
Neurodevelopmental Outcomes among Brazilian Children with Cyanotic Congenital Heart Disease and Its Associated Factors

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
2.2. Sample and Study Site
- (1)
- All study participants were between 5 and 11 years, 11 months old;
- (2)
- All participants were previously being followed up at the pediatric cardiology or pediatric outpatient clinics of the HU-FURG;
- (3)
- Patients with CHD were only included in the survey after confirmation of the diagnosis through pediatric Doppler echocardiography, (tetralogy of Fallot—37.8%; transposition of great vessels—18.9%; pulmonary atresia—16.2%; tricuspid atresia—13.5%; tricuspid atresia with RV hypoplasia—8.1%; and cyanotic complex heart disease—5.4%);
- (4)
- The volunteers in the control group came from the pediatric outpatient clinic, and only those who were exclusively in childcare consultations were included.
- (1)
- Participants who had associated syndromes that could interfere with the results of neurodevelopment tests or chronic cyanotic diseases were excluded;
- (2)
- Participants who were not within the age group established above were excluded;
- (3)
- Participants who did not complete all stages of the research were excluded.
2.3. Socioeconomic, Demographic, and Clinical Data
2.4. Dependent Variables
2.4.1. Motor Development
2.4.2. Nonverbal Intelligence
2.4.3. Attention Deficit
2.5. Data Analysis
3. Results
3.1. Sociodemographic Questionnaire
3.2. Motor Development Scale
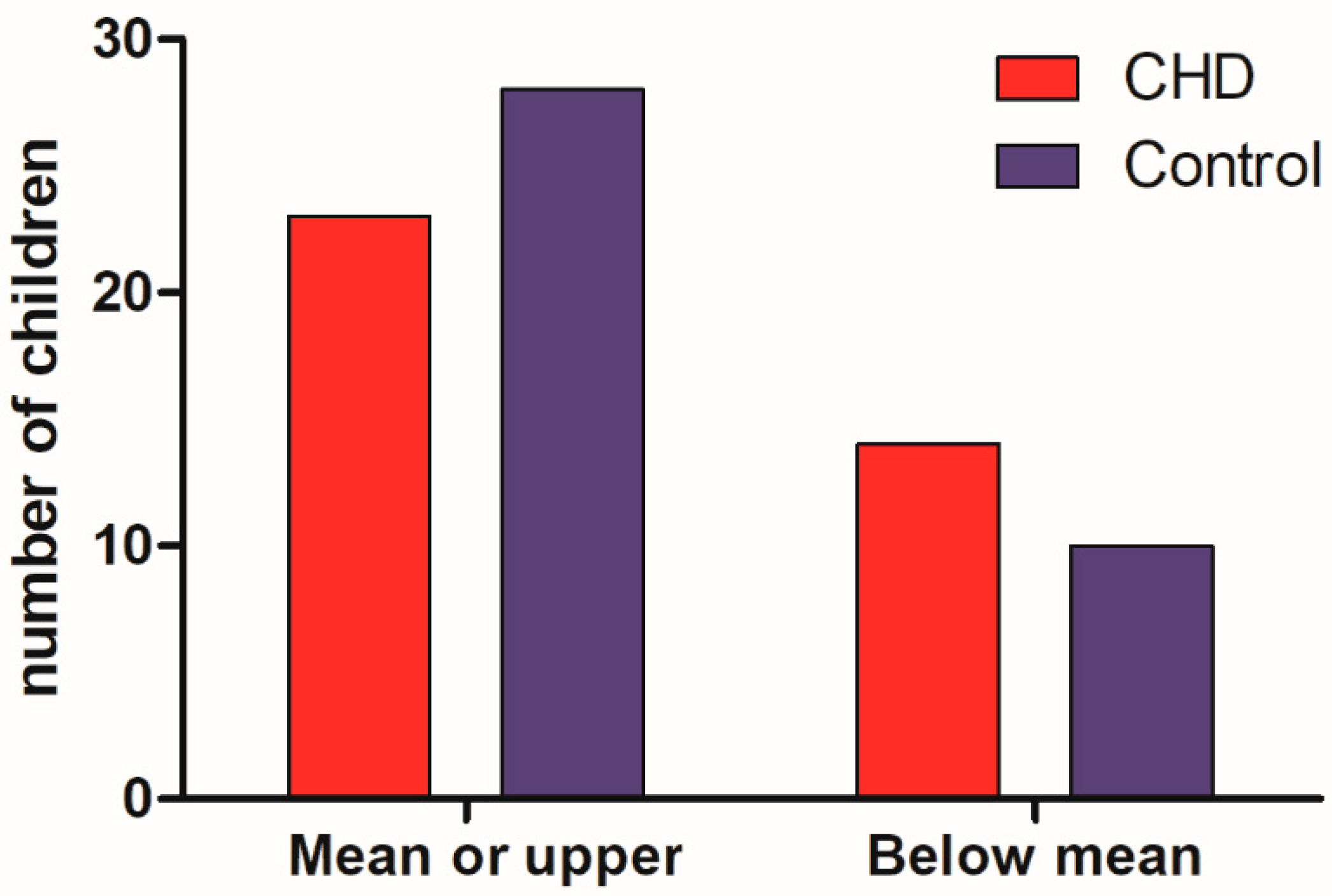
3.3. R-2 Nonverbal Intelligence Test
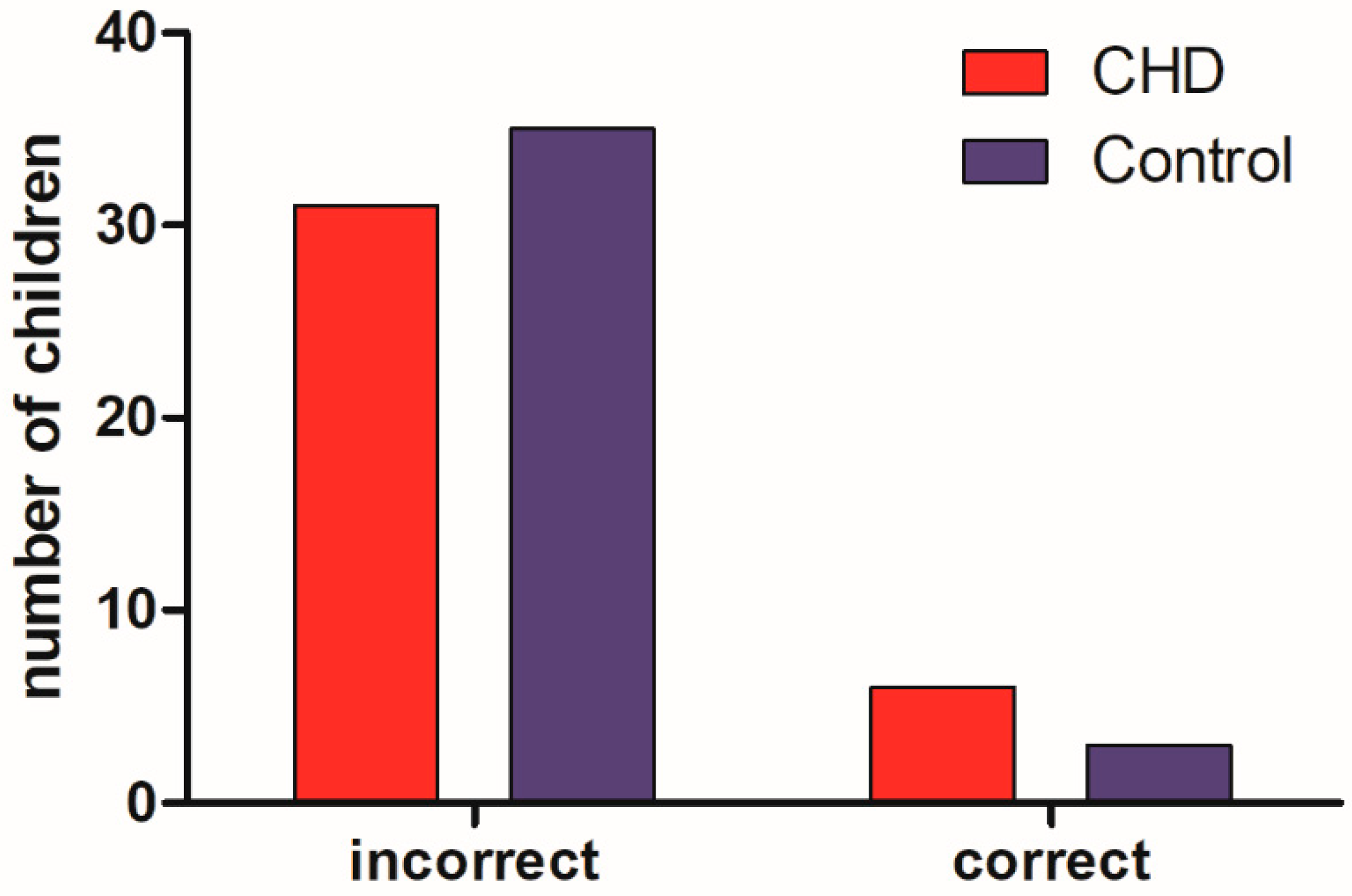
3.4. Attention Deficit Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sun, R.; Liu, M.; Lu, L.; Zheng, Y.; Zhang, P. Congenital heart disease: Causes, diagnosis, symptoms, and treatments. Cell Biochem. Biophys. 2015, 72, 857–860. [Google Scholar] [CrossRef] [PubMed]
- Paula, Í.R.; Oliveira, J.C.S.; Batista, A.C.F.; Nascimento, L.C.S.; Araújo, L.B.D.; Ferreira, M.B.; Gomes, M.B.; Vmgdo, A. Influência da cardiopatia congênita no desenvolvimento lactentes. Fisioter Pesqui 2020, 27, 41–47. [Google Scholar] [CrossRef]
