
Gender Related Differences in the Clinical Presentation of Hypertrophic Cardiomyopathy—An Analysis from the SILICOFCM Database

 , , , ,
, , , ,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Echocardiography
2.3. Genetic Testing
2.4. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Clinical Presentation
3.3. Blood Laboratory Analyses
3.4. Electrocardiography
3.5. Echocardiography
3.6. Genetic Testing
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maron, B.J.; Maron, M.S. Hypertrophic cardiomyopathy. Lancet 2013, 381, 242–255. [Google Scholar] [CrossRef]
- Maron, B.J. Clinical Course and Management of Hypertrophic Cardiomyopathy. N. Engl. J. Med. 2018, 379, 1977. [Google Scholar] [CrossRef]
- Maron, M.S.; Hellawell, J.L.; Lucove, J.C.; Farzaneh-Far, R.; Olivotto, I. Occurrence of Clinically Diagnosed Hypertrophic Cardiomyopathy in the United States. Am. J. Cardiol. 2016, 117, 1651–1654. [Google Scholar] [CrossRef] [PubMed]
- Gersh, B.J.; Maron, B.J.; Bonow, R.O.; Dearani, J.A.; Fifer, M.A.; Link, M.S.; Naidu, S.S.; Nishimura, R.A.; Ommen, S.R.; Rakowski, H.; et al. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: Executive summary: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2011, 124, 2761–2796. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Ommen, S.R.; Semsarian, C.; Spirito, P.; Olivotto, I.; Maron, M.S. Hypertrophic cardiomyopathy: Present and future, with translation into contemporary cardiovascular medicine. J. Am. Coll. Cardiol. 2014, 64, 83–99. [Google Scholar] [CrossRef] [Green Version]
- Task Force, M.; Elliott, P.M.; Anastasakis, A.; Borger, M.A.; Borggrefe, M.; Cecchi, F.; Charron, P.; Hagege, A.A.; Lafont, A.; Limongelli, G.; et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar] [CrossRef]
- Force, T.; Bonow, R.O.; Houser, S.R.; Solaro, R.J.; Hershberger, R.E.; Adhikari, B.; Anderson, M.E.; Boineau, R.; Byrne, B.J.; Cappola, T.P.; et al. Research priorities in hypertrophic cardiomyopathy: Report of a Working Group of the National Heart, Lung, and Blood Institute. Circulation 2010, 122, 1130–1133. [Google Scholar] [CrossRef]
- Lu, D.Y.; Pozios, I.; Haileselassie, B.; Ventoulis, I.; Liu, H.; Sorensen, L.L.; Canepa, M.; Phillip, S.; Abraham, M.R.; Abraham, T.P. Clinical Outcomes in Patients With Nonobstructive, Labile, and Obstructive Hypertrophic Cardiomyopathy. J. Am. Heart Assoc. 2018, 7, e006657. [Google Scholar] [CrossRef] [Green Version]
- Szyguła-Jurkiewicz, B.; Szczurek-Wasilewicz, W.; Osadnik, T.; Frycz-Kurek, A.M.; Macioł-Skurk, K.; Małyszek-Tumidajewicz, J.; Skrzypek, M.; Romuk, E.; Gąsior, M.; Banach, M.; et al. Oxidative Stress Markers in Hypertrophic Cardiomyopathy. Medicina 2022, 58, 31. [Google Scholar] [CrossRef]
