
Prevalence and Antifungal Susceptibility Profile of Oral Candida spp. Isolates from a Hospital in Slovakia



Abstract
:1. Introduction
2. Materials and Methods
2.1. Collection and Identification of the Clinical Isolates
2.1.1. Germ-Tube Formation Test, CHROMID® Candida, Auxacolor 2 (Bio-Rad®) Test
2.1.2. The ID 32C Automated Method
2.2. Antifungal Susceptibility Testing
2.3. Software and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- WHO. Oral Health—WHO Fact Sheets. Available online: https://www.who.int/news-room/fact-sheets/detail/oral-health (accessed on 15 January 2019).
- Tonetti, M.S.; Jepsen, S.; Jin, L.; Otomo-Corgel, J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: A call for global action. J. Clin. Periodontol. 2017, 44, 456–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, D.; Lewis, M. Pathogenesis and treatment of oral candidosis. J. Oral Microbiol. 2011, 3, 5771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bongomin, F.; Gago, S.; Oladele, R.; Denning, D. Global and Multi-National Prevalence of Fungal Diseases—Estimate Precision. J. Fungi 2017, 3, 57. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.A.O.; Williams, D.W. Diagnosis and management of oral candidosis. BDJ 2017, 223, 675–681. [Google Scholar] [PubMed] [Green Version]
- Taylor, M.; Raja, A. Oral Candidiasis (Thrush); StatPearls Publishing: Treasure Island, FL, USA, 2019. [Google Scholar]
- Andrade, J.C.; Kumar, S.; Kumar, A.; Černáková, L.; Rodrigues, C.F. Application of probiotics in candidiasis management. Crit. Rev. Food Sci. Nutr. 2021, 2021, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Salehi, B.; Kregiel, D.; Mahady, G.; Sharifi-Rad, J.; Martins, N.; Rodrigues, C.F. Management of Streptococcus mutans-Candida spp. Oral Biofilms’ Infections: Paving the Way for Effective Clinical Interventions. J. Clin. Med. 2020, 9, 517. [Google Scholar] [CrossRef] [Green Version]
- Benito-Cruz, B.; Aranda-Romo, S.; López-Esqueda, F.J.; de la Rosa-García, E.; Rosas-Hernández, R.; Sánchez-Vargas, L.O. Oral Candida isolates and fluconazole susceptibility patterns in older Mexican women. Arch. Gerontol. Geriatr. 2016, 65, 204–210. [Google Scholar] [CrossRef]
- Neville, B.W.; Damm, D.D.; Allen, C.M.; Bouquot, J.E. Oral and maxillofacial pathology. In Fungal and Protozoal Diseases; Elsevier: London, UK, 2011; pp. 213–221. [Google Scholar]
- Regezi, J.; Sciubba, J.; Jordan, R. Oral pathology clinical pathologic correlations. In White Lesions; Elsevier: St. Louis, MO, USA, 2008; pp. 98–102. [Google Scholar]
- Javed, F.; Klingspor, L.; Sundin, U.; Altamash, M.; Klinge, B.; Engström, P.-E. Periodontal conditions, oral Candida albicans and salivary proteins in type 2 diabetic subjects with emphasis on gender. BMC Oral Health 2009, 9, 12. [Google Scholar] [CrossRef] [Green Version]
- Al Mubarak, S.; Robert, A.A.; Baskaradoss, J.K.; Al-Zoman, K.; Al Sohail, A.; Alsuwyed, A.; Ciancio, S. The prevalence of oral Candida infections in periodontitis patients with type 2 diabetes mellitus. J. Infect. Public Health 2013, 6, 296–301. [Google Scholar] [CrossRef]