- da Silva, E.M.; de Olinda, A.G.; Barros, F.H.V.; Roseno, M.A.S.G. Óbitos por Anomalias Congênitas do Coração e Circulatório no Estado do Pará nos anos de 2007 a 2017: Revisão Sistemática da Literatura. Rev. Psicol. 2018, 12, 823–831. [Google Scholar] [CrossRef] [Green Version]
- Braunwald, E.; Zipes, D.P.; Libby, P. Tratado de Medicina Cardiovascular Braunwald; Roca: São Paulo, Brazil, 2003. [Google Scholar]
- Aragão, J.A.; Mendonça, M.P.; Silva, M.S.; Moreira, A.N.; Aragão, M.E.C.S.; Reis, F.P. O perfil epidemiológico dos pacientes com cardiopatias congênitas submetidos à cirurgia no Hospital do Coração. Rev. Bras. Ciênc. Saúde 2013, 17, 263–268. [Google Scholar] [CrossRef]
- Belo, W.A.; Oselame, G.B.; Neves, E.B. Clinical-hospital profile of children with congenital heart disease. Cad. Saúde Coletiva 2016, 24, 216–220. [Google Scholar] [CrossRef] [Green Version]
- Frota, M.A.; Andrade, S.I.; Santos, Z.M.S.A.; Silva, C.A.B.F.A.; Frota, M.A.; Andrade, S.I.; Santos, Z.M.S.A.; Silva, C.A.B.; Carvalho, A.F. Perfil sociodemográfico familiar e clínico de crianças com cardiopatiacongênita atendidasem uma instituição hospitalar. Rev. Bras. Promoção Saúde 2014, 27, 239–246. [Google Scholar] [CrossRef]
- Amorim, L.F.P.; Pires, C.A.B.; Lana, A.M.A.; Campos, A.S.; Aguiar, R.A.L.P.; Tibúrcio, J.D.; Siqueira, A.L.; Mota, C.C.C.; Aguiar, M.J.B. Presentation of Congenital Heart Disease Diagnosed at Birth: Analysis of 29,770 Newborn Infants. J. Pediatr. 2008, 84, 83–90. Available online: http://www.jped.com.br/conteudo/Ing_resumo.asp?varArtigo=1749&cod=&idSecao=1 (accessed on 15 April 2022). [CrossRef] [Green Version]
- Simão, A.F.; Precoma, D.B.; Andrade, J.P.; Correa Filho, H.; Saraiva, J.F.K.; Oliveira, G.M.M.; Murro, A.B.M.; Campos, A.; Alessi, A.; Souza, W.K.S.B.; et al. I Brazilian guidelines on cardiovascular prevention. Arq. Bras. Cardiol. 2013, 101, 1–63. [Google Scholar] [CrossRef]
