

The Relationship between Neuropsychiatric Symptoms and Cognitive Performance in Older Adults with Normal Cognition

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
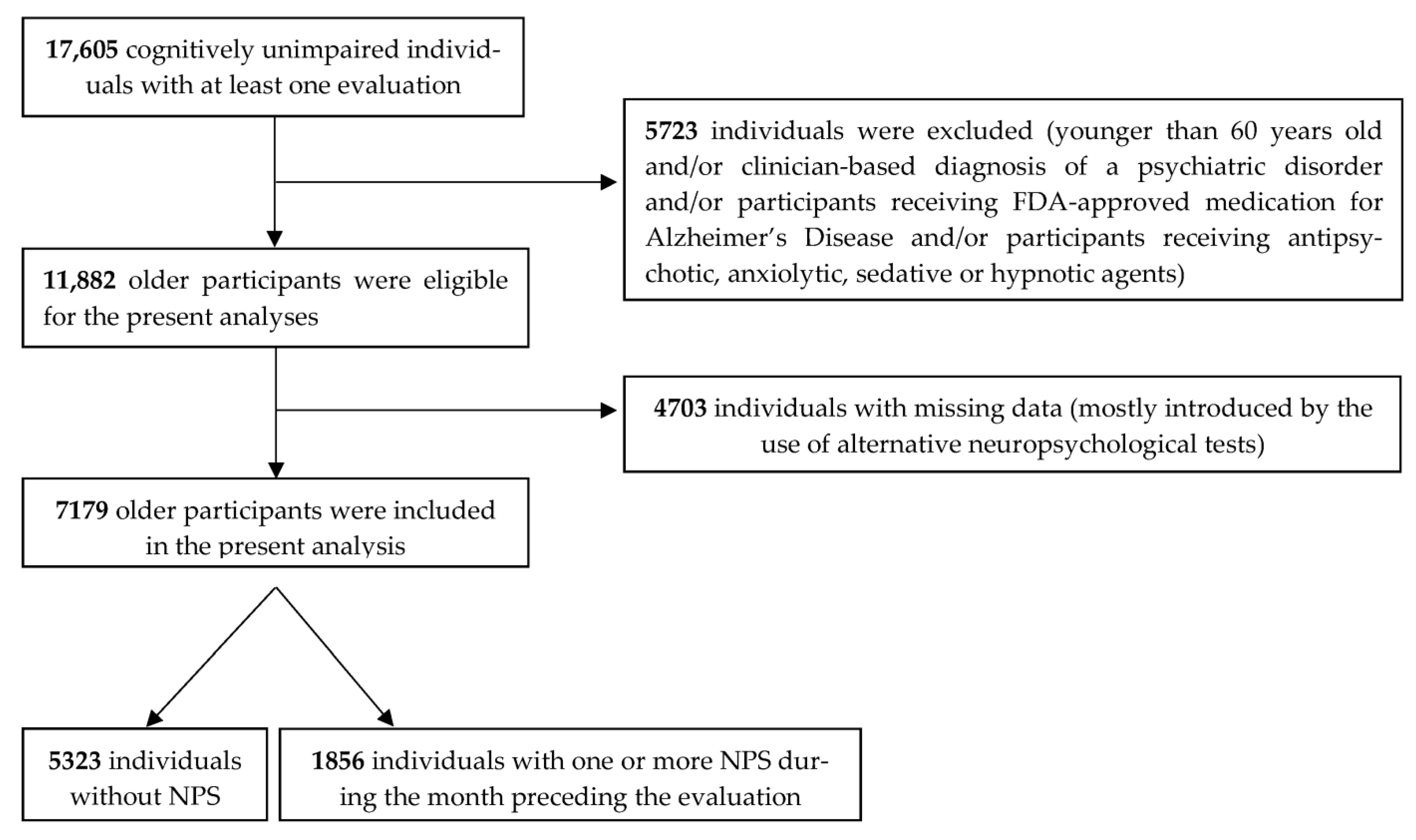
2.1. Eligibility Criteria and Selection of Older Cognitively Unimpaired Participants
2.2. Measurement of Neuropsychiatric Symptoms
2.3. Measurement of Cognitive Performance
2.4. Factors and Covariates Considered
2.5. Statistical Analysis
2.6. Supplementary Analyses
3. Results
3.1. Patient Characteristics and Missing Data
3.2. The Relationship between Neuropsychiatric Symptoms and Cognitive Performance in Older Cognitively Unimpaired Adults
4. Discussion
4.1. Strengths and Limitations
4.2. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lyketsos, C.G.; Lopez, O.; Jones, B.; Fitzpatrick, A.L.; Breitner, J.; DeKosky, S. Prevalence of Neuropsychiatric Symptoms in Dementia and Mild Cognitive Impairment: Results from the Cardiovascular Health Study. JAMA 2002, 288, 1475–1483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Martinez, M.; Molano, A.; Castro, J.; Zarranz, J.J. Prevalence of Neuropsychiatric Symptoms in Mild Cognitive Impairment and Alzheimers Disease, and its Relationship with Cognitive Impairment. Curr. Alzheimer Res. 2010, 7, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Siafarikas, N.; Selbaek, G.; Fladby, T.; Benth, J.; Auning, E.; Aarsland, D. Frequency and subgroups of neuropsychiatric symptoms in mild cognitive impairment and different stages of dementia in Alzheimer’s disease. Int. Psychogeriatr. 2018, 30, 103–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geda, Y.E.; Roberts, R.O.; Mielke, M.; Knopman, D.S.; Christianson, T.J.; Pankratz, V.S.; Boeve, B.F.; Sochor, O.; Tangalos, E.G.; Petersen, R.C.; et al. Baseline Neuropsychiatric Symptoms and the Risk of Incident Mild Cognitive Impairment: A Population-Based Study. Am. J. Psychiatry 2014, 171, 572–581. [Google Scholar] [CrossRef] [Green Version]
- Krell-Roesch, J.; Syrjanen, J.A.; Machulda, M.M.; Christianson, T.J.; Kremers, W.K.; Mielke, M.M.; Knopman, D.S.; Petersen, R.C.; Vassilaki, M.; Geda, Y.E. Neuropsychiatric symptoms and the outcome of cognitive trajectories in older adults free of dementia: The Mayo Clinic Study of Aging. Int. J. Geriatr. Psychiatry 2021, 36, 1362–1369. [Google Scholar] [CrossRef] [PubMed]
- Liew, T.M. Neuropsychiatric symptoms in cognitively normal older persons, and the association with Alzheimer’s and non-Alzheimer’s dementia. Alzheimer’s Res. Ther. 2020, 12, 35. [Google Scholar] [CrossRef]
- Wise, E.A.; Rosenberg, P.B.; Lyketsos, C.G.; Leoutsakos, J. Time course of neuropsychiatric symptoms and cognitive diagnosis in National Alzheimer’s Coordinating Centers volunteers. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2019, 11, 333–339. [Google Scholar] [CrossRef]