- Garfinkel, A.C.; Seidman, J.G.; Seidman, C.E. Genetic Pathogenesis of Hypertrophic and Dilated Cardiomyopathy. Heart Fail. Clin. 2018, 14, 139–146. [Google Scholar] [CrossRef]
- Olivotto, I.; Girolami, F.; Ackerman, M.J.; Nistri, S.; Bos, J.M.; Zachara, E.; Ommen, S.R.; Theis, J.L.; Vaubel, R.A.; Re, F.; et al. Myofilament protein gene mutation screening and outcome of patients with hypertrophic cardiomyopathy. Mayo Clin. Proc. 2008, 83, 630–638. [Google Scholar] [CrossRef]
- Michels, M.; Soliman, O.I.; Phefferkorn, J.; Hoedemaekers, Y.M.; Kofflard, M.J.; Dooijes, D.; Majoor-Krakauer, D.; Ten Cate, F.J. Disease penetrance and risk stratification for sudden cardiac death in asymptomatic hypertrophic cardiomyopathy mutation carriers. Eur. Heart J. 2009, 30, 2593–2598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorenzini, M.; Norrish, G.; Field, E.; Ochoa, J.P.; Cicerchia, M.; Akhtar, M.M.; Syrris, P.; Lopes, L.R.; Kaski, J.P.; Elliott, P.M. Penetrance of Hypertrophic Cardiomyopathy in Sarcomere Protein Mutation Carriers. J. Am. Coll. Cardiol. 2020, 76, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Millat, G.; Bouvagnet, P.; Chevalier, P.; Dauphin, C.; Jouk, P.S.; Da Costa, A.; Prieur, F.; Bresson, J.L.; Faivre, L.; Eicher, J.C.; et al. Prevalence and spectrum of mutations in a cohort of 192 unrelated patients with hypertrophic cardiomyopathy. Eur. J. Med. Genet. 2010, 53, 261–267. [Google Scholar] [CrossRef]
- Liu, X.; Jiang, T.; Piao, C.; Li, X.; Guo, J.; Zheng, S.; Zhang, X.; Cai, T.; Du, J. Screening Mutations of MYBPC3 in 114 Unrelated Patients with Hypertrophic Cardiomyopathy by Targeted Capture and Next-generation Sequencing. Sci. Rep. 2015, 5, 11411. [Google Scholar] [CrossRef]
- Velicki, L.; Jakovljevic, D.G.; Preveden, A.; Golubovic, M.; Bjelobrk, M.; Ilic, A.; Stojsic, S.; Barlocco, F.; Tafelmeier, M.; Okwose, N.; et al. Genetic determinants of clinical phenotype in hypertrophic cardiomyopathy. BMC Cardiovasc. Disord. 2020, 20, 516. [Google Scholar] [CrossRef]
- Weissler-Snir, A.; Hindieh, W.; Gruner, C.; Fourey, D.; Appelbaum, E.; Rowin, E.; Care, M.; Lesser, J.R.; Haas, T.S.; Udelson, J.E.; et al. Lack of Phenotypic Differences by Cardiovascular Magnetic Resonance Imaging in MYH7 (beta-Myosin Heavy Chain)- Versus MYBPC3 (Myosin-Binding Protein C)-Related Hypertrophic Cardiomyopathy. Circ. Cardiovasc. Imaging 2017, 10, e005311. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Wang, J.; Zou, Y.; Bao, J.; Sun, K.; Zhu, L.; Tian, T.; Shen, H.; Zhou, X.; Ahmad, F.; et al. Female sex is associated with worse prognosis in patients with hypertrophic cardiomyopathy in China. PLoS ONE 2014, 9, e102969. [Google Scholar] [CrossRef]