- Robles-Vizcaíno, M.C.; Poo-Argüelles, M.P.P.-O.M. Atención Temprana: Recursos y Pautas de Intervención en Niños de Riesgo o Con Retrasos del Desarrollo; Narbona-García, J., Casas-Fernández, C., Eds.; Coords. Protocolos de neurología; Protoc la Association Española Pediatría Madrid AEP/SENEP: Madrid, Spain, 2008; pp. 278–285. [Google Scholar]
- Castro, P.S. Avaliação do Desenvolvimento Neuropsicomotor de Crianças Com Cardiopatias Congênitas; SEMPESq-Semana Pesqui da Unit-Alagoas: Alagoas, Brasil, 2017; p. 5. [Google Scholar]
- Caçola, P.M.; Gabbard, C.; Montebelo, M.I.; Santos, D.C. Further development and validation of the affordances in the home environment for motor development–infant scale (AHEMD-IS). Phys. Ther. 2015, 95, 901–923. [Google Scholar] [CrossRef] [Green Version]
- de Fátima Dornelas, L.; de Castro Duarte, N.M.; de Castro Magalhães, L. Atraso do desenvolvimento neuropsicomotor: Mapa conceitual, definições, usos e limitações do termo. Rev. Paul. Pediatr. 2015, 33, 88–103. [Google Scholar] [CrossRef]
- Salamanca-Zarzuela, B.; Morales-Luego, F.; Alcalde-Martin, C.; Centeno-Malfaz, F. Desenvolvimento psicomotor em pacientes com cardiopatia congênita grave. Rev. Neurol. 2018, 66, 409–414. [Google Scholar] [PubMed]
- Herberg, U.; Hövels-Gürich, H. Neurologische Und Psychomotorische Entwicklung von Feten Und Neugeborenen mit Angeborenen Herzfehlern-Ursachen Und Prävalenz von Störungen im Langzeitverlauf. Z Geburtshilfe Neonatol. 2012, 216, 132–140. Available online: http://www.thieme-connect.de/DOI/DOI?10.1055/s-0032-1312670 (accessed on 22 May 2022). [CrossRef] [PubMed]
- Moraes, B.R.; Bassi, D.; dos Santos, P.H.M.; Santos-de-Araújo, A.D.; de Souza, P.H.V.A.; do Nascimento Calles, A.C. Desenvolvimento neuropsicomotor de crianças com cardiopatias congênitas. Rev. Pesqui Fisioter 2019, 9, 316–320. [Google Scholar] [CrossRef]
- de Sousa Amorim, M.; Guimarães Filho, G.C.; Fernandes, N.A.; do Lopes, I.C.L.; Cabral, F.R.S.; Guimarães, A.M.; Ribeiro, L.O. The reality of congenital heart disease in Brazil: Bibliographic review. Braz. J. Health Rev. 2021, 4, 19378–19388. [Google Scholar] [CrossRef]
- Rosa Neto, F. Escala de Desenvolvimento Motor (EDM): Manual de Avaliação Motora; Artmed: Porto Alegre, Brazil, 2002. [Google Scholar]