- Cummings, J.; Ritter, A.; Rothenberg, K. Advances in Management of Neuropsychiatric Syndromes in Neurodegenerative Diseases. Curr. Psychiatry Rep. 2019, 21, 79. [Google Scholar] [CrossRef] [Green Version]
- Mulsant, B.H.; Gharabawi, G.M.; Bossie, C.A.; Mao, L.; Martinez, R.A.; Tune, L.E.; Greenspan, A.J.; Bastean, J.N.; Pollock, B.G. Correlates of Anticholinergic Activity in Patients with Dementia and Psychosis Treated with Risperidone or Olanzapine. J. Clin. Psychiatry 2004, 65, 1708–1714. [Google Scholar] [CrossRef]
- Stewart, S.A. The effects of benzodiazepines on cognition. J. Clin. Psychiatry 2005, 66 (Suppl. S2), 9–13. [Google Scholar]
- Leng, Y.; Diem, S.J.; Stone, K.L.; Yaffe, K. Antidepressant Use and Cognitive Outcomes in Very Old Women. J. Gerontol. Ser. A 2018, 73, 1390–1395. [Google Scholar] [CrossRef] [PubMed]
- Lyketsos, C.G.; DelCampo, L.; Steinberg, M.; Miles, Q.; Steele, C.D.; Munro, C.; Baker, A.S.; Sheppard, J.-M.E.; Frangakis, C.; Brandt, J.; et al. Treating Depression in Alzheimer Disease: Efficacy and Safety of Sertraline Therapy, and the Benefits of Depression Reduction: The DIADS. Arch. Gen. Psychiatry 2003, 60, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Porsteinsson, A.P.; Drye, L.T.; Pollock, B.G.; Devanand, D.P.; Frangakis, C.; Ismail, Z.; Marano, C.; Meinert, C.L.; Mintzer, J.E.; Munro, C.A.; et al. Effect of Citalopram on Agitation in Alzheimer Disease. JAMA 2014, 311, 682–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassidy-Eagle, E.; Siebern, A.; Unti, L.; Glassman, J.; O’Hara, R. Neuropsychological Functioning in Older Adults with Mild Cognitive Impairment and Insomnia Randomized to CBT-I or Control Group. Clin. Gerontol. 2018, 41, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Kanellopoulos, D.; Rosenberg, P.; Ravdin, L.D.; Maldonado, D.; Jamil, N.; Quinn, C.; Kiosses, D.N. Depression, cognitive, and functional outcomes of Problem Adaptation Therapy (PATH) in older adults with major depression and mild cognitive deficits. Int. Psychogeriatr. 2020, 32, 485–493. [Google Scholar] [CrossRef]
- Morimoto, S.S.; Kanellopoulos, T.; Alexopoulos, G.S. Cognitive Impairment in Depressed Older Adults: Implications for Prognosis and Treatment. Psychiatr. Ann. 2014, 44, 138–142. [Google Scholar] [CrossRef] [Green Version]
- Orgeta, V.; Qazi, A.; Spector, A.E.; Orrell, M. Psychological treatments for depression and anxiety in dementia and mild cognitive impairment. Cochrane Database Syst. Rev. 2014, 22, CD009125. [Google Scholar] [CrossRef]
