
Efficacy of Topical Intervention for Recurrent Aphthous Stomatitis: A Network Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Statement
2.2. Data Sources and Search Strategy
2.3. Selection Criteria
- (1)
- Clinical or histopathological examination confirms a diagnosis of recurrent aphthous ulcers, with ulcer-like lesions visible anywhere on the oral mucosa.
- (2)
- Simple ulcerative lesions of any undetermined cause such as psychological, nutritional and immunological factors, rather than oral manifestations of systemic diseases such as leukoaraiosis, diabetes mellitus, etc., or specific ulcerative lesions due to trauma, radiotherapy, etc.
- (3)
- The population enrolled received only local interventions or placebo during the trial and did not receive any other treatment that might alter the RAS prior to or during the trial, such as receiving systemic steroids or immunosuppressants.
- (4)
- For studies in patients with multiple oral mucosal diseases, we extracted only RAS data. If this was not possible, we excluded the study.
2.4. Outcomes
2.5. Data Collection and Risk of Bias Assessment
2.6. Data Synthesis and Statistical Analysis
3. Results
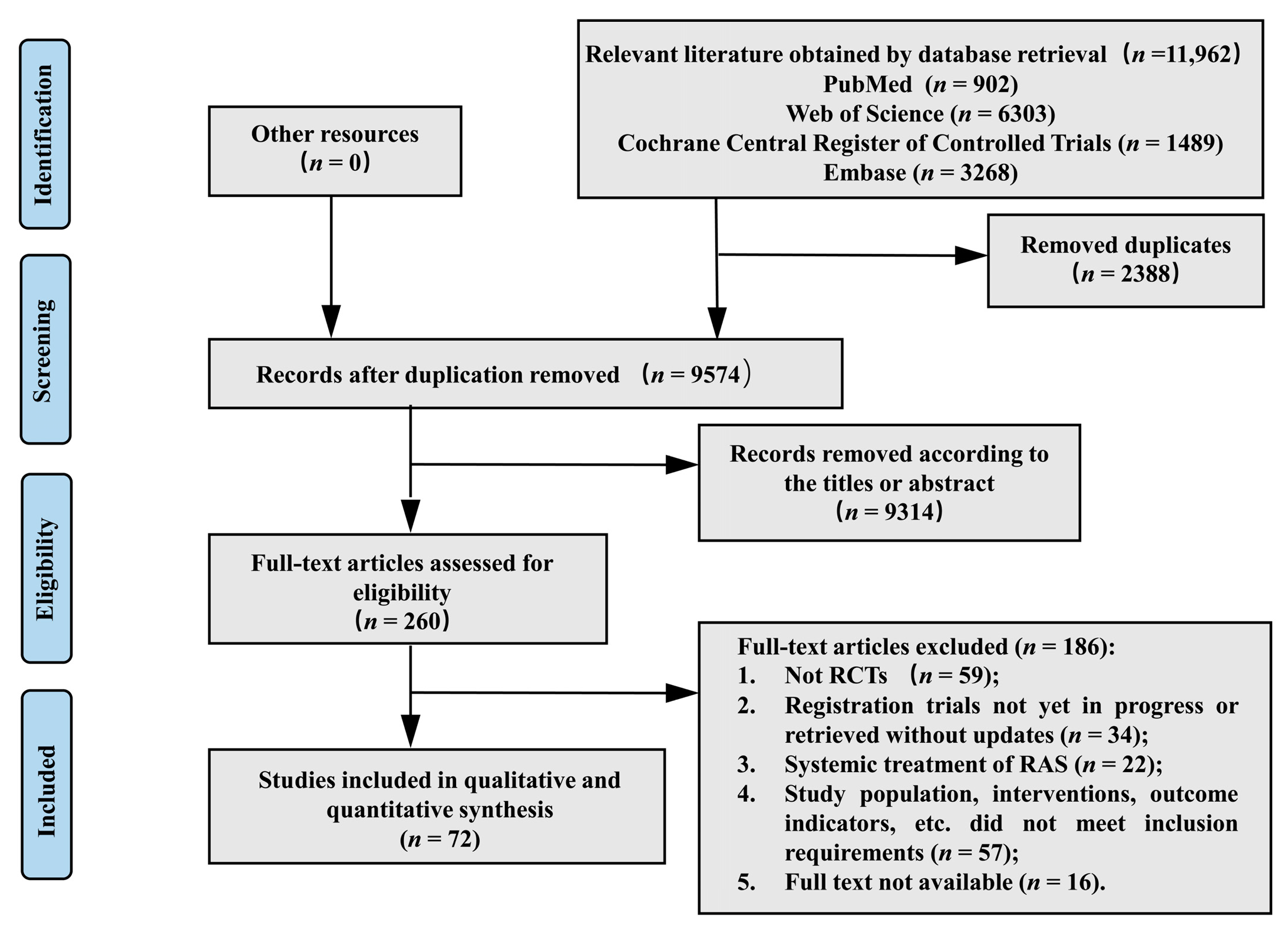
3.1. Study Selection
3.2. Characteristics and Quality of Studies
3.3. Pairwise Meta-Analysis
3.4. Network Meta-Analysis
3.4.1. Healing Effect
3.4.2. Size-Reducing Effect
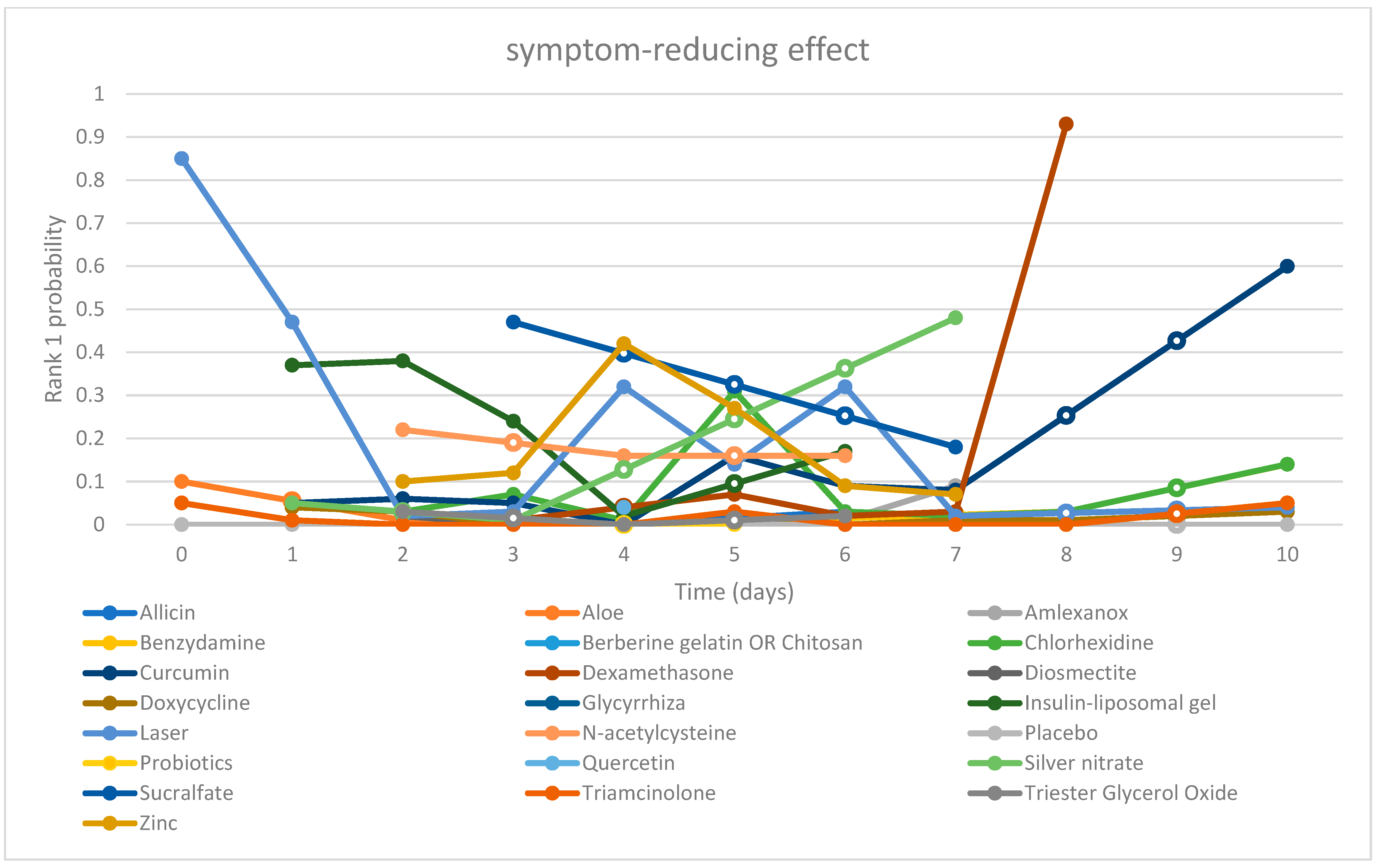
3.4.3. Symptom-Reducing Effect
3.4.4. Adverse Effect
3.5. Other Outcome Indicators
3.5.1. Hematologic Values
3.5.2. Relapse
3.6. Consistency and Sensitivity Analysis
3.7. Our Perspective
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Kaur, R.; Behl, A.B.; Punia, R.S.; Nirav, K.; Singh, K.B.; Kaur, S. Assessment of Prevalence of Recurrent Aphthous Stomatitis in the North Indian Population: A Cross-Sectional Study. J. Pharm. Bioallied Sci. 2021, 13, S363–S366. [Google Scholar] [CrossRef] [PubMed]
- Darjani, A.; Joukar, F.; Naghipour, M.; Asgharnezhad, M.; Mansour-Ghanaei, F. Lifetime prevalence of recurrent aphthous stomatitis and its related factors in Northern Iranian population: The PERSIAN Guilan Cohort Study. Clin. Oral. Investig. 2021, 25, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Xu, K.; Zhou, C.; Huang, F.; Duan, N.; Wang, Y.; Zheng, L.; Wang, X.; Wang, W. Relationship between dietary factors and recurrent aphthous stomatitis in China: A cross-sectional study. J. Int. Med. Res. 2021, 49, 675888644. [Google Scholar] [CrossRef]
- Hariyani, N.; Bramantoro, T.; Nair, R.; Singh, A.; Sengupta, K. Depression symptoms and recurrent aphthous stomatitis—Evidence from a population-based study in Indonesia. Oral Dis. 2020, 26, 948–954. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, S.; Silva, M.; Medeiros, A.; Oliveira, P.T.; Gurgel, B.; Silveira, É. Recurrent aphthous ulceration: An epidemiological study of etiological factors, treatment and differential diagnosis. An. Bras. Dermatol. 2018, 93, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Gasmi, B.A.; Noor, S.; Menzel, A.; Gasmi, A. Oral Aphthous: Pathophysiology, Clinical Aspects and Medical Treatment. Arch. Razi Inst. 2021, 76, 1155–1163. [Google Scholar]
- Bankvall, M.; Sjöberg, F.; Gale, G.; Wold, A.; Jontell, M.; Östman, S. The oral microbiota of patients with recurrent aphthous stomatitis. J. Oral Microbiol. 2014, 6, 25739. [Google Scholar] [CrossRef] [Green Version]
- Kazanowska-Dygdała, M.; Duś, I.; Radwan-Oczko, M. The presence of Helicobacter pylori in oral cavities of patients with leukoplakia and oral lichen planus. J. Appl. Oral Sci. 2016, 24, 18–23. [Google Scholar] [CrossRef] [Green Version]
- Irani, S. New Insights into Oral Cancer-Risk Factors and Prevention: A Review of Literature. Int. J. Prev. Med. 2020, 11, 202. [Google Scholar] [CrossRef]
- Slebioda, Z.; Szponar, E.; Kowalska, A. Etiopathogenesis of recurrent aphthous stomatitis and the role of immunologic aspects: Literature review. Arch. Immunol. Ther. Exp. 2014, 62, 205–215. [Google Scholar] [CrossRef] [Green Version]
- Ludovichetti, F.S.; Signoriello, A.G.; Girotto, L.; Del Dot, L.; Piovan, S.; Mazzoleni, S. Oro-dental lesions in paediatric patients with coeliac disease: An observational retrospective clinical study. Rev. Esp. Enferm. Dig. 2022; Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Scully, C.; Porter, S. Oral mucosal disease: Recurrent aphthous stomatitis. Br. J. Oral Maxillofac. Surg. 2008, 46, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Saikaly, S.K.; Saikaly, T.S.; Saikaly, L.E. Recurrent aphthous ulceration: A review of potential causes and novel treatments. J. Dermatolog. Treat. 2018, 29, 542–552. [Google Scholar] [CrossRef] [PubMed]
- Ahluwalia, A. Topical glucocorticoids and the skin—Mechanisms of action: An update. Mediat. Inflamm. 1998, 7, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Golub, L.M.; Ramamurthy, N.S.; Mcnamara, T.F.; Greenwald, R.A.; Rifkin, B.R. Tetracyclines inhibit connective tissue breakdown: New therapeutic implications for an old family of drugs. Crit. Rev. Oral Biol. Med. 1991, 2, 297–321. [Google Scholar] [CrossRef]
