
Characteristics and Outcomes of Critically Ill Pregnant/Postpartum Women with COVID-19 Pneumonia in Western Balkans, The Republic of Srpska Report

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients’ Selection
2.3. Criteria for MICU Admission
2.4. Study Parameters
2.5. MICU Treatment of Critically Ill Patients in MICU of the University Clinical Centre of the Republic of Srpska
- (a)
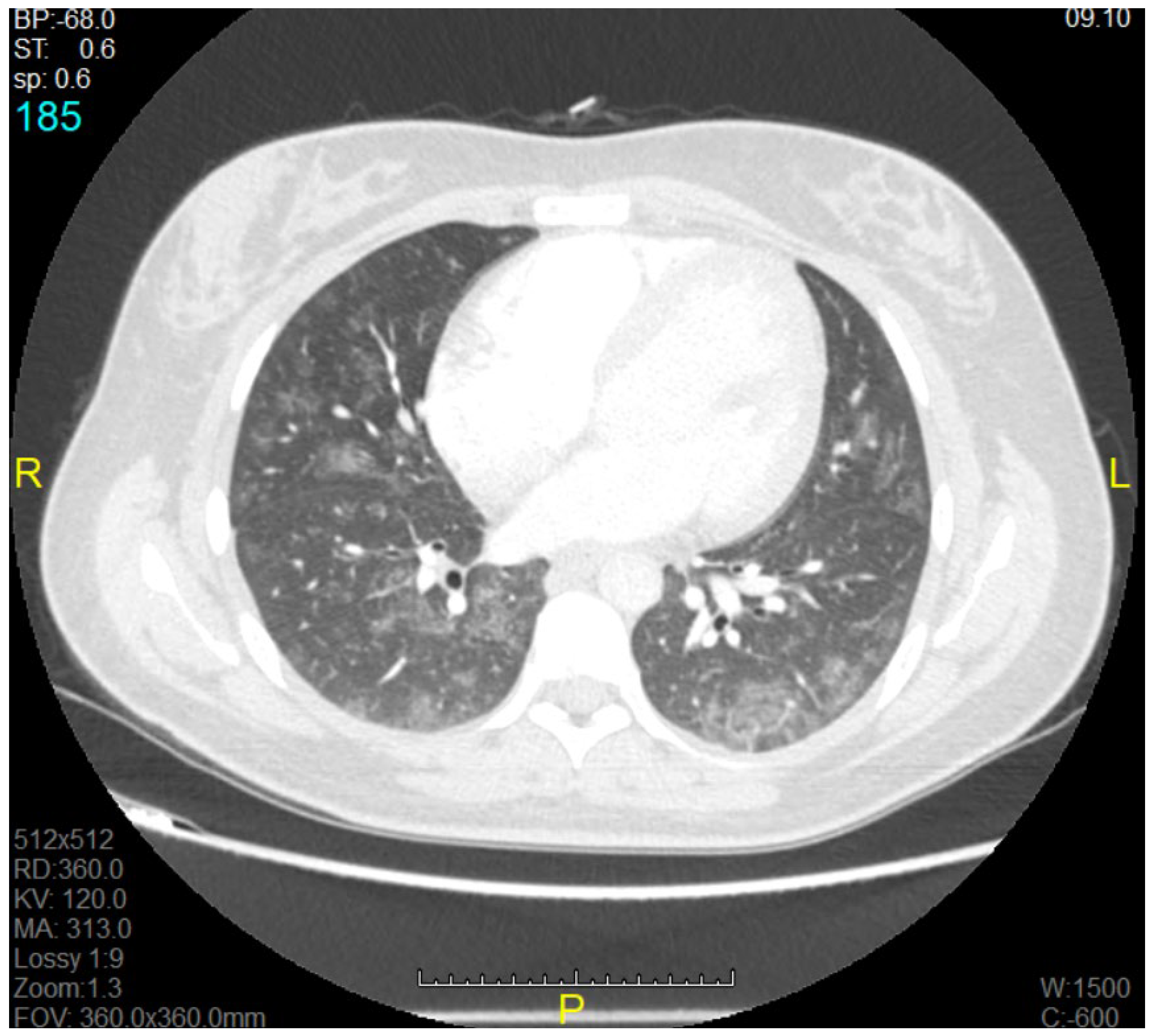
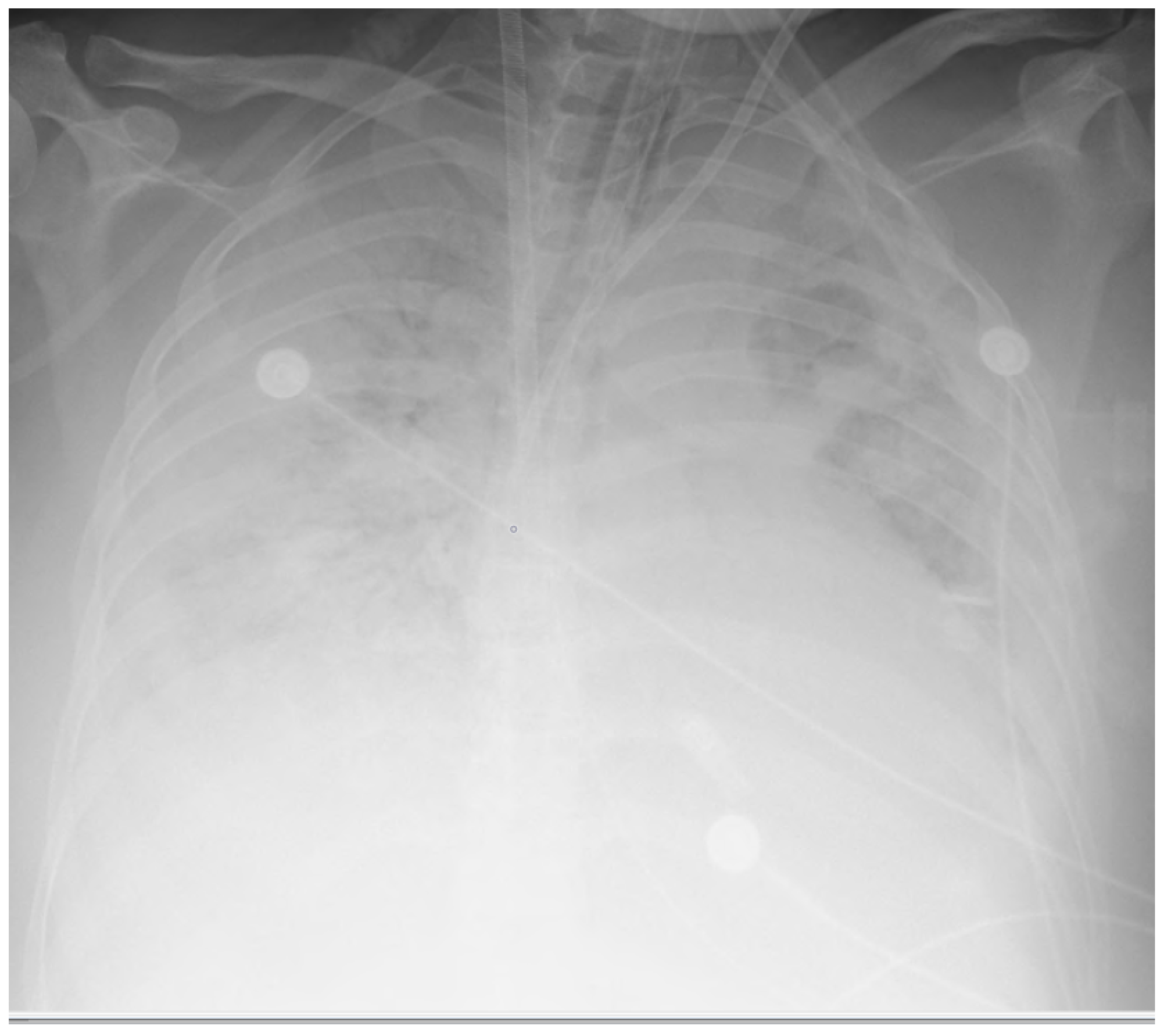
- Corticosteroids: All women requiring oxygen therapy were treated with corticosteroids. Intravenous methylprednisolone, to limit transplacental passage, was administered in a dose of 1 mg/kg daily for 10 consecutive days, or for a shorter period if oxygen therapy was no longer required. In case foetal lung maturation was required between 24 and 34 weeks of gestation, methylprednisolone was replaced by 6 mg of dexamethasone intravenously twice a day for 48 h. In case of moderate/severe ARDS (P/F ratio < 200 mmHg) and poor response to prone positioning or progression of disease on chest computed tomography (Group B), higher dose of methylprednisolone was administered (2 mg/kg) intravenously. Progression on CT was reported in presence of bilateral ground-glass opacity and/or consolidation, which was in the line with other clinical recommendations, and CT scans for all patients were performed before transfer to MICU [18,19,20].
