
Potential Circumferential Bone Engagement following Tooth Extraction in the Posterior Mandible: Computed Tomography Assessment

 ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Design
2.2. Procedure
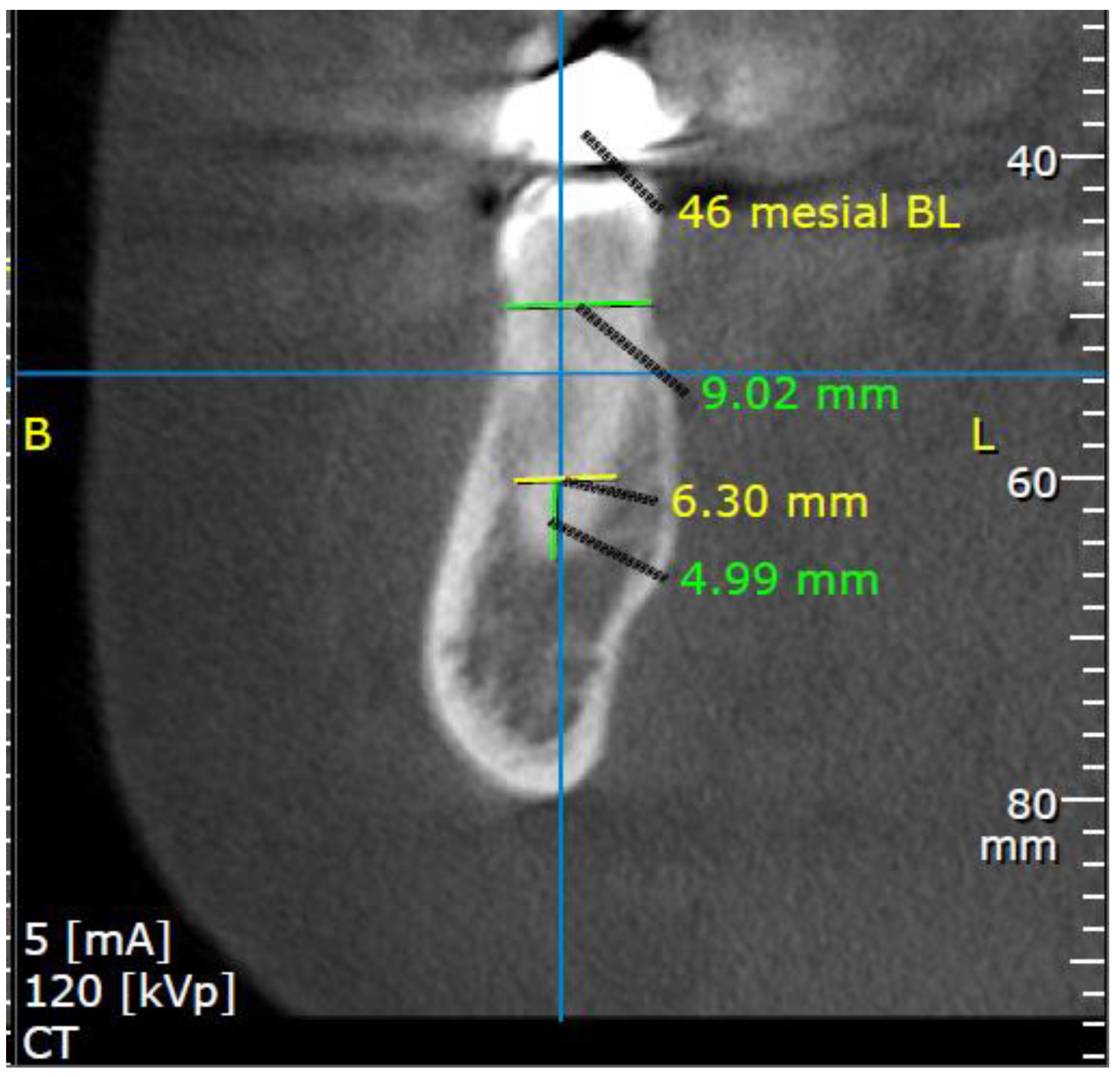
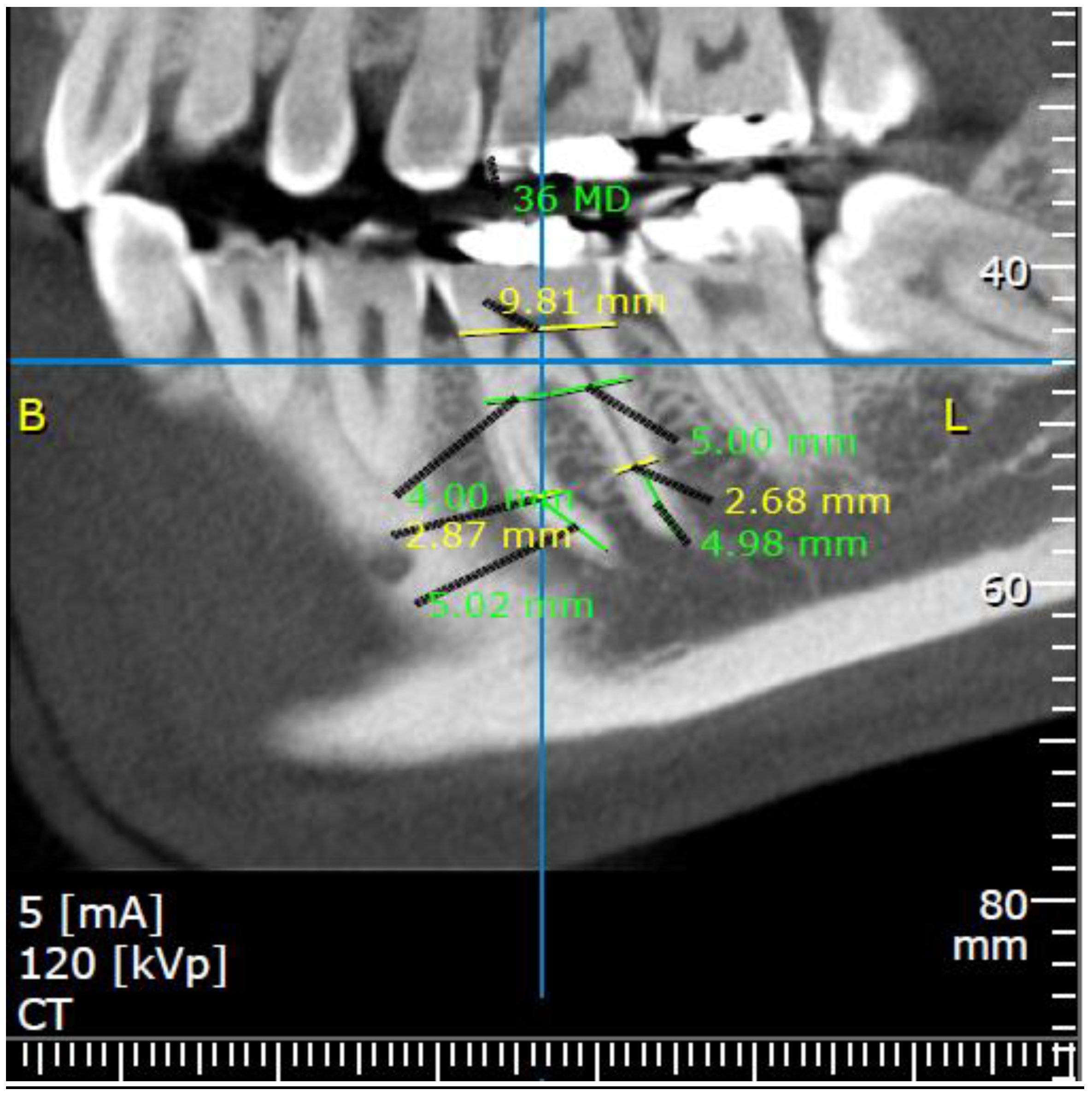
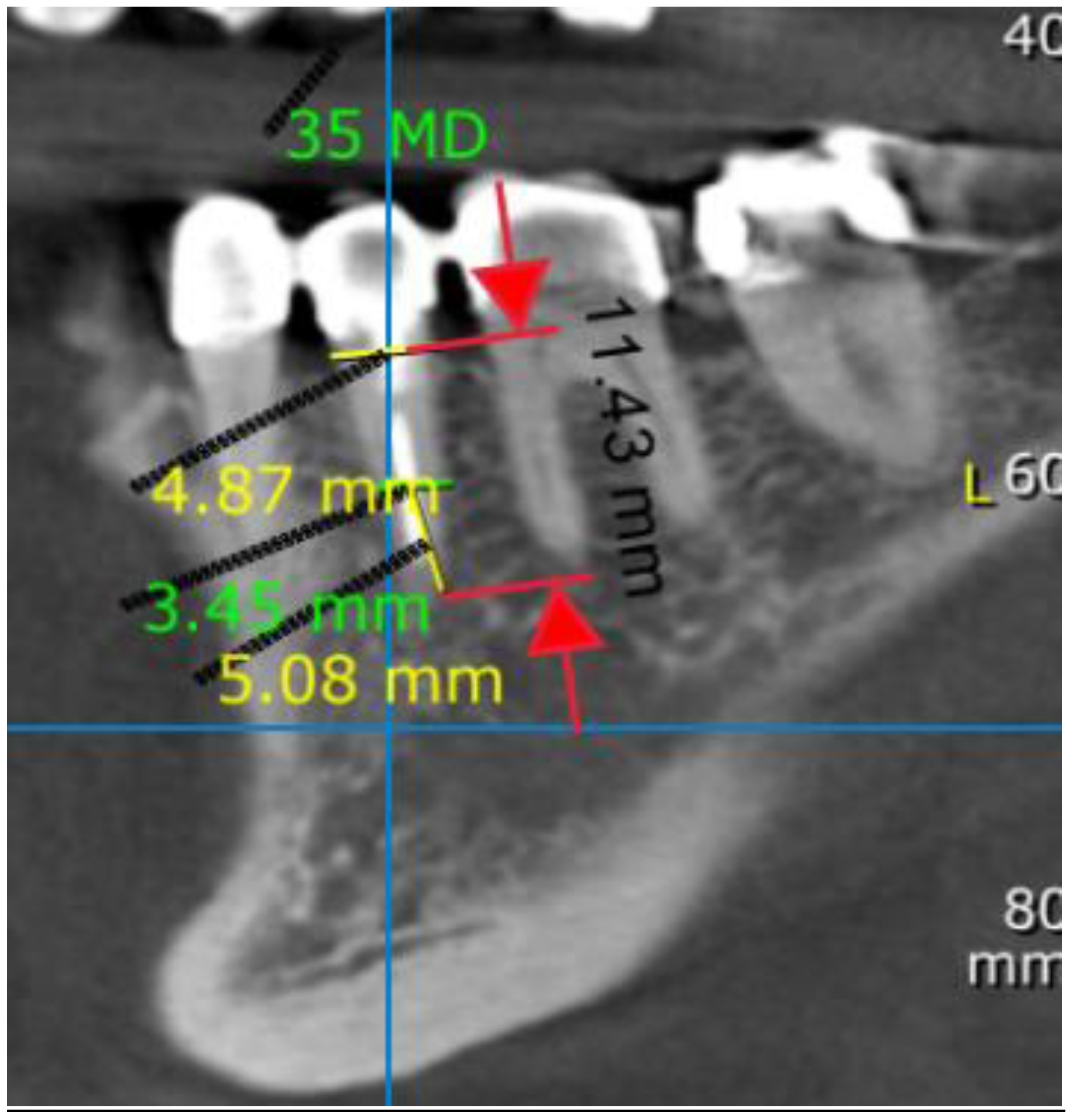
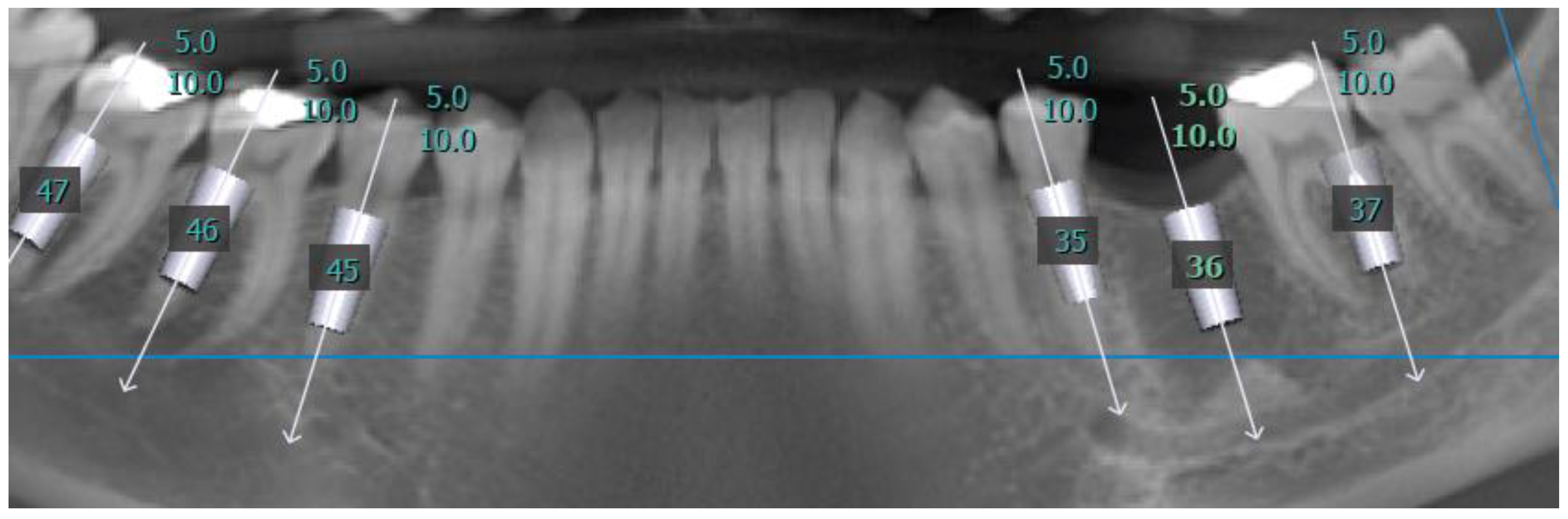
2.3. Measurements
2.4. Patient Characteristics
2.5. Statistical Analysis
3. Results
3.1. Patients
3.2. Distance Measurements
3.2.1. Mesiodistal Aspect
3.2.2. Vertical Aspect
3.2.3. Buccolingual Aspect
3.3. Modifiers
3.3.1. Sex
3.3.2. Age
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
References
- Buser, D.; Chappuis, V.; Belser, U.C.; Chen, S. Implant placement post extraction in esthetic single tooth sites: When immediate, when early, when late? Periodontology 2017, 73, 84–102. [Google Scholar] [CrossRef]
- Cosyn, J.; De Lat, L.; Seyssens, L.; Doornewaard, R.; Deschepper, E.; Vervaeke, S. The effectiveness of immediate implant placement for single tooth replacement compared to delayed implant placement: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46 (Suppl. 21), 224–241. [Google Scholar] [CrossRef] [Green Version]
- Ketabi, M.; Deporter, D.; Atenafu, E.G. A systematic review of outcomes following immediate molar implant placement based on recently published studies. Clin. Implant Dent. Relat. Res. 2016, 18, 1084–1094. [Google Scholar] [CrossRef]
- Lang, N.P.; Lui, P.; Lau, K.Y.; Li, K.Y.; Wong, M.C. A systematic review on survival and success rates of implants placed immediately into fresh extraction sockets after at least 1 year. Clin. Oral Implants Res. 2012, 23, 39–66. [Google Scholar] [CrossRef]
