
Effect of Dupilumab on Sexual Desire in Adult Patients with Moderate to Severe Atopic Dermatitis

 ,
, 
 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
5. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weidinger, S.; Novak, N. Atopic dermatitis. Lancet 2016, 387, 1109–1122. [Google Scholar] [CrossRef] [PubMed]
- Nutten, S. Atopic Dermatitis: Global Epidemiology and Risk Factors. Ann. Nutr. Metab. 2015, 66 (Suppl. S1), 8–16. [Google Scholar] [CrossRef] [PubMed]
- Patruno, C.; Fabbrocini, G.; Napolitano, M. Clinical phenotypes of atopic dermatitis of the adult. Ital. J. Dermatol. Venereol. 2022, 156, 721–722. [Google Scholar] [CrossRef] [PubMed]
- Sampogna, F.; Abeni, D.; Gieler, U.; Tomas-Aragones, L.; Lien, L.; Titeca, G.; Jemec, G.; Misery, L.; Szabó, C.; Linder, M.; et al. Impairment of Sexual Life in 3485 Dermatological Outpatients From a Multicentre Study in 13 European Countries. Acta Derm. Venereol. 2017, 97, 478–482. [Google Scholar] [CrossRef] [Green Version]
- Linares-Gonzalez, L.; Lozano-Lozano, I.; Gutierrez-Rojas, L.; Ruiz-Villaverde, R.; Lozano-Lozano, M. Sexual dysfunction in a cohort of patients with moderate-to-severe atopic dermatitis. Influence of dupilumab treatment. Int. J. Dermatol. 2022, 61, 607–610. [Google Scholar] [CrossRef] [PubMed]
- WHO|Gender and Human Rights. World Health Organization: Sexual and reproductive rights. Available online: https://www.who.int/reproductivehealth/topics/gender_rights/defining_sexual_health/en/ (accessed on 28 January 2002).
- Ludwig, C.M.; Fernandez, J.M.; Hsiao, J.L.; Shi, V.Y. The Interplay of Atopic Dermatitis and Sexual Health. Dermatitis 2020, 31, 303–308. [Google Scholar] [CrossRef]