- (b)
- Anticoagulation: All patients were on therapeutic doses of heparin, except for patients with contraindication for this medication. Unfractionated heparin was dosed in accordance with levels of Activated Partial Thromboplastin Clotting Time (aPTT). None of observed patients experienced thromboembolic or bleeding events. This is in contrary to other clinical approaches [21,22].
- (c)
- Veno-venous extracorporeal membrane oxygenation (vvECMO) was applied to four patients (21.05%); this very sophisticated and very challenging therapeutic mode was accessible to all patients from this population (pregnant/postpartal women with COVID-19).
- (d)
- Specific medication: None of our patients received antiviral therapy, tocilizumab, or orcasirivimab/imdevimab. Some centres had experience with mentioned medications [23].
2.6. Statistical Analysis
3. Results
3.1. Maternal and Neonatal Outcomes
3.2. Basic Characteristics of Patients (Maternal) and Neonates
3.3. Characteristics of Treatment in MICU
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Chauhan, S. Comprehensive review of coronavirus disease 2019 (COVID-19). Biomed. J. 2020, 43, 334–340. [Google Scholar] [CrossRef] [PubMed]
- Goletic, T.; Konjhodzic, R.; Fejzic, N.; Goletic, S.; Eterovac, T.; Softic, A.; Kustura, A.; Salihefendic, L.; Ostojic, M.; Travar, M.; et al. Phylogenetic pattern of SARS-CoV-2 from COVID-19 patients from Bosnia and Herzegovina: Lessons learned to optimize future molecular and epidemiological approaches. Bosn. J. Basic Med. Sci. 2021, 21, 484–487. [Google Scholar] [CrossRef] [PubMed]
- The Public Health Institute of the Republic of Srpska. 2022. Available online: https://www.phi.rs.ba/ (accessed on 1 April 2022).
- Ministry of Civil Affairs of Bosnia and Herzegovina. 2022. Available online: http://mcp.gov.ba/publication/read/epidemioloska-slika-bih2022godina?pageId=3&lang=en (accessed on 1 May 2022).
- Arapović, J.; Skočibušić, S. The first two months of the COVID-19 pandemic in Bosnia and Herzegovina: Single-center experience. Bosn. J. Basic Med. Sci. 2020, 20, 396–400. [Google Scholar] [CrossRef] [PubMed]
- Wastnedge, E.A.N.; Reynolds, R.M.; Van Boeckel, S.R.; Stock, S.J.; Denison, F.C.; Maybin, J.A.; Critchley, H.O.D. Pregnancy and COVID-19. Physiol. Rev. 2021, 101, 303–318. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Zeng, J.; Liu, X.; Sun, G.; Gao, Y.; Liao, J.; Yu, J.; Luo, X.; Qi, H. Changes in physiology and immune system during pregnancy and coronavirus infection: A review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 255, 124–128. [Google Scholar] [CrossRef]
- Ellington, S.; Strid, P.; Tong, V.T.; Woodworth, K.; Galang, R.R.; Zambrano, L.D.; Nahabedian, J.; Anderson, K.; Gilboa, S.M. Characteristics of Women of Reproductive Age with Laboratory-Confirmed SARS-CoV-2 Infection by Pregnancy Status—United States, 22 January–7 June, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 769–775. [Google Scholar] [CrossRef]
- Losonczy, L.I.; Papali, A.; Kivlehan, S.; Hynes, E.J.C.; Calderon, G.; Laytin, A.; Moll, V.; Al Hazmi, A.; Alsabri, M.; Aryal, D.; et al. White Paper on Early Critical Care Services in Low Resource Settings. Ann. Glob. Health 2021, 87, 105. [Google Scholar] [CrossRef]