- Mello, C.C.; Lemos, C.A.A.; Verri, F.R.; Dos Santos, D.M.; Goiato, M.C.; Pellizzer, E.P. Immediate implant placement into fresh extraction sockets versus delayed implants into healed sockets: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 1162–1177. [Google Scholar] [CrossRef] [Green Version]
- Moy, P.K.; Nishimura, G.H.; Pozzi, A.; Danda, A.K. Single implants in dorsal areas—A systematic review. Eur. J. Oral Implantol. 2016, 9 (Suppl. 1), 163–172. [Google Scholar]
- Altintas, N.Y.; Taskesen, F.; Bagis, B.; Baltacioglu, E.; Cezairli, B.; Senel, F.C. IIP in fresh sockets versus implant placement in healed bone for full-arch fixed prostheses with conventional loading. Int. J. Oral Maxillofac. Surg. 2016, 45, 226–231. [Google Scholar] [CrossRef]
- Werbitt, M.J.; Goldberg, P.V. The immediate implant: Bone preservation and bone regeneration. Int. J. Periodontics Restor. Dent. 1992, 12, 206–217. [Google Scholar]
- Chan, H.L.; Benavides, E.; Yeh, C.Y.; Fu, J.H.; Rudek, I.E.; Wang, H.L. Risk assessment of lingual plate perforation in posterior mandibular region: A virtual implant placement study using cone-beam computed tomography. J. Periodontol. 2011, 82, 129–135. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; de Carvalho Machado, V.; Gjelvold, B. Immediate implant placement in the posterior mandible: A cone beam computed tomography study. Quintessence Int. 2016, 47, 505–514. [Google Scholar]
- Leong, D.J.; Chan, H.L.; Yeh, C.Y.; Takarakis, N.; Fu, J.H.; Wang, H.L. Risk of lingual plate perforation during implant placement in the posterior mandible: A human cadaver study. Implant Dent. 2011, 20, 360–363. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.B.; Tarnow, D.P. Classification of molar extraction sites for immediate dental implant placement: Technical note. Int. J. Oral Maxillofac. Implants 2013, 28, 911–916. [Google Scholar] [CrossRef] [Green Version]
