
Extended, Double-Pedicled Facial Artery Musculomucosal (dpFAMM) Flap in Tongue Reconstruction in Edentulous Patients: Preliminary Report and Flap Design

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
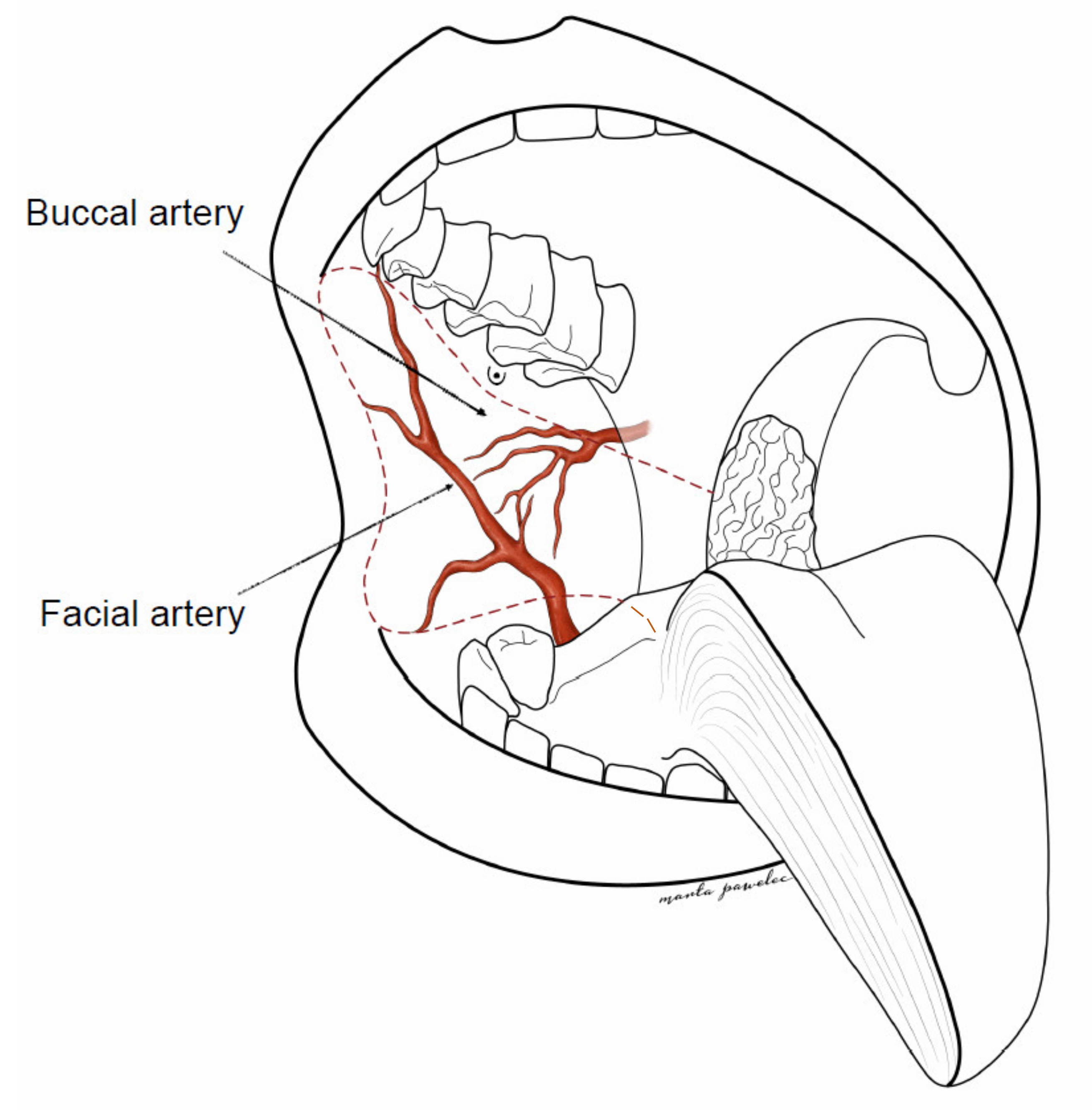
2.1. Flap Anatomy
2.2. Surgical Technique
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bokhari, W.A.; Wang, S.J. Tongue reconstruction: Recent advances. Curr. Opin. Otolaryngol. Head Neck Surg. 2007, 15, 202–207. [Google Scholar] [CrossRef]
- Gontarz, M.; Wyszynska-Pawelec, G.; Zapala, J. Clinico-pathological predictive factors in squamous cell carcinoma of the tongue and the floor of the mouth. Folia Med. Crac. 2013, 53, 73–86. [Google Scholar]
- Mannelli, G.; Arcuri, F.; Agostini, T.; Innocenti, M.; Raffaini, M.; Spinelli, G. Classification of tongue cancer resection and treatment algorithm. J. Surg. Oncol. 2018, 117, 1092–1099. [Google Scholar] [CrossRef] [PubMed]
- Pribaz, J.; Stephens, W.; Crespo, L.; Gifford, G. A new intraoral flap: Facial artery musculomucosal (FAMM) flap. Plast. Reconstr. Surg. 1992, 90, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Ayad, T.; Xie, L. Facial artery musculomucosal flap in head and neck reconstruction: A systematic review. Head Neck 2015, 37, 1375–1386. [Google Scholar] [CrossRef] [PubMed]
- Bozola, A.R.; Gasques, J.A.; Carriquiry, C.E.; Cardoso de Oliveira, M. The buccinator musculomucosal flap: Anatomic study and clinical application. Plast. Reconstr. Surg. 1989, 84, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, S.; Copelli, C.; Bianchi, B.; Ferri, A.; Sesenna, E. The Bozola flap in oral cavity reconstruction. Oral Oncol. 2012, 48, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Bardazzi, A.; Beltramini, G.A.; Autelitano, L.; Bazzacchi, R.; Rabbiosi, D.; Pedrazzoli, M.; Tewfik, K.; Rezzonico, A.; Biglioli, F. Use of Buccinator Myomucosal Flap in Tongue Reconstruction. J. Craniofac. Surg. 2017, 28, 1084–1087. [Google Scholar] [CrossRef] [PubMed]
- Joseph, S.T.; Naveen, B.S.; Mohan, M.T.; Tharayil, J. Comparison of islanded facial artery myomucosal flap with fasciocutaneous free flaps in the reconstruction of lateral oral tongue defects. Int. J. Oral Maxillofac. Surg. 2020, 49, 1000–1006. [Google Scholar] [CrossRef] [PubMed]
- Jowett, N.; Hadlock, T.A.; Sela, E.; Toth, M.; Knecht, R.; Lörincz, B.B. Facial mimetic, cosmetic, and functional standardized assessment of the facial artery musculomucosal (FAMM) flap. Auris Nasus Larynx 2017, 44, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Anzai, Y.; Brizel, D.M.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; Colevas, A.D.; et al. Head and Neck Cancers, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 873–898. [Google Scholar] [CrossRef] [PubMed]
- Duranceau, M.; Ayad, T. The facial artery musculomucosal flap: Modification of the harvesting technique for a single-stage procedure. Laryngoscope 2011, 121, 2586–2589. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Li, S.; Yan, Y.; Li, Y.; Yang, M.; Mu, L.; Huang, W.; Liu, Y.; Zhai, H.; Jin, J.; et al. New buccinator myomucosal island flap: Anatomic study and clinical application. Plast. Reconstr. Surg. 1999, 104, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Zhang, Z.; Li, Y.; Li, S.; Xiao, S.; Fan, X.; Li, Y.; Liu, P.; He, M.; Deng, C. The buccinator musculomucosal island flap for partial tongue reconstruction. J. Am. Coll. Surg. 2003, 196, 753–760. [Google Scholar] [CrossRef]