- Baccaglini, L.; Lalla, R.V.; Bruce, A.J.; Sartori-Valinotti, J.C.; Latortue, M.C.; Carrozzo, M.; Rogers, R.R. Urban legends: Recurrent aphthous stomatitis. Oral Dis. 2011, 17, 755–770. [Google Scholar] [CrossRef] [Green Version]
- Yuan, H.; Qiu, J.; Zhang, T.; Wu, X.; Zhou, J.; Park, S. Quantitative changes of Veillonella, Streptococcus, and Neisseria in the oral cavity of patients with recurrent aphthous stomatitis: A systematic review and meta-analysis. Arch. Oral Biol. 2021, 129, 105198. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, J.P.; Da Silva, M.A.; Almeida, A.P.; Lombardi, J.I.; Matos, A.P. Laser therapy in the tissue repair process: A literature review. Photomed. Laser Surg. 2010, 28, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Arikan, O.K.; Birol, A.; Tuncez, F.; Erkek, E.; Koc, C. A prospective randomized controlled trial to determine if cryotherapy can reduce the pain of patients with minor form of recurrent aphthous stomatitis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, E1–E5. [Google Scholar] [CrossRef]
- Soylu Özler, G. Silver nitrate cauterization: A treatment option for aphthous stomatitis. J. Cranio-Maxillofac. Surg. 2014, 42, e281–e283. [Google Scholar] [CrossRef] [PubMed]
- Al-Maweri, S.A.; Halboub, E.; Al-Sharani, H.M.; Shamala, A.; Al-Kamel, A.; Al-Wesabi, M.; Albashari, A.; Al-Sharani, A.; Abdulrab, S. Association between serum zinc levels and recurrent aphthous stomatitis: A meta-analysis with trial sequential analysis. Clin. Oral Investig. 2021, 25, 407–415. [Google Scholar] [CrossRef]
- Manifar, S.; Obwaller, A.; Gharehgozloo, A.; Boorboor Shirazi Kordi, H.R.; Akhondzadeh, S. Curcumin gel in the treatment of minor aphthous ulcer: A randomized, placebo-controlled trial. J. Med. Plants 2012, 11, 40–45. [Google Scholar]
- Martin, M.D.; Sherman, J.; Van Der Ven, P.; Burgess, J. A controlled trial of a dissolving oral patch concerning glycyrrhiza (licorice) herbal extract for the treatment of aphthous ulcers. Gen. Dent. 2008, 56, 206–210. [Google Scholar] [PubMed]
- El-Haddad, S.A.; Asiri, F.Y.; Al-Qahtani, H.H.; Al-Ghmlas, A.S. Efficacy of honey in comparison to topical corticosteroid for treatment of recurrent minor aphthous ulceration: A randomized, blind, controlled, parallel, double-center clinical trial. Quintessence Int. 2014, 45, 691–701. [Google Scholar]
- Pandya, M.; Kalappanavar, A.N.; Annigeri, R.G.; Rao, D.S. Relative Efficacy of Quercetin Compared with Benzydamine Hydrochloride in Minor Aphthae: A Prospective, Parallel, Double Blind, Active Control, Preliminary Study. Int. J. Dent. 2017, 2017, 7034390. [Google Scholar] [CrossRef] [Green Version]
- Rahmani, F.; Moghadamnia, A.A.; Kazemi, S.; Shirzad, A.; Motallebnejad, M. Effect of 0.5% Chitosan mouthwash on recurrent aphthous stomatitis: A randomized double-blind crossover clinical trial. Electron. Physician 2018, 10, 6912–6919. [Google Scholar] [CrossRef]
- Babaee, N.; Zabihi, E.; Mohseni, S.; Moghadamnia, A.A. Evaluation of the therapeutic effects of Aloe vera gel on minor recurrent aphthous stomatitis. Dent. Res. J. 2012, 9, 381–385. [Google Scholar]
- Jiang, X.W.; Zhang, Y.; Zhu, Y.L.; Zhang, H.; Lu, K.; Li, F.F.; Peng, H.Y. Effects of berberine gelatin on recurrent aphthous stomatitis: A randomized, placebo-controlled, double-blind trial in a Chinese cohort. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.W.; Zhang, Y.; Zhang, H.; Lu, K.; Yang, S.K.; Sun, G.L. Double-blind, randomized, controlled clinical trial of the effects of diosmectite and basic fibroblast growth factor paste on the treatment of minor recurrent aphthous stomatitis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 570–575. [Google Scholar] [CrossRef]
- Jiang, X.W.; Zhang, Y.; Song, G.D.; Li, F.F.; Peng, H.Y.; Yang, S.K.; Sun, G.L. Clinical evaluation of allicin oral adhesive tablets in the treatment of recurrent aphthous ulceration. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 113, 500–504. [Google Scholar] [CrossRef] [PubMed]
- Al-Omiri, M.K.; Karasneh, J.; Alhijawi, M.M.; Zwiri, A.M.; Scully, C.; Lynch, E. Recurrent aphthous stomatitis (RAS): A preliminary within-subject study of quality of life, oral health impacts and personality profiles. J. Oral Pathol. Med. 2015, 44, 278–283. [Google Scholar] [CrossRef]
- Cheng, B.; Zeng, X.; Liu, S.; Zou, J.; Wang, Y. The efficacy of probiotics in management of recurrent aphthous stomatitis: A systematic review and meta-analysis. Sci. Rep. 2020, 10, 21181. [Google Scholar] [CrossRef]