- Rostamzadeh, A.; Kahlert, A.; Kalthegener, F.; Jessen, F. Psychotherapeutic interventions in individuals at risk for Alzheimer’s dementia: A systematic review. Alzheimer’s Res. Ther. 2022, 14, 18. [Google Scholar] [CrossRef]
- Burhanullah, M.H.; Tschanz, J.T.; Peters, M.E.; Leoutsakos, J.-M.; Matyi, J.; Lyketsos, C.G.; Nowrangi, M.A.; Rosenberg, P.B. Neuropsychiatric Symptoms as Risk Factors for Cognitive Decline in Clinically Normal Older Adults: The Cache County Study. Am. J. Geriatr. Psychiatry 2020, 28, 64–71. [Google Scholar] [CrossRef]
- Creese, B.; Brooker, H.; Ismail, Z.; Wesnes, K.A.; Hampshire, A.; Khan, Z.; Megalogeni, M.; Corbett, A.; Aarsland, D.; Ballard, C. Mild Behavioral Impairment as a Marker of Cognitive Decline in Cognitively Normal Older Adults. Am. J. Geriatr. Psychiatry 2019, 27, 823–834. [Google Scholar] [CrossRef] [Green Version]
- Köhler, S.; Allardyce, J.; Verhey, F.R.; McKeith, I.G.; Matthews, F.; Brayne, C.; Savva, G.M. Cognitive Decline and Dementia Risk in Older Adults with Psychotic Symptoms: A Prospective Cohort Study. Am. J. Geriatr. Psychiatry 2013, 21, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Beekly, D.L.; Ramos, E.M.; Lee, W.W.; Deitrich, W.D.; Jacka, M.E.; Wu, J.; Hubbard, J.L.; Koepsell, T.D.; Morris, J.C.; Kukull, W.A. The National Alzheimer’s Coordinating Center (NACC) Database: The Uniform Data Set. Alzheimer Dis. Assoc. Disord. 2007, 21, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.C.; Weintraub, S.; Chui, H.C.; Cummings, J.; DeCarli, C.; Ferris, S.; Foster, N.L.; Galasko, D.; Graff-Radford, N.; Peskind, E.R.; et al. The Uniform Data Set (UDS): Clinical and Cognitive Variables and Descriptive Data from Alzheimer Disease Centers. Alzheimer Dis. Assoc. Disord. 2006, 20, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, S.; Salmon, D.; Mercaldo, N.; Ferris, S.; Graff-Radford, N.R.; Chui, H.; Cummings, J.; DeCarli, C.; Foster, N.L.; Galasko, D.; et al. The Alzheimer’s Disease Centers’ Uniform Data Set (UDS). Alzheimer Dis. Assoc. Disord. 2009, 23, 91–101. [Google Scholar] [CrossRef]
- McKeith, I.G.; Dickson, D.W.; Lowe, J.; Emre, M.; O’Brien, J.T.; Feldman, H.; Cummings, J.; Duda, J.E.; Lippa, C.; Perry, E.K.; et al. Diagnosis and management of dementia with Lewy bodies: Third report of the DLB consortium. Neurology 2005, 65, 1863–1872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKhann, G.; Drachman, D.; Folstein, M.; Katzman, R.; Price, D.; Stadlan, E.M. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology 1984, 34, 939–944. [Google Scholar] [CrossRef] [Green Version]
- Neary, D.; Snowden, J.S.; Gustafson, L.; Passant, U.; Stuss, D.; Black, S.; Freedman, M.; Kertesz, A.; Robert, P.H.; Albert, M.; et al. Frontotemporal lobar degeneration: A consensus on clinical diagnostic criteria. Neurology 1998, 51, 1546–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild Cognitive Impairment: Clinical characterization and outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef]
