
The Added Value of Point-Light Display Observation in Total Knee Arthroplasty Rehabilitation Program: A Prospective Randomized Controlled Pilot Study

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
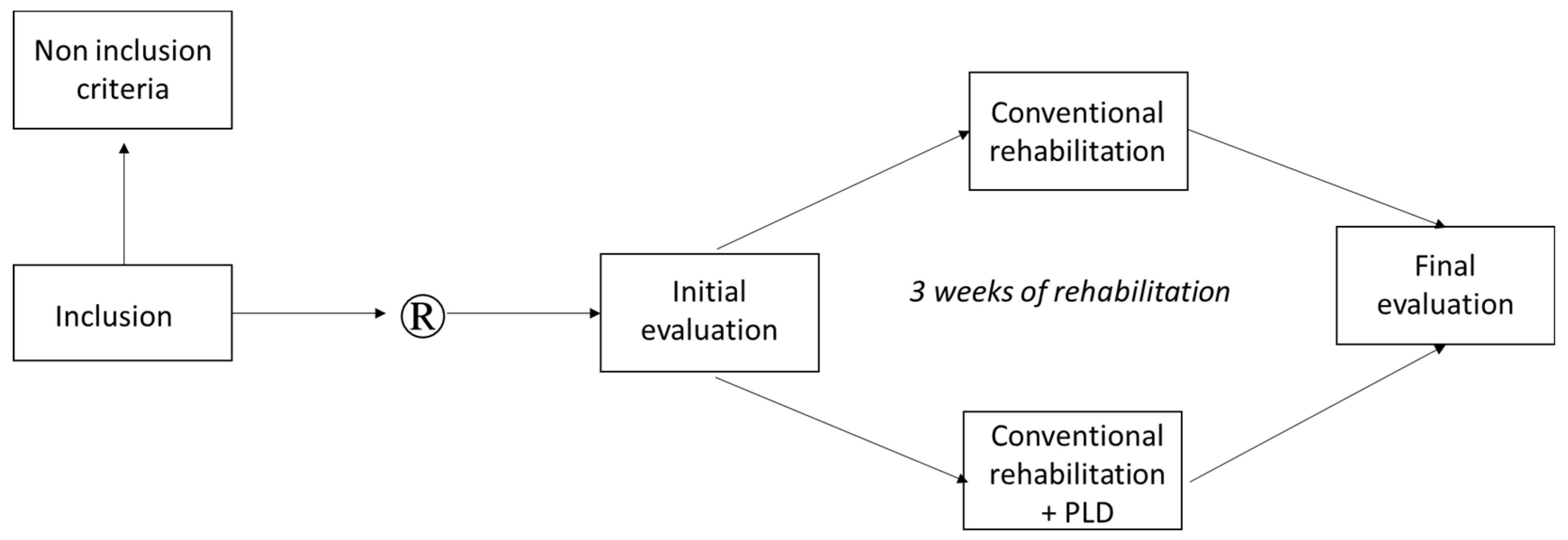
2.1. Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Procedure
2.4. Primary Outcome
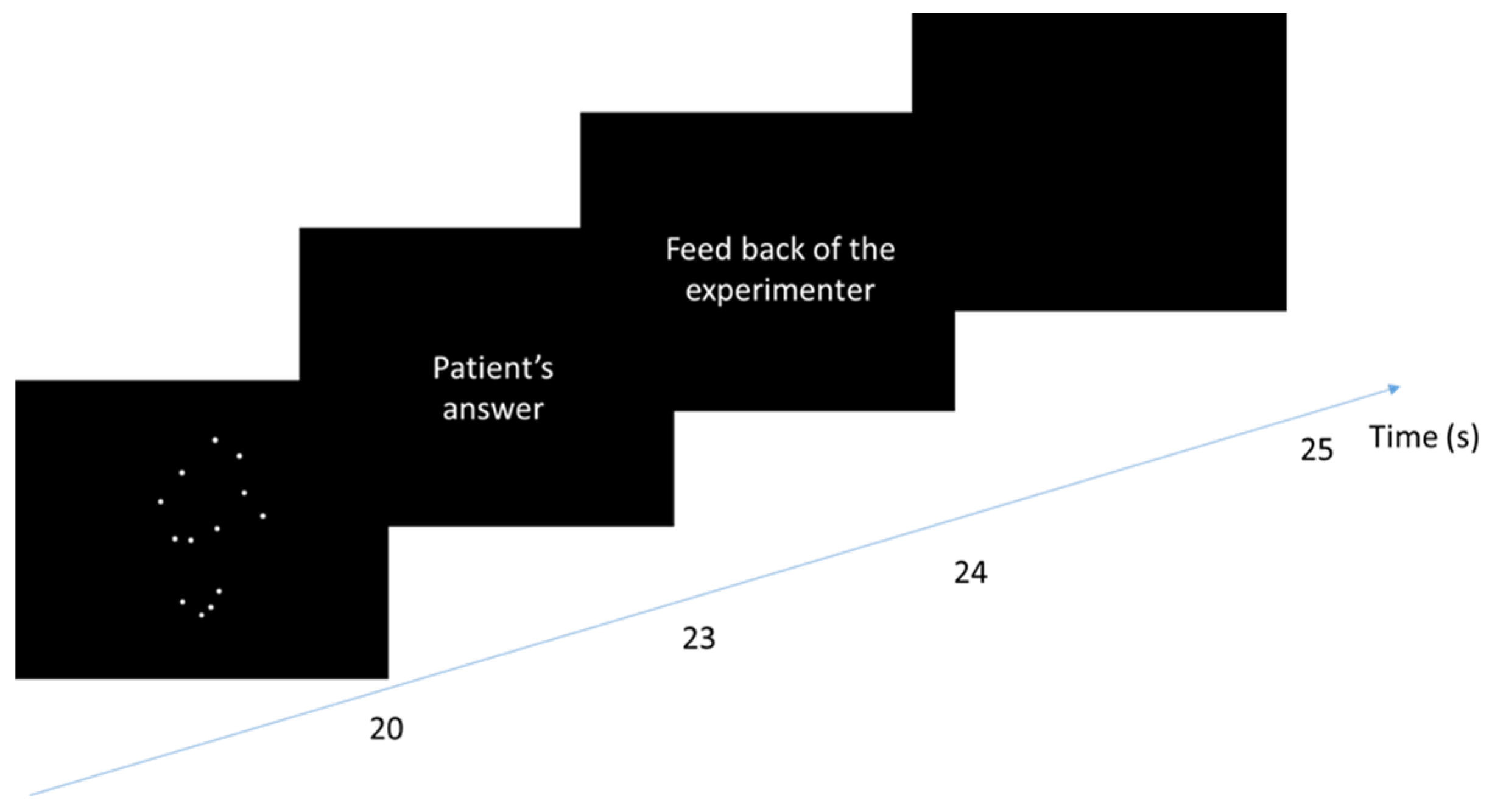
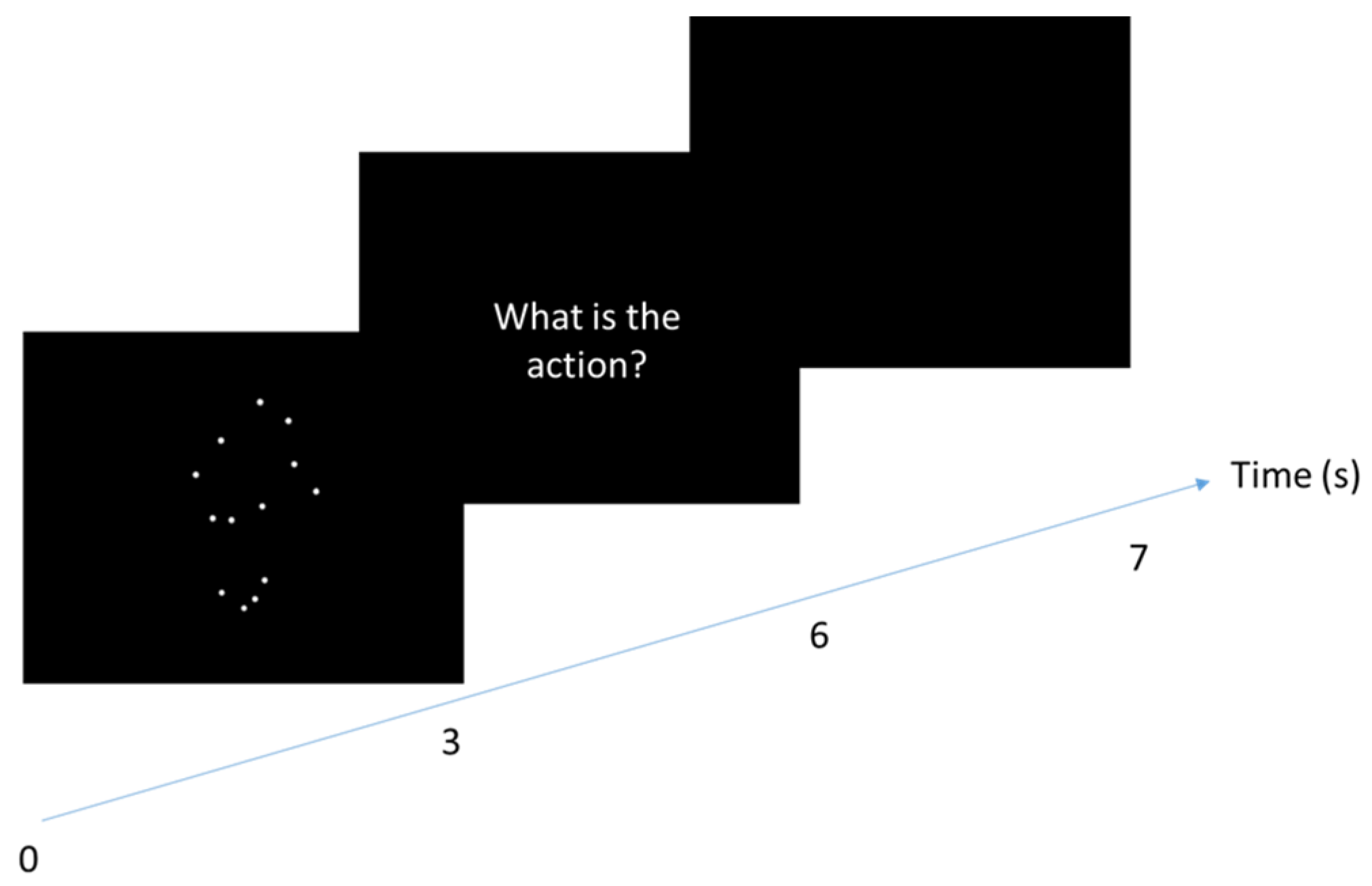
2.5. Secondary Outcomes
2.6. Statistical Analysis
3. Results
3.1. Participants
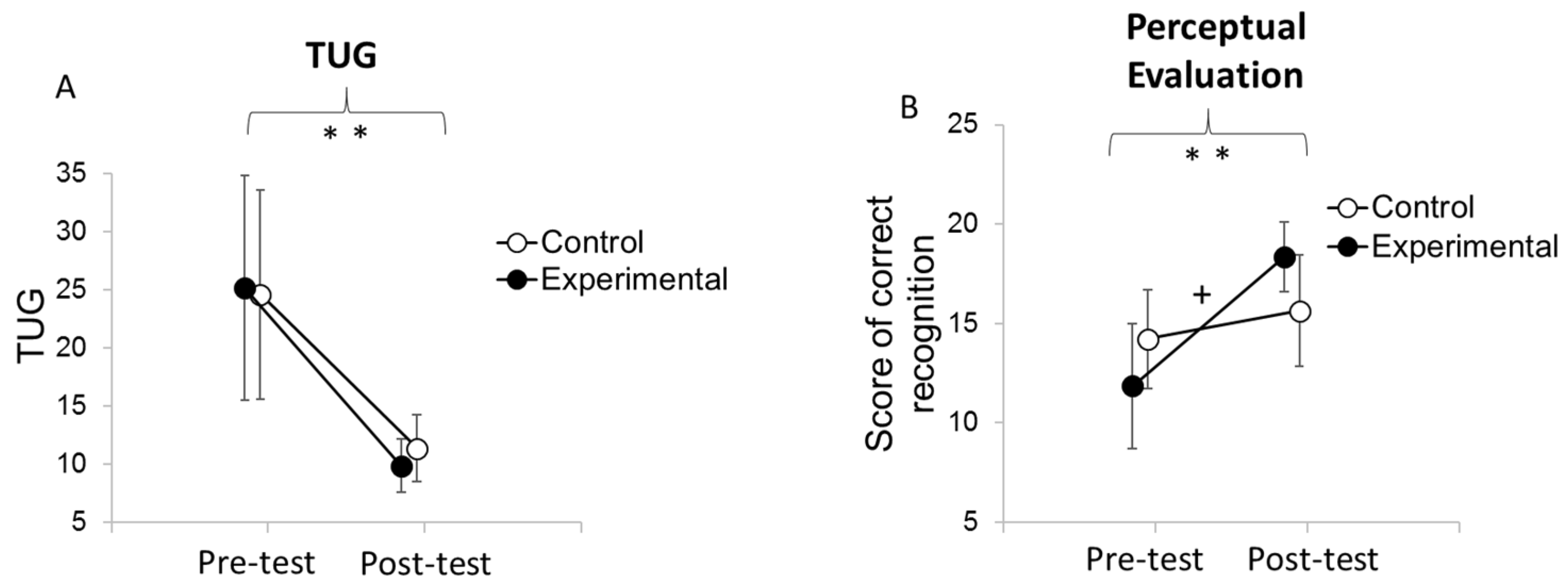
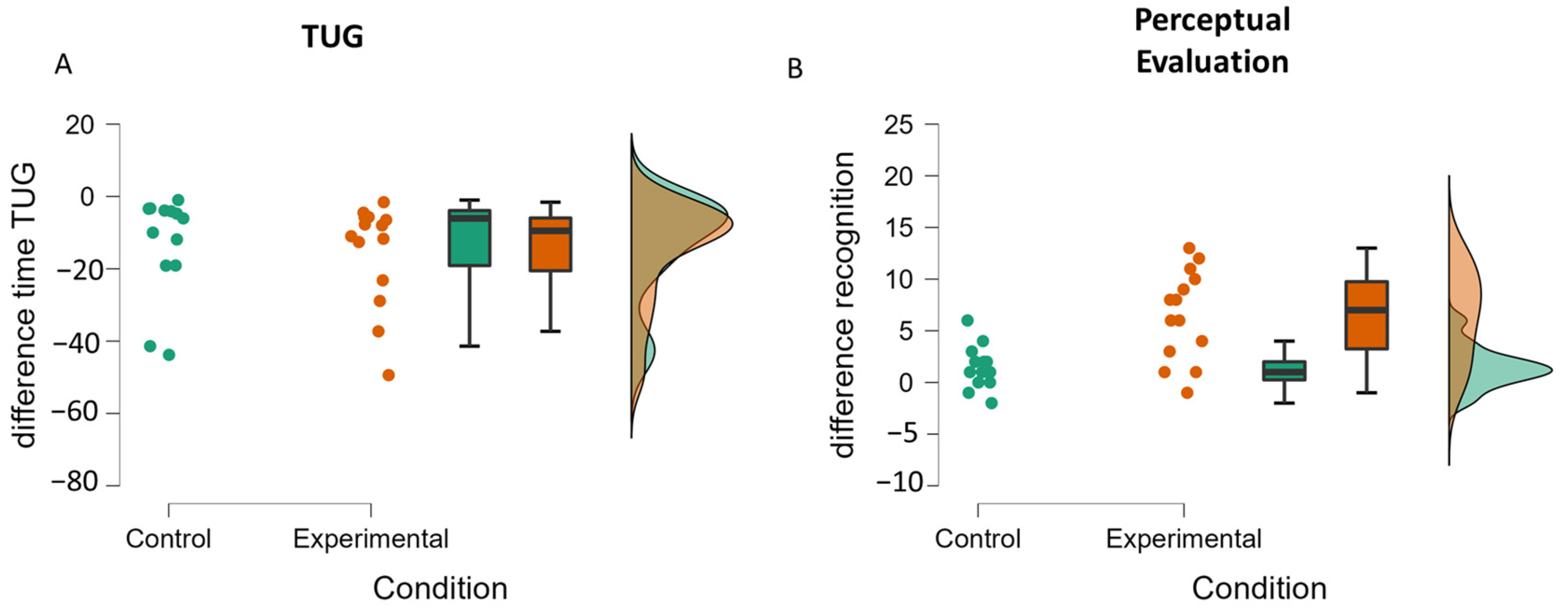
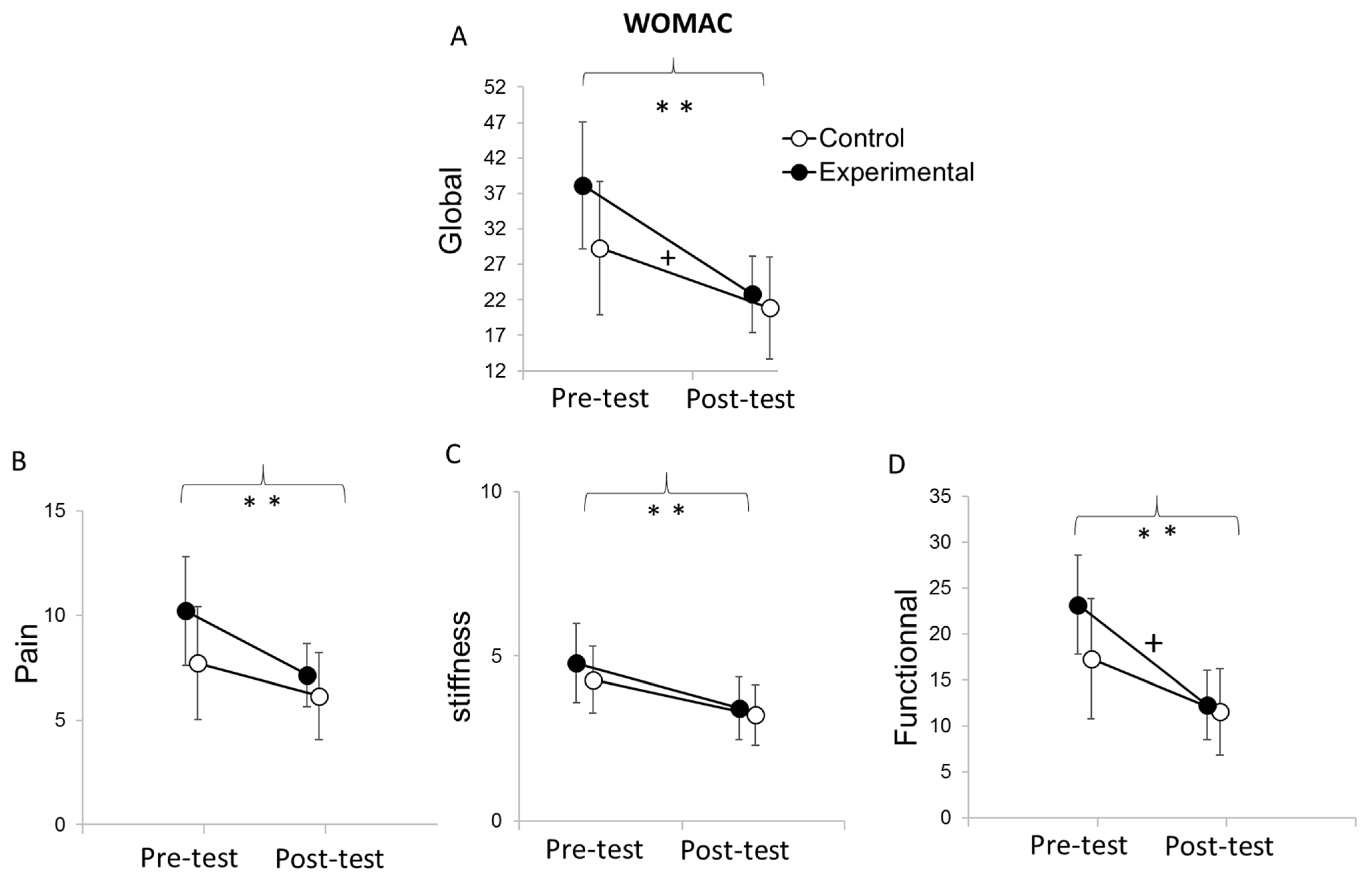
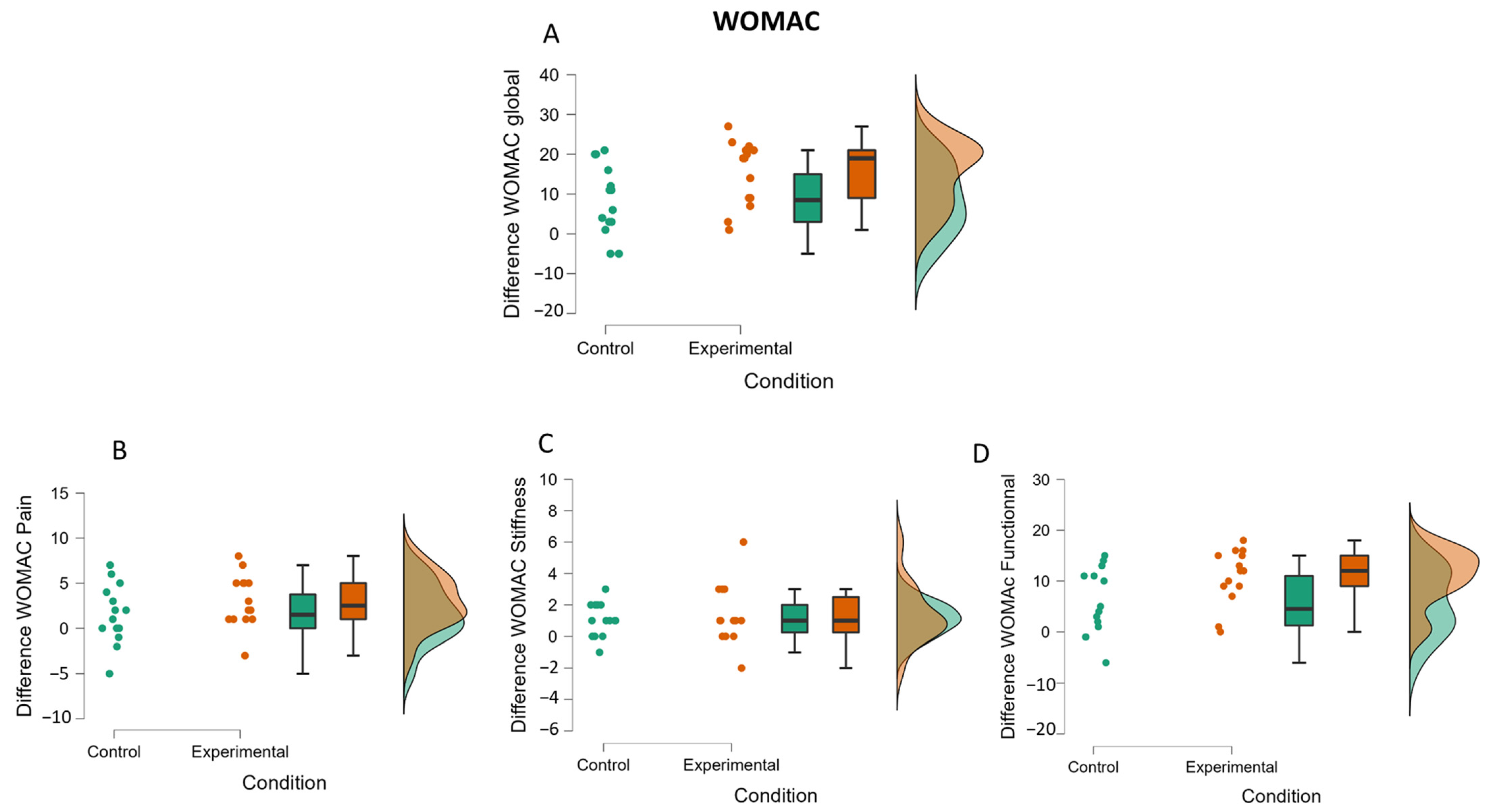
3.2. Functional Mobility
3.3. Motor Outcome
3.4. Perceptual Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. PLD Used in the Experiment
| PLD | Type of Movement | Used in the Recognition’s Task | Used in the Observation’s Task |
| Acquiese | Upper-limb | * | |
| Applaud | Upper-limb | * | |
| Catch | Upper-limb | * | |
| Climb ladder | Lower-limb | * | * |
| Climb steps | Lower-limb | * | * |
| Crouch | Lower-limb | * | * |
| Decline | Upper-limb | * | |
| French military salute | Upper-limb | * | |
| Get off ladder | Lower-limb | * | * |
| Kick | Lower-limb | * | * |
| Move back | Lower-limb | * | * |
| Pedal | Lower-limb | * | * |
| Push somebody | Upper-limb | * | |
| Push up | Upper-limb | * | |
| Run | Lower-limb | * | * |
| Salute | Upper-limb | * | |
| Say Hello | Upper-limb | * | |
| Scratch | Upper-limb | * | |
| Sit down | Lower-limb | * | * |
| Stand up | Lower-limb | * | * |
| Sweep | Upper-limb | * | |
| Throw | Upper-limb | * | |
| Turn | Lower-limb | * | * |
| Walk | Lower-limb | * | * |
| * means that the PLD was used in the task. | |||
Appendix B. Position of the Markers for the Motion Capture of Each Action Used