- Haj Yahya, B.; Chaushu, G.; Hamzani, Y. Computed tomography for the assessment of the potential risk following implant placement in fresh extraction sites in the posterior mandible. J. Oral Implantol. 2021, 47, 2–8. [Google Scholar] [CrossRef]
- Froum, S.; Casanova, L.; Byrne, S.; Cho, S.C. Risk assessment before extraction for immediate implant placement in the posterior mandible: A computerized tomographic scan study. J. Periodontol. 2011, 82, 395–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, M.H.; Mau, L.P.; Cochran, D.L.; Shieh, Y.S.; Huang, P.H.; Huang, R.Y. Risk assessment of inferior alveolar nerve injury for immediate implant placement in the posterior mandible: A virtual implant placement study. J. Dent. 2014, 42, 263–270. [Google Scholar] [CrossRef] [PubMed]
- Lazzara, R.J. Immediate implant placement into extraction sites: Surgical and restorative advantages. Int. J. Periodontics Restor. Dent. 1989, 9, 333–343. [Google Scholar]
- Lioubavina-Hack, N.; Lang, N.P.; Karring, T. Significance of primary stability for osseointegration of dental implants. Clin. Oral Implants Res. 2006, 17, 244–250. [Google Scholar] [CrossRef]
- Zitzmann, N.U.; Naef, R.; Schärer, P. Resorbable versus nonresorbable membranes in combination with Bio-Oss for guided bone regeneration. Int. J. Oral Maxillofac. Implants 1997, 12, 844–852. [Google Scholar]
- Zitzmann, N.; Naef, R.; Schärer, P. Gesteuerte Knochenregeneration und Augmentation in der Implantatchirurgie mit Bio-Oss und Membrantechniken. Dtsch Zahnärztl Zeitschr. 1996, 51, 366–369. [Google Scholar]