- Geske, J.B.; Ong, K.C.; Siontis, K.C.; Hebl, V.B.; Ackerman, M.J.; Hodge, D.O.; Miller, V.M.; Nishimura, R.A.; Oh, J.K.; Schaff, H.V.; et al. Women with hypertrophic cardiomyopathy have worse survival. Eur. Heart J. 2017, 38, 3434–3440. [Google Scholar] [CrossRef] [Green Version]
- Schiller, N.B.; Shah, P.M.; Crawford, M.; DeMaria, A.; Devereux, R.; Feigenbaum, H.; Gutgesell, H.; Reichek, N.; Sahn, D.; Schnittger, I.; et al. Recommendations for quantitation of the left ventricle by two-dimensional echocardiography. American Society of Echocardiography Committee on Standards, Subcommittee on Quantitation of Two-Dimensional Echocardiograms. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 1989, 2, 358–367. [Google Scholar] [CrossRef]
- Lang, R.M.; Bierig, M.; Devereux, R.B.; Flachskampf, F.A.; Foster, E.; Pellikka, P.A.; Picard, M.H.; Roman, M.J.; Seward, J.; Shanewise, J.; et al. Recommendations for chamber quantification. Eur. J. Echocardiogr. J. Work. Group Echocardiogr. Eur. Soc. Cardiol. 2006, 7, 79–108. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Appleton, C.P.; Gillebert, T.C.; Marino, P.N.; Oh, J.K.; Smiseth, O.A.; Waggoner, A.D.; Flachskampf, F.A.; Pellikka, P.A.; Evangelista, A. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2009, 22, 107–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulus, W.J.; Tschope, C.; Sanderson, J.E.; Rusconi, C.; Flachskampf, F.A.; Rademakers, F.E.; Marino, P.; Smiseth, O.A.; De Keulenaer, G.; Leite-Moreira, A.F.; et al. How to diagnose diastolic heart failure: A consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur. Heart J. 2007, 28, 2539–2550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimitrow, P.P.; Czarnecka, D.; Jaszcz, K.K.; Dubiel, J.S. Sex differences in age at onset of symptoms in patients with hypertrophic cardiomyopathy. J. Cardiovasc. Risk 1997, 4, 33–35. [Google Scholar] [CrossRef] [PubMed]
- Dimitrow, P.P.; Czarnecka, D.; Jaszcz, K.K.; Dubiel, J.S. Comparison of left ventricular hypertrophy expression in patients with hypertrophic cardiomyopathy on the basis of sex. J. Cardiovasc. Risk 1998, 5, 85–87. [Google Scholar] [CrossRef] [PubMed]
- Dimitrow, P.P.; Czarnecka, D.; Strojny, J.A.; Kawecka-Jaszcz, K.; Dubiel, J.S. Impact of gender on the left ventricular cavity size and contractility in patients with hypertrophic cardiomyopathy. Int. J. Cardiol. 2001, 77, 43–48. [Google Scholar] [CrossRef]
- Dimitrow, P.P.; Czarnecka, D.; Kawecka-Jaszcz, K.; Dubiel, J.S. The influence of age on gender-specific differences in the left ventricular cavity size and contractility in patients with hypertrophic cardiomyopathy. Int. J. Cardiol. 2003, 88, 11–16; discussion 16–17. [Google Scholar] [CrossRef]