Appendix C. The WOMAC Questionnaire
| None (0) | Slight (1) | Moderate (2) | Severe (3) | Extreme (4) | ||
| Rate your pain when? | Walking | |||||
| Climbing stairs | ||||||
| Sleeping at night | ||||||
| Resting | ||||||
| Standing | ||||||
| Rate your stiffness in the | Morning | |||||
| Evening | ||||||
| Rate your difficulty when | Descending stairs | |||||
| Ascending stairs | ||||||
| Rising from sitting | ||||||
| Standing | ||||||
| Bending to floor | ||||||
| Walking on even floor | ||||||
| Getting in/out a car | ||||||
| Going Shopping | ||||||
| Putting on socks | ||||||
| Rising from bed | ||||||
| Taking off socks | ||||||
| Lying in bed | ||||||
| Getting in/out of bath | ||||||
| Sitting | ||||||
| Getting on/off toilet | ||||||
| Doing light domestic duties | ||||||
| Doing heavy domestic duties | ||||||
| Items in italic have not be assessed because they are not adapted for hospitalized patients. | ||||||
References
- Kurtz, S.M.; Ong, K.L.; Lau, E.; Widmer, M.; Maravic, M.; Gómez-Barrena, E.; de Pina, M.d.F.; Manno, V.; Torre, M.; Walter, W.L.; et al. International Survey of Primary and Revision Total Knee Replacement. Int. Orthop. 2011, 35, 1783–1789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delgado-González, A.; Morales-Viaji, J.J.; Arteaga-Hernández, J.G.; Larrosa-Arranz, Á.; Criado-Albillos, G.; Martin-Rodríguez, A.D.P.; Jahouh, M.; González-Santos, J.; Mendieta Díaz, L.; Collazo Riobo, C.; et al. To Resurface or Not to Resurface the Patella in Total Knee Arthroplasty, That Is the Question: A Meta-Analysis of Randomized Controlled Trials. Medicina 2022, 58, 227. [Google Scholar] [CrossRef] [PubMed]