- Roman, G.C.; Tatemichi, T.K.; Erkinjuntti, T.; Cummings, J.L.; Masdeu, J.C.; Garcia, J.H.; Amaducci, L.; Orgogozo, J.-M.; Brun, A.; Hofman, A.; et al. Vascular dementia: Diagnostic criteria for research studies: Report of the NINDS-AIREN International Workshop. Neurology 1993, 43, 250–260. [Google Scholar] [CrossRef]
- Winblad, B.; Palmer, K.; Kivipelto, M.; Jelic, V.; Fratiglioni, L.; Wahlund, L.-O.; Nordberg, A.; Backman, L.J.; Albert, M.S.; Almkvist, O.; et al. Mild cognitive impairment—Beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 2004, 256, 240–246. [Google Scholar] [CrossRef]
- Kaufer, D.I.; Cummings, J.L.; Ketchel, P.; Smith, V.; Macmillan, A.; Shelley, T.; Lopez, O.L.; DeKosky, S.T. Validation of the NPI-Q, a Brief Clinical Form of the Neuropsychiatric Inventory. J. Neuropsychiatry Clin. Neurosci. 2000, 12, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Leoutsakos, J.-M.S.; Forrester, S.N.; Lyketsos, C.G.; Smith, G.S. Latent Classes of Neuropsychiatric Symptoms in NACC Controls and Conversion to Mild Cognitive Impairment or Dementia. J. Alzheimer’s Dis. 2015, 48, 483–493. [Google Scholar] [CrossRef] [Green Version]
- Wechsler, D. WMS-R: Wechsler Memory Scale-Revised; Psychological Corporation: San Antonio, TX, USA, 1987. [Google Scholar]
- Morris, J.C.; Heyman, A.; Mohs, R.C.; Hughes, J.P.; van Belle, G.; Fillenbaum, G.; Mellits, E.D.; Clark, C. The consortium to establish a registry for Alzheimer’s disease (CERAD). Part I. Clinical and neuropsychological assessment of Alzheimer’s disease. Neurology 1989, 39, 1159–1165. [Google Scholar]
- Goodglass, H.; Kaplan, E.; Weintraub, S. BDAE: The Boston Diagnostic Aphasia Examination; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2001. [Google Scholar]
- Hultsch, D.F.; Strauss, E.; Hunter, M.A.; MacDonald, S.W.S.; Craik, F.I.M.; Salthouse, T.A. The Handbook of Aging and Cognition; Psychology Press: Hove, UK, 2008. [Google Scholar]
- Beaudreau, S.A.; O’Hara, R. The association of anxiety and depressive symptoms with cognitive performance in community-dwelling older adults. Psychol. Aging 2009, 24, 507–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parra-Díaz, A.B.; Aibar-Almazán, A.; Martínez-Amat, A.; Jiménez-García, J.D.; Álvarez-Salvago, F.; Hita-Contreras, F. Associations of Sleep Quality, Anxiety, and Depression with Cognitive and Executive Functions among Community-Dwelling Women Aged ≥65 Years: A Cross-Sectional Study. Healthcare 2021, 9, 1599. [Google Scholar] [CrossRef]