- Lamey, P.J.; Darwaza, A.; Fisher, B.M.; Samaranayake, L.P.; Macfarlane, T.W.; Frier, B.M. Secretor status, candidal carriage and candidal infection in patients with diabetes mellitus. J. Oral Pathol. 1988, 17, 354–357. [Google Scholar] [CrossRef] [PubMed]
- Mulu, A.; Kassu, A.; Anagaw, B.; Moges, B.; Gelaw, A.; Alemayehu, M.; Belyhun, Y.; Biadglegne, F.; Hurissa, Z.; Moges, F.; et al. Frequent detection of ‘azole’ resistant Candida species among late presenting AIDS patients in northwest Ethiopia. BMC Infect. Dis. 2013, 13, 82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goregen, M.; Miloglu, O.; Buyukkurt, M.C.; Caglayan, F.; Aktas, A.E. Median rhomboid glossitis: A clinical and microbiological study. Eur. J. Dent. 2011, 5, 367–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arendorf, T.M.; Walker, D.M. Tobacco smoking and denture wearing as local aetiological factors in median rhomboid glossitis. Int. J. Oral Surg. 1984, 13, 411–415. [Google Scholar] [CrossRef]
- Flaitz, C.M.; Nichols, C.M.; Hicks, M.J. An overview of the oral manifestations of AIDS-related Kaposi’s sarcoma. Compend. Contin. Educ. Dent. 1995, 16, 136–138. [Google Scholar] [PubMed]
- Kumar, B.V.; Padshetty, N.S.; Bai, K.Y.; Rao, M.S. Prevalence of Candida in the oral cavity of diabetic subjects. J. Assoc. Physicians India 2005, 53, 599–602. [Google Scholar]
- Lott, T.J.; Holloway, B.P.; Logan, D.A.; Fundyga, R.; Arnold, J. Towards understanding the evolution of the human commensal yeast Candida albicans. Microbiology 1999, 145, 1137–1143. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, C.; Rodrigues, M.; Henriques, M. Candida sp. Infections in Patients with Diabetes Mellitus. J. Clin. Med. 2019, 8, 76. [Google Scholar] [CrossRef] [Green Version]
- Černáková, L.; Rodrigues, C.F. Microbial interactions and immunity response in oral Candida species. Future Microbiol. 2020, 15, 1653–1677. [Google Scholar] [CrossRef]
- Panariello, B.H.D.; de Araújo Costa, C.A.G.; Pavarina, A.C.; Santiago, S.L.; Duarte, S. Advances and Challenges in Oral Biofilm Control. Curr. Oral Health Rep. 2017, 4, 29–33. [Google Scholar] [CrossRef]
- Rodrigues, C.C.F.; Gonçalves, B.; Rodrigues, M.M.E.; Silva, S.; Azeredo, J.; Henriques, M. The Effectiveness of Voriconazole in Therapy of Candida glabrata’s Biofilms Oral Infections and Its Influence on the Matrix Composition and Gene Expression. Mycopathologia 2017, 182, 653–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, C.F.; Henriques, M. Liposomal and Deoxycholate Amphotericin B Formulations: Effectiveness against Biofilm Infections of Candida spp. Pathogens 2017, 6, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanz, M.; Beighton, D.; Curtis, M.A.; Cury, J.A.; Dige, I.; Dommisch, H.; Ellwood, R.; Giacaman, R.A.; Herrera, D.; Herzberg, M.C.; et al. Role of microbial biofilms in the maintenance of oral health and in the development of dental caries and periodontal diseases. Consensus report of group 1 of the Joint EFP/ORCA workshop on the boundaries between caries and periodontal disease. J. Clin. Periodontol. 2017, 44, S5–S11. [Google Scholar] [CrossRef] [PubMed]
