
Longitudinal Cognitive Assessment in Low-Risk Very Preterm Infants

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Neurodevelopmental Assessment at 12 and 24 Months
2.2. Cognitive Function at Preschool Age
2.3. Statistical Analysis
3. Results
3.1. Neurodevelopmental Assessment at 12 and 24 Months
3.2. Cognitive Function at Preschool Age
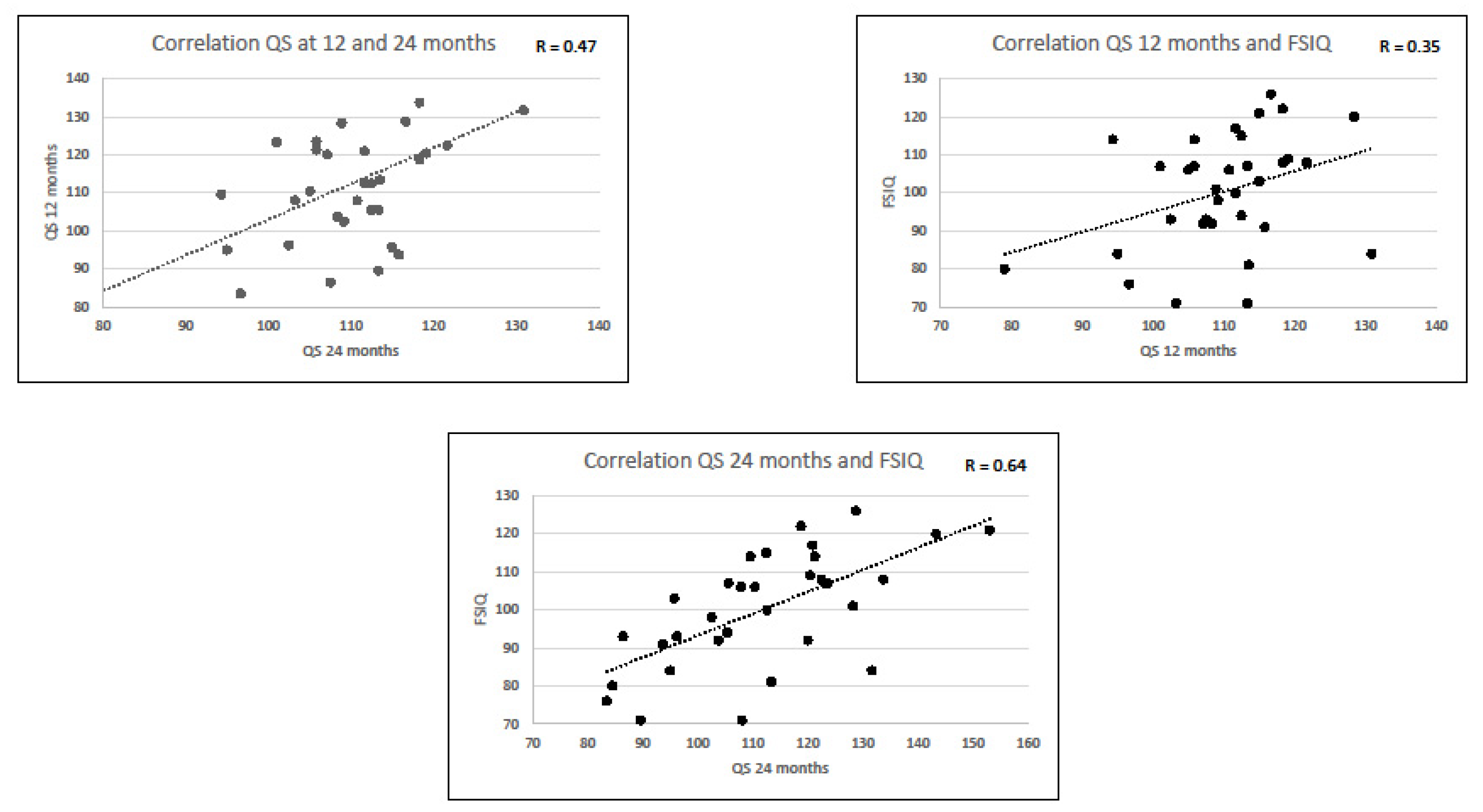
3.3. Neurodevelopmental Scores at 12 and 24 Months and IQs at Preschool Age
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vogel, J.P.; Chawanpaiboon, S.; Moller, A.B. The global epidemiology of preterm birth. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 52, 3–12. [Google Scholar] [CrossRef]
- Allotey, J.; Zamora, J.; Cheong-See, F. Cognitive, motor, behavioural and academic performances of children born preterm: A meta-analysis and systematic review involving 64061 children. BJOG 2018, 125, 16–25. [Google Scholar] [CrossRef] [Green Version]
- Howe, T.U.; Sheu, C.F.; Hsu, Y.W. Predicting neurodevelopmental outcomes at preschool age for children with very low birth weight. Res. Dev. Disabil. 2016, 48, 231–241. [Google Scholar] [CrossRef]
- Ionio, C.; Riboni, E.; Confalonieri, E. Paths of cognitive and language development in healthy preterm infants. Infant Behav. Dev. 2016, 44, 199–207. [Google Scholar] [CrossRef]
- Romeo, D.M.; Di Stefano, A.; Conversano, M. Neurodevelopmental outcome at 12 and 18 months in late preterm infants. Eur. J. Paediatr. Neurol. 2010, 14, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Bhutta, A.T.; Cleves, M.A.; Casey, P.H. Cognitive and behavioral outcomes of school-aged children who were born preterm. JAMA 2002, 288, 728–733. [Google Scholar] [CrossRef]
- Stein, M.T.; Lukasik, M.K. Developmental screening and assessment: Infants, toddlers, and preschoolers. In Developmental-Behavioral Pediatrics, 3rd ed.; Levine, M.D., Carey, W.B., Crocker, A.C., Eds.; Saunders Elsevier: Philadelphia, CA, USA, 2009; p. 785. [Google Scholar]
- Aisa, M.C.; Barbati, A.; Gerli, S. Brain 3D-echographic early predictors of neuro behavioral disorders in infants: A prospective observational study. J. Matern. Fetal. Neonatal. Med. 2020, 5, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Wong, H.S.; Santhakumaran, S.; Cowan, F.M.; Modi, N. Medicines for Neonates Investigator Group. Developmental Assessments in Preterm Children: A Meta-analysis. Pediatrics 2016, 138, e20160251. [Google Scholar] [CrossRef] [Green Version]