- Yochim, B.P.; Mueller, A.E.; Segal, D.L. Late life anxiety is associated with decreased memory and executive functioning in community dwelling older adults. J. Anxiety Disord. 2013, 27, 567–575. [Google Scholar] [CrossRef]
- Derakhshan, N.; Eysenck, M.W. Anxiety, Processing Efficiency, and Cognitive Performance: New Developments from Attentional Control Theory. Eur. Psychol. 2009, 14, 168–176. [Google Scholar] [CrossRef]
- Wetherell, J.L.; Reynolds, C.A.; Gatz, M.; Pedersen, N.L. Anxiety, Cognitive Performance, and Cognitive Decline in Normal Aging. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2002, 57, P246–P255. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, K.; Ryali, V.; Prakash, J.; Bhat, P.S.; Shashikumar, R.; Khan, S. Neuropsychophysiological correlates of depression. Ind. Psychiatry J. 2010, 19, 82–89. [Google Scholar] [CrossRef]
- Sannemann, L.; Schild, A.-K.; Altenstein, S.; Bartels, C.; Brosseron, F.; Buerger, K.; Cosma, N.C.; Fliessbach, K.; Freiesleben, S.D.; Glanz, W.; et al. Neuropsychiatric symptoms in at-risk groups for AD dementia and their association with worry and AD biomarkers—Results from the DELCODE study. Alzheimer’s Res. Ther. 2020, 12, 131. [Google Scholar] [CrossRef]
- Johns, E.K.; Phillips, N.A.; Belleville, S.; Goupil, D.; Babins, L.; Kelner, N.; Ska, B.; Gilbert, B.; Inglis, G.; Panisset, M.; et al. Executive functions in frontotemporal dementia and Lewy body dementia. Neuropsychology 2009, 23, 765–777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botzung, A.; Mondino, M.; Noblet, V.; Philippi, N.; Blanc, F. Attention processing speed impairment in early dementia with Lewy bodies correlates with white matter damage on volumetric and diffusion tensor imaging: Neuroimaging/multi-modal comparisons. Alzheimer’s Dement. 2020, 16, e042729. [Google Scholar] [CrossRef]
- Daalman, K.; van Zandvoort, M.; Bootsman, F.; Boks, M.; Kahn, R.; Sommer, I. Auditory verbal hallucinations and cognitive functioning in healthy individuals. Schizophr. Res. 2011, 132, 203–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michie, P.T.; Badcock, J.C.; Waters, F.A.V.; Maybery, M. Auditory hallucinations: Failure to inhibit irrelevant memories. Cogn. Neuropsychiatry 2005, 10, 125–136. [Google Scholar] [CrossRef]
- Soriano, M.F.; Jiménez, J.F.; Román, P.; Bajo, M.T. Intentional inhibition in memory and hallucinations: Directed forgetting and updating. Neuropsychology 2009, 23, 61–70. [Google Scholar] [CrossRef] [Green Version]
- Harvey, P.D.; Rosenthal, J.B. Cognitive and functional deficits in people with schizophrenia: Evidence for accelerated or exaggerated aging? Schizophr. Res. 2018, 196, 14–21. [Google Scholar] [CrossRef]