- Caminati, M.; Giorgis, V.; Palterer, B.; Racca, F.; Salvottini, C.; Rossi, O. Allergy and Sexual Behaviours: An Update. Clin. Rev. Allergy Immunol. 2017, 56, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Misery, L.; Finlay, A.; Martin, N.; Boussetta, S.; Nguyen, C.; Myon, E.; Taieb, C. Atopic Dermatitis: Impact on the Quality of Life of Patients and Their Partners. Dermatology 2007, 215, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Levine, S.B. The Nature of Sexual Desire: A Clinician’s Perspective. Arch. Sex. Behav. 2003, 32, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, M.; Ferrillo, M.; Patruno, C.; Scalvenzi, M.; D’Andrea, M.; Fabbrocini, G. Efficacy and Safety of Dupilumab in Clinical Practice: One Year of Experience on 165 Adult Patients from a Tertiary Referral Centre. Dermatol. Ther. 2021, 11, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Patruno, C.; Potestio, L.; Scalvenzi, M.; Battista, T.; Raia, F.; Picone, V.; Fabbrocini, G.; Napolitano, M. Dupilumab for the treatment of adult atopic dermatitis in special populations. J. Dermatol. Treat. 2022, 33, 3028–3033. [Google Scholar] [CrossRef] [PubMed]
- Tánczosová, M.; Kojanová, M.; Arenbergerová, M.; Arenberger, P.; Doležal, T.; Štrosová, D.; Fialová, J.; Gkalpakiotis, S. Real-life experience in the effectiveness, impact on quality of life and safety of dupilumab treatment in patients with moderate to severe atopic dermatitis in the Czech Republic. Cent. Eur. J. Public Health 2022, 30, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Spector, I.P.; Carey, M.P.; Steinberg, L. The sexual desire inventory: Development, factor structure, and evidence of reliability. J. Sex Marital Ther. 1996, 22, 175–190. [Google Scholar] [CrossRef] [PubMed]