- Misch, C.E. Root form surgery in the edentulous mandible: Stage I implant insertion. In Implant Dentistry-2; Misch, C.E., Ed.; CV Mosby Co.: St. Louis, MI, USA, 1999; pp. 347–370. [Google Scholar]
- Law, C.; Alam, P.; Borumandi, F. Floor-of-mouth hematoma following dental implant placement: Literature review and case presentation. J. Oral Maxillofac. Surg. 2017, 75, 2340–2346. [Google Scholar] [CrossRef]
- Shah, Z.; Shah, A.; Raiyani, P. Two narrow implants replacing a mandibular right first molar: A case study. J. Dent. Implants 2016, 6, 75–78. [Google Scholar]
- Monje, A.; Fu, J.H.; Chan, H.L.; Suarez, F.; Galindo-Moreno, P.; Catena, A.; Wang, H.L. Do implant length and width matter for short dental implants (<10 mm)? A meta-analysis of prospective studies. J. Periodontol. 2013, 84, 1783–1791. [Google Scholar] [CrossRef] [PubMed]
- Padhye, N.M.; Shirsekar, V.U.; Bhatavadekar, N.B. Three-dimensional alveolar bone assessment of mandibular first molars with implications for immediate implant placement. Int. J. Periodontics Restor. Dent. 2020, 40, e163–e167. [Google Scholar] [CrossRef]
- Chen, S.T.; Wilson, T.G., Jr.; Hämmerle, C.H. Immediate or early placement of implants following tooth extraction: Review of biologic basis, clinical procedures, and outcomes. Int. J. Oral Maxillofac. Implants 2004, 19, 12–25. [Google Scholar]
- Bartling, R.; Freeman, K.; Kraut, R.A. The incidence of altered sensation of the mental nerve after mandibular implant placement. J. Oral Maxillofac. Surg. 1999, 57, 1408–1412. [Google Scholar] [CrossRef]
- Goodacre, C.J.; Kan, J.Y.; Rungcharassaeng, K. Clinical complications of osseointegrated implants. J. Prosthet. Dent. 1999, 81, 537–552. [Google Scholar] [CrossRef]