- Kovacevic, P.; Meyer, F.J.; Gajic, O. Successful implementation of modern critical care in the low-resources country Bosnia and Herzegovina: Single-center experience. Med. Klin. Intensivmed. Notfmed. 2021, 117, 269–275. [Google Scholar] [CrossRef]
- Vukoja, M.; Riviello, E.D.; Schultz, M.J. Critical care outcomes in resource-limited settings. Curr. Opin. Crit. Care 2018, 24, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Thiéry, G.; Kovačević, P.; Štraus, S.; Vidović, J.; Iglica, A.; Festić, E.; Gajić, O. From mechanical ventilation to intensive care medicine: A challenge for Bosnia and Herzegovina. Bosn. J. Basic Med. Sci. 2009, 9 (Suppl. 1), 69–76. [Google Scholar] [CrossRef]
- Kovacevic, P.; Dragic, S.; Kovacevic, T.; Momcicevic, D.; Festic, E.; Kashyap, R.; Niven, A.S.; Dong, Y.; Gajic, O. Impact of weekly case-based tele-education on quality of care in a limited resource medical intensive care unit. Crit. Care 2019, 23, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ARDS Definition Task Force; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [PubMed]
- Vincent, J.L.; De Mendonça, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.M.; Blecher, S. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: Results of a multicenter, prospective study. Working group on “sepsis-related problems” of the European Society of Intensive Care Medicine. Crit. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Endeman, H.; van der Zee, P.; van Genderen, M.E.; van den Akker, J.P.C.; Gommers, D. Progressive respiratory failure in COVID-19: A hypothesis. Lancet Infect. Dis. 2020, 20, 1365. [Google Scholar] [CrossRef]
- Crowther, C.A.; Ashwood, P.; Andersen, C.C.; Middleton, P.F.; Tran, T.; Doyle, L.W.; Robinson, J.S.; E Harding, J.; Ball, V.; Holst, C.; et al. ASTEROID Study Group. Maternal intramuscular dexamethasone versus betamethasone before preterm birth (ASTEROID): A multicentre, double-blind, randomised controlled trial. Lancet Child Adolesc. Health 2019, 3, 769–780. [Google Scholar] [CrossRef]
- Ranjbar, K.; Moghadami, M.; Mirahmadizadeh, A.; Fallahi, M.J.; Khaloo, V.; Shahriarirad, R.; Erfani, A.; Khodamoradi, Z.; Saadi, M.H.G. Methylprednisolone or dexamethasone, which one is superior corticosteroid in the treatment of hospitalized COVID-19 patients: A triple-blinded randomized controlled trial. BMC Infect. Dis. 2021, 21, 337. [Google Scholar] [CrossRef]
- Saad, A.F.; Chappell, L.; Saade, G.R.; Pacheco, L.D. Corticosteroids in the management of pregnant patients with Coronavirus disease (COVID-19). Obstet. Gynecol. 2020, 136, 823–826. [Google Scholar] [CrossRef]
- Leffert, L.R.; Dubois, H.M.; Butwick, A.J.; Carvalho, B.; Houle, T.T.; Landau, R. Neuraxial anesthesia in obstetric patients receiving thromboprophylaxis with unfractionated or low-molecular-weight heparin: A systematic review of spinal epidural hematoma. Anesth. Analg. 2017, 125, 223–231. [Google Scholar] [CrossRef]