- Callea, A.; Rossi, G. Italian Validation of the Sexual Desire Inventory (SDI-2): Psychometric Properties and Factorial Structure. Clin. Neuropsychiatry 2021, 18, 223–230. [Google Scholar] [PubMed]
- Ermertcan, A. Sexual dysfunction in dermatological diseases. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Latif, E.Z.; Diamond, M.P. Arriving at the diagnosis of female sexual dysfunction. Fertil. Steril. 2013, 100, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Murray, G.; O’Kane, M.; Watson, R.; Tobin, A.M. Psychosocial burden, and out-of-pocket costs in patients with atopic dermatitis in Ireland. Clin. Exp. Dermatol. 2021, 46, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.; Keller, J.J.; Lin, H. Association of Erectile Dysfunction with Atopic Dermatitis: A Population-Based Case-Control Study. J. Sex. Med. 2012, 9, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Cork, M.; Eckert, L.; Simpson, E.L.; Armstrong, A.; Barbarot, S.; Puig, L.; Girolomoni, G.; De Bruin-Weller, M.; Wollenberg, A.; Kataoka, Y.; et al. Dupilumab improves patient-reported symptoms of atopic dermatitis, symptoms of anxiety and depression, and health-related quality of life in moderate-to-severe atopic dermatitis: Analysis of pooled data from the randomized trials SOLO 1 and SOLO 2. J. Dermatol. Treat. 2019, 31, 606–614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thaçi, D.; LSimpson, E.; Deleuran, M.; Kataoka, Y.; Chen, Z.; Gadkari, A.; Eckert, L.; Akinlade, B.; Graham, N.M.H.; Pirozzi, G.; et al. Efficacy, and safety of dupilumab monotherapy in adults with moderate-to-severe atopic dermatitis: A pooled analysis of two phase 3 randomized trials (LIBERTY AD SOLO 1 and LIBERTY AD SOLO 2). J. Dermatol. Sci. 2019, 94, 266–275. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients | 328 |