- Greenstein, G.; Tarnow, D. The mental foramen and nerve: Clinical and anatomical factors related to dental implant placement: A literature review. J. Periodontol. 2006, 77, 1933–1943. [Google Scholar] [CrossRef] [PubMed]
- Greenstein, G.; Cavallaro, J.; Romanos, G.; Tarnow, D. Clinical recommendations for avoiding and managing surgical complications associated with implant dentistry: A review. J. Periodontol. 2008, 79, 1317–1329. [Google Scholar] [CrossRef] [PubMed]
- Lamas Pelayo, J.; Peñarrocha Diago, M.; Martí Bowen, E.; Peñarrocha Diago, M. Intraoperative complications during oral implantology. Med. Oral Patol. Oral Cir. Bucal. 2008, 13, E239–E243. [Google Scholar]
- Nunes, L.S.; Bornstein, M.M.; Sendi, P.; Buser, D. Anatomical characteristics and dimensions of edentulous sites in the posterior maxillae of patients referred for implant therapy. Int. J. Periodontics Restor. Dent. 2013, 33, 337–345. [Google Scholar] [CrossRef] [Green Version]
- Kerr, N.W.; Ringrose, T.J. Factors affecting the lifespan of the human dentition in Britain prior to the seventeenth century. Br. Dent. J. 1998, 184, 242–246. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tooth Type/Root | Mesiodistal Distance (mm), Mean (SD) | Predicted Prevalence of Radiological Circumferential Engagement by Implant Diameter | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No. Teeth (Roots) | A Point | F Point | X Point (for Tooth) | Implant Diameter | ||||||
| 3.3 mm | 3.754.1 mm | 4–4.2 mm | 4.5–4.8 mm | 5 mm | 5.5 mm | |||||
| Second molar | 156(312) | 3.11(0.5) | 4.32(0.6) | 9.19(0.58) | 59% | 77% | 88% | 99% | 100% | 100% |
| 37D | 79 | 3.3(0.49) | 4.67(0.48) | 9.25(0.57) | 42% | 64% | 82% | 96% | 99% | 99% |
| 37M | 79 | 2.91(0.44) | 4.1(0.47) | 9.25(0.57) | 82% | 90% | 93% | 99% | 100% | 100% |