- Billot, M.; Calvani, R.; Urtamo, A.; Sánchez-Sánchez, J.L.; Ciccolari-Micaldi, C.; Chang, M.; Roller-Wirnsberger, R.; Wirnsberger, G.; Sinclair, A.; Vaquero-Pinto, N.; et al. Preserving Mobility in Older Adults with Physical Frailty and Sarcopenia: Opportunities, Challenges, and Recommendations for Physical Activity Interventions. Clin. Interv. Aging 2020, 15, 1675–1690. [Google Scholar] [CrossRef] [PubMed]
- Middleton, A.; Fritz, S.L.; Lusardi, M. Walking Speed: The Functional Vital Sign. J. Aging Phys. Act. 2015, 23, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Dapretto, M.; Davies, M.S.; Pfeifer, J.H.; Scott, A.A.; Sigman, M.; Bookheimer, S.Y.; Iacoboni, M. Understanding Emotions in Others: Mirror Neuron Dysfunction in Children with Autism Spectrum Disorders. Nat. Neurosci. 2006, 9, 28–30. [Google Scholar] [CrossRef] [Green Version]
- Grézès, J.; Decety, J. Functional Anatomy of Execution, Mental Simulation, Observation, and Verb Generation of Actions: A Meta-Analysis. Hum. Brain Mapp. 2001, 12, 1–19. [Google Scholar] [CrossRef]
- Bang, D.-H.; Shin, W.-S.; Kim, S.-Y.; Choi, J.-D. The Effects of Action Observational Training on Walking Ability in Chronic Stroke Patients: A Double-Blind Randomized Controlled Trial. Clin. Rehabil. 2013, 27, 1118–1125. [Google Scholar] [CrossRef]
- Ertelt, D.; Small, S.; Solodkin, A.; Dettmers, C.; McNamara, A.; Binkofski, F.; Buccino, G. Action Observation Has a Positive Impact on Rehabilitation of Motor Deficits after Stroke. Neuroimage 2007, 36 (Suppl. S2), T164–T173. [Google Scholar] [CrossRef]
- Buccino, G.; Arisi, D.; Gough, P.; Aprile, D.; Ferri, C.; Serotti, L.; Tiberti, A.; Fazzi, E. Improving Upper Limb Motor Functions through Action Observation Treatment: A Pilot Study in Children with Cerebral Palsy. Dev. Med. Child Neurol. 2012, 54, 822–828. [Google Scholar] [CrossRef]