- The REMAP-CAP, ACTIV-4a, ATTACC Investigators. Therapeutic Anticoagulation with Heparin in Critically Ill Patients with COVID-19. N. Engl. J. Med. 2021, 385, 777–789. [Google Scholar] [CrossRef]
- Munshi, L.; Wright, J.K.; Zipursky, J.; Jorgensen, S.; Bogler, T.; Miller, K.; Mandhari, M.A.; Barrett, K.; Gandhi, S.; Gundy, S.; et al. The incidence, severity, and management of COVID-19 across acutely ill pregnant individuals. Sci. Briefs Ont. COVID-19 Sci. Advis. Table 2021, 2, 43. [Google Scholar] [CrossRef]
- Abbassi-Ghanavati, M.; Greer, L.G.; Cunningham , F.G. Pregnancy and laboratory studies: A reference table for clinicians. Obstet. Gynecol 2009, 114, 1326–1331. [Google Scholar] [CrossRef]
- Eman, A.; Balaban, O.; Kocayiğit, H.; Süner, K.Ö.; Cırdı, Y.; Erdem, A.F. Maternal and Neonatal Outcomes of Critically Ill Pregnant and Puerperal Patients Diagnosed with COVID-19 Disease: Retrospective Comparative Study. J. Korean Med. Sci. 2021, 36, e309. [Google Scholar] [CrossRef] [PubMed]
- Faraz, S.; Aftab, N.; Ammar, A.; Al Mulai, I.; Paulose, L.; Fernandes, S. An Insight on the Maternal-Fetal Outcomes of Critically Ill Pregnant Women During the Second Wave of COVID-19. Cureus 2022, 14, e20998. [Google Scholar] [CrossRef] [PubMed]
- Oakes, M.C.; Kernberg, A.S.; Carter, E.B.; Foeller, M.E.; Palanisamy, A.; Raghuraman, N.; Kelly, J.C. Pregnancy as a risk factor for severe coronavirus disease 2019 using standardized clinical criteria. Am. J. Obstet. Gynecol. MFM 2021, 3, 100319. [Google Scholar] [CrossRef] [PubMed]
- Serra, F.E.; Francisco, R.P.V.; de Rossi, P.; de Lourdes Brizot, M.; Rodrigues, A.S. COVID-19 outcomes in hospitalized puerperal, pregnant, and neither pregnant nor puerperal women. PLoS ONE 2021, 16, e0259911. [Google Scholar] [CrossRef]
- Kuzan, T.Y.; Altıntoprak, K.M.; Çiftçi, H.; Kuzan, B.N.; Yassa, M.; Tuğ, N.; Çimşit, N. Clinical and radiologic characteristics of symptomatic pregnant women with COVID-19 pneumonia. J. Turk. Ger. Gynecol. Assoc. 2021, 22, 196–205. [Google Scholar] [CrossRef]
- Sitter, M.; Pecks, U.; Rüdiger, M.; Friedrich, S.; Malfertheiner, S.F.; Hein, A.; Königbauer, J.T.; Becke-Jakob, K.; Zöllkau, J.; Ramsauer, B.; et al. Pregnant and Postpartum Women Requiring Intensive Care Treatment for COVID-19-First Data from the CRONOS-Registry. J. Clin. Med. 2022, 11, 701. [Google Scholar] [CrossRef]
- Van Genderen, M.E.; van Uitert, E.; Duvekot, J.J.; Gommers, D.; COVPREG Study Group. Management and outcome of critically ill pregnant women with COVID-19. Intensive Care Med. 2022, 48, 613–615. [Google Scholar] [CrossRef]
- Aliberti, S.; Amati, F.; Pappalettera, M.; Di Pasquale, M.; D’Adda, A.; Mantero, M.; Gramegna, A.; Simonetta, E.; Oneta, A.M.; Privitera, E.; et al. COVID-19 multidisciplinary high dependency unit: The Milan model. Respir. Res. 2020, 21, 260. [Google Scholar] [CrossRef]
- Bachani, S.; Arora, R.; Dabral, A.; Marwah, S.; Anand, P.; Reddy, K.S.; Gupta, N.; Singh, B. Clinical Profile, Viral Load, Maternal-Fetal Outcomes of Pregnancy With COVID-19: 4-Week Retrospective, Tertiary Care Single-Centre Descriptive Study. J. Obstet. Gynaecol. Can. 2021, 43, 474–482. [Google Scholar] [CrossRef]