- Al-Maweri, S.A.; Halboub, E.; Ashraf, S.; Alqutaibi, A.Y.; Qaid, N.M.; Yahya, K.; Alhajj, M.N. Single application of topical doxycycline in management of recurrent aphthous stomatitis: A systematic review and meta-analysis of the available evidence. BMC Oral Health 2020, 20, 231. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.L. Limited Evidence Suggests That Patients with Recurrent Aphthous Stomatitis May Benefit from Using Sodium Lauryl Sulfate-free Dentifrices. J. Evid. Based Dent. Pract. 2019, 19, 101349. [Google Scholar] [CrossRef]
- Watt, J.; Tricco, A.C.; Straus, S.; Veroniki, A.A.; Naglie, G.; Drucker, A.M. Research Techniques Made Simple: Network Meta-Analysis. J. Invest. Dermatol. 2019, 139, 4–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [Green Version]
- van Valkenhoef, G.; Tervonen, T.; Zwinkels, T.; de Brock, B.; Hillege, H. ADDIS: A decision support system for evidence-based medicine. Decis. Support Syst. 2013, 55, 459–475. [Google Scholar] [CrossRef] [Green Version]
- Huo, X.; Han, N.; Liu, L. Effect of different treatments on recurrent aphthous stomatitis: Laser versus medication. Lasers Med. Sci. 2021, 36, 1095–1100. [Google Scholar] [CrossRef]
- Shi, Y.; Wei, K.; Lu, J.; Wei, J.; Hu, X.; Chen, T. A Clinic Trial Evaluating the Effects of Aloe Vera Fermentation Gel on Recurrent Aphthous Stomatitis. Can. J. Infect. Dis. Med. Microbiol. 2020, 2020, 8867548. [Google Scholar] [CrossRef]
- Ibrahim, S.A.; Elkot, R.A.; Soliman, H.E. Lactic acid 5% mouth wash vs Kenalog in Orabase 0.1% for treatment and prophylaxis of recurrent aphthous ulcer. J. Cosmet. Dermatol. 2020, 19, 964–969. [Google Scholar] [CrossRef]
- Owlia, M.B.; Mirzadeh, M.; Mehrpoor, G. Penicillin in oral aphthosis, new insight for an old drug: A randomized, double-blind, controlled clinical trial. J. Res. Med. Sci. 2020, 25, 95. [Google Scholar]
- Raman, P.; Pitty, R.; Krithika, C.L.; Anand, S.P.N.; Subramani, G.P. Topical Curcumin and Triamcinolone Acetonide in Recurrent Minor Aphthous Ulcers: A Pilot Trial. J. Contemp. Dent. Pract. 2020, 21, 884–890. [Google Scholar]
- Halboub, E.; Alkadasi, B.; Alakhali, M.; Alkhairat, A.; Mdabesh, H.; Alkahsah, S.; Abdulrab, S. N-acetylcysteine versus chlorhexidine in treatment of aphthous ulcers: A preliminary clinical trial. J. Dermatol. Treat. 2019, 32, 649–653. [Google Scholar] [CrossRef] [PubMed]
- El-Wakeel, N.M.; Dawoud, M.H.S. Topical insulin-liposomal formulation in management of recurrent aphthous ulcers: A randomized placebo-controlled trial. J. Investig. Clin. Dent. 2019, 10, e12437. [Google Scholar] [CrossRef]
- Tavangar, A.; Aslani, A.; Nikbakht, N. Comparative Study of Punica granatum Gel and Triadent Oral Paste Effect on Recurrent Aphthous Stomatitis, a Double Blind Clinical Trial. J. Dent. 2019, 20, 184–189. [Google Scholar]
- Zeini, J.N.; Ghapanchi, J.; Pourshahidi, S.; Zahed, M.; Ebrahimi, H. Clinical Evaluation of High and Low-Level Laser Treatment (CO2vsInGaAlP Diode Laser) for Recurrent Aphthous Stomatitis. J. Dent. 2017, 18, 17–23. [Google Scholar]
- Rodríguez-Archilla, A.; Raissouni, T. Randomized clinical trial of the effectiveness of complementary therapies for recurrent aphthous stomatitis. Med. Clin. 2017, 149, 55–60. [Google Scholar] [CrossRef]
- Raeesi, V.; Arbabi-Kalati, F.; Akbari, N.; Hamishekar, H. Comparison effectiveness of the bioadhesive paste containing licorice 5% with bioadhesive paste without drug in the management of recurrent aphthous stomatitis. Acta Med. Mediterr. 2015, 31, 1331–1335. [Google Scholar]
- Aggarwal, H.; Pal Singh, M.; Nahar, P.; Mathur, H.; Sowmya, G.V. Efficacy of low-level laser therapy in treatment of recurrent aphthous ulcers—A sham controlled, split mouth follow up study. J. Clin. Diagn. Res. 2014, 8, 218–221. [Google Scholar] [CrossRef]
- Deshmukh, R.A.; Bagewadi, A.S. Comparison of effectiveness of curcumin with triamcinolone acetonide in the gel form in treatment of minor recurrent aphthous stomatitis: A randomized clinical trial. Int. J. Pharm. Investig. 2014, 4, 138–141. [Google Scholar] [CrossRef] [Green Version]
- Soylu, Ö.G.; Okuyucu, Ş.; Akoğlu, E. The Efficacy of Sucralfate and Chlorhexidine as an Oral Rinse in Patients with Recurrent Aphthous Stomatitis. Adv. Med. 2014, 2014, 986203. [Google Scholar]
- Prasad, R.S.; Pai, A. Assessment of immediate pain relief with laser treatment in recurrent aphthous stomatitis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 189–193. [Google Scholar] [CrossRef] [PubMed]
- Vijayabala, G.S.; Kalappanavar, A.N.; Annigeri, R.G.; Sudarshan, R.; Shettar, S.S. Single application of topical doxycycline hyclate in the management of recurrent aphthous stomatitis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 116, 440–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zand, N.; Fateh, M.; Ataie-Fashtami, L.; Djavid, G.E.; Fatemi, S.M.; Shirkavand, A. Promoting wound healing in minor recurrent aphthous stomatitis by non-thermal, non-ablative CO2 laser therapy: A pilot study. Photomed. Laser Surg. 2012, 30, 719–723. [Google Scholar] [CrossRef] [PubMed]