- Okuda, P.M.M.; Erika, F.; Cogo-Moreira, H.; Liu, T.; Surkan, P.J.; Martins, S.S.; Caetano, S.C. Construct validity of the Motor Development Scale (MDS). Trends Psychiatry Psychother. 2020, 42, 82–85. [Google Scholar] [CrossRef]
- Martins Luz, M.; Alexandre Felício Brito, C.; Natacha Ferreira Batista, J.; Moura Lourenço, P. A Utilização Da Escala De Desenvolvimento Motor (Edm) E A Sua Aplicação Na Fase Escolar: Uma Realidade Brasileira? Rev. Estud. Apl. Em Educ. 2018, 3, 5. [Google Scholar] [CrossRef] [Green Version]
- Iara Socorro Martins, M.; Aguiar Moraes Vitoriano, N.; Azevedo Martins, C.; Mendes Carvalho, E.; de Moura Jucá, R.V.B.; Jamill e Simões Ferreira, S.M.A.; Gardano Bucharles Mont’Alverne, H. Daniela Aspects of motor development and quality of life in the context of child obesity. J. Hum. Growth Dev. 2021, 31, 58–65. [Google Scholar] [CrossRef]
- Rosa, H.R. R-2: Teste não-verbal de inteligência para crianças-Pesquisa Piloto com crianças da cidade de São Paulo. Rev. Vetor 2003, 4, 18–25. [Google Scholar]
- Rosa, H.R.; Pires ML, N.; Alves IC, B.; Esteves, C. Estudo normativo do R-2: Teste não verbal de inteligência para crianças. Bol. Acad. Paul. Psicol. 2013, 33, 373–387. [Google Scholar]
- de Oliveira Leite, I.C.; Casado, C.D.C.C. O Uso do Teste de Inteligência Não Verbal (R-2) Em Crianças Com Diagnóstico de Transtorno do Espectro Autista (Tea): Um Estudo Exploratório. Rev. Ibero-Am. Humanid. Ciências E Educ. 2022, 8, 1339–1359. [Google Scholar]
- de Macedo, E.C.; Mecca, T.P.; Valentini, F.; Laros, J.A.; de Lima, R.M.F.; Schwartzman, J.S. Utilizando o teste não verbal de inteligência SON-R 2 1/2-7 [a] para avaliar crianças com Transtornos do Espectro do Autismo. Rev. Educ. Espec. 2013, 26, 603–617. [Google Scholar] [CrossRef] [Green Version]
- Alves, I.C.B.; Rosa, H.R. Relação do teste de Bender (avaliação Koppitz) com o R-2: Teste não verbal de inteligência para crianças. Psicol. Teor. E Prática 2012, 14, 153–167. [Google Scholar]