- Olivotto, I.; Maron, M.S.; Adabag, A.S.; Casey, S.A.; Vargiu, D.; Link, M.S.; Udelson, J.E.; Cecchi, F.; Maron, B.J. Gender-related differences in the clinical presentation and outcome of hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2005, 46, 480–487. [Google Scholar] [CrossRef] [Green Version]
- Kubo, T.; Kitaoka, H.; Okawa, M.; Hirota, T.; Hayato, K.; Yamasaki, N.; Matsumura, Y.; Yabe, T.; Doi, Y.L. Gender-specific differences in the clinical features of hypertrophic cardiomyopathy in a community-based Japanese population: Results from Kochi RYOMA study. J. Cardiol. 2010, 56, 314–319. [Google Scholar] [CrossRef] [Green Version]
- Husser, D.; Ueberham, L.; Jacob, J.; Heuer, D.; Riedel-Heller, S.; Walker, J.; Hindricks, G.; Bollmann, A. Prevalence of clinically apparent hypertrophic cardiomyopathy in Germany—An analysis of over 5 million patients. PLoS ONE 2018, 13, e0196612. [Google Scholar] [CrossRef] [Green Version]
- Enzan, N.; Matsushima, S.; Ide, T.; Kaku, H.; Tohyama, T.; Funakoshi, K.; Higo, T.; Tsutsui, H. Sex Differences in Time-Dependent Changes in B-Type Natriuretic Peptide in Hypertrophic Cardiomyopathy. Circ. Rep. 2021, 3, 594–603. [Google Scholar] [CrossRef] [PubMed]
- Lakdawala, N.K.; Olivotto, I.; Day, S.M.; Han, L.; Ashley, E.A.; Michels, M.; Ingles, J.; Semsarian, C.; Jacoby, D.; Jefferies, J.L.; et al. Associations Between Female Sex, Sarcomere Variants, and Clinical Outcomes in Hypertrophic Cardiomyopathy. Circ. Genom. Precis Med. 2021, 14, e003062. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Kim, B.; Choi, Y.J.; Lee, H.J.; Lee, H.; Park, J.B.; Lee, S.P.; Han, K.D.; Kim, Y.J.; Kim, H.K. Sex differences in the prognosis of patients with hypertrophic cardiomyopathy. Sci. Rep. 2021, 11, 4854. [Google Scholar] [CrossRef] [PubMed]
- Butters, A.; Lakdawala, N.K.; Ingles, J. Sex Differences in Hypertrophic Cardiomyopathy: Interaction With Genetics and Environment. Curr. Heart Fail. Rep. 2021, 18, 264–273. [Google Scholar] [CrossRef]
- Lind, J.M.; Chiu, C.; Ingles, J.; Yeates, L.; Humphries, S.E.; Heather, A.K.; Semsarian, C. Sex hormone receptor gene variation associated with phenotype in male hypertrophic cardiomyopathy patients. J. Mol. Cell Cardiol. 2008, 45, 217–222. [Google Scholar] [CrossRef]
- Marsiglia, J.D.; Credidio, F.L.; de Oliveira, T.G.; Reis, R.F.; Antunes Mde, O.; de Araujo, A.Q.; Pedrosa, R.P.; Barbosa-Ferreira, J.M.; Mady, C.; Krieger, J.E.; et al. Screening of MYH7, MYBPC3, and TNNT2 genes in Brazilian patients with hypertrophic cardiomyopathy. Am. Heart J. 2013, 166, 775–782. [Google Scholar] [CrossRef]
