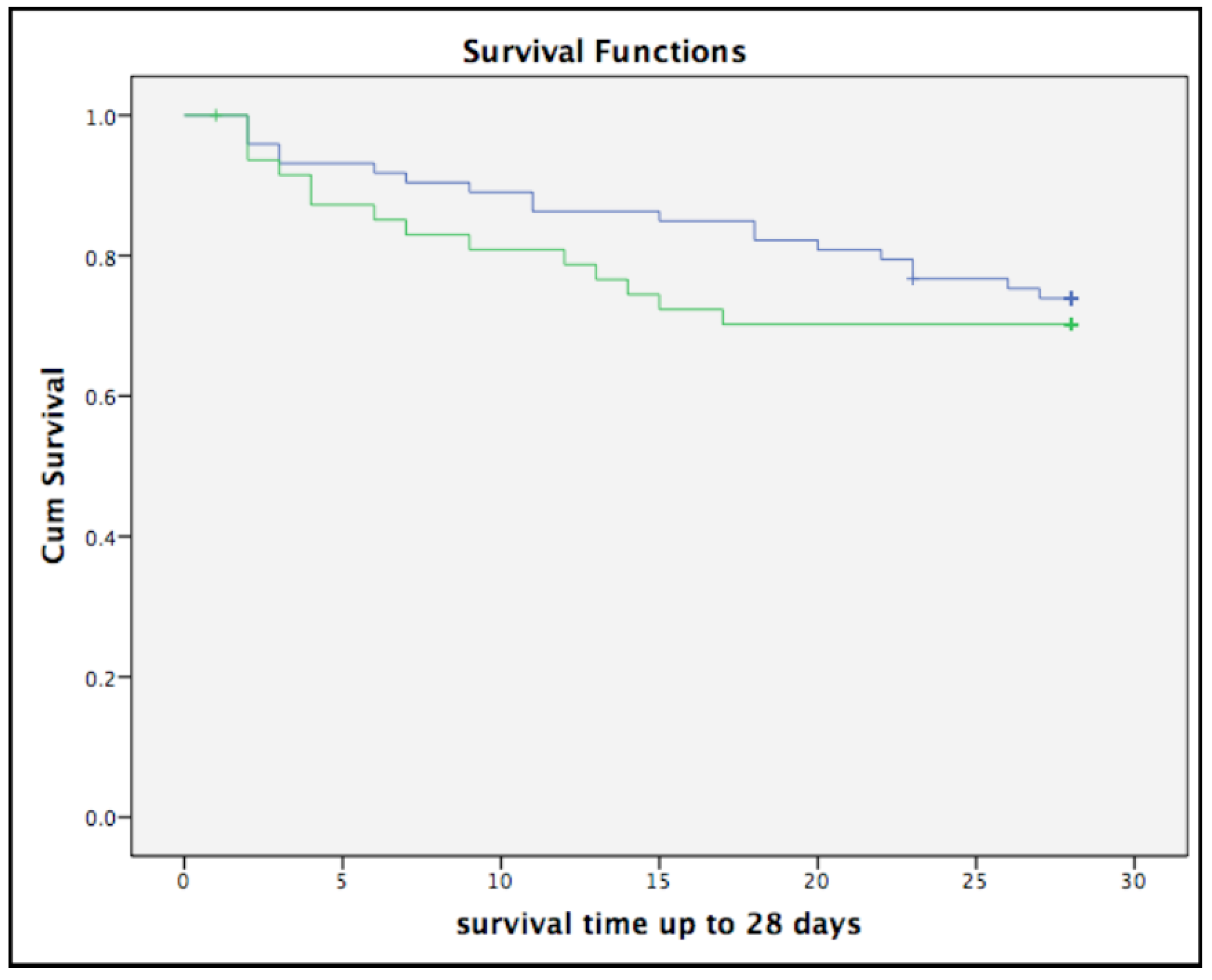
3.2. Association between Obesity and 28-Day Mortality
3.3. Association between Obesity and Duration Mechanical Ventilation, LOS ICU and Hospital
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Li, Z.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Sethuraman, N.; Jeremiah, S.S.; Ryo, A. Interpreting Diagnostic Tests for SARS-CoV-2. JAMA 2020, 323, 2249–2251. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Sanches, E.; Timmermans, M.; Topal, B.; Celik, A.; Sundbom, M.; Ribeiro, R.; Parmar, C.; Ugale, S.; Proczko, M.; Stepaniak, P.S.; et al. Cardiac remodeling in obesity and after bariatric and metabolic surgery; is there a role for gastro-intestinal hormones? Expert Rev. Cardiovasc. Ther. 2019, 17, 771–790. [Google Scholar] [CrossRef]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013, a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Sjostrom, L.; Narbro, K.; Sjostrom, C.D.; Karason, K.; Larsson, B.; Wedel, H.; Lystig, T.; Sullivan, M.; Bouchard, C.; Carlsson, B.; et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N. Engl. J. Med. 2007, 357, 741–752. [Google Scholar] [CrossRef] [Green Version]
- Appachi, S.; Kelly, K.R.; Schauer, P.R.; Kirwan, J.P.; Hazen, S.; Gupta, M.; Kashyap, S.R. Reduced cardiovascular risk following bariatric surgeries is related to a partial recovery from “adiposopathy”. Obes. Surg. 2011, 21, 1928–1936. [Google Scholar] [CrossRef] [PubMed]
- Appachi, S.; Kashyap, S.R. ‘Adiposopathy’ and cardiovascular disease: The benefits of bariatric surgery. Curr. Opin. Cardiol. 2013, 28, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Lupoli, R.; Di Minno, M.N.; Guidone, C.; Cefalo, C.; Capaldo, B.; Riccardi, G.; Mingrone, G. Effects of bariatric surgery on markers of subclinical atherosclerosis and endothelial function: A meta-analysis of literature studies. Int. J. Obes. 2016, 40, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Simonnet, A.; Chetboun, M.; Poissy, J.; Raverdy, V.; Noulette, J.; Duhamel, A.; Labreuche, A.; Mathieu, D.; Pattou, F.; Jourdain, M.; et al. High prevalence of obesity in severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) requiring invasive mechanical ventilation. Obesity 2020, 28, 1195–1199. [Google Scholar] [CrossRef]