|---|---|
| Sex | |
| Male | 170 (51.8%) |
| Female | 158 (48.2%) |
| Family status | |
| Single | 102 (31.1%) |
| In a relationship | 138 (42.1%) |
| Divorced or separated | 88 (26.8%) |
| Occurrence | |
| Persistent | 192 (58.5%) |
| Adult-onset | 136 (41.5%) |
| Average disease duration (years) | 14.82 ± 10.33 |
| Atopic comorbidities | |
| Rhinitis | 91 (27.7%) |
| Asthma | 63 (19.2%) |
| Conjunctivitis | 42 (12.8%) |
| Food allergy | 8 (2.4%) |
| Clinical phenotype | |
| Flexural dermatitis | 121 (36.8%) |
| Generalized eczema | 93 (28.4%) |
| Prurigo nodularis-like | 53 (16.2%) |
| Hand eczema | 42 (12.8%) |
| Nummular eczema | 6 (1.8%) |
| Head and neck eczema | 3 (0.9%) |
| Involvement of genital area | 92 (28.04%) |
| Involvement of nipples | 31 (9.45%) |
| Previous systemic treatment | |
| Cyclosporine | 125 (38.1%) |
| Systemic steroids | 98 (29.9%) |
| Others | 13 (4%) |
| AD severity score (mean ± SD; median) | |
| Baseline | |
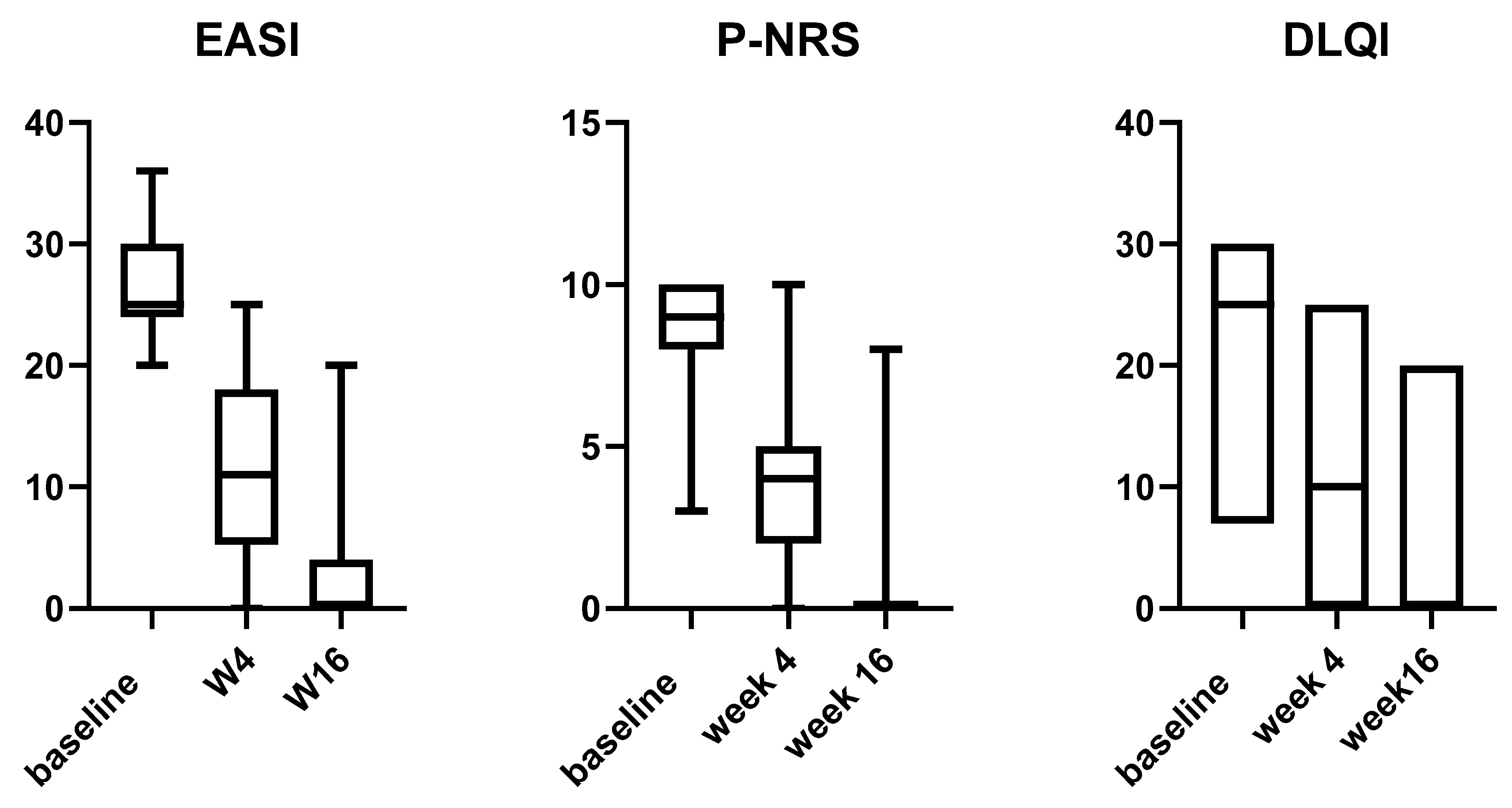
| EASI | 26.84 ± 3.38; 25 |
| P-NRS | 8.89 ± 1.28; 9 |
| DLQI | 22.8 ± 5.31; 25 |
| Week 4 | |
| EASI | 11.39 ± 6.83; 11 (p < 0.0001) |
| P-NRS | 3.76 ± 2.49; 4 (p < 0.0001) |
| DLQI | 9 ± 6.49; 10 (p < 0.0001) |
| Week 16 | |
| EASI | 2.11 ± 3.82; 0 (p < 0.0001) |
| P-NRS | 0.84 ± 1.75; 0 (p < 0.0001) |
| DLQI | 1.75 ± 3.54; 0 (p < 0.0001) |
| Average EASI percentage improvement | |
| After 4 weeks | 57.56% |
| After 16 weeks | 92.13% |
| Average P-NRS percentage improvement | |
| After 4 weeks | 57.76% |
| After 16 weeks | 90.55% |
| Average DLQI percentage improvement | |
| After 4 weeks | 60.52% |
| After 16 weeks | 76.75% |
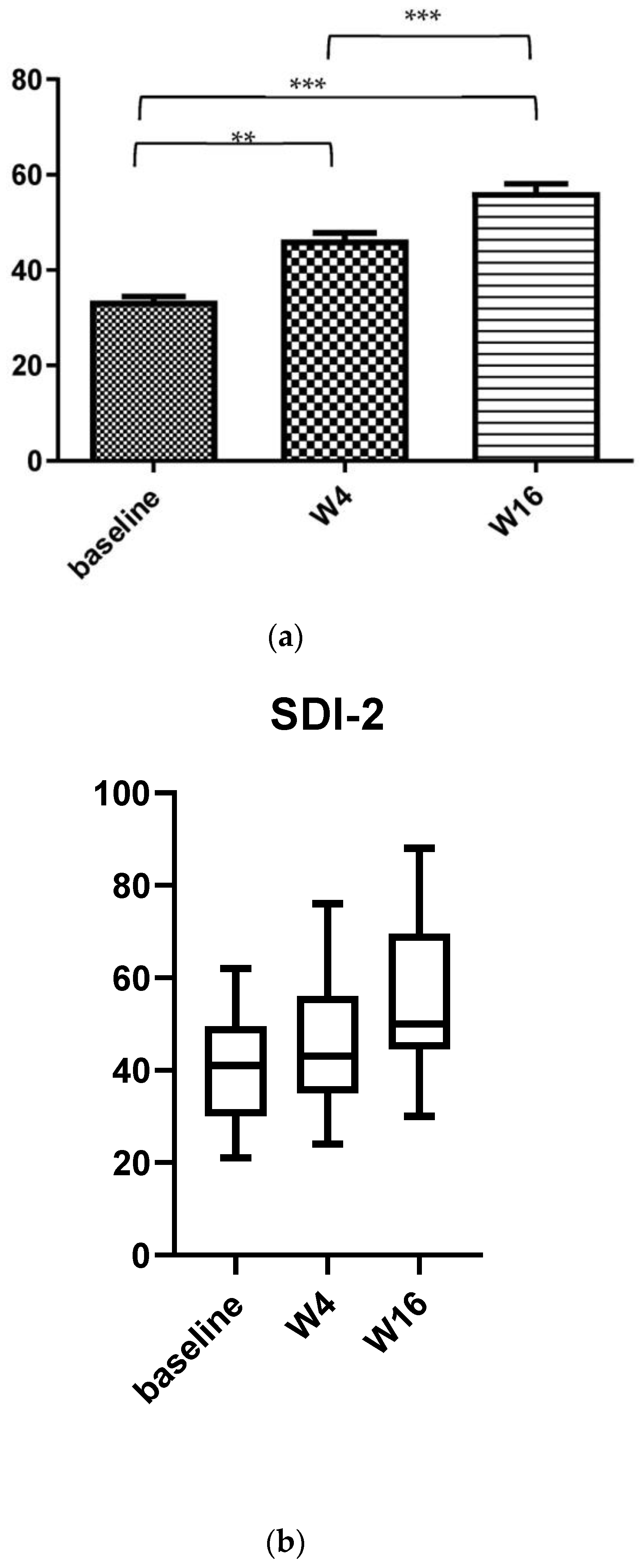