- BDJ Team. Antibiotic resistance among patients with severe gum disease is increasing. BDJ Team 2018, 5, 18117. [Google Scholar] [CrossRef]
- Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of oral diseases and risks to oral health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar]
- Han, Y.W.; Wang, X. Mobile microbiome: Oral bacteria in extra-oral infections and inflammation. J. Dent. Res. 2013, 92, 485–491. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, C.; Henriques, M. Oral mucositis caused by Candida glabrata biofilms: Failure of the concomitant use of fluconazole and ascorbic acid. Ther. Adv. Infect. Dis. 2017, 4, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Vanden Abbeele, A.; de Meel, H.; Ahariz, M.; Perraudin, J.-P.; Beyer, I.; Courtois, P. Denture contamination by yeasts in the elderly. Gerodontology 2008, 25, 222–228. [Google Scholar] [CrossRef] [Green Version]
- Sendid, B.; Salvetat, N.; Sarter, H.; Loridant, S.; Cunisse, C.; François, N.; Aijjou, R.; Gelé, P.; Leroy, J.; Deplanque, D.; et al. A pilot clinical study on post-operative recurrence provides biological clues for a role of candida yeasts and fluconazole in Crohn’s disease. J. Fungi 2021, 7, 324. [Google Scholar] [CrossRef]
- Moorhouse, A.J.; Moreno-Lopez, R.; Gow, N.A.R.; Hijazi, K. Clonal evolution of Candida albicans, Candida glabrata and Candida dubliniensis at oral niche level in health and disease. J. Oral Microbiol. 2021, 13, 1894047. [Google Scholar] [CrossRef] [PubMed]
- Černáková, L.; Light, C.; Salehi, B.; Rogel-Castillo, C.; Victoriano, M.; Martorell, M.; Sharifi-Rad, J.; Martins, N.; Rodrigues, C.F. Novel Therapies for Biofilm-Based Candida spp. Infections. Adv. Exp. Med. Biol. 2019, 1214, 93–123. [Google Scholar] [PubMed]
- Doi, A.M.; Pignatari, A.C.C.; Edmond, M.B.; Marra, A.R.; Camargo, L.F.A.; Siqueira, R.A.; da Mota, V.P.; Colombo, A.L. Epidemiology and Microbiologic Characterization of Nosocomial Candidemia from a Brazilian National Surveillance Program. PLoS ONE 2016, 11, e0146909. [Google Scholar] [CrossRef] [PubMed]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2015, 62, e1–e50. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing EUCAST Breakpoint Tables for Interpretation of MICs for Antifungal Agents v.10.0. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/AFST/Clinical_breakpoints/AFST_BP_v10.0_200204_updatd_links_200924.pdf (accessed on 20 February 2022).
- Pfaller, M.A.; Diekema, D.J. Epidemiology of invasive candidiasis: A persistent public health problem. Clin. Microbiol. Rev. 2007, 20, 133–163. [Google Scholar] [CrossRef] [Green Version]
- Rodrigues, C.F.; Rodrigues, M.E.; Henriques, M.C.R. Promising alternative therapeutics for oral candidiasis. Curr. Med. Chem. 2018, 25, 2515–2528. [Google Scholar] [CrossRef]