- Moghadamnia, A.A.; Motallebnejad, M.; Khanian, M. The efficacy of the bioadhesive patches containing licorice extract in the management of recurrent aphthous stomatitis. Phytother. Res. 2009, 23, 246–250. [Google Scholar] [CrossRef]
- Garnick, J.J.; Singh, B.; Winkley, G. Effectiveness of a medicament containing silicon dioxide, aloe, and allantoin on aphthous stomatitis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 86, 550–556. [Google Scholar] [CrossRef]
- Taylor, L.J.; Walker, D.M.; Bagg, J. A clinical trial of prostaglandin E2 in recurrent aphthous ulceration. Brit. Dent. J. 1993, 175, 125–129. [Google Scholar] [CrossRef]
- Hunter, L.; Addy, M. Chlorhexidine gluconate mouthwash in the management of minor aphthous ulceration. A double-blind, placebo-controlled cross-over trial. Brit. Dent. J. 1987, 162, 106–110. [Google Scholar] [CrossRef] [PubMed]
- Addy, M.; Carpenter, R.; Roberts, W.R. Management of recurrent aphthous ulceration. A trial of chlorhexidine gluconate gel. Br. Dent. J. 1976, 141, 118–120. [Google Scholar] [CrossRef]
- Addy, M.; Tapper-Jones, L.; Seal, M. Trial of astringent and antibacterial mouthwashes in the management of recurrent aphthous ulceration. Br. Dent. J. 1974, 136, 452–455. [Google Scholar] [CrossRef]
- Aggour, R.L.; Mahmoud, S.H.; Abdelwhab, A. Evaluation of the effect of probiotic lozenges in the treatment of recurrent aphthous stomatitis: A randomized, controlled clinical trial. Clin. Oral Invest. 2021, 25, 2151–2158. [Google Scholar] [CrossRef]
- Kavita, K.; Singh, R.; Singh, R.; Gonuguntla, S.; Luke, A.M.; Jois, H.S. Assessment of efficacy of 5% topical amlexanox and 0.1% topical triamcinolone acetonide in management of recurrent aphthous stomatitis. J. Pharm. Bioallied Sci. 2020, 12, S444–S447. [Google Scholar]
- Shao, Y.; Zhou, H. Clinical evaluation of an oral mucoadhesive film containing chitosan for the treatment of recurrent aphthous stomatitis: A randomized, double-blind study. J. Dermatol. Treat. 2020, 31, 739–743. [Google Scholar] [CrossRef]
- Ghorbani, A.; Akbari, J.; Boorboor, M.; Nekoukar, Z.; Eslami, G. Evaluation of zinc sulfate mucoadhesive formulation on recurrent aphthous stomatitis: A randomized double-blind, placebo-controlled clinical trial. BMC Oral Health 2020, 20, 212. [Google Scholar] [CrossRef] [PubMed]
- Kia, S.J.; Mansourian, A.; Basirat, M.; Akhavan, M.; Mohtasham-Amiri, Z.; Moosavi, M.S. New concentration of curcumin orabase in recurrent aphthous stomatitis: A randomized, controlled clinical trial. J. Herb. Med. 2020, 22, 100336. [Google Scholar] [CrossRef]
- Bardellini, E.; Veneri, F.; Amadori, F.; Conti, G.; Majorana, A. Photobiomodulation therapy for the management of recurrent aphthous sto-matitis in children: Clinical effectiveness and parental satisfaction. Med. Oral Patol. Oral 2020, 25, e549–e553. [Google Scholar] [CrossRef] [PubMed]
- Seyyedi, S.A.; Olyaee, P.; Fekrazad, R.; Partovi, S.; Baghizadeh, F.M. The Effect of Carbon Dioxide Laser on Aphthous stomatitis Treatment: A Double-Blind Randomized Clinical Trial. J. Lasers Med. Sci. 2020, 11, S67–S72. [Google Scholar] [CrossRef] [PubMed]
- Nirmala, M.; Smitha, S.G.; Kamath, G.J. A Study to Assess the Efficacy of Local Application of Oral Probiotic in Treating Recurrent Aphthous Ulcer and Oral Candidiasis. Indian J. Otolaryngol. Head Neck Surg. 2019, 71, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Soliman, H.A.; Mostafaa, D. Clinical evaluation of 660 nm diode laser therapy on the pain, size and functional disorders of recurrent aphthous stomatitis. Open Access Maced. J. Med. Sci. 2019, 7, 1516–1522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, R.; Pallagatti, S.; Aggarwal, A.; Sheikh, S.; Singh, R.; Gupta, D. A Randomized, Double-Blind, Placebo-Controlled Trial on Clinical Efficacy of Topical Agents in Reducing Pain and Frequency of Recurrent Aphthous Ulcers. Open Dent. J. 2018, 12, 700–713. [Google Scholar] [CrossRef] [PubMed]
- Ofluoglu, D.; Ergun, S.; Warnakulasuriya, S.; Namdar-Pekiner, F.; Tanyeri, H. An evaluation of the efficacy of a topical gel with Triester Glycerol Oxide (TGO) in the treatment of minor recurrent aphthous stomatitis in a turkish cohort: A randomized, double-blind, placebo-controlled clinical trial. Med. Oral Patol. Oral Cir. Bucal 2017, 22, e159–e166. [Google Scholar] [CrossRef] [Green Version]
- Nasry, S.A.; El Shenawy, H.M.; Mostafa, D.; Ammar, N.M. Different modalities for treatment of recurrent aphthous stomatitis. A randomized clinical trial. J. Clin. Exp. Dent. 2016, 8, e517–e522. [Google Scholar] [CrossRef]
- Abbasi, F.; Raoof, M.; Khatami, R.; Shadman, N.; Borjian-Boroojeni, F.; Nazari, F. Effectiveness of Amlexanox and Adcortyl for the treatment of recurrent aphthous ulcers. J. Clin. Exp. Dent. 2016, 8, e368–e372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andishe Tadbir, A.; Pourshahidi, S.; Ebrahimi, H.; Hajipour, Z.; Memarzade, M.R.; Shirazian, S. The effect of Matricaria chamomilla (chamomile) extract in Orabase on minor aphthous stomatitis, a randomized clinical trial. J. Herb. Med. 2015, 5, 71–76. [Google Scholar] [CrossRef]