- Smits-Engelsman, B.; Hill, E.L. The relationship between motor coordination and intelligence across the IQ range. Pediatrics 2012, 130, e950–e956. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyttälä, M.; Lehto, J.E. Some factors underlying mathematical performance: The role of visuospatial working memory and non-verbal intelligence. Eur. J. Psychol. Educ. 2008, 23, 77–94. [Google Scholar] [CrossRef]
- Matos, P.; Serra-Pinheiro, M.A.; Rohde, L.A.; Pinto, D. Apresentação de uma versão em português para uso no Brasil do instrumento MTA-SNAP-IV de avaliação de sintomas de transtorno do déficit de atenção/hiperatividade e sintomas de transtorno desafiador e de oposição. Rev. Psiquiatr. RS 2006, 3, 290–297. [Google Scholar] [CrossRef]
- Hövels-Gürich, H. Psychomotor and cognitive development and quality of life in children and adolescents with congenital heart disease. Klin. Pädiatr. 2019, 231, 183–190. [Google Scholar]
- Hall Charlotte, L.; Guo, B.; Valentine Althea, Z.; Groom Madeline, J.; Daley, D.; Sayal, K.; Hollis, C. The Validity of the SNAP-IV in Children Displaying ADHD Symptoms. Assessment 2020, 27, 1258–1271. [Google Scholar] [CrossRef]
- Costa, D.S.; de Paula, J.J.; Malloy-Diniz, L.F.; Romano-Silva, M.A.; Miranda, D.M. Parent SNAP-IV rating of attention-deficit/hyperactivity disorder: Accuracy in a clinical sample of ADHD, validity, and reliability in a Brazilian sample. J. Pediatr. 2019, 95, 736–743. [Google Scholar] [CrossRef]
- Pereira, E.E.L.D.; Minervino, C.A.D.S.M.; Cruz, L.F.P.D.; Roama-Alves, R.J.; Andrade, J.M. Executive Functions in Children with ADHD and/or Reading Difficulty. Psicol. Teor. E Pesqui. 2020, 36, 1–11. [Google Scholar] [CrossRef]
- Guerreiro, T.B.F.; Cavalcante, L.I.C.; Costa, E.F.; Valente, M.D.R. Triagem do Desenvolvimento Neuropsicomotor de Crianças das Unidades de Educação Infantil do Município de Belém, Pará, Brasil. J. Hum. Growth Dev. 2016, 26, 181–189. [Google Scholar] [CrossRef] [Green Version]
- Sabates, A.L.; David, E.T.M. Assessment of Growth and Development of Infants with Congenital Heart Disease: A Descriptive Study. Online Braz j Nurs(Online). 2006. Available online: https://pesquisa.bvsalud.org/portal/resource/pt/lil-490076 (accessed on 20 May 2022).