- Hajjeh, R.A.; Sofair, A.N.; Harrison, L.H.; Lyon, G.M.; Arthington-Skaggs, B.A.; Mirza, S.A.; Phelan, M.; Morgan, J.; Lee-Yang, W.; Ciblak, M.A.; et al. Incidence of bloodstream infections due to Candida species and in vitro susceptibilities of isolates collected from 1998 to 2000 in a population-based active surveillance program. J. Clin. Microbiol. 2004, 42, 1519–1527. [Google Scholar] [CrossRef] [Green Version]
- Horn, D.L.; Neofytos, D.; Anaissie, E.J.; Fishman, J.A.; Steinbach, W.J.; Olyaei, A.J.; Marr, K.A.; Pfaller, M.A.; Chang, C.; Webster, K.M. Epidemiology and Outcomes of Candidemia in 2019 Patients: Data from the Prospective Antifungal Therapy Alliance Registry. Clin. Infect. Dis. 2009, 48, 1695–1703. [Google Scholar] [CrossRef]
- Krcmery, V.; Barnes, A.J. Non-albicans Candida spp. causing fungaemia: Pathogenicity and antifungal resistance. J. Hosp. Infect. 2002, 50, 243–260. [Google Scholar] [CrossRef]
- Miranda, L.N.; van der Heijden, I.M.; Costa, S.F.; Sousa, A.P.I.; Sienra, R.A.; Gobara, S.; Santos, C.R.; Lobo, R.D.; Pessoa, V.P.; Levin, A.S. Candida colonisation as a source for candidaemia. J. Hosp. Infect. 2009, 72, 9–16. [Google Scholar] [CrossRef]
- Katz, J. Prevalence of candidiasis and oral candidiasis in COVID-19 patients: A cross-sectional pilot study from the patients’ registry in a large health center. Quintessence Int. 2021, 52, 714–718. [Google Scholar] [PubMed]
- Naidu, G.S.; Thakur, R.; Singh, A.K.; Rajbhandary, S.; Mishra, R.K.; Sagtani, A. Oral lesions and immune status of HIV infected adults from eastern Nepal. J. Clin. Exp. Dent. 2013, 5, e1–e7. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Fay, V.; Schäffer Gregianini, T.; Gorini da Veiga, A.B.; Bottin Gonçalves, S.M.; Rodrigues, D.M.; Bonamigo, R.R. A 12-year study of fungal infections in Rio Grande do Sul, Southern Brazil. Rev. Iberoam. Micol. 2019, 36, 55–60. [Google Scholar]
- Gupta, B.; Gupta, S.; Chaudhary, M.; Raj, A.T.; Awan, K.H.; Patil, S. Oral candida prevalence and species specificity in leprosy. Disease Month 2020, 66, 100920. [Google Scholar] [CrossRef] [PubMed]
- Esebelahie, N.O.; Enweani, I.B.; Omoregie, R. Candida colonisation in asymptomatic HIV patients attending a tertiary hospital in Benin City, Nigeria. Libyan J. Med. 2013, 8, 20322. [Google Scholar] [CrossRef] [Green Version]
- Álvaro-Meca, A.; Jensen, J.; Micheloud, D.; Díaz, A.; Gurbindo, D.; Resino, S. Rate of candidiasis among HIV-infected children in Spain in the era of highly active antiretroviral therapy (1997–2008). BMC Infect. Dis. 2013, 13, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arslan, S.; Koç, A.N.; Şekerci, A.E.; Tanriverdi, F.; Sav, H.; Aydemir, G.; Diri, H. Genotypes and virulence factors of Candida species isolated from oralcavities of patients with type 2 diabetes mellitus. Turk. J. Med. Sci. 2016, 46, 18–27. [Google Scholar] [CrossRef]