- Mansour, G.; Ouda, S.; Shaker, A.; Abdallah, H.M. Clinical efficacy of new aloe vera- and myrrh-based oral mucoadhesive gels in the management of minor recurrent aphthous stomatitis: A randomized, double-blind, vehicle-controlled study. J. Oral Pathol. Med. 2014, 43, 405–409. [Google Scholar] [CrossRef]
- Bhat, S.; Sujatha, D. A clinical evaluation of 5% amlexanox oral paste in the treatment of minor recurrent aphthous ulcers and comparison with the placebo paste: A randomized, vehicle controlled, parallel, single center clinical trial. Indian J. Dent. Res. Off. Publ. Indian Soc. Dent. Res. 2013, 24, 593–598. [Google Scholar] [CrossRef]
- Bhalang, K.; Thunyakitpisal, P.; Rungsirisatean, N. Acemannan, a polysaccharide extracted from aloe vera, is effective in the treatment of oral aphthous ulceration. J. Altern. Complem. Med. 2013, 19, 429–434. [Google Scholar] [CrossRef]
- Halim, D.S.; Khalik, N.I.B.A.; Taib, H.; Pohchi, A.; Hassan, A.; Alam, M.K. Novel material in the treatment of minor oral recurrent aphthous stomatitis. Int. Med. J. 2013, 20, 392–394. [Google Scholar]
- Sattayut, S.; Trivibulwanich, J.; Pipithirunkarn, N.; Danvirutai, N. A clinical efficacy of using CO2 laser irradiating to transparent gel on aphthous stomatitis patients. Laser Ther. 2013, 22, 283–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.; Zhou, Z.; Liu, G.; Wang, Q.; Chen, J.; Wang, L.; Zhou, Y.; Dong, G.; Xu, X.; Wang, Y.; et al. Efficacy and safety of dexamethasone ointment on recurrent aphthous ulceration. Am. J. Med. 2012, 125, 292–301. [Google Scholar] [CrossRef]
- Galal, M.; Nasry, S.A.; Mostafa, D.M.; Ammar, N.M. Therapeutic Efficacy of Herbal Formulations for Recurrent Aphthous Ulcer. Correlation with Salivary Epidermal Growth Factor. Life Sci. J. 2012, 9, 2398–2406. [Google Scholar]
- Meng, W.; Dong, Y.; Liu, J.; Wang, Z.; Zhong, X.; Chen, R.; Zhou, H.; Lin, M.; Jiang, L.; Gao, F.; et al. A clinical evaluation of amlexanox oral adhesive pellicles in the treatment of recurrent aphthous stomatitis and comparison with amlexanox oral tablets: A randomized, placebo controlled, blinded, multicenter clinical trial. Trials 2009, 10, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.; Zeng, X.; Chen, Q.; Cai, Y.; Chen, F.; Wang, Y.; Zhou, H.; Lin, M.; Shi, J.; Wang, Z.; et al. An evaluation on the efficacy and safety of amlexanox oral adhesive tablets in the treatment of recurrent minor aphthous ulceration in a Chinese cohort: A randomized, double-blind, vehicle-controlled, unparallel multicenter clinical trial. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 102, 475–481. [Google Scholar] [CrossRef]
- Khandwala, A.; Van Inwegen, R.G.; Alfano, M.C. 5% amlexanox oral paste, a new treatment for recurrent minor aphthous ulcers: I. Clinical demonstration of acceleration of healing and resolution of pain. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1997, 83, 222–230. [Google Scholar] [CrossRef]
- Pedersen, A.M.L.; Bukkehave, K.H.; Bennett, E.P.; Twetman, S. Effect of Lozenges Containing Lactobacillus reuteri on the Severity of Recurrent Aphthous Ulcers: A Pilot Study. Probiotics Antimicrob. Proteins 2020, 12, 819–823. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, H.G.; Albaba, M.R.; Caygur, A.; Cengiz, E.; Boke-Karacaoglu, F.; Tumer, H. Treatment of recurrent aphthous stomatitis with Er,Cr:YSGG laser irradiation: A randomized controlled split mouth clinical study. J. Photochem. Photobiol. B Biol. 2017, 170, 1–5. [Google Scholar] [CrossRef]
- Tezel, A.; Kara, C.; Balkaya, V.; Orbak, R. An evaluation of different treatments for recurrent aphthous stomatitis and patient perceptions: Nd:YAG laser versus medication. Photomed. Laser Surg. 2009, 27, 101–106. [Google Scholar] [CrossRef]
- Skulason, S.; Holbrook, W.P.; Kristmundsdottir, T. Clinical assessment of the effect of a matrix metalloproteinase inhibitor on aphthous ulcers. Acta Odontol. Scand. 2009, 67, 25–29. [Google Scholar] [CrossRef]
- Zand, N.; Ataie-Fashtami, L.; Djavid, G.E.; Fateh, M.; Alinaghizadeh, M.R.; Fatemi, S.M.; Arbabi-Kalati, F. Relieving pain in minor aphthous stomatitis by a single session of non-thermal carbon dioxide laser irradiation. Laser. Med. Sci. 2009, 24, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Ylikontiola, L.; Sorsa, T.; Häyrinen-Immonen, R.; Salo, T. Doxymycine-cyanoacrylate treatment of recurrent aphthous ulcers. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1997, 83, 329–333. [Google Scholar] [CrossRef]
- Miles, D.A.; Bricker, S.L.; Razmus, T.F.; Potter, R.H. Triamcinolone acetonide versus chlorhexidine for treatment of recurrent stomatitis. Oral Surg. Oral Med. Oral Pathol. 1993, 75, 397–402. [Google Scholar] [CrossRef]