- Joseph, S.T.; Naveen, B.S.; Mohan, T.M. Islanded facial artery musculomucosal flap for tongue reconstruction. Int. J. Oral Maxillofac. Surg. 2017, 46, 453–455. [Google Scholar] [CrossRef] [PubMed]
- Massarelli, O.; Gobbi, R.; Biglio, A.; Tullio, A. Facial artery myomucosal free flap for cheek mucosa reconstruction: A case report. Microsurgery 2013, 33, 401–405. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | Age | Sex | cTNM | Neck Dissection | pTN | Grade | Comorbidities | Additional Treatment |
|---|---|---|---|---|---|---|---|---|
| 1 | 74 | M | T2N1M0 | Bilateral SND | T3N1 | G2 | External iliac artery angioplasty with stent implantation, hypertension, atherosclerosis, cataract | PORT |
| 2 | 64 | F | T2N1M0 | Bilateral SND | T3N0 | G3 | Stroke with left hemiplegia, hypertension, alcohol dependence syndrome, mitral valve regurgitation, stomach ulcer, cholecystolithiasis | PORT |
| 3 | 79 | M | T3N2cM0 | Bilateral SND | T3N2b | G2 | Senile dementia, diabetes mellitus, hypertension | PORT |
| 4 | 83 | F | T3N0M0 (recurrence after definitive radiotherapy) | No (patient after bilateral SND due to tongue SCC on the oposite side in 2019) | T3Nx | G2 | After tongue SCC T3N1M0 resection with bilateral SND, radioterapy due to new foci of tongue SCC, chemotherapy due to breast cancer, hypertension | No |
| 5 | 49 | F | T3N1M0 | Bilateral SND | T3N0 | G1 | No | PORT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gontarz, M.; Bargiel, J.; Gąsiorowski, K.; Marecik, T.; Szczurowski, P.; Zapała, J.; Wyszyńska-Pawelec, G. Extended, Double-Pedicled Facial Artery Musculomucosal (dpFAMM) Flap in Tongue Reconstruction in Edentulous Patients: Preliminary Report and Flap Design. Medicina 2021, 57, 758. https://doi.org/10.3390/medicina57080758
Gontarz M, Bargiel J, Gąsiorowski K, Marecik T, Szczurowski P, Zapała J, Wyszyńska-Pawelec G. Extended, Double-Pedicled Facial Artery Musculomucosal (dpFAMM) Flap in Tongue Reconstruction in Edentulous Patients: Preliminary Report and Flap Design. Medicina. 2021; 57(8):758. https://doi.org/10.3390/medicina57080758
Chicago/Turabian StyleGontarz, Michał, Jakub Bargiel, Krzysztof Gąsiorowski, Tomasz Marecik, Paweł Szczurowski, Jan Zapała, and Grażyna Wyszyńska-Pawelec. 2021. "Extended, Double-Pedicled Facial Artery Musculomucosal (dpFAMM) Flap in Tongue Reconstruction in Edentulous Patients: Preliminary Report and Flap Design" Medicina 57, no. 8: 758. https://doi.org/10.3390/medicina57080758
APA StyleGontarz, M., Bargiel, J., Gąsiorowski, K., Marecik, T., Szczurowski, P., Zapała, J., & Wyszyńska-Pawelec, G. (2021). Extended, Double-Pedicled Facial Artery Musculomucosal (dpFAMM) Flap in Tongue Reconstruction in Edentulous Patients: Preliminary Report and Flap Design. Medicina, 57(8), 758. https://doi.org/10.3390/medicina57080758