- Buccino, G.; Molinaro, A.; Ambrosi, C.; Arisi, D.; Mascaro, L.; Pinardi, C.; Rossi, A.; Gasparotti, R.; Fazzi, E.; Galli, J. Action Observation Treatment Improves Upper Limb Motor Functions in Children with Cerebral Palsy: A Combined Clinical and Brain Imaging Study. Neural Plast. 2018, 2018, 4843985. [Google Scholar] [CrossRef]
- Buccino, G.; Gatti, R.; Giusti, M.C.; Negrotti, A.; Rossi, A.; Calzetti, S.; Cappa, S.F. Action Observation Treatment Improves Autonomy in Daily Activities in Parkinson’s Disease Patients: Results from a Pilot Study. Mov. Disord. Off. J. Mov. Disord. Soc. 2011, 26, 1963–1964. [Google Scholar] [CrossRef] [PubMed]
- Ryan, D.; Fullen, B.; Rio, E.; Segurado, R.; Stokes, D.; O’Sullivan, C. Effect of Action Observation Therapy in the Rehabilitation of Neurologic and Musculoskeletal Conditions: A Systematic Review. Arch. Rehabil. Res. Clin. Transl. 2021, 3, 100106. [Google Scholar] [CrossRef] [PubMed]
- Bellelli, G.; Buccino, G.; Bernardini, B.; Padovani, A.; Trabucchi, M. Action Observation Treatment Improves Recovery of Postsurgical Orthopedic Patients: Evidence for a Top-down Effect? Arch. Phys. Med. Rehabil. 2010, 91, 1489–1494. [Google Scholar] [CrossRef] [PubMed]
- Park, S.D.; Song, H.S.; Kim, J.Y. The Effect of Action Observation Training on Knee Joint Function and Gait Ability in Total Knee Replacement Patients. J. Exerc. Rehabil. 2014, 10, 168–171. [Google Scholar] [CrossRef] [PubMed]
- Villafañe, J.H.; Isgrò, M.; Borsatti, M.; Berjano, P.; Pirali, C.; Negrini, S. Effects of Action Observation Treatment in Recovery after Total Knee Replacement: A Prospective Clinical Trial. Clin. Rehabil. 2017, 31, 361–368. [Google Scholar] [CrossRef]