- Mathias, S.R.; Knowles, E.E.M.; Barrett, J.; Leach, O.; Buccheri, S.; Beetham, T.; Blangero, J.; Poldrack, R.A.; Glahn, D.C. The Processing-Speed Impairment in Psychosis Is More Than Just Accelerated Aging. Schizophr. Bull. 2017, 43, 814–823. [Google Scholar] [CrossRef] [Green Version]
- Thuaire, F.; Rondepierre, F.; Vallet, G.T.; Jalenques, I.; Izaute, M. Executive deficits in schizophrenia: Mediation by processing speed and its relationships with aging. Psychol. Med. 2020, 52, 1126–1134. [Google Scholar] [CrossRef]
- Boeve, A.; Halpin, A.; Michaud, S.; Fagan, M.; MacAulay, R.K. Specific Sleep Health Domains as Predictors of Executive Function in Older Adults. J. Neuropsychiatry Clin. Neurosci. 2022, 34, 422–427. [Google Scholar] [CrossRef]
- Dzierzewski, J.M.; Dautovich, N.; Ravyts, S. Sleep and Cognition in Older Adults. Sleep Med. Clin. 2018, 13, 93–106. [Google Scholar] [CrossRef]
- Lü, W.; Duan, J.; Zhang, W.; Yang, W.; Yu, W. Relationship between neuropsychiatric symptoms and cognitive functions in patients with cognitive impairment. Psychogeriatrics 2021, 21, 773–782. [Google Scholar] [CrossRef] [PubMed]
- Liampas, I.; Hatzimanolis, A.; Siokas, V.; Yannakoulia, M.; Kosmidis, M.H.; Sakka, P.; Hadjigeorgiou, G.M.; Scarmeas, N.; Dardiotis, E. Antihypertensive Medication Class and the Risk of Dementia and Cognitive Decline in Older Adults: A Secondary Analysis of the Prospective HELIAD Cohort. J. Alzheimer’s Dis. 2022, 89, 709–719. [Google Scholar] [CrossRef] [PubMed]
- Folia, V.; Liampas, I.; Ntanasi, E.; Yannakoulia, M.; Sakka, P.; Hadjigeorgiou, G.; Scarmeas, N.; Dardiotis, E.; Kosmidis, M.H. Longitudinal trajectories and normative language standards in older adults with normal cognitive status. Neuropsychology 2022, 36, 626–639. [Google Scholar] [CrossRef] [PubMed]
- Liampas, I.; Folia, V.; Ntanasi, E.; Yannakoulia, M.; Sakka, P.; Hadjigeorgiou, G.; Scarmeas, N.; Dardiotis, E.; Kosmidis, M.H. Longitudinal episodic memory trajectories in older adults with normal cognition. Clin. Neuropsychol. 2022, 1–18. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Without NPS (n = 5323) | With NPS (n = 1856) | p-Value |
|---|---|---|---|
| Age in years | 73.63 ± 7.81 | 73.65 ± 7.87 | 0.913 |
| Formal education in years | 15.72 ± 2.94 | 15.42 ± 3.11 | <0.001 |
| Sex (male/female) | 1788 (33.6%)/3535 (66.4%) | 762 (41.1%)/1094 (58.9%) | <0.001 |
| Race (Caucasian/African American/American Indian or Alaska Native/Native Hawaiian or Pacific Islander/Asian/Multiracial) | 4130 (77.5%)/916 (17.2%)/14 (0.3%)/3 (0.1%)/120 (2.3%)/140 (2.6%) | 1580 (85.1%)/190 (10.2%)/8 (0.4%)/1 (0.1%)/22 (2.2%)/55 (3.0%) | <0.001 |
| Cardiovascular disease (No/Yes) | 4748 (89.2%)/575 (10.8%) | 1608 (86.6%)/248 (13.4%) | 0.003 |
| Cerebrovascular disease (No/Yes) | 5028 (94.5%)/295 (5.5%) | 1706 (91.9%)/150 (8.1%) | <0.001 |