- Aitken-Saavedra, J.; Lund, R.G.; González, J.; Huenchunao, R.; Perez-Vallespir, I.; Morales-Bozo, I.; Urzúa, B.; Tarquinio, S.C.; Maturana-Ramírez, A.; Martos, J.; et al. Diversity, frequency and antifungal resistance of Candida species in patients with type 2 diabetes mellitus. Acta Odontol. Scand. 2018, 76, 580–586. [Google Scholar] [CrossRef]
- Indira, P.; Kumar, P.M.; Shalini, S.; Vaman, K. Opportunistic infections among People Living with HIV (PLHIV) with Diabetes Mellitus (DM) attending a tertiary care hospital in coastal city of South India. PLoS ONE 2015, 10, e0136280. [Google Scholar] [CrossRef]
- Wu, J.; Gan, C.; Li, J.; Liu, Y.; Chen, Z.; Zhang, Y.; Yi, G.; Sui, J.; Xu, J. Species Diversity and Antifungal Susceptibilities of Oral Yeasts from Patients with Head and Neck Cancer. Infect. Drug Resist. 2021, 14, 2279–2288. [Google Scholar] [CrossRef]
- Maheronnaghsh, M.; Fatahinia, M.; Dehghan, P.; Teimoori, A. Identification of Candida Species and Antifungal Susceptibility in Cancer Patients with Oral Lesions in Ahvaz, Southern West of Iran. Adv. Biomed. Res. 2020, 9, 50. [Google Scholar] [PubMed]
- Xiao, J.L.; Xu, G.C.; de Hoog, S.; Qiao, J.J.; Fang, H.; Li, Y.L. Oral Prevalence of Candida Species in Patients Undergoing Systemic Glucocorticoid Therapy and the Antifungal Sensitivity of the Isolates. Infect. Drug Resist. 2020, 13, 2601–2607. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.; Silva, S.; Azeredo, J.; Henriques, M. Candida glabrata’s recurrent infections: Biofilm formation during Amphotericin B treatment. Lett. Appl. Microbiol. 2016, 63, 77–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanitá, P.V.; De Oliveira Mima, E.G.; Pavarina, A.C.; Jorge, J.H.; Machado, A.L.; Vergani, C.E. Susceptibility profile of a Brazilian yeast stock collection of Candida species isolated from subjects with Candida-associated denture stomatitis with or without diabetes. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 562–569. [Google Scholar] [CrossRef] [Green Version]
- Song, Y.B.; Suh, M.K.; Ha, G.Y.; Kim, H. Antifungal susceptibility testing with etest for Candida species isolated from patients with oral candidiasis. Ann. Dermatol. 2015, 27, 715–720. [Google Scholar] [CrossRef] [Green Version]
- LaFleur, M.; Qingguo, Q.; Lewis, K. Patients with long-term oral carriage harbor high-persister mutants of Candida albicans. Antimicrob. Agents Chemother. 2010, 54, 39–44. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, T.; Imamura, A. A case of chronic mucocutaneous candidasis cured with micafungin. Kansenshogaku Zasshi. 2005, 79, 143–148. [Google Scholar] [CrossRef]
- Rajakumari, M.L.; Saravana Kumari, P. Prevalence of Candida species in the buccal cavity of diabetic and non-diabetic individuals in and around Pondicherry. J. Mycol. Med. 2016, 26, 359–367. [Google Scholar] [CrossRef]
- Premkumar, J.; Ramani, P.; Chandrasekar, T.; Natesan, A.; Premkumar, P. Detection of species diversity in oral candida colonization and anti-fungal susceptibility among non-oral habit adult diabetic patients. J. Nat. Sci. Biol. Med. 2014, 5, 148. [Google Scholar] [CrossRef] [Green Version]