- Caussy, C.; Wallet, F.; Laville, M.; Disse, E. Obesity is associated with severe forms of COVID-19. Obesity 2020, 28, 1175. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Hayek, S.S.; Wang, W.; Chan, L.; Mathews, K.S.; Melamed, M.L.; Brenner, S.K.; Leonberg-Yoo, A.; Schenck, E.J.; Radbel, J.; et al. Factors Associated with Death in Critically Ill Patients with Coronavirus Disease 2019 in the US. JAMA Intern. Med. 2020, 180, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Ebinger, J.E.; Achamallah, N.; Ji, H.; Claggett, B.L.; Sun, N.; Botting, P.; Nguyen, T.-T.; Luong, E.; Kim, E.H.; Park, E.; et al. Pre-existing traits associated with Covid-19 illness severity. PLoS ONE 2020, 15, e0236240. [Google Scholar] [CrossRef]
- Czernichow, S.; Beeker, N.; Rives-Lange, C.; Guerot, E.; Diehl, J.L.; Katsahian, S.; Hulot, J.-S.; Poghosyan, T.; Carette, C.; Jannot, A.S.; et al. Obesity doubles mortality in patients hospitalized for SARS-CoV-2 in Paris hospitals, France: A cohort study on 5795 patients. Obesity 2020, 28, 2282–2289. [Google Scholar] [CrossRef] [PubMed]
- Fakhry AbdelMassih, A.; Ghaly, R.; Amin, A.; Gaballah, A.; Kamel, A.; Heikal, B.; Menshawey, E.; Ismail, H.-A.; Hesham, H.; Attallah, J.; et al. Obese communities among the best predictors of COVID-19-related deaths. Cardiovasc. Endocrinol. Metab. 2020, 9, 102–107. [Google Scholar] [CrossRef]
- Onder, G.; Palmieri, L.; Vanacore, N.; Giuliano, M.; Brusaferro, S. Non-respiratory Complications and Obesity in Patients Dying with COVID-19 in Italy. Obesity 2020. [Google Scholar] [CrossRef]
- Van Kerkhove, M.D.; Vandemaele, K.A.; Shinde, V.; Jaramillo-Gutierrez, G.; Koukounari, A.; Donnelly, C.; Carlino, L.O.; Owen, R.; Paterson, B.; Pelletier, L.; et al. Risk factors for severe outcomes following 2009 influenza A (H1N1) infection: A global pooled analysis. PLoS Med. 2011, 8, e1001053. [Google Scholar] [CrossRef] [Green Version]
- Dixon, A.E.; Peters, U. The effect of obesity on lung function. Expert Rev. Respir. Med. 2018, 12, 755–767. [Google Scholar] [CrossRef]
- Huttunen, R.; Syrjanen, J. Obesity and the risk and outcome of infection. Int. J. Obes. 2013, 37, 333–340. [Google Scholar] [CrossRef] [Green Version]
- Robinson, A.T.; Fancher, I.S.; Mahmoud, A.M.; Phillips, S.A. Microvascular Vasodilator Plasticity after Acute Exercise. Exerc. Sport Sci. Rev. 2018, 46, 48–55. [Google Scholar] [CrossRef]