- Oliveira Cmlbov, D.C. Desenvolvimento neuropsicomotor: O teste de Denver na triagem dos atrasos cognitivos e neuromotores de pré-escolares. Cad. Saúde Pública 2011, 27, 7. [Google Scholar]
- Arcaya, M.C.; Arcaya, A.L.; Subramanian, S.V. Inequalities in health: Definitions, concepts, and theories. Glob. Health Action 2015, 8, 27106. [Google Scholar] [CrossRef] [PubMed]
- Almeida, C.; Sommer JA, P.; da Silveira, E.F.; Vivian, A.G. Gestação de alto risco: Vulnerabilidade social e fatores socioeconômicos. Conjecturas 2021, 1, 591–608. [Google Scholar]
- Ribeiro, K.G.; Andrade, L.O.M.D.; Aguiar, J.B.D.; Moreira, A.E.M.M.; Frota, A.C. Educação e saúde em uma região em situação de vulnerabilidade social: Avanços e desafios para as políticas públicas. Interface-Comun. Saúde Educ. 2018, 22, 1387–1398. [Google Scholar] [CrossRef] [Green Version]
- Araujo, W.R.M. Prevalência e Fatores Associados ao Atraso no Desenvolvimento Neuropsicomotor em Crianças de Uma Coorte Na Região Amazônica. Ph.D. Thesis, Universidade de São Paulo, São Paulo, Brazil, 2021.
- De Zago, J.T.C.; Pinto, P.A.F.; Leite, H.R.; Santos, J.N.; de Morais, R.L.S. Associação Entre o Desenvolvimento Neuropsicomotor e Fatores de Risco Biológico e Ambientais em Crianças na Primeira Infância. Rev. CEFAC 2017, 19, 320–329. Available online: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1516-18462017000300320&lng=pt&tlng=pt (accessed on 3 June 2022). [CrossRef] [Green Version]
- Moreira, S.C.; Barreto, M.A.M. Transtorno de Déficit de Atenção e Hiperatividade: Conhecendo Para Intervir. Rev. Práxis 2017, 1, 2. Available online: https://revistas.unifoa.edu.br/praxis/article/view/1123 (accessed on 3 June 2022). [CrossRef]
- Healthtalk.org. Parents of Children with Congenital Heart Diease. 2020. Available online: https://healthtalk.org/parents-children-congenital-heart-disease/overview (accessed on 8 June 2021).