| Parkinson’s disease (No/Yes) | 5293 (99.4%)/30 (0.6%) | 1810 (97.5%)/46 (2.5%) | <0.001 |
| Traumatic brain injury (No/Yes) | 4896 (92.0%)/427 (8.0%) | 1662 (89.5%)/194 (10.5%) | 0.001 |
| History of seizures (No/Yes) | 5237 (98.5%)/82 (1.5%) | 1826 (98.5%)/27 (1.5%) | 0.798 |
| Thyroid disease (No/Yes) | 4324 (81.4%)/990 (18.6%) | 1508 (81.3%)/348 (18.7%) | 0.909 |
| B12 deficiency (No/Yes) | 5146 (96.7%)/177 (3.3%) | 1771 (95.4%)/85 (4.6%) | 0.013 |
| Alcohol abuse (No/Yes) | 5221 (98.1%)/102 (1.9%) | 1774 (95.6%)/82 (4.4%) | <0.001 |
| Other substance abuse (No/Yes) | 5289 (99.4%)/34 (0.6%) | 1835 (98.9%)/21 (1.1%) | 0.036 |
| Current antidepressant use (No/Yes) | 4844 (91.0%)/479 (9.0%) | 1547 (83.4%)/309 (16.6%) | <0.001 |
| Episodic memory (sum of items recalled in the immediate and delayed recall tasks) | 25.66 ± 7.71 | 24.55 ± 7.71 | <0.001 |
| Language (sum of word production in the animals and vegetables lists) | 34.61 ± 8.57 | 33.70 ± 8.16 | <0.001 |
| Semantic Memory (BNT-30) | 26.94 ± 3.41 | 27.09 ± 3.15 | 0.104 |
| Attention (sum of longest sequences in DST forward & backward conditions) | 11.58 ± 1.99 | 11.50 ± 1.99 | 0.139 |
| Processing speed (TMT-A seconds) | 35.15 ± 15.27 | 35.68 ± 17.20 | 0.212 |
| Executive function (TMT-B seconds) | 93.04 ± 50.88 | 96.25 ± 53.65 | 0.021 |
| NPS | Episodic Memory | Language | Semantic Memory | Attentio | Processing Speed | Executive Function | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | p | B | p | B | p | B | p | B | p | B | p | ||
| Depression | 0 | 0.145 | 0.844 | 0.398 | 0.610 | −0.382 | 0.202 | 0.028 | 0.887 | 1.476 | 0.314 | 2.080 | 0.645 |
| 1 | −0.165 | 0.832 | −0.018 | 0.982 | −0.140 | 0.656 | 0.157 | 0.445 | 2.872 | 0.063 | 4.381 | 0.357 | |
| 2 | Ref | Ref | Ref | Ref | Ref | Ref | |||||||
| Anxiety | 0 | 1.205 | 0.100 | −0.679 | 0.379 | 0.966 (1) | 0.001 | 0.387 (3) | 0.046 | −1.533 | 0.291 | −10.220 (4) | 0.022 |
| 1 | 0.345 | 0.670 | −1.641 | 0.055 | 0.816 (2) | 0.013 | 0.286 | 0.183 | −1.530 | 0.341 | −6.187 | 0.211 | |
| 2 | Ref | Ref | Ref | Ref | Ref | Ref | |||||||
| Agitation | 0 | 0.437 | 0.619 | −0.099 | 0.915 | −0.323 | 0.365 | 0.059 | 0.802 | −0.599 | 0.731 | −0.306 | 0.955 |
| 1 | 0.708 | 0.454 | 0.079 | 0.937 | −0.168 | 0.662 | 0.018 | 0.944 | −3.146 | 0.094 | −7.669 | 0.185 | |
| 2 | Ref | Ref | Ref | Ref | Ref | Ref | |||||||
| Apathy | 0 | 0.922 | 0.437 | 1.687 | 0.178 | −0.048 | 0.920 | 0.198 | 0.529 | −0.697 | 0.767 | −1.510 | 0.835 |
| 1 | 0.283 | 0.824 | 0.760 | 0.573 | −0.312 | 0.547 | 0.066 | 0.846 | 0.780 | 0.758 | 2.161 | 0.782 | |
| 2 | Ref | Ref | Ref | Ref | Ref | Ref | |||||||
| Disinhibition | 0 | 0.439 | 0.724 | −0.209 | 0.874 | 0.168 | 0.740 | −0.023 | 0.944 | 1.012 | 0.682 | −9.822 | 0.197 |