- De Marco, D.; Scalona, E.; Bazzini, M.C.; Nuara, A.; Taglione, E.; Lopomo, N.F.; Rizzolatti, G.; Fabbri-Destro, M.; Avanzini, P. Observation of Others’ Actions during Limb Immobilization Prevents the Subsequent Decay of Motor Performance. Proc. Natl. Acad. Sci. USA 2021, 118, e2025979118. [Google Scholar] [CrossRef]
- Johansson, G. Visual Perception of Biological Motion and a Model for Its Analysis. Percept. Psychophys. 1973, 14, 201–211. [Google Scholar] [CrossRef]
- Beauprez, S.A.; Bidet-Ildei, C. The Kinematics, Not the Orientation, of an Action Influences Language Processing. J. Exp. Psychol. Hum. Percept. Perform. 2018, 44, 1712. [Google Scholar] [CrossRef]
- Johansson, G. Visual Motion Perception. Sci. Am. 1975, 232, 76–88. [Google Scholar] [CrossRef]
- Martel, L.; Bidet-Ildei, C.; Coello, Y. Anticipating the Terminal Position of an Observed Action: Effect of Kinematic, Structural, and Identity Information. Vis. Cogn. 2011, 19, 785–798. [Google Scholar] [CrossRef]
- Pavlova, M.; Sokolov, A.N.; Bidet-Ildei, C. Sex Differences in the Neuromagnetic Cortical Response to Biological Motion. Cereb. Cortex 2015, 25, 3468–3474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollick, F.E.; Lestou, V.; Ryu, J.; Cho, S.B. Estimating the Efficiency of Recognizing Gender and Affect from Biological Motion. Vis. Res. 2002, 42, 2345–2355. [Google Scholar] [CrossRef] [Green Version]
- Vanrie, J.; Verfaillie, K. Perception of Biological Motion: A Stimulus Set of Human Point-Light Actions. Behav. Res. Methods Instrum. Comput. 2004, 36, 625–629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blake, R.; Shiffrar, M. Perception of Human Motion. Annu. Rev. Psychol. 2007, 58, 47–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giese, M.A.; Poggio, T. Neural Mechanisms for the Recognition of Biological Movements. Nat. Rev. Neurosci. 2003, 4, 179–192. [Google Scholar] [CrossRef]