- Rowin, E.J.; Maron, M.S.; Wells, S.; Patel, P.P.; Koethe, B.C.; Maron, B.J. Impact of Sex on Clinical Course and Survival in the Contemporary Treatment Era for Hypertrophic Cardiomyopathy. J. Am. Heart Assoc. 2019, 8, e012041. [Google Scholar] [CrossRef]
- Mosca, L.; Ferris, A.; Fabunmi, R.; Robertson, R.M.; American Heart, A. Tracking women’s awareness of heart disease: An American Heart Association national study. Circulation 2004, 109, 573–579. [Google Scholar] [CrossRef] [Green Version]
- Collins, P.; Stevenson, J.C.; Mosca, L. Spotlight on gender. Cardiovasc. Res. 2002, 53, 535–537. [Google Scholar] [CrossRef] [Green Version]
- Greendale, G.A.; Lee, N.P.; Arriola, E.R. The menopause. Lancet 1999, 353, 571–580. [Google Scholar] [CrossRef]
- Ommen, S.R.; Mital, S.; Burke, M.A.; Day, S.M.; Deswal, A.; Elliott, P.; Evanovich, L.L.; Hung, J.; Joglar, J.A.; Kantor, P.; et al. 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients With Hypertrophic Cardiomyopathy: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2020, 142, e558–e631. [Google Scholar] [CrossRef] [PubMed]
- Van Driel, B.; Nijenkamp, L.; Huurman, R.; Michels, M.; van der Velden, J. Sex differences in hypertrophic cardiomyopathy: New insights. Curr. Opin. Cardiol. 2019, 34, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Olivotto, I.; Cecchi, F.; Poggesi, C.; Yacoub, M.H. Patterns of disease progression in hypertrophic cardiomyopathy: An individualized approach to clinical staging. Circ. Heart Fail. 2012, 5, 535–546. [Google Scholar] [CrossRef] [Green Version]
- Ommen, S.R.; Shah, P.M.; Tajik, A.J. Left ventricular outflow tract obstruction in hypertrophic cardiomyopathy: Past, present and future. Heart 2008, 94, 1276–1281. [Google Scholar] [CrossRef] [PubMed]
- Nogales-Romo, M.T.; Cecconi, A.; Olivera, M.J.; Caballero, P.; Hernández, S.; Jiménez-Borreguero, L.J.; Alfonso, F. Sex differences in cardiac magnetic resonance features in patients with hypertrophic cardiomyopathy. Int. J. Cardiovasc. Imaging 2020, 36, 1751–1759. [Google Scholar] [CrossRef]
- Lorenzini, M.; Anastasiou, Z.; O’Mahony, C.; Guttman, O.P.; Gimeno, J.R.; Monserrat, L.; Anastasakis, A.; Rapezzi, C.; Biagini, E.; Garcia-Pavia, P.; et al. Mortality Among Referral Patients With Hypertrophic Cardiomyopathy vs the General European Population. JAMA Cardiol. 2020, 5, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Tafelmeier, M.; Baessler, A.; Wagner, S.; Unsoeld, B.; Preveden, A.; Barlocco, F.; Tomberli, A.; Popovic, D.; Brennan, P.; MacGowan, G.A.; et al. Design of the SILICOFCM study: Effect of sacubitril/valsartan vs lifestyle intervention on functional capacity in patients with hypertrophic cardiomyopathy. Clin. Cardiol. 2020, 43, 430–440. [Google Scholar] [CrossRef] [Green Version]