- Sansavini, A.; Savini, S.; Guarini, A.; Broccoli, S.; Alessandroni, R.; Faldella, G. The effect of gestational age on developmental outcomes: A longitudinal study in the first 2 years of life. Child Care Health Dev. 2011, 37, 26–36. [Google Scholar] [CrossRef]
- De Vries, L.S.; Eken, P.; Dubowitz, L.M. The spectrum of leukomalacia using cranial ultrasound. Behav. Brain Res. 1992, 49, 1–6. [Google Scholar] [CrossRef]
- Griffiths, R. The Abilities of Young Children: A Comprehensive System of Mental Measurement for the First 8 Years of Life; Child Development Research Centre London: London, UK, 1970. [Google Scholar]
- Wechsler, D. WPPSI-III Administration and Scoring Manual; The Psychological Corporation: San Antonio, TX, USA, 2002. [Google Scholar]
- Pérez-Pereira, M.; Fernández, M.P.; Gómez-Taibo, M.L.; Martínez-López, Z.; Arce, C. A Follow-Up Study of Cognitive Development in Low Risk Preterm Children. Int. J. Environ. Res. Public Health 2020, 17, 2380. [Google Scholar] [CrossRef] [Green Version]
- Dall’oglio, A.M.; Rossiello, B.; Coletti, M.F.; Bultrini, M.; De Marchis, C.; Ravà, L.; Caselli, C.; Paris, S.; Cuttini, M. Do healthy preterm children need neuropsychological follow-up? Preschool outcomes compared with term peers. Dev. Med. Child. Neurol. 2010, 52, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Caravale, B.; Tozzi, C.; Albino, G.; Vicari, S. Cognitive development in low risk preterm infants at 3–4 years of life. Arch. Dis. Child. Fetal Neonatal 2005, 90, F474-9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guzzetta, F. Neurology of the Infant; Mariani Foundation Paediatric Neurology Series; John Libbey Eurotext: Montrouge, France, 2009. [Google Scholar]
- Cizmeci, M.N.; de Vries, L.S.; Ly, L.G.; van Haastert, I.C.; Groenendaal, F.; Kelly, E.N.; Traubici, J.; Whyte, H.E.; Leijser, L.M. Periventricular Hemorrhagic Infarction in Very Preterm Infants: Characteristic Sonographic Findings and Association with Neurodevelopmental Outcome at Age 2 Years. J. Pediatr. 2020, 217, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Gunkel, J.; de Vries, L.S.; Jongmans, M.; Koopman-Esseboom, C.; van Haastert, I.C.; Eijsermans, M.C.J.; van Stam, C.; van Zanten, B.G.A.; Wolfs, T.F.W.; Nijman, J. Outcome of Preterm Infants With Postnatal Cytomegalovirus Infection. Pediatrics 2018, 141, e20170635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Squarza, C.; Picciolini, O.; Gardon, L.; Ravasi, M.; Giannì, M.L.; Porro, M.; Bonzini, M.; Gangi, S.; Mosca, F. Seven Years Cognitive Functioning and Early Assessment in Extremely Low Birth Weight Children. Front. Psychol. 