- Kandel, S.; Orliaguet, J.P.; Viviani, P. Perceptual Anticipation in Handwriting: The Role of Implicit Motor Competence. Percept. Psychophys. 2000, 62, 706–716. [Google Scholar] [CrossRef] [Green Version]
- Farsi, A.; Bahmanbegloo, Z.H.; Abdoli, B.; Ghorbani, S. The Effect of Observational Practice by a Point-Light Model on Learning a Novel Motor Skill. Percept. Mot. Skills 2016, 123, 477–488. [Google Scholar] [CrossRef]
- Francisco, V.; Decatoire, A.; Bidet-Ildei, C. Action Observation and Motor Learning: The Role of Action Observation in Learning Judo Techniques. Eur. J. Sport Sci. 2022, 1–23. [Google Scholar] [CrossRef]
- Hayes, S.J.; Hodges, N.J.; Scott, M.A.; Horn, R.R.; Williams, A.M. The Efficacy of Demonstrations in Teaching Children an Unfamiliar Movement Skill: The Effects of Object-Orientated Actions and Point-Light Demonstrations. J. Sports Sci. 2007, 25, 559–575. [Google Scholar] [CrossRef]
- Horn, R.R.; Williams, A.M.; Scott, M.A. Learning from Demonstrations: The Role of Visual Search during Observational Learning from Video and Point-Light Models. J. Sports Sci. 2002, 20, 253–269. [Google Scholar] [CrossRef]
- Saber Sotoodeh, M.; Taheri-Torbati, H. A Point-Light Display Model for Teaching Motor Skills to Children With Autism Spectrum Disorder: An Eye-Tracking Study. Percept. Mot. Skills 2021, 128, 1485–1503. [Google Scholar] [CrossRef] [PubMed]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilz, K.S.; Bennett, P.J.; Sekuler, A.B. Effects of Aging on Biological Motion Discrimination. Vis. Res. 2010, 50, 211–219. [Google Scholar] [CrossRef] [Green Version]
- Saygin, A.P.; Wilson, S.M.; Hagler, D.J., Jr.; Bates, E.; Sereno, M.I. Point-Light Biological Motion Perception Activates Human Premotor Cortex. J. Neurosci. 2004, 24, 6181–6188. [Google Scholar] [CrossRef] [Green Version]