- Albrektson, M. Recurrent aphthous stomatitis and pain management with low-level laser therapy: A randomized controlled trial. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 590–594. [Google Scholar] [CrossRef]
- Trinchieri, V.; Di Carlo, S.; Bossu’, M.; Polimeni, A. Use of lozenges containing Lactobacillus brevis CD2 in recurrent aphthous stomatitis: A double-blind placebo-controlled trial. Ulcers 2011, 2011, 439425. [Google Scholar] [CrossRef] [Green Version]
- Gorsky, M.; Epstein, J.; Raviv, A.; Yaniv, R.; Truelove, E. Topical minocycline for managing symptoms of recurrent aphthous stomatitis. Spec. Care Dent. 2008, 28, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, M.; Rubio, J.A.; Sanchez, R. Effectiveness of two oral pastes for the treatment of recurrent aphthous stomatitis. Oral Dis. 2007, 13, 490–494. [Google Scholar] [CrossRef] [PubMed]
- Greer, R.O., Jr.; Lindenmuth, J.E.; Juarez, T.; Khandwala, A.; Kaugars, G.E. A double-blind study of topically applied 5% amlexanox in the treatment of aphthous ulcers. J. Oral Maxillofac. Surg. 1993, 51, 243–249. [Google Scholar] [CrossRef]
- Matthews, R.W.; Scully, C.M.; Levers, B.G.H.; Hislop, W.S. Clinical evaluation of benzydamine, chlorhexidine, and placebo mouthwashes in the management of recurrent aphthous stomatitis. Oral Surg. Oral Med. Oral Pathol. 1987, 63, 189–191. [Google Scholar] [CrossRef]
- Browne, R.M.; Fox, E.C.; Anderson, R.J. Topical triamcinolone acetonide in recurrent aphthous stomatitis. A clinical trial. Lancet 1968, 1, 565–567. [Google Scholar] [CrossRef]
- Diegelmann, R.F.; Evans, M.C. Wound healing: An overview of acute, fibrotic and delayed healing. Front. Biosci. 2004, 9, 283–289. [Google Scholar] [CrossRef]
- Manfredini, M.; Guida, S.; Giovani, M.; Lippolis, N.; Spinas, E.; Farnetani, F.; Dattola, A.; Di Matteo, E.; Pellacani, G.; Giannetti, L. Recurrent Aphthous Stomatitis: Treatment and Management. Dermatol. Pract. Concept. 2021, 11, e2021099. [Google Scholar] [CrossRef]
- Daugėlaitė, G.; Užkuraitytė, K.; Jagelavičienė, E.; Filipauskas, A. Prevention and Treatment of Chemotherapy and Radiotherapy Induced Oral Mucositis. Medicina 2019, 55, 25. [Google Scholar] [CrossRef] [Green Version]
- Gondivkar, D.; Gadbail, D.; Sarode, D.; Gondivkar, D.; Patil, S.; Gaikwad, D.; Dinh-Toi, C.; Yuwanati, D.M. Treatment outcomes of laser therapy in oral submucous fibrosis—A systematic review. J. Oral Biol. Craniofac. Res. 2020, 10, 253–258. [Google Scholar] [CrossRef]
- García-Pola, M.J.; González-Álvarez, L.; Garcia-Martin, J.M. Treatment of oral lichen planus. Systematic review and therapeutic guide. Med. Clin. 2017, 149, 351–362. [Google Scholar] [CrossRef]
- Lodi, G.; Franchini, R.; Warnakulasuriya, S.; Varoni, E.M.; Sardella, A.; Kerr, A.R.; Carrassi, A.; Macdonald, L.C.; Worthington, H.V. Interventions for treating oral leukoplakia to prevent oral cancer. Cochrane Database Syst. Rev. 2016, 7, D1829. [Google Scholar] [CrossRef]
- Matos, A.L.; Silva, P.U.; Paranhos, L.R.; Santana, I.T.; Matos, F.R. Efficacy of the laser at low intensity on primary burning oral syndrome: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2021, 26, e216–e225. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, A.L.; Lins, L.; Cattony, A.C.; Falcão, A.F. Laser therapy in the control of oral mucositis: A meta-analysis. Rev. Assoc. Med. Bras. 2013, 59, 467–474. [Google Scholar] [CrossRef] [Green Version]
- Lino, M.D.; Carvalho, F.B.; Oliveira, L.R.; Magalhães, E.B.; Pinheiro, A.L.; Ramalho, L.M. Laser phototherapy as a treatment for radiotherapy-induced oral mucositis. Braz. Dent. J. 2011, 22, 162–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silveira, P.C.; Streck, E.L.; Pinho, R.A. Evaluation of mitochondrial respiratory chain activity in wound healing by low-level laser therapy. J. Photochem. Photobiol. B 2007, 86, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Karu, T.I.; Kolyakov, S.F. Exact action spectra for cellular responses relevant to phototherapy. Photomed. Laser Surg. 2005, 23, 355–361. [Google Scholar] [CrossRef] [Green Version]
- Medrado, A.R.; Pugliese, L.S.; Reis, S.R.; Andrade, Z.A. Influence of low level laser therapy on wound healing and its biological action upon myofibroblasts. Lasers Surg. Med. 2003, 32, 239–244. [Google Scholar] [CrossRef]
- Suter, V.; Sjölund, S.; Bornstein, M.M. Effect of laser on pain relief and wound healing of recurrent aphthous stomatitis: A systematic review. Lasers Med. Sci. 2017, 32, 953–963. [Google Scholar] [CrossRef]
- Han, M.; Fang, H.; Li, Q.L.; Cao, Y.; Xia, R.; Zhang, Z.H. Effectiveness of Laser Therapy in the Management of Recurrent Aphthous Stomatitis: A Systematic Review. Scientifica 2016, 2016, 9062430. [Google Scholar] [CrossRef]
- Najeeb, S.; Khurshid, Z.; Zohaib, S.; Najeeb, B.; Qasim, S.B.; Zafar, M.S. Management of recurrent aphthous ulcers using low-level lasers: A systematic review. Medicina 2016, 52, 263–268. [Google Scholar] [CrossRef]