- Kotsis, V.; Stabouli, S.; Papakatsika, S.; Rizos, Z.; Parati, G. Mechanisms of obesity-induced hypertension. Hypertens. Res. Off. J. Jpn. Soc. Hypertens. 2010, 33, 386–393. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Zheng, J.; Zhang, L.; Liu, Y.; Chen, G.P.; Zhang, H.P.; Lei, W.; De, Y.K.; Wang, G.; Wood, L.G. Systemic inflammation mediates the detrimental effects of obesity on asthma control. Allergy Asthma Proc. 2018, 39, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Sanchis-Gomar, F.; Lavie, C.J.; Mehra, M.R.; Henry, B.M.; Lippi, G. Obesity and Outcomes in COVID-19, When an Epidemic and Pandemic Collide. Mayo Clin. Proc. 2020, 95, 1445–1453. [Google Scholar] [CrossRef]
- Chu, Y.; Yang, J.; Shi, J.; Zhang, P.; Wang, X. Obesity is associated with increased severity of disease in COVID-19 pneumonia: A systematic review and meta-analysis. Eur. J. Med Res. 2020, 25, 64. [Google Scholar] [CrossRef] [PubMed]
- Hendren, N.S.; de Lemos, J.A.; Ayers, C.; Das, S.R.; Rao, A.; Carter, S.; Rosenblatt, A.; Walchok, J.G.; Omar, W.; Khera, R.; et al. Association of Body Mass Index and Age with Morbidity and Mortality in Patients Hospitalized with COVID-19, Results from the American Heart Association COVID-19 Cardiovascular Disease Registry. Circulation 2021, 143, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Kooistra, E.J.; de Nooijer, A.H.; Claassen, W.J.; Grondman, I.; Janssen, N.A.F.; Netea, M.G.; van de Veerdonk, F.L.; van der Hoeven, J.G.; Kox, M.; Pickkers, P. A higher BMI is not associated with a different immune response and disease course in critically ill COVID-19 patients. Int. J. Obes. 2021, 45, 687–694. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | Non-Obese (BMI ≤ 30 kg/m2) | Obese (BMI > 30 kg/m2) | p Value | |
|---|---|---|---|---|
| (n = 121) | (n = 73) | (n = 48) | ||
| Age (years) (median, IQR) | 68 (60–74) | 71 (63–75) | 65 (56–71) | 0.003 |
| Male gender (N, %) | 91 (75.2%) | 58 (79.5%) | 33 (68.8%) | 0.182 |
| Pre-existing comorbidities (N, %) | ||||
| Hypertension | 37 (30.6%) | 21 (28%) | 16 (33.3%) | 0.594 |
| Congestive heart failure | 23 (19%) | 11 (15.1%) | 12 (25%) | 0.173 |
| COPD | 20 (16.5%) | 10 (13.7%) | 10 (20.8%) | 0.301 |
| Diabetes mellitus | 31 (25.6%) | 16 (21.9%) | 15 (31.3 %) | 0.250 |
| Cerebrovascular disease | 6 (5%) | 4 (5.5%) | 2 (4.2%) | 0.745 |
| Malignancy | 18 (14.9%) | 11 (15.1%) | 7 (14.6%) | 0.942 |
| Chronic renal disease | 6 (5%) | 2 (2.7%) | 4 (8.3%) | 0.166 |
| Auto-immune disorder | 9 (7.4%) | 7 (9.6%) | 2 (4.2%) | 0.266 |
| Severity of illness | ||||
| Sepsis-3, sepsis (N, %) | 116 (95.9%) | 71 (97.3%) | 45 (93.8 %) | 0.343 |