- Ulloa, E.R.; Pineda, J.A. Recognition of Point-Light Biological Motion: Mu Rhythms and Mirror Neuron Activity. Behav. Brain Res. 2007, 183, 188–194. [Google Scholar] [CrossRef]
- Decatoire, A.; Beauprez, S.A.; Pylouster, J.; Lacouture, P.; Blandin, Y.; Bidet-Ildei, C. PLAViMoP: How to Standardize and Simplify the Use of Point-Light Displays. Behav. Res. Methods 2018, 51, 2573–2596. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation Study of WOMAC: A Health Status Instrument for Measuring Clinically Important Patient Relevant Outcomes to Antirheumatic Drug Therapy in Patients with Osteoarthritis of the Hip or Knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Bidet-Ildei, C.; Chauvin, A.; Coello, Y. Observing or Producing a Motor Action Improves Later Perception of Biological Motion: Evidence for a Gender Effect. Acta Psychol. 2010, 134, 215–224. [Google Scholar] [CrossRef]
- Casile, A.; Giese, M.A. Nonvisual Motor Training Influences Biological Motion Perception. Curr. Biol. 2006, 16, 69–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chary, C.; Meary, D.; Orliaguet, J.P.; David, D.; Moreaud, O.; Kandel, S. Influence of Motor Disorders on the Visual Perception of Human Movements in a Case of Peripheral Dysgraphia. Neurocase 2004, 10, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Agosta, F.; Gatti, R.; Sarasso, E.; Volonté, M.A.; Canu, E.; Meani, A.; Sarro, L.; Copetti, M.; Cattrysse, E.; Kerckhofs, E.; et al. Brain Plasticity in Parkinson’s Disease with Freezing of Gait Induced by Action Observation Training. J. Neurol. 2017, 264, 88–101. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Control Group | PLD Group | p-Value |