- Preveden, A.; Golubovic, M.; Bjelobrk, M.; Miljkovic, T.; Stojsic, S.; Ilic, A.; Gajic, D.; Stojsic-Milosavljevic, A.; Velicki, L. Hypertrophic cardiomyopathy: Perspectives of drug therapy. Srce Krvni Sudovi. 2021, 40, 19–25. [Google Scholar]
- Marian, A.J.; Braunwald, E. Hypertrophic Cardiomyopathy: Genetics, Pathogenesis, Clinical Manifestations, Diagnosis, and Therapy. Circ. Res. 2017, 121, 749–770. [Google Scholar] [CrossRef]
- Coppini, R.; Santini, L.; Olivotto, I.; Ackerman, M.J.; Cerbai, E. Abnormalities in sodium current and calcium homoeostasis as drivers of arrhythmogenesis in hypertrophic cardiomyopathy. Cardiovasc. Res. 2020, 116, 1585–1599. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall | Females | Males | p Value | |
|---|---|---|---|---|
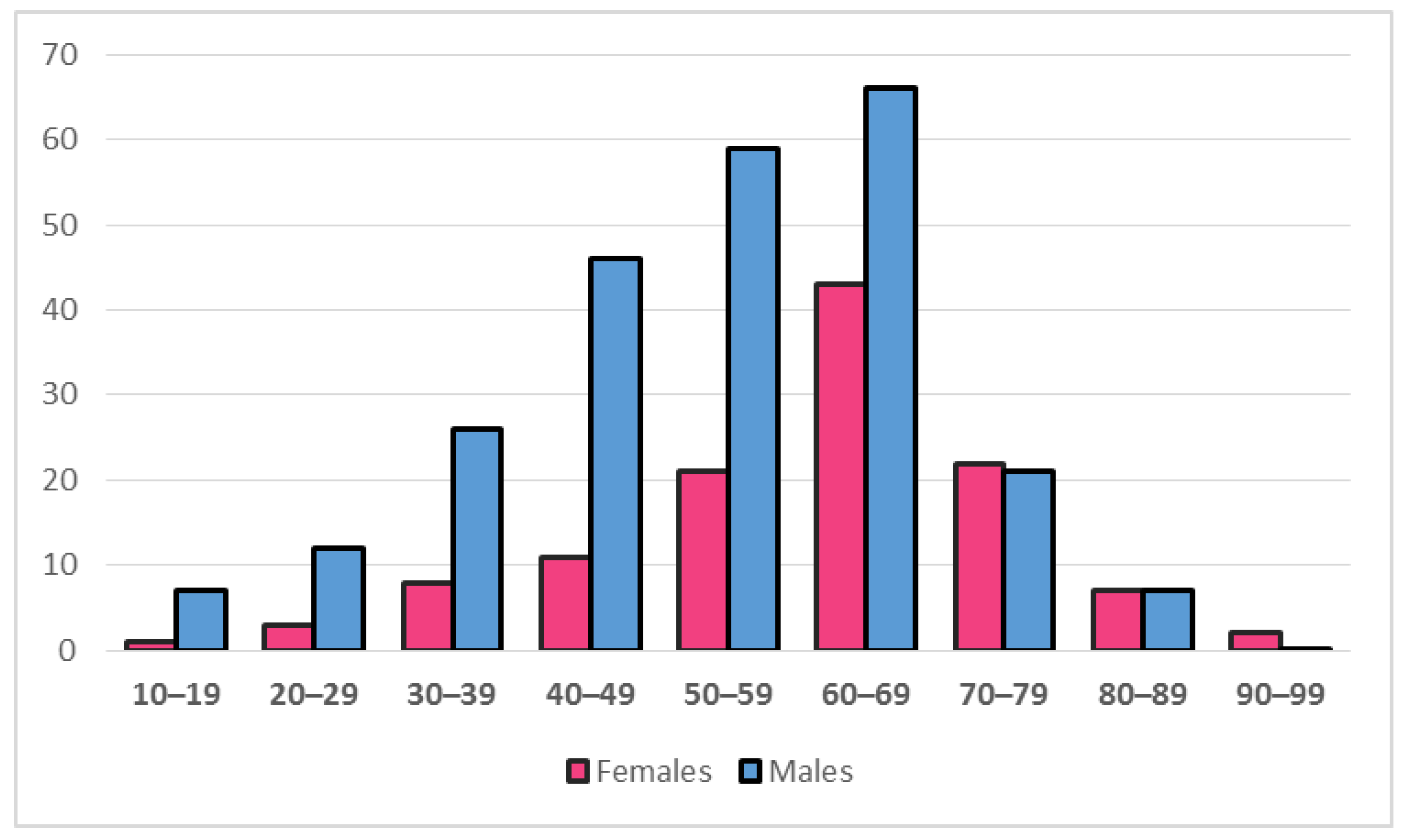
| Number of patients | 362 (100.0%) | 118 (32.6%) | 244 (67.4%) | |
| Age (years) | 57 (46–67) | 64.5 (54–70) | 53.5 (42–64) | <0.0005 * |
| Age ≥ 50 years | 248 (68.5%) | 95 (80.5%) | 153 (62.7%) | 0.001 * |
| Body mass index (kg/m2) | 27.2 (23.9–30.0) | 25.9 (22.8–29.9) | 27.5 (24.5–30.0) | 0.029 * |
| Symptoms | ||||
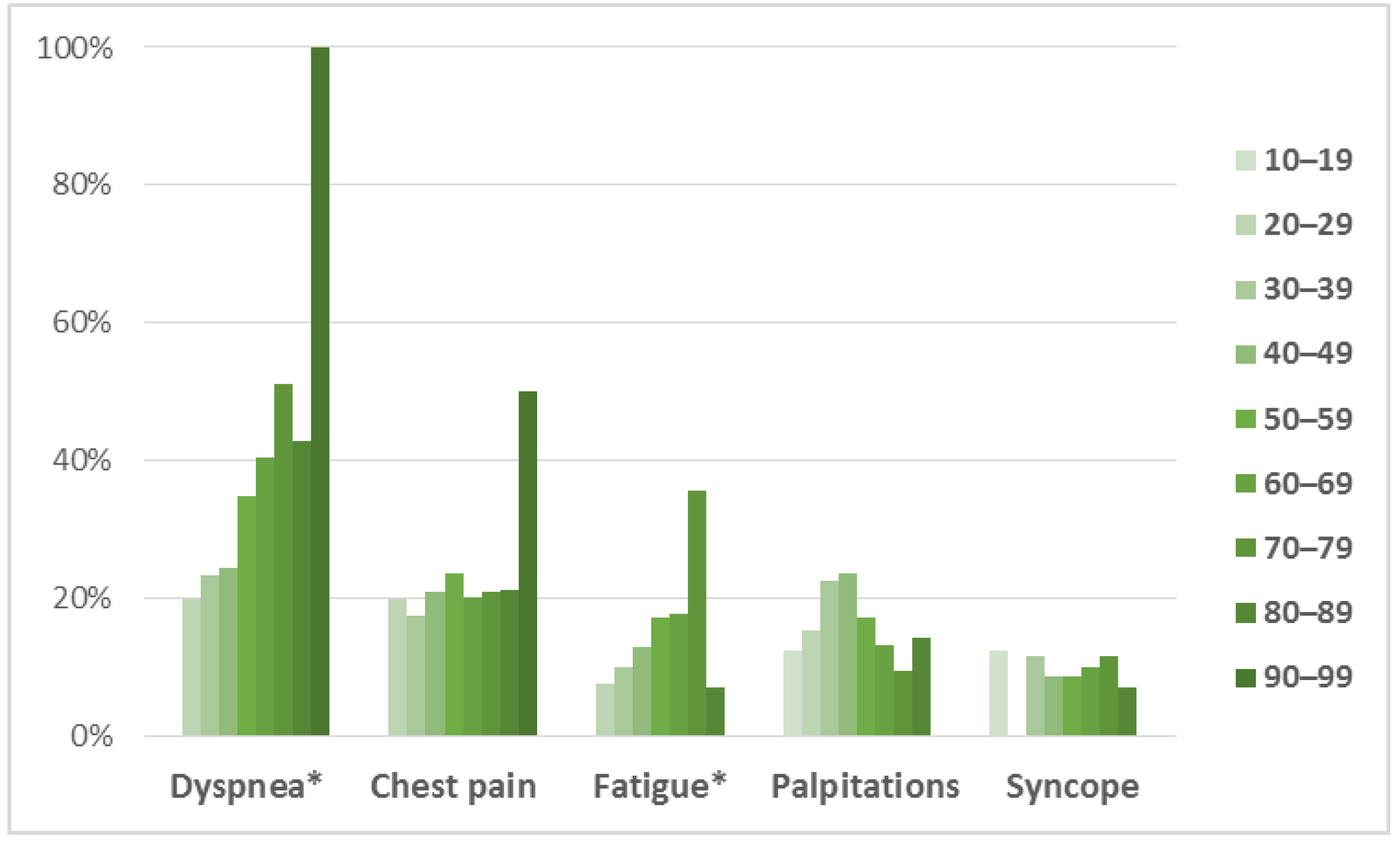
| Fatigue | 59 (17.2%) | 30 (25.9%) | 29 (12.7%) | 0.004 * |
| Dyspnea | 127 (36.8%) | 58 (50.4%) | 69 (30.0%) | <0.0005 * |
| Chest pain | 75 (21.6%) | 35 (30.2%) | 40 (17.3%) | 0.009 * |
| Palpitations | 56 (16.2%) | 25 (21.6%) | 31 (13.5%) | 0.077 |
| Syncope | 34 (9.8%) | 15 (12.9%) | 19 (8.2%) | 0.230 |
| Other | 15 (10.4%) | 9 (17.6%) | 6 (6.5%) | 0.047 * |
| NYHA classification | ||||
| I | 183 (59.8%) | 50 (48.1%) | 133 (65.8%) | 0.007 * |
| II | 96 (31.4%) | 40 (38.5%) | 56 (27.7%) | |
| III | 27 (8.8%) | 14 (13.5%) | 13 (6.4%) | |
| Comorbidities | ||||
| Diabetes mellitus | 47 (13.6%) | 19 (16.5%) | 28 (12.1%) | 0.338 |
| Thyroid disease | 32 (9.3%) | 19 (16.5%) | 13 (5.7%) | 0.002 * |
| Renal dysfunction | 16 (4.7%) | 8 (7.0%) | 8 (3.5%) | 0.177 |
| Hepatic dysfunction | 3 (0.9%) | 1 (0.9%) | 2 (0.9%) | 1.000 |
| COPD | 16 (4.6%) | 5 (4.3%) | 11 (4.8%) | 1.000 |
| Anemia | 7 (1.9%) | 4 (3.4%) | 3 (1.2%) | 0.162 |
| Neuromuscular disease | 3 (0.9%) | 2 (1.8%) | 1 (0.4%) | 0.253 |
| Positive family history | ||||
| HCM | 72 (43.6%) | 26 (46.4%) | 46 (42.2%) | 0.724 |
| Sudden cardiac death | 30 (8.3%) | 16 (13.5%) | 14 (5.7%) | 0.011 * |
| Vital signs | ||||
| Systolic blood pressure (mmHg) | 120 (110–140) | 120 (110–140) | 123 (115–140) | 0.169 |
| Diastolic blood pressure (mmHg) | 78 (70–80) | 70 (67–82.5) | 80 (70–80) | 0.052 |