| Sepsis-3, septic shock (N, %) | 12 (9.9%) | 6 (8.2%) | 6 (12.5%) | 0.441 |
| SOFA score (points) (median, IQR) | 5 (3–7) | 6 (3–7) | 5 (3–7) | 0.504 |
| Inflammatory biomarkers | ||||
| WBC, 10E9/L, (median, IQR) | 8.3 (6.1–11.8) | 8.4 (6.4–12.2) | 7.6 (5.4–11.2) | 0.317 |
| CRP (mg/L), (mean, sd) | 141 (90–205) | 138 (90–221) | 149 (87–185) | 0.592 |
| Treatment during ICU stay (N, %) | ||||
| High flow nasal cannula | 10 (8.3%) | 6 (8.2%) | 4 (8.3%) | 0.982 |
| Invasive mechanical ventilation | 111 (91.7%) | 67 (91.8%) | 44 (91.7%) | 0.982 |
| Prone position ventilation | 65 (53.7%) | 37 (50.7%) | 28 (53.8%) | 0.409 |
| Corticosteroids (methylprednisolone) | 5 (4.1%) | 1 (1.4%) | 4 (8.3%) | 0.060 |
| Vasopressors | 99 (81.8%) | 61 (83.6%) | 38 (79.2%) | 0.540 |
| Renal replacement therapy | 9 (7.4%) | 3 (4.1%) | 6 (12.5%) | 0.085 |
| Anti-COVID-19 therapy | ||||
| Chloroquine only | 84 (69.4%) | 54 (74%) | 30 (62.5%) | 0.180 |
| Chloroquine + lopinavir/ritonavir | 36 (29.8%) | 18 (24.7%) | 18 (37.5%) | 0.131 |
| IL 1 antagonist | 2 (1.7%) | 0 (0%) | 2 (4.2%) | 0.079 |
| Outcome | ||||
| Ventilation in days (median, IQR) | 14 (8–23) | 14 (7–23) | 12 (8–17) | 0.945 |
| ICU LOS (days) (median, IQR) | 16 (9–31) | 18 (9–29) | 14 (9–17) | 0.621 |
| Hospital LOS (days) (median, IQR) | 20 (12–30) | 23 (12–33) | 17 (10–27) | 0.252 |
| 28-day mortality (N, %) | 34 (28.1%) | 19 (26%) | 15 (31.3%) | 0.532 |
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| Patients | Mortality | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age | 121 | 34 | 1.09 (1.04–1.15) | <0.001 | 1.11 (1.05–1.17) | <0.001 |
| Male | 121 | 34 | 1.45 (0.57–3.52) | 0.407 | 0.84 (0.33–2.13) | 0.710 |
| Diabetes | 121 | 34 | 1.17 (0.54–2.51) | 0.697 | 0.74 (0.32–1.73) | 0.493 |
| Hypertension | 121 | 34 | 1.17 (0.57–2.42) | 0.666 | 1.38 (0.61–3.15) | 0.439 |
| SOFA | 121 | 34 | 1.34 (1.12–1.60) | 0.001 | 1.37 (1.12–1.67) | 0.002 |
| BMI | 121 | 34 | ||||
| ≤30 kg/m2 | 1.0 (Reference) | 1.0 (Reference) | ||||
| >30 kg/m2 | 1.24 (0.62–2.47) | 0.548 | 1.74 (0.86–3.54) | 0.124 |
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| Patients | Mortality | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age | 91 | 27 | 1.10 (1.04–1.17) | <0.001 | 1.12 (1.05–1.20) | 0.001 |
| Diabetes | 91 | 27 | 1.31 (0.547–2.30) | 0.520 | 0.59 (0.24–1.49) | 0.267 |
| Hypertension | 91 | 27 | 1.44 (0.66–3.14) | 0.363 | 1.70 (0.73–3.99) | 0.222 |
| SOFA | 91 | 27 | 1.33 (1.08–1.63) | 0.007 | 1.36 (1.08–1.73) | 0.010 |