- Juan, J.; Gil, M.M.; Rong, Z.; Zhang, Y.; Yang, H.; Poon, L.C. Effect of coronavirus disease 2019 (COVID-19) on maternal, perinatal and neonatal outcome: Systematic review. Ultrasound Obs. Gynecol. 2020, 56, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Elshafeey, F.; Magdi, R.; Hindi, N.; Elshebiny, M.; Farrag, N.; Mahdy, S.; Sabbour, M.; Gebril, S.; Nasser, M.; Kamel, M.; et al. A systematic scoping review of COVID-19 during pregnancy and childbirth. Int. J. Gynaecol. Obstet. 2020, 150, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, A.; Duiella, S.; Piani, L.L.; Comelli, A.; Ceriotti, F.; Oggioni, M.; Muscatello, A.; Bandera, A.; Gori, A.; Ferrazzi, E. Inflammatory biomarkers in pregnant women with COVID-19: A retrospective cohort study. Sci. Rep. 2021, 11, 13350. [Google Scholar] [CrossRef] [PubMed]
- Omoush, S.A.; Alzyoud, J.A.M. The Prevalence and Impact of Coinfection and Superinfection on the Severity and Outcome of COVID-19 Infection: An Updated Literature Review. Pathogens 2022, 11, 445. [Google Scholar] [CrossRef] [PubMed]
- Signorini, L.; Moioli, G.; Calza, S.; Van Hauwermeiren, E.; Lorenzotti, S.; Del Fabro, G.; Renisi, G.; Lanza, P.; Saccani, B.; Zambolin, G.; et al. Epidemiological and Clinical Characterization of Superinfections in Critically Ill Coronavirus Disease 2019 Patients. Crit. Care Explor. 2021, 3, e0430. [Google Scholar] [CrossRef]
- Brillo, E.; Tosto, V.; Gerli, S.; Buonomo, E. COVID-19 vaccination in pregnancy and postpartum. J. Matern. Fetal. Neonatal Med. 2021, 21, 1–21. [Google Scholar] [CrossRef]
- Delara, M.; Sadarangani, M. Immunization in pregnancy to protect pregnant people and their newborns against COVID-19. Expert Rev. Vaccines 2022, 21, 593–595. [Google Scholar] [CrossRef]
- Waring, M.E.; Pagoto, S.L.; Rudin, L.R.; Ho, C.; Horkachuck, A.; Kapoor, I.A.; Foye, Q. Factors associated with mothers’ hesitancy to receive a COVID-19 vaccine. J. Behav. Med. 2022, 4, 1–6. [Google Scholar] [CrossRef]
- King, W.C.; Rubinstein, M.; Reinhart, A.; Mejia, R. Time trends, factors associated with, and reasons for COVID-19 vaccine hesitancy: A massive online survey of US adults from January–May 2021. PLoS ONE 2021, 16, e0260731. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Groups | Mild ARDS (O2 + HFNC) N = 11 | Moderate ARDS (NIV) N = 8 | Severe ARDS (IMV) | Severe ARDS (vvECMO) | All |
|---|---|---|---|---|---|
| Recovery | 11 | 2 | 1 | 1 | 15 |
| Death | 0 | 0 | 1 | 3 | 4 |
| Labor (preterm) | 7 | 2 | 1 | 4 | 14 |
| Ongoing pregnancy | 4 | 0 | 0 | 0 | 4 |
| Livebirth | 7 | 2 | 1 | 4 | 14 |
| Groups | O2 + HFNC (Group A), N = 11 (57.89%) | NIV + IMV + ECMO (Group B), N = 8 (42.10%) | p |
|---|---|---|---|
| Maternal age, median (IQR) | 31 (25–37) | 36 (35–40.75) | 0.199 |
| Gestational age at diagnosis (weeks), (mean ± SD) | 32.86 ± 4.56 | 30.00 ± 3.92 | 0.233 |
| Birth weight in grams (mean ± SD) | 2758.57 ± 669.36 | 1664.29 ± 634.16 | 0.009 |
| Apgar in 1 minute (median, IQR) | 9 (7–9) | 8 (6–8) | 0.316 |
| Apgar in 5 minutes (median, IQR) | 9 (9–9) | 8 (8–9) | 0.259 |
| Length of ICU stay (days), median (IQR) | 4 (3–5) | 13.5 (8.5–20.5) | 0.015 |