- Silva, L.D.C.; Pavão, T.D.C.A.; Souza, J.C.B.; Frias, L.D.M.P. Diagnóstico precoce das cardiopatias congênitas: Uma revisão integrativa. J. Manag. Prim. Health Care 2018, 9, 1–24. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total n (%) | CHD n (%) | Control n (%) | p Value | |
|---|---|---|---|---|
| Age (months) (mean ± DP) | 97.5 (±25.7) | 95.7 (±26.5) | 99.3 (±25.3) | 0.54 |
| Socioeconomic class | 0.01 | |||
| A-B1-B2 (upper) | 11 (15) | 7 (19) | 4 (10) | |
| C1-C2 | 59 (79) | 26 (70) | 33 (87) | |
| D-E (lower) | 5 (6) | 4(11) | 1 (3) | |
| Gender | 0.39 | |||
| Boys | 44 (59) | 23 (62) | 21 (55) | |
| Girls | 31 (41) | 14 (38) | 17 (45) | |
| Number of siblings | 0.49 | |||
| 0 | 14 (19) | 7 (19) | 7 (18) | |
| 1 | 30 (40) | 14 (38) | 16 (42) | |
| 2 | 15 (20) | 9 (24) | 6 (16) | |
| 3 or more | 16 (21) | 7 (19) | 9 (24) | |
| Reason for medical referral | <0.0001 | |||
| Established CHD | 22 (29) | 22 (59) | 0 (0) | |
| Suspected CHD | 9 (12) | 7 (19) | 2 (5) | |
| Another motive | 44 (59) | 8 (22) | 36 (95) | |
| Mother had prenatal care | 0.06 | |||
| No | 2 (3) | 0 (0) | 2 (5) | |
| Yes | 73 (97) | 37 (100) | 36 (95) | |
| Normal pulse oximetry | 1.00 | |||
| No | 7 (14) | 4 (14) | 3 (14) | |
| Yes | 42 (86) | 24 (86) | 18 (86) | |
| Fetal echocardiogram | 0.006 | |||
| No | 45 (78) | 20 (69) | 25 (86) | |
| Yes | 13 (22) | 9 (31) | 4 (14) |
| Total | CHD | Control | p Value | |
|---|---|---|---|---|
| Thumb Tip | 75.7 | 72.2 | 78.9 | 0.40 |
| Jumps at a height of 40 cm | 77.0 | 80.6 | 73.7 | 0.31 |
| Squatting balance | 68.9 | 72.2 | 65.8 | 0.44 |
| Speed test | 23.0 | 22.2 | 23.7 | 0.87 |
| Recognizes human figures | 59.4 | 55.6 | 63.1 | 0.39 |
| Variables | Crude Analysis (95% CI) | p Value | Adjusted Analysis (95% CI) | p Value |
|---|---|---|---|---|
| Age | 1.001 (0.998–1.004) | 0.661 | 1.001 (0.998–1.004) | 0.571 |
| Socioeconomic class | 0.995 (0.978–1.013) | 0.579 | 0.995 (0.978–1.013) | 0.579 |
| Gender | 0.579 | 0.603 | ||
| Girls | 1.049 (0.886–1.242) | 1.046 (0.883–1.240) | ||
| Boys | 1 | 1 | ||
| Number of siblings | 0.996 (0.937–1.058) | 0.889 | 0.989 (0.930–1.052) | 0.730 |
| Reason for medical referral | 0.183 | 0.183 | ||
| Established CHD | 0.798 (0.623–1.022) | 0.798 (0.623–1.022) | ||
| Suspected CHD | 0.931 (0.733–1.184) | 0.931 (0.733–1.184) | ||
| Another motive | 1 | 1 | ||
| Normal pulse oximetry | 0.887 | 0.517 | ||
| Yes | 1.012 (0.859–1.193) | 0.953 (0.822–1.103) | ||
| No | 1 | 1 | ||
| Previous admissions | 0.748 | 0.480 | ||
| Yes | 1.027 (0.873–1.207) | 1.057 (0.906–1.233) | ||
| No | 1 | 1 |
| Variables | Crude Analysis (95% CI) | p Value | Adjusted Analysis (95% CI) | p Value |
|---|---|---|---|---|
| Age | 0.996 (0.993–0.999) | 0.008 * | 0.996 (0.994–0.999) | 0.012 * |
| Socioeconomic class | 0.982 (0.969–0.994) | 0.005 * | 0.983 | 0.007 * |
| Gender | 0.326 | 0.318 | ||