|---|---|---|---|
| Age (years) | 60.4 ± 10.3 | 64.8 ± 6.4 | 0.192 |
| BMI (kg/m²) | 30.7 ± 4.8 | 29.9 ± 4.8 | 0.691 |
| Score VAS | 2.8 ± 2.2 | 3.9 ± 1.9 | 0.149 |
| MMSE | 27.6 ± 2.4 | 28.8 ± 1.3 | 0.127 |
| Beck depression score | 1.07 ± 1.73 | 1.00 ± 2.45 | 0.930 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bidet-Ildei, C.; Deborde, Q.; Francisco, V.; Gand, E.; Blandin, Y.; Delaubier, A.; Jossart, A.; Rigoard, P.; Billot, M.; David, R. The Added Value of Point-Light Display Observation in Total Knee Arthroplasty Rehabilitation Program: A Prospective Randomized Controlled Pilot Study. Medicina 2022, 58, 868. https://doi.org/10.3390/medicina58070868
Bidet-Ildei C, Deborde Q, Francisco V, Gand E, Blandin Y, Delaubier A, Jossart A, Rigoard P, Billot M, David R. The Added Value of Point-Light Display Observation in Total Knee Arthroplasty Rehabilitation Program: A Prospective Randomized Controlled Pilot Study. Medicina. 2022; 58(7):868. https://doi.org/10.3390/medicina58070868
Chicago/Turabian StyleBidet-Ildei, Christel, Quentin Deborde, Victor Francisco, Elise Gand, Yannick Blandin, Anne Delaubier, Anne Jossart, Philippe Rigoard, Maxime Billot, and Romain David. 2022. "The Added Value of Point-Light Display Observation in Total Knee Arthroplasty Rehabilitation Program: A Prospective Randomized Controlled Pilot Study" Medicina 58, no. 7: 868. https://doi.org/10.3390/medicina58070868
APA StyleBidet-Ildei, C., Deborde, Q., Francisco, V., Gand, E., Blandin, Y., Delaubier, A., Jossart, A., Rigoard, P., Billot, M., & David, R. (2022). The Added Value of Point-Light Display Observation in Total Knee Arthroplasty Rehabilitation Program: A Prospective Randomized Controlled Pilot Study. Medicina, 58(7), 868. https://doi.org/10.3390/medicina58070868