| Renal replacement therapy | 0 | 3 (100%) | 0.021 |
| Vasoactive substances | 0 | 6 (75%) | 0.001 |
| Thromboembolic events | 0 | 0 | - |
| Anticoagulation: | |||
| Prophylactic | 0 | 0 | - |
| Therapeutic | 11 (100%) | 8 (100%) | - |
| Steroids | 11 (100%) | 8 (100%) | - |
| Coexisting conditions: | 3 (27.27%) | 3 (37.50%) | 0.636 |
| COVID-19 vaccination | 0 | 0 | - |
| Severity of illness: | |||
| SAPS II | 6 (6–7) | 16.5 (8.25–20.75) | 0.007 |
| APACHE II | 4 (4–5) | 10 (4.75–10-75) | 0.012 |
| SOFA on admission | 4 (4–4) | 4 (3–4.75) | 0.904 |
| P/F ratio | >200 | <200 | - |
| Parameters | Normal Values | Pregnancy Effect * | O2 + HFNC (Group A), N = 11 (57.9%) | NIV + IMV + ECMO (Group B) N = 8 (42.10%) | p |
|---|---|---|---|---|---|
| CRP, mean ± SD | 0–5 mg/L | 0.4–8.1 (third trimester) | 88.38 ± 64.53 | 104.30 ± 31.56 | 0.530 |
| Haemoglobin levels, mean ± SD | 138–175 g/L | decreased for 14–20 g/L | 109.45 ± 12.03 | 105.50 ± 12.58 | 0.501 |
| Platelet count, mean ± SD | 158–424 × 109/L | Slight decrease | 241.36 ± 104.15 | 189.13 ± 69.19 | 0.235 |
| White blood count, median (IQR) | 3.4–9.7 × 109/L | Increased for 3.5 | 9.36 (7.57–14.11) | 7.04 (5.30–10.40) | 0.137 |
| D-dimer, median (IQR) | 0–0.05 mg/L | 0.13–1.7 (third trimester) | 1.53 (0.95–5.45) | 1.84 (1.21–2.11) | 0.804 |
| BUN, median (IQR) | 2.8–7.2 mmol/L | 1.1–3.9 (third trimester) | 48.5 (46–51.5) | 58 (54–62) | 0.010 |
| PCT, median (IQR) | <0.02 ng/mL | - | 0.09 (0.05–0.20) | 0.26 (0.16–0.51) | 0.047 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kovacevic, P.; Topolovac, S.; Dragic, S.; Jandric, M.; Momcicevic, D.; Zlojutro, B.; Kovacevic, T.; Loncar-Stojiljkovic, D.; Djajic, V.; Skrbic, R.; et al. Characteristics and Outcomes of Critically Ill Pregnant/Postpartum Women with COVID-19 Pneumonia in Western Balkans, The Republic of Srpska Report. Medicina 2022, 58, 1730. https://doi.org/10.3390/medicina58121730
Kovacevic P, Topolovac S, Dragic S, Jandric M, Momcicevic D, Zlojutro B, Kovacevic T, Loncar-Stojiljkovic D, Djajic V, Skrbic R, et al. Characteristics and Outcomes of Critically Ill Pregnant/Postpartum Women with COVID-19 Pneumonia in Western Balkans, The Republic of Srpska Report. Medicina. 2022; 58(12):1730. https://doi.org/10.3390/medicina58121730
Chicago/Turabian StyleKovacevic, Pedja, Sandra Topolovac, Sasa Dragic, Milka Jandric, Danica Momcicevic, Biljana Zlojutro, Tijana Kovacevic, Dragana Loncar-Stojiljkovic, Vlado Djajic, Ranko Skrbic, and et al. 2022. "Characteristics and Outcomes of Critically Ill Pregnant/Postpartum Women with COVID-19 Pneumonia in Western Balkans, The Republic of Srpska Report" Medicina 58, no. 12: 1730. https://doi.org/10.3390/medicina58121730
APA StyleKovacevic, P., Topolovac, S., Dragic, S., Jandric, M., Momcicevic, D., Zlojutro, B., Kovacevic, T., Loncar-Stojiljkovic, D., Djajic, V., Skrbic, R., & Ećim-Zlojutro, V. (2022). Characteristics and Outcomes of Critically Ill Pregnant/Postpartum Women with COVID-19 Pneumonia in Western Balkans, The Republic of Srpska Report. Medicina, 58(12), 1730. https://doi.org/10.3390/medicina58121730