2017, 21, 1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarra, R.; Sestieri, C.; Conte, E.; Salomone, R.; Mattei, P.A.; Romani, G.L.; Domizio, S.; Caulo, M. Perinatal MRI diffusivity is related to early assessment of motor performance in preterm neonates. Neuroradiol. J. 2016, 29, 137–145. [Google Scholar] [CrossRef] [Green Version]
- Moon, N.M.; Mohay, H.A.; Gray, P.H. Developmental patterns from 1 to 4 years of extremely preterm infants who required home oxygen therapy. Early Hum. Dev. 2007, 83, 209–216. [Google Scholar] [CrossRef] [Green Version]
- Pasman, J.W.; Rotteveel, J.J.; Maassen, B. Neurodevelopmental profile in low-risk preterm infants at 5 years of age. Eur. J. Paediatr. Neurol. 1998, 2, 7–17. [Google Scholar] [CrossRef]
- O’Connor, C.M.; Ryan, C.A.; Boylan, G.B.; Murray, D.M. The ability of early serial developmental assessment to predict outcome at 5years following neonatal hypoxic-ischaemic encephalopathy. Early Hum. Dev. 2017, 110, 1–8. [Google Scholar] [CrossRef]
- Barnett, A.L.; Guzzetta, A.; Mercuri, E.; Henderson, S.E.; Haataja, L.; Cowan, F.; Dubowitz, L. Can the Griffiths scales predict neuromotor and perceptual-motor impairment in term infants with neonatal encephalopathy? Arch. Dis. Child. 2004, 89, 637–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutcliffe, A.G.; Soo, A.; Barnes, J. Predictive value of developmental testing in the second year for cognitive development at five years of age. Pediatr. Rep. 2010, 2, e15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fedrizzi, E.; Inverno, M.; Botteon, G.; Anderloni, A.; Filippini, G.; Farinotti, M. The cognitive development of children born preterm and affected by spastic diplegia. Brain Dev. 1993, 15, 428–432. [Google Scholar] [CrossRef]
- Romeo, D.M.; Guzzardi, S.; Ricci, D.; Cilauro, S.; Brogna, C.; Cowan, F.; Romeo, M.G.; Mercuri, E. Longitudinal cognitive assessment in healthy late preterm infants. Eur. J. Paediatr. Neurol. 2012, 16, 243–247. [Google Scholar] [CrossRef]
- Hindmarsh, G.J.; O’Callaghan, M.J.; Mohay, H.A.; Rogers, Y.M. Gender differences in cognitive abilities at 2 years in ELBW infants. Extremely low birth weight. Early Hum. Dev. 2000, 60, 115–122. [Google Scholar] [CrossRef]


{kind=link}
| SQ-A (Mean ± SD) | SQ-B (Mean± SD) | SQ-C (Mean ± SD) | SQ-D (Mean ± SD) | SQ-E (Mean ± SD) | GDQ (Mean ± SD) | |
|---|---|---|---|---|---|---|
| Total | 106 ± 15 | 115 ± 13.4 | 112,3 ± 16 | 110 ± 12.1 | 115 ± 16.7 | 111.5 ± 10 |