- Mantri, S.S.; Parkhedkar, R.D.; Mantri, S.P. Candida colonisation and the efficacy of chlorhexidine gluconate on soft silicone-lined dentures of diabetic and non-diabetic patients. Gerodontology 2013, 30, 288–295. [Google Scholar] [CrossRef]
- Alves, D.; Borges, P.; Grainha, T.; Rodrigues, C.F.; Pereira, M.O. Tailoring the immobilization and release of chlorhexidine using dopamine chemistry to fight infections associated to orthopedic devices. Mater. Sci. Eng. C 2021, 120, 111742. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
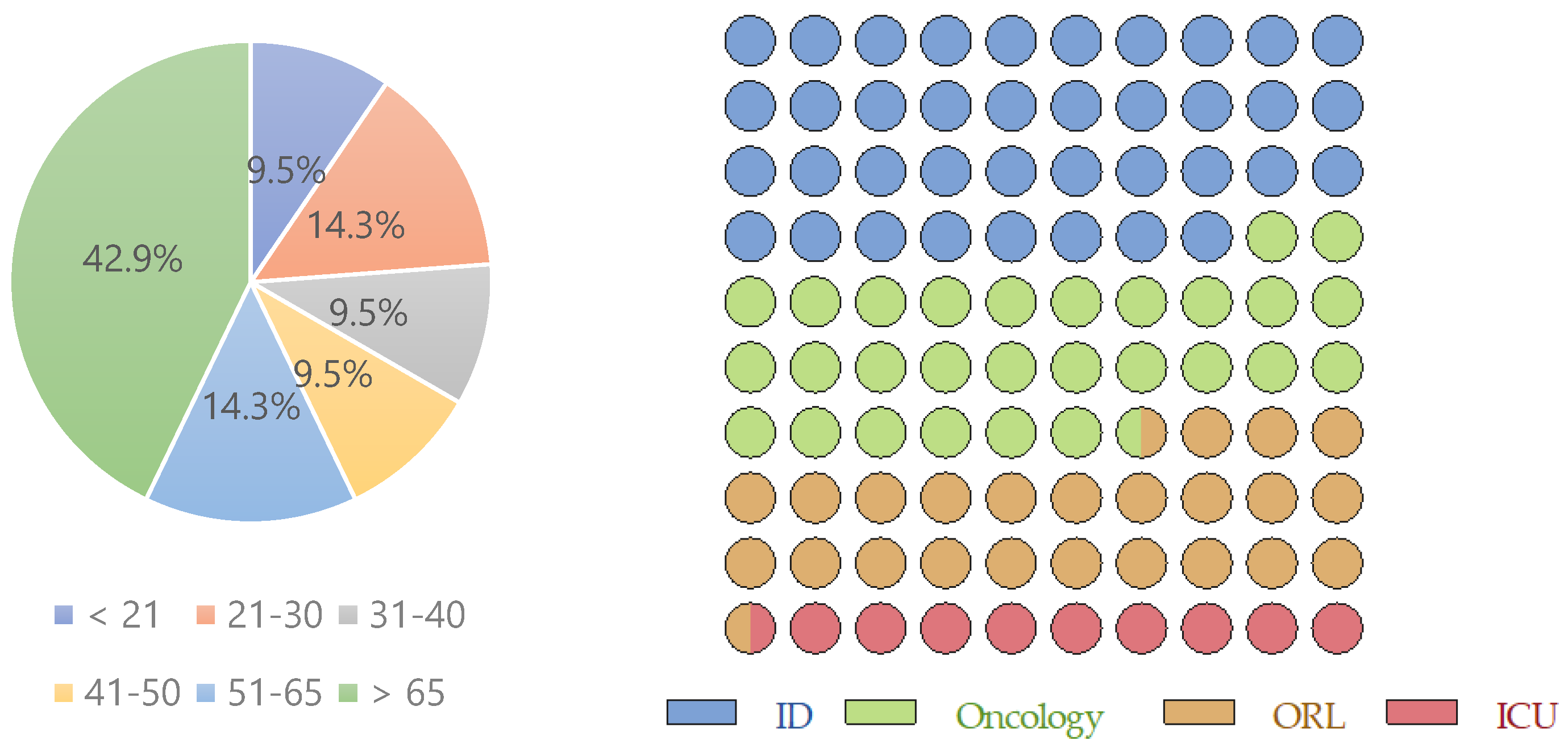
| <21 | 21–30 | 31–40 | 41–50 | 51–65 | >65 | |
|---|---|---|---|---|---|---|
| Female | 1 (4.8%) | 1 (4.8%) | 1 (4.8%) | 1 (4.8%) | 1 (4.8%) | 3 (14.3%) |
| Male | 1 (4.8%) | 2 (9.5%) | 1 (4.8%) | 1 (4.8%) | 2 (9.5%) | 6 (28.6%) |
| Total | 2 (9.5%) | 3 (14.3%) | 2 (9.5%) | 2 (9.5%) | 3 (14.3%) | 9 (42.9%) |
| ID | Oncology | ORL | ICU | |
|---|---|---|---|---|
| Female | 4 (19%) | 2 (9.5%) | 1 (4.8%) | 1 (4.8%) |
| Male | 4 (19%) | 4 (19%) | 4 (19%) | 1 (4.8%) |
| Total | 8 (38.1%) | 6 (28.6%) | 5 (23.8%) | 2 (9.5%) |
| Candida spp. | n | % | Susceptibility Profile | |||
|---|---|---|---|---|---|---|
| Flu | Vcz | 5FC | AmB | |||
| C. albicans | 13 | 61.9 | S | S | R | S |
| S | S | S | S | |||
| S | S | R | S | |||
| S | S | R | S | |||
| S | S | S | S | |||
| S | S | R | S | |||
| S | S | S | S | |||
| S | S | R | S | |||
| S | S | S | S | |||
| S | S | R | S | |||
| S | S | R | S | |||
| S | S | S | S | |||
| S | S | S | S | |||
| C. krusei | 3 | 14.3 | R | S | R | S |
| R | S | R | S | |||
| R | S | S | S | |||
| C. valida | 2 | 9.5 | R | I | S | S |
| R | I | S | S | |||
| C. tropicalis | 1 | 4.8 | S | S | R | S |
| C. glabrata | 1 | 4.8 | S | S | S | S |
| C. intermedia | 1 | 4.8 | R | S | R | S |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Černáková, L.; Líšková, A.; Lengyelová, L.; Rodrigues, C.F. Prevalence and Antifungal Susceptibility Profile of Oral Candida spp. Isolates from a Hospital in Slovakia. Medicina 2022, 58, 576. https://doi.org/10.3390/medicina58050576
Černáková L, Líšková A, Lengyelová L, Rodrigues CF. Prevalence and Antifungal Susceptibility Profile of Oral Candida spp. Isolates from a Hospital in Slovakia. Medicina. 2022; 58(5):576. https://doi.org/10.3390/medicina58050576
Chicago/Turabian StyleČernáková, Lucia, Anna Líšková, Libuša Lengyelová, and Célia F. Rodrigues. 2022. "Prevalence and Antifungal Susceptibility Profile of Oral Candida spp. Isolates from a Hospital in Slovakia" Medicina 58, no. 5: 576. https://doi.org/10.3390/medicina58050576
APA StyleČernáková, L., Líšková, A., Lengyelová, L., & Rodrigues, C. F. (2022). Prevalence and Antifungal Susceptibility Profile of Oral Candida spp. Isolates from a Hospital in Slovakia. Medicina, 58(5), 576. https://doi.org/10.3390/medicina58050576