| Heart rate (beats per minute) | 64 (57–73) | 64 (59–75) | 63 (57–70) | 0.203 |
| Laboratory results | ||||
| Sodium (mmol/L) | 140 (193–142) | 140 (193–142) | 140 (193–142) | 0.920 |
| Potassium (mmol/L) | 4.2 (4.0–4.5) | 4.1 (3.9–4.3) | 4.3 (4.0–4.6) | 0.001 * |
| Blood urea nitrogen (mmol/L) | 6.4 (4.9–9.6) | 5.7 (4.2–6.8) | 7.2 (5.3–10.7) | <0.0005 * |
| Creatinine (µmol/L) | 82 (70–98) | 80 (66–94) | 82 (71–102) | 0.176 |
| Uric acid (µmol/L) | 352 (287–417) | 355 (277–415) | 351 (294–416) | 0.980 |
| ALT (U/L) | 27 (19–39) | 30 (21–39) | 26 (19–37) | 0.151 |
| AST (U/L) | 23 (18–33) | 25 (17–39) | 23 (18–31) | 0.137 |
| LDH (U/L) | 216 (176–275) | 222 (196–283) | 209 (169–267) | 0.092 |
| Total protein (g/L) | 72 (67–76) | 75 (69–78) | 71 (67–75) | 0.064 |
| Albumin (g/L) | 42 (36–45) | 40 (36–43) | 46 (44–49) | <0.0005 * |
| Creatine kinase (U/L) | 105 (67–145) | 111 (71–164) | 104 (66–134) | 0.479 |
| LDL cholesterol (mmol/L) | 3.1 (±1.0) | 3.0 (±1.0) | 3.3 (±1.0) | 0.129 |
| HDL cholesterol (mmol/L) | 1.2 (1.0–1.5) | 1.3 (1.1–1.5) | 1.2 (1.0–1.5) | 0.258 |
| NT-proBNP (ng/L) | 728 (291–1789) | 571 (173–1507) | 794 (372–1857) | 0.244 |
| KERRYPNX | Overall | Females | Males | p Value |
|---|---|---|---|---|
| Sinus rhythm | 277 (78.5%) | 87 (75.7%) | 190 (79.8%) | 0.449 |
| Atrial flutter | 11 (3.1%) | 4 (3.5%) | 7 (2.9%) | 0.753 |
| Atrial fibrillation | 54 (15.3%) | 22 (19.1%) | 32 (13.4%) | 0.218 |
| PSVT | 7 (2.3%) | 6 (5.7%) | 1 (0.5%) | 0.007 * |
| Ventricular tachycardia | 25 (8.1%) | 7 (6.7%) | 18 (8.9%) | 0.661 |
| PR interval (ms) | 182 (160–206) | 177 (160–200) | 184 (161–207) | 0.206 |
| QRS duration (ms) | 108 (94–127) | 106 (90–132) | 108 (96–124) | 0.448 |
| Sokolow-Lyon index (mm) | 30 (22–37) | 26 (21–35) | 32 (25–38) | 0.166 |
| Significant Q waves | 47 (13.0%) | 13 (11.0%) | 34 (13.4%) | 0.342 |
| ST segment abnormalities | 85 (23.5%) | 34 (28.8%) | 51 (20.9%) | 0.096 |
| Negative T waves | 155 (42.8%) | 62 (52.5%) | 93 (38.1%) | 0.017 * |
| LBBB | 31 (8.6%) | 12 (10.2%) | 19 (7.8%) | 0.448 |
| RBBB | 32 (8.8%) | 12 (10.2%) | 20 (8.2%) | 0.535 |
| Overall | Females | Males | p Value | |
|---|---|---|---|---|
| Interventicular septum thickness (mm) | 17 (15–21) | 18 (15–20) | 17 (15–21) | 0.121 |
| Posterolateral wall thickness (mm) | 13 (10–15) | 13 (11–14) | 12 (10–15) | 0.656 |
| LA diameter (mm) | 43 (39–49) | 34 (32–37) | 44 (39–49) | <0.0005 * |
| LA volume (ml) | 82 (59–107) | 54 (35–67) | 85 (64–110) | <0.0005 * |
| LA volume/BSA (ml/m2) | 39 (27–52) | 28 (20–36) | 40 (28–53) | 0.003 * |
| LVEDD (mm) | 47 (42–51) | 45 (42–50) | 48 (44–53) | 0.009 * |