| Girls | 1.084 (0.923–1.273) | 1.075 (0.933–1.239) | ||
| Boys | 1 | 1 | ||
| 0.534 | 0.450 | |||
| Number of siblings | 1.022 (0.960–1.096) | 1.024 (0.963–1088) | ||
| Reason for medical referral | 0.258 | 0.440 | ||
| Established CHD | 1.143 (0.958–1.263) | 1.113 (0.932–1.329) | ||
| Suspected CHD | 0.960 (0.752–1.227) | 0.978 (0.802–1.193) | ||
| Another motive | 1 | 1 | ||
| Normal pulse oximetry | 0.887 | 0.517 | ||
| Yes | 1.012 (0.859–1.193) | 0.953 (0.822–1.103) | ||
| No | 1 | 1 | ||
| Previous admissions | 0.661 | 0.816 | ||
| Yes | 1.037 (0.883–1.217) | 0.983 (0.852–1.134) | ||
| No | 1 | 1 |
| Variables | Crude Analysis (95% CI) | p Value | Adjusted Analysis (95% CI) | p Value |
|---|---|---|---|---|
| Age | 0.998 (0.978–1.018) | 0.842 | 0.998 (0.982–1.013) | 0.759 |
| Socioeconomic class | 0.863 (0.782–0.954) | 0.004 * | 0.868 (0782–0.963) | 0.008 * |
| Gender | 0.939 | 0.668 | ||
| Girls | 1.268 (0.470–3.420) | 1.231 (0.477–3.172) | ||
| Boys | 1 | 1 | ||
| Number of siblings | 1.374 (1.073–1.760) | 0.012 * | 1.289 (1.043–1.593) | 0.019 * |
| Reason for medical referral | 0.437 | 0.382 | ||
| Established CHD | 1.143 (0.374–3.491) | 0.915 (0.305–2.741) | ||
| Suspected CHD | 2.095 (0.666–6.596) | 2.067 (0.616–6.938) | ||
| Another motive | 1 | 1 | ||
| Normal pulse oximetry | 0.123 | 0.066 | ||
| Yes | 0.473 (0.183–1.224) | 0.433 (0.177–1.058) | ||
| No | 1 | 1 | ||
| Previous admissions | 0.180 | 0.897 | ||
| Yes | 2.073 (0.713–6.024) | 1.081 (0.330–3.541) | ||
| No | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vignol, F.S.; Aikawa, P.; da Silveira, T.B.; Tavella, R.A.; Mahtani-Chugani, V.; Sanz, E.J.; da Silva Júnior, F.M.R. Neurodevelopmental Outcomes among Brazilian Children with Cyanotic Congenital Heart Disease and Its Associated Factors. Medicina 2022, 58, 1669. https://doi.org/10.3390/medicina58111669
Vignol FS, Aikawa P, da Silveira TB, Tavella RA, Mahtani-Chugani V, Sanz EJ, da Silva Júnior FMR. Neurodevelopmental Outcomes among Brazilian Children with Cyanotic Congenital Heart Disease and Its Associated Factors. Medicina. 2022; 58(11):1669. https://doi.org/10.3390/medicina58111669
Chicago/Turabian StyleVignol, Flávia Saraçol, Priscila Aikawa, Tatiane Britto da Silveira, Ronan Adler Tavella, Vinita Mahtani-Chugani, Emílio J. Sanz, and Flavio Manoel Rodrigues da Silva Júnior. 2022. "Neurodevelopmental Outcomes among Brazilian Children with Cyanotic Congenital Heart Disease and Its Associated Factors" Medicina 58, no. 11: 1669. https://doi.org/10.3390/medicina58111669
APA StyleVignol, F. S., Aikawa, P., da Silveira, T. B., Tavella, R. A., Mahtani-Chugani, V., Sanz, E. J., & da Silva Júnior, F. M. R. (2022). Neurodevelopmental Outcomes among Brazilian Children with Cyanotic Congenital Heart Disease and Its Associated Factors. Medicina, 58(11), 1669. https://doi.org/10.3390/medicina58111669