| 47D | 77 | 3.34(0.45) | 4.66(0.5) | 9.12(0.6) | 37% | 64% | 78% | 100% | 100% | 100% |
| 47M | 77 | 2.87(0.41) | 3.86(0.49) | 9.12(0.6) | 77% | 91% | 99% | 100% | 100% | 100% |
| First molar | 147(294) | 2.98(0.5) | 4.41(0.56) | 9.14(0.71) | 70% | 87% | 94% | 97% | 99% | 100% |
| 36D | 74 | 3.03(0.41) | 4.59(0.46) | 9.14(0.78) | 67% | 88% | 97% | 99% | 100% | 100% |
| 36M | 74 | 2.74(0.41) | 4.25(0.46) | 9.14(0.78) | 88% | 95% | 99% | 99% | 100% | 100% |
| 46D | 73 | 3.23(0.53) | 4.76(0.6) | 9.14(0.63) | 46% | 78% | 88% | 94% | 97% | 100% |
| 46M | 73 | 2.9(0.51) | 4.06(0.43) | 9.14(0.63) | 78% | 88% | 94% | 97% | 99% | 100% |
| Second premolar | 175(175) | 3.64(0.51) | 5.41(0.68) | 19% | 39% | 58% | 88% | 96% | 99% | |
| 35 | 83 | 3.61(0.55) | 5.46(0.77) | 21% | 43% | 64% | 88% | 95% | 99% | |
| 45 | 92 | 3.66(0.48) | 5.37(0.59) | 18% | 35% | 54% | 88% | 97% | 100% | |
| Tooth Type/Root | Vertical Distance (mm), Mean (SD) | Prevalence of Predicted Available Implant Length | |||
|---|---|---|---|---|---|
| No. Teeth (Roots) | X Point (for Tooth) | Implant Length | |||
| 10 mm | 8 mm | 6 mm | |||
| Second molar | 156 (312) | 11.83 (1.73) | 86% | 97% | 100% |
| 37D | 79 | 11.46 (1.74) | 84% | 95% | 99% |
| 37M | 79 | 12.29 (1.72) | 91% | 97% | 100% |
| 47D | 77 | 11.5 4 (1.72) | 82% | 97% | 100% |
| 47M | 77 | 12.03 (1.78) | 87% | 100% | 100% |
| First molar | 147(294) | 12.61 (1.86) | 90% | 98% | 100% |
| 36D | 74 | 12.1 (1.96) | 86% | 96% | 100% |
| 36M | 74 | 13.07 (1.83) | 95% | 97% | 100% |
| 46D | 73 | 12.21 (1.86) | 88% | 99% | 100% |
| 46M | 73 | 13.07 (1.8) | 92% | 100% | 100% |
| Second premolar | 175 (175) | 13.8 7(1.87) | 99% | 100% | 100% |