| SDI-2 (mean value ± SD; median) | |
| At baseline | 33.57 ± 8.18; 41 |
| After 4 weeks | 46.34 ± 13.5; 43 |
| After 16 weeks | 56.34 ± 16.5; 50 |
| Baseline Median; % of Patients (Number of Patients) | Week 4 (W4) Median; % of Patients (Number of Patients) | Week 16 (W16) Median; % of Patients (Number of Patients) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Score 0–3 | Score: 4–6 | Score 7–10 | Score 0–3 | Score 4–6 | Score 7–10 | Score 0–3 | Score 4–6 | Score 7–10 | |
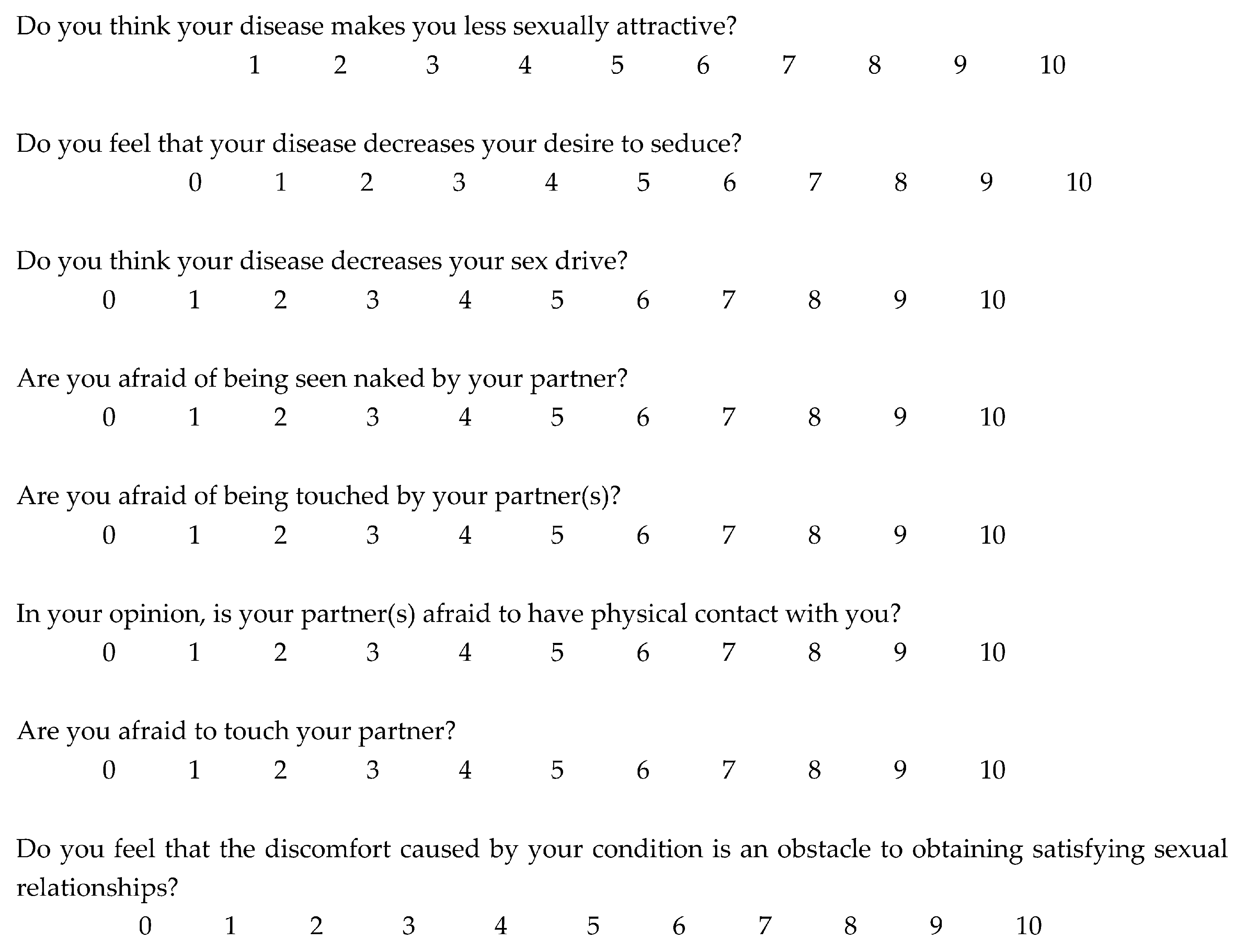
| Q1 | 2; 6.7% (n = 22) | 5; 41.8% (n = 137) | 9; 51.5% (n = 169) | 1; 50.6% *** (n = 166) | 5; 43.3% NS (n = 142) | 8; 6.1% *** (n = 20) | 1; 89.9% *** (n = 295) | 4; 8.5% *** (n = 28) | 7; 1.5% *** (n = 5) |
| Q2 | 2; 14% (n = 46) | 5; 59.1% (n = 194) | 9; 26.9% (n = 88) | 0; 53.7% *** (n = 176) | 4; 44.2% * (n = 145) | 7; 2.1% *** (n = 7) | 1; 86% *** (n = 282) | 4; 11.6% *** (n = 38) | 7; 2.4% *** (n = 8) |
| Q3 | 2; 48.2% (n = 158) | 5; 47.6% (n = 156) | 9; 4.2% (n = 14) | 2; 55.5% NS (n = 182) | 5; 43.6% NS (n = 143) | 8; 0.9% ** (n = 3) | 1; 91.5% *** (n = 300) | 5; 7.9% *** (n = 26) | 7; 0.6% ** (n = 2) |
| Q4 | 2; 9.7% (n = 32) | 5; 43.3% (n = 142) | 9; 46.9% (n = 154) | 2; 16.2% NS (n = 53) | 5; 57.9% NS (n = 190) | 9; 25.9% *** (n = 85) | 1; 91.2% *** (n = 299) | 4; 7.6% *** (n = 25) | 7; 1.2% *** (n = 4) |
| Q5 | 3; 14.3% (n = 47) | 5; 59.5% (n = 195) | 9; 26.2% (n = 86) | 1; 51.8% *** (n = 170) | 5; 43.6% NS (n = 143) | 9; 4.6% *** (n = 15) | 1; 93.6% *** (n = 307) | 6; 5.8% *** (n = 19) | 7; 0.6% *** (n = 2) |
| Q6 | 3; 8.8% (n = 29) | 6; 42.7% (n = 140) | 9; 48.5% (n = 159) | 1; 22.2% *** (n = 73) | 4; 62.5% ** (n = 205) | 8; 27.4% *** (n = 90) | 1; 94.8% *** (n = 311) | 4; 4.6% *** (n = 15) | 7; 0.6% *** (n = 2) |