| Female | 105.7± 14.3 | 116 ± 13.8 | 112.1 ± 15.8 | 109.4 ± 12 | 114.5 ± 11.8 | 111.5 ± 9.7 |
| Male | 106.3 ± 16.6 | 112.7 ± 12.7 | 112.6 ± 16.3 | 111 ± 12.5 | 115.3 ± 22.8 | 111.6 ± 10.7 |
| SQ-A (Mean ± SD) | SQ-B (Mean ± SD) | SQ-C (Mean ± SD) | SQ-D (Mean ± SD) | SQ-E (Mean ± SD) | GDQ (Mean ± SD) | |
|---|---|---|---|---|---|---|
| Total | 107.9 ± 20 | 120.6 ± 21.5 | 109.7 ±22.5 | 103.2 ± 13.2 | 111.3 ± 20.4 | 110.5 ± 15.5 |
| Female | 106.9 ± 21.3 | 120.3 ± 21.5 | 109.4 ±24.2 | 102 ± 13.4 | 110.2 ± 19.9 | 109.7 ± 16 |
| Male | 109.5 ±17.8 | 121.1 ± 22 | 110.1 ± 20 | 105.3 ± 13 | 113.2 ±21.5 | 111.8 ± 15 |
| SQ-A 12 m | SQ-A 24 m | SQ-B 12 m | SQ-B 24 m | SQ-C 12 m | SQ-C 24 m | SQ-D 12 m | SQ-D 24 m | SQ-E 12 m | SQ-E 24 m | GDQ 12 m | GDQ 24 m |
|---|---|---|---|---|---|---|---|---|---|---|---|
| r = 0.40 | r = 0.32 | r = 0.30 | r = 0.28 | r = 0.30 | r = 0.47 | ||||||
| p < 0.001 | p < 0.01 | p < 0.05 | p < 0.05 | p < 0.05 | p < 0.001 | ||||||
| VIQ (Mean ± SD) | PIQ (Mean ± SD) | FSIQ (Mean ± SD) | |
|---|---|---|---|
| Total | 103.3 ± 15.1 | 98.9 ± 16.3 | 100.3 ± 15 |
| Female | 100.6 ± 14.3 | 99 ± 17.7 | 99.2 ± 16 |
| Male | 107.9 ± 16 | 98.7 ± 14.4 | 102.3 ± 13.4 |
| GDQ 12 m | GDQ 24 m | |
|---|---|---|
| Correlation coefficient | ||
| FSIQ | 0.35 (p < 0.05) | 0.64 (p < 0.001) |
| VIQ | 0.44 (p < 0.01) | 0.60 (p < 0.001) |
| PIQ | 0.05 (p > 0.4) | 0.40 (p < 0.05) |
| Sensitivity/Specificity | ||
| FSIQ | 0.2/1 | 0.6/1 |
| VIQ | 0/0.98 | 0.6/0.98 |
| PIQ | 0/0.98 | 0.38/0.98 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romeo, D.M.; Ricci, M.; Mirra, F.; Venezia, I.; Mallardi, M.; Pede, E.; Mercuri, E. Longitudinal Cognitive Assessment in Low-Risk Very Preterm Infants. Medicina 2022, 58, 133. https://doi.org/10.3390/medicina58010133
Romeo DM, Ricci M, Mirra F, Venezia I, Mallardi M, Pede E, Mercuri E. Longitudinal Cognitive Assessment in Low-Risk Very Preterm Infants. Medicina. 2022; 58(1):133. https://doi.org/10.3390/medicina58010133
Chicago/Turabian StyleRomeo, Domenico M., Martina Ricci, Federica Mirra, Ilaria Venezia, Maria Mallardi, Elisa Pede, and Eugenio Mercuri. 2022. "Longitudinal Cognitive Assessment in Low-Risk Very Preterm Infants" Medicina 58, no. 1: 133. https://doi.org/10.3390/medicina58010133
APA StyleRomeo, D. M., Ricci, M., Mirra, F., Venezia, I., Mallardi, M., Pede, E., & Mercuri, E. (2022). Longitudinal Cognitive Assessment in Low-Risk Very Preterm Infants. Medicina, 58(1), 133. https://doi.org/10.3390/medicina58010133