- Pavlić, V.; Vujić-Aleksić, V.; Aoki, A.; Nežić, L. Treatment of recurrent aphthous stomatitis by laser therapy: A systematic review of the literature. Vojnosanit. Pregl. 2015, 72, 722–728. [Google Scholar] [CrossRef]
- Bizzini, B.; Pizzo, G.; Scapagnini, G.; Nuzzo, D.; Vasto, S. Probiotics and oral health. Curr. Pharm. Des. 2012, 18, 5522–5531. [Google Scholar] [CrossRef]
- Bandara, H.; Panduwawala, C.P.; Samaranayake, L.P. Biodiversity of the human oral mycobiome in health and disease. Oral Dis. 2019, 25, 363–371. [Google Scholar] [CrossRef]
- Nyvad, B.; Crielaard, W.; Mira, A.; Takahashi, N.; Beighton, D. Dental caries from a molecular microbiological perspective. Caries Res. 2013, 47, 89–102. [Google Scholar] [CrossRef] [PubMed]
- Dye, B.A. Global periodontal disease epidemiology. Periodontol. 2000 2012, 58, 10–25. [Google Scholar] [CrossRef]
- Telles, D.R.; Karki, N.; Marshall, M.W. Oral Fungal Infections: Diagnosis and Management. Dent. Clin. North Am. 2017, 61, 319–349. [Google Scholar] [CrossRef]
- Gruner, D.; Paris, S.; Schwendicke, F. Probiotics for managing caries and periodontitis: Systematic review and meta-analysis. J. Dent. 2016, 48, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Laleman, I.; Teughels, W. Probiotics in the dental practice: A review. Quintessence Int. 2015, 46, 255–264. [Google Scholar] [PubMed]
- Laleman, I.; Detailleur, V.; Slot, D.E.; Slomka, V.; Quirynen, M.; Teughels, W. Probiotics reduce mutans streptococci counts in humans: A systematic review and meta-analysis. Clin. Oral Investig. 2014, 18, 1539–1552. [Google Scholar] [CrossRef] [Green Version]
- Laleman, I.; Yilmaz, E.; Ozcelik, O.; Haytac, C.; Pauwels, M.; Herrero, E.R.; Slomka, V.; Quirynen, M.; Alkaya, B.; Teughels, W. The effect of a streptococci containing probiotic in periodontal therapy: A randomized controlled trial. J. Clin. Periodontol. 2015, 42, 1032–1041. [Google Scholar] [CrossRef]
- Shimauchi, H.; Mayanagi, G.; Nakaya, S.; Minamibuchi, M.; Ito, Y.; Yamaki, K.; Hirata, H. Improvement of periodontal condition by probiotics with Lactobacillus salivarius WB21: A randomized, double-blind, placebo-controlled study. J. Clin. Periodontol. 2008, 35, 897–905. [Google Scholar] [CrossRef] [PubMed]
- Wylleman, A.; Vuylsteke, F.; Dekeyser, C.; Teughels, W.; Quirynen, M.; Laleman, I. Alternative therapies in controlling oral malodour: A systematic review. J. Breath Res. 2021, 15, 026009. [Google Scholar] [CrossRef]
- Georgiou, A.C.; Laine, M.L.; Deng, D.M.; Brandt, B.W.; van Loveren, C.; Dereka, X. Efficacy of probiotics: Clinical and microbial parameters of halitosis. J. Breath Res. 2018, 12, 46010. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Olivos, R.; Muñoz, M.; Núñez, E.; Camargo-Ayala, P.A.; Garcia-Huidobro, J.; Pereira, A.; Nachtigall, F.M.; Santos, L.S.; Rivera, C. Salivary proteome of aphthous stomatitis reveals the participation of vitamin metabolism, nutrients, and bacteria. Sci. Rep. 2021, 11, 15646. [Google Scholar] [CrossRef]
- Koybasi, S.; Parlak, A.H.; Serin, E.; Yilmaz, F.; Serin, D. Recurrent aphthous stomatitis: Investigation of possible etiologic factors. Am. J. Otolaryngol. 2006, 27, 229–232. [Google Scholar] [CrossRef]
- Cappello, F.; Rappa, F.; Canepa, F.; Carini, F.; Mazzola, M.; Tomasello, G.; Bonaventura, G.; Giuliana, G.; Leone, A.; Saguto, D.; et al. Probiotics Can Cure Oral Aphthous-Like Ulcers in Inflammatory Bowel Disease Patients: A Review of the Literature and a Working Hypothesis. Int. J. Mol. Sci. 2019, 20, 5026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piwat, S.; Sophatha, B.; Teanpaisan, R. An assessment of adhesion, aggregation and surface charges of Lactobacillus strains derived from the human oral cavity. Lett. Appl. Microbiol. 2015, 61, 98–105. [Google Scholar] [CrossRef]
- Takahashi, N. Oral Microbiome Metabolism: From “Who Are They?” to “What Are They Doing?”. J. Dent. Res. 2015, 94, 1628–1637. [Google Scholar] [CrossRef]
- Twetman, S. Are we ready for caries prevention through bacteriotherapy? Braz. Oral Res. 2012, 26 (Suppl. S1), 64–70. [Google Scholar] [CrossRef] [Green Version]
- Maldonado, G.C.; Cazorla, S.I.; Lemme, D.J.; Vélez, E.; Perdigón, G. Beneficial Effects of Probiotic Consumption on the Immune System. Ann. Nutr. Metab. 2019, 74, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Haukioja, A. Probiotics and oral health. Eur. J. Dent. 2010, 4, 348–355. [Google Scholar] [CrossRef] [Green Version]
- Stamatova, I.; Meurman, J.H. Probiotics: Health benefits in the mouth. Am. J. Dent. 2009, 22, 329–338. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healing Effect | |||
| Comparison | Honey vs. placebo | Insulin-liposomal gel vs. placebo | Laser vs. placebo |
| Relative effect estimate | −3.55 (−5.90, −1.13) | −3.90 (−7.53, −0.23) | −3.08 (−4.81, −1.19) |