| 1 | −0.285 | 0.838 | −0.413 | 0.779 | −0.375 | 0.508 | 0.260 | 0.482 | 0.142 | 0.959 | −12.496 | 0.143 | |
| 2 | Ref | Ref | Ref | Ref | Ref | Ref | |||||||
| Irritability | 0 | 0.586 | 0.403 | −0.320 | 0.665 | −0.113 | 0.690 | −0.162 | 0.384 | −2.652 | 0.056 | −2.918 | 0.495 |
| 1 | 0.452 | 0.538 | −0.371 | 0.632 | −0.044 | 0.883 | −0.227 | 0.244 | −2.430 | 0.095 | −1.893 | 0.673 | |
| 2 | Ref | Ref | Ref | Ref | Ref | Ref | |||||||
| Night-time | 0 | 0.373 | 0.519 | 0.552 | 0.366 | 0.134 | 0.570 | 0.076 | 0.621 | 1.033 | 0.368 | 4.938 | 0.163 |
| 1 | −0.292 | 0.655 | 0.387 | 0.575 | 0.195 | 0.462 | −0.025 | 0.885 | 0.789 | 0.543 | 6.174 | 0.122 | |
| 2 | Ref | Ref | Ref | Ref | Ref | Ref | |||||||
| Appetite | 0 | 0.233 | 0.777 | 1.381 | 0.112 | 0.608 | 0.069 | 0.137 | 0.529 | −2.717 | 0.096 | −9.708 | 0.054 |
| 1 | −0.336 | 0.715 | 1.093 | 0.260 | 0.428 | 0.251 | 0.089 | 0.714 | −1.296 | 0.477 | −0.913 | 0.871 | |
| 2 | Ref | Ref | Ref | Ref | Ref | Ref | |||||||
| Elation | No | 0.565 | 0.613 | 0.509 | 0.666 | 0.069 | 0.880 | 0.764 (5) | 0.010 | −2.484 | 0.263 | −3.593 | 0.599 |
| Yes | Ref | Ref | Ref | Ref | Ref | Ref | |||||||
| Motor | No | 1.339 | 0.152 | 2.129 (6) | 0.031 | −0.225 | 0.554 | 0.085 | 0.732 | 1.752 | 0.345 | −0.173 | 0.976 |
| Yes | Ref | Ref | Ref | Ref | Ref | Ref | |||||||
| Delusions | No | 0.866 | 0.479 | 0.845 | 0.513 | 0.437 | 0.378 | 0.415 | 0.200 | −2.535 | 0.296 | −4.524 | 0.545 |
| Yes | Ref | Ref | Ref | Ref | Ref | Ref | |||||||
| Hallucinations | No | 3.692 | 0.094 | 0.015 | 0.995 | 0.324 | 0.717 | 0.125 | 0.830 | −10.272 (7) | 0.019 | −43.103 (8) | 0.001 |
| Yes | Ref | Ref | Ref | Ref | Ref | Ref | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liampas, I.; Siokas, V.; Lyketsos, C.G.; Dardiotis, E. The Relationship between Neuropsychiatric Symptoms and Cognitive Performance in Older Adults with Normal Cognition. Medicina 2022, 58, 1586. https://doi.org/10.3390/medicina58111586
Liampas I, Siokas V, Lyketsos CG, Dardiotis E. The Relationship between Neuropsychiatric Symptoms and Cognitive Performance in Older Adults with Normal Cognition. Medicina. 2022; 58(11):1586. https://doi.org/10.3390/medicina58111586
Chicago/Turabian StyleLiampas, Ioannis, Vasileios Siokas, Constantine George Lyketsos, and Efthimios Dardiotis. 2022. "The Relationship between Neuropsychiatric Symptoms and Cognitive Performance in Older Adults with Normal Cognition" Medicina 58, no. 11: 1586. https://doi.org/10.3390/medicina58111586
APA StyleLiampas, I., Siokas, V., Lyketsos, C. G., & Dardiotis, E. (2022). The Relationship between Neuropsychiatric Symptoms and Cognitive Performance in Older Adults with Normal Cognition. Medicina, 58(11), 1586. https://doi.org/10.3390/medicina58111586