| 35 | 83 | 13.99 (1.78) | 99% | 100% | 100% |
| 45 | 92 | 13.76 (1.94) | 98% | 99% | 100% |
| Tooth Type/Root | All | Side | Sex | Age (year) | |||
|---|---|---|---|---|---|---|---|
| Right | Left | Female | Male | ≤40 y | 40+ y | ||
| Total teeth | 478 | 242 | 236 | 245 | 233 | 326 | 152 |
| Total roots | 781 | 394 | 387 | 402 | 379 | 534 | 247 |
| Number of roots by tooth type | |||||||
| 2nd premolars | 175 | 92 | 83 | 88 | 87 | 118 | 57 |
| 1st molars | 294 | 148 | 146 | 150 | 144 | 198 | 96 |
| 2nd molars | 312 | 154 | 158 | 164 | 148 | 218 | 94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamzani, Y.; Yassien, E.; Moskovich, L.; Becker, T.; Chaushu, G.; Haj Yahya, B. Potential Circumferential Bone Engagement following Tooth Extraction in the Posterior Mandible: Computed Tomography Assessment. Medicina 2021, 57, 874. https://doi.org/10.3390/medicina57090874
Hamzani Y, Yassien E, Moskovich L, Becker T, Chaushu G, Haj Yahya B. Potential Circumferential Bone Engagement following Tooth Extraction in the Posterior Mandible: Computed Tomography Assessment. Medicina. 2021; 57(9):874. https://doi.org/10.3390/medicina57090874
Chicago/Turabian StyleHamzani, Yafit, Emran Yassien, Liad Moskovich, Talia Becker, Gavriel Chaushu, and Bahaa Haj Yahya. 2021. "Potential Circumferential Bone Engagement following Tooth Extraction in the Posterior Mandible: Computed Tomography Assessment" Medicina 57, no. 9: 874. https://doi.org/10.3390/medicina57090874
APA StyleHamzani, Y., Yassien, E., Moskovich, L., Becker, T., Chaushu, G., & Haj Yahya, B. (2021). Potential Circumferential Bone Engagement following Tooth Extraction in the Posterior Mandible: Computed Tomography Assessment. Medicina, 57(9), 874. https://doi.org/10.3390/medicina57090874