| Size-reducing Effect | |||
| Comparison | Amlexanox vs. placebo | Glycyrrhiza vs. placebo | Triamcinolone vs. placebo |
| Relative effect estimate | 35.29 (15.53, 54.72) | 29.07 (3.58, 54.49) | 25.83 (7.91, 45.48) |
| Symptom-Reducing Effect | |||
| Comparison | Amlexanox vs. placebo | Laser vs. placebo | Triamcinolone vs. placebo |
| Relative effect estimate | 23.26 (4.15, 42.15) | 32.21 (16.39, 48.08) | 28.45 (10.36, 46.76) |
| Adverse Effect | |||
| Comparison | Triamcinolone vs. amlexanox | Triamcinolone vs. chitosan | Triamcinolone vs. dexamethasone |
| Relative effect estimate | 0.00 (0.00, 0.00) | 0.00 (0.00, 0.08) | 0.00 (0.00, 0.00) |
| Comparison | Dexamethasone vs. penicillin | Placebo vs. doxycycline | Triamcinolone vs. doxycycline |
| Relative effect estimate | 0.00 (0.00, 0.10) | 0.00 (0.00, 0.06) | 0.00 (0.00, 0.00) |
| Comparison | Triamcinolone vs. penicillin | Triamcinolone vs. placebo | Placebo vs. penicillin |
| Relative effect estimate | 0.00 (0.00, 0.00) | 0.00 (0.00, 0.00) | 0.00 (0.00, 0.14) |
| Comparison | Dexamethasone vs. doxycycline | ||
| Relative effect estimate | 0.00 (0.00, 0.06) | ||
| Healing Effect | Size-Reducing Effect | Symptom-Reducing Effect | Adverse Effect | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Rank | Treatment | p-Core | Rank | Treatment | p-Core | Rank | Treatment | p-Core | Rank | Treatment | p-Core |
| 18 | Insulin-liposomal gel | 0.24 | 1 | Quercetin | 0.27 | 1 | Insulin-liposomal gel | 0.24 | 22 | Triamcinolone | 0.15 |
| 17 | Honey | 0.15 | 2 | Dexamethasone | 0.14 | 2 | N-acetylcysteine or sucralfate | 0.12 | 21 | Berberine gelatin | 0.08 |
| 16 | Laser | 0.11 | 3 | Amlexanox | 0.13 | 3 | Curcumin | 0.08 | 20 | Glycyrrhiza or laser | 0.07 |
| 15 | Penicillin | 0.09 | 4 | Glycyrrhiza or laser | 0.08 | 4 | Laser | 0.09 | 19 | Aloe or honey or probiotics | 0.06 |
| 14 | Aloe | 0.06 | 5 | Curcumin | 0.08 | 5 | Chlorhexidine | 0.07 | 18 | Curcumin, silver nitrate, triester glycerol oxide or zinc | 0.06 |
| Interventions | Total | Hematologic Values |
|---|---|---|
| Dexamethasone | 114 | Blood level < 0.502 ng/mL |
| Aloe | 60 | No significant differences between the blood test values before and after 7 days of application |
| Allicin | 48 | None of the hematologic values on day 6 were considered clinically abnormal |
| Amlexanox | 108 | None of the hematologic values were considered clinically abnormal |
| Interventions | Total | Relapse | Statistical Significance |
|---|---|---|---|
| Probiotics | Adult group: 30 Children group: 30 | Adult group: (Outbreak frequency/6 months) Probiotics: 3.33 (0.64) Placebo: 3.65 (0.32) Children group: (Outbreak frequency/6 months) Probiotics: 2.65 (0.54) Placebo: 3.65 (0.62) | Adult group: No change in outbreak frequency was reported within the 6 months next to treatment (p > 0.05). Children group: A statistically significant decrease in outbreak frequency was reported for probiotics group within the 6 months next to treatment. The change was significantly different from placebo group (p < 0.05). |
| Chlorhexidine | 38 | Total ulcer numbers (6 weeks): Chlorhexidine: 7.54 ± 6.52 Placebo: 8.32 ± 5.52 Interval between ulcers (6 weeks): Chlorhexidine: 7.26 ± 8.61 Placebo:3.86 ± 2.05 | Total ulcer numbers: NA Interval between ulcers: Chlorhexidine significantly increased the interval between successive ulcers (p < 0.05). For the total group, the increase was from 3.86 days with the placebo to 7.26 days with chlorhexidine. |
| Benzydamine | 18 | Number of new ulcers (3 months) Benzydamine: 7 (2–33) Placebo: 8 (2–20) | p = 0.07 |
| Chlorhexidine | 18 | Number of new ulcers (3 months) Chlorhexidine: 6.5 (3–20) Placebo: 8 (2–20) | p = 0.27 |
| Triamcinolone | 26 | No. of new ulcers (8 months) Placebo: 7.81 Triamcinolone acetonide in orabase: 7.00 Triamcinolone acetonide in watery base: 6.42 | Although there was a slight reduction in the number of new ulcers during treatment with both steroid preparations, this was not statistically significant. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, H.; Tan, L.; Fu, G.; Chen, L.; Tan, H. Efficacy of Topical Intervention for Recurrent Aphthous Stomatitis: A Network Meta-Analysis. Medicina 2022, 58, 771. https://doi.org/10.3390/medicina58060771
Liu H, Tan L, Fu G, Chen L, Tan H. Efficacy of Topical Intervention for Recurrent Aphthous Stomatitis: A Network Meta-Analysis. Medicina. 2022; 58(6):771. https://doi.org/10.3390/medicina58060771
Chicago/Turabian StyleLiu, Hao, Lei Tan, Gege Fu, Ling Chen, and Hua Tan. 2022. "Efficacy of Topical Intervention for Recurrent Aphthous Stomatitis: A Network Meta-Analysis" Medicina 58, no. 6: 771. https://doi.org/10.3390/medicina58060771
APA StyleLiu, H., Tan, L., Fu, G., Chen, L., & Tan, H. (2022). Efficacy of Topical Intervention for Recurrent Aphthous Stomatitis: A Network Meta-Analysis. Medicina, 58(6), 771. https://doi.org/10.3390/medicina58060771