| Q7 | 3; 51.2% (n = 168) | 6; 42.7% (n = 140) | 9; 6.1% (n = 20) | 1; 94.5% *** (n = 310) | 4; 4.9% *** (n = 16) | 8; 0.6% *** (n = 2) | 1; 96.3% *** (n = 316) | 4; 3.4% *** (n = 11) | 7; 0.3% *** (n = 1) |
| Q8 | 2; 7.6% (n = 25) | 6; 41.8% (n = 137) | 9; 50.6% (n = 166) | 0; 26.5% *** (n = 87) | 4; 59.1% * (n = 194) | 7; 14.3% *** (n = 47) | 1; 93.3% *** (n = 306) | 4; 5.8% *** (n = 19) | 7; 0.9% * (n = 3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Napolitano, M.; Fabbrocini, G.; Kastl, S.; Battista, T.; Di Guida, A.; Martora, F.; Picone, V.; Ventura, V.; Patruno, C. Effect of Dupilumab on Sexual Desire in Adult Patients with Moderate to Severe Atopic Dermatitis. Medicina 2022, 58, 1708. https://doi.org/10.3390/medicina58121708
Napolitano M, Fabbrocini G, Kastl S, Battista T, Di Guida A, Martora F, Picone V, Ventura V, Patruno C. Effect of Dupilumab on Sexual Desire in Adult Patients with Moderate to Severe Atopic Dermatitis. Medicina. 2022; 58(12):1708. https://doi.org/10.3390/medicina58121708
Chicago/Turabian StyleNapolitano, Maddalena, Gabriella Fabbrocini, Sara Kastl, Teresa Battista, Adriana Di Guida, Fabrizio Martora, Vincenzo Picone, Virginia Ventura, and Cataldo Patruno. 2022. "Effect of Dupilumab on Sexual Desire in Adult Patients with Moderate to Severe Atopic Dermatitis" Medicina 58, no. 12: 1708. https://doi.org/10.3390/medicina58121708
APA StyleNapolitano, M., Fabbrocini, G., Kastl, S., Battista, T., Di Guida, A., Martora, F., Picone, V., Ventura, V., & Patruno, C. (2022). Effect of Dupilumab on Sexual Desire in Adult Patients with Moderate to Severe Atopic Dermatitis. Medicina, 58(12), 1708. https://doi.org/10.3390/medicina58121708