| LVESD (mm) | 28.6 (±7.4) | 26.5 (±6.1) | 29.2 (±7.7) | 0.036 * |
| LVEF (%) | 60 (55–65) | 55 (55–66) | 60 (55–64) | 0.672 |
| E/E’ ratio | 10 (8–14) | 11 (8–14) | 10 (8–14) | 0.900 |
| Diastolic dysfunction | 198 (54.7%) | 48 (40.7%) | 150 (61.5%) | <0.0005 * |
| LVOT gradient (mmHg) | 9 (5–15) | 18 (10–36) | 7 (5–13) | <0.0005 * |
| LVOT gradient >30 mmHg | 28 (7.7%) | 13 (11.0%) | 15 (6.1%) | 0.104 |
| Mitral valve abnormalities | 0.020 * | |||
| Systolic anterior motion | 50 (13.8%) | 10 (8.5 %) | 40 (16.4%) | |
| Papillary muscle abnormalities | 13 (3.6%) | 0 (0.0%) | 13 (5.3%) | 0.005 * |
| Mitral leaflet abnormalities | 80 (22.1%) | 4 (3.4 %) | 76 (31.1%) | <0.0005 * |
| Calcification of mitral annulus | 28 (7.7%) | 1 (0.8%) | 27 (11.1%) | <0.0005 * |
| Myocardial fibrosis | 13 (3.6%) | 0 (0.0%) | 13 (5.3%) | 0.006 * |
| Wall motion abnormalities | ||||
| Hypokinesia | 50 (13.8%) | 1 (0.8%) | 49 (20.1%) | <0.0005 * |
| Akinesia | 14 (3.9%) | 1 (0.8%) | 13 (5.3%) | 0.014 * |
| Dyskinesia | 60 (16.6%) | 47 (39.8%) | 13 (5.3%) | <0.0005 * |
| TAPSE (mm) | 22 (20–26) | 22 (20–24) | 23 (20–26) | 0.436 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Preveden, A.; Golubovic, M.; Bjelobrk, M.; Miljkovic, T.; Ilic, A.; Stojsic, S.; Gajic, D.; Glavaski, M.; Maier, L.S.; Okwose, N.; et al. Gender Related Differences in the Clinical Presentation of Hypertrophic Cardiomyopathy—An Analysis from the SILICOFCM Database. Medicina 2022, 58, 314. https://doi.org/10.3390/medicina58020314
Preveden A, Golubovic M, Bjelobrk M, Miljkovic T, Ilic A, Stojsic S, Gajic D, Glavaski M, Maier LS, Okwose N, et al. Gender Related Differences in the Clinical Presentation of Hypertrophic Cardiomyopathy—An Analysis from the SILICOFCM Database. Medicina. 2022; 58(2):314. https://doi.org/10.3390/medicina58020314
Chicago/Turabian StylePreveden, Andrej, Miodrag Golubovic, Marija Bjelobrk, Tatjana Miljkovic, Aleksandra Ilic, Snezana Stojsic, Dragan Gajic, Mila Glavaski, Lars S. Maier, Nduka Okwose, and et al. 2022. "Gender Related Differences in the Clinical Presentation of Hypertrophic Cardiomyopathy—An Analysis from the SILICOFCM Database" Medicina 58, no. 2: 314. https://doi.org/10.3390/medicina58020314
APA StylePreveden, A., Golubovic, M., Bjelobrk, M., Miljkovic, T., Ilic, A., Stojsic, S., Gajic, D., Glavaski, M., Maier, L. S., Okwose, N., Popovic, D., Barlocco, F., Ristic, A., MacGowan, G. A., Olivotto, I., Filipovic, N., Jakovljevic, D. G., & Velicki, L. (2022). Gender Related Differences in the Clinical Presentation of Hypertrophic Cardiomyopathy—An Analysis from the SILICOFCM Database. Medicina, 58(2), 314. https://doi.org/10.3390/medicina58020314