| BMI | 91 | 27 | ||||
| ≤30 kg/m2 | 1.0 (Reference) | 1.0 (Reference) | ||||
| >30 kg/m2 | 1.10(0.50–2.39) | 0.821 | 1.50 (0.66–3.41) | 0.337 |
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| Patients | Mortality | HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age | 30 | 7 | 1.01 (0.95–1.09) | 0.756 | 1.07 (0.95–1.21) | 0.278 |
| Diabetes | 30 | 7 | 0.55 (0.07–4.58) | 0.582 | 0.97 (0.07–13.33) | 0.984 |
| Hypertension | 30 | 7 | 0.38 (0.05–3.14) | 0.367 | 0.38 (0.03–5.35) | 0.476 |
| SOFA | 30 | 7 | 1.42 (0.99–2.02 | 0.054 | 1.33 (0.97–1.82) | 0.078 |
| BMI | 30 | 7 | ||||
| ≤30 kg/m2 | 1.0 (Reference) | 1.0 (Reference) | ||||
| >30 kg/m2 | 2.93 (0.57–15.11) | 0.200 | 4.99 (0.65–38.06) | 0.121 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pouwels, S.; Ramnarain, D.; Aupers, E.; Rutjes-Weurding, L.; van Oers, J. Obesity May Not Be Associated with 28-Day Mortality, Duration of Invasive Mechanical Ventilation and Length of Intensive Care Unit and Hospital Stay in Critically Ill Patients with Severe Acute Respiratory Syndrome Coronavirus-2: A Retrospective Cohort Study. Medicina 2021, 57, 674. https://doi.org/10.3390/medicina57070674
Pouwels S, Ramnarain D, Aupers E, Rutjes-Weurding L, van Oers J. Obesity May Not Be Associated with 28-Day Mortality, Duration of Invasive Mechanical Ventilation and Length of Intensive Care Unit and Hospital Stay in Critically Ill Patients with Severe Acute Respiratory Syndrome Coronavirus-2: A Retrospective Cohort Study. Medicina. 2021; 57(7):674. https://doi.org/10.3390/medicina57070674
Chicago/Turabian StylePouwels, Sjaak, Dharmanand Ramnarain, Emily Aupers, Laura Rutjes-Weurding, and Jos van Oers. 2021. "Obesity May Not Be Associated with 28-Day Mortality, Duration of Invasive Mechanical Ventilation and Length of Intensive Care Unit and Hospital Stay in Critically Ill Patients with Severe Acute Respiratory Syndrome Coronavirus-2: A Retrospective Cohort Study" Medicina 57, no. 7: 674. https://doi.org/10.3390/medicina57070674
APA StylePouwels, S., Ramnarain, D., Aupers, E., Rutjes-Weurding, L., & van Oers, J. (2021). Obesity May Not Be Associated with 28-Day Mortality, Duration of Invasive Mechanical Ventilation and Length of Intensive Care Unit and Hospital Stay in Critically Ill Patients with Severe Acute Respiratory Syndrome Coronavirus-2: A Retrospective Cohort Study. Medicina, 57(7), 674. https://doi.org/10.3390/medicina57070674