
Hemp Seed Oil in Association with β-Caryophyllene, Myrcene and Ginger Extract as a Nutraceutical Integration in Knee Osteoarthritis: A Double-Blind Prospective Case-Control Study

 , ,
, ,  ,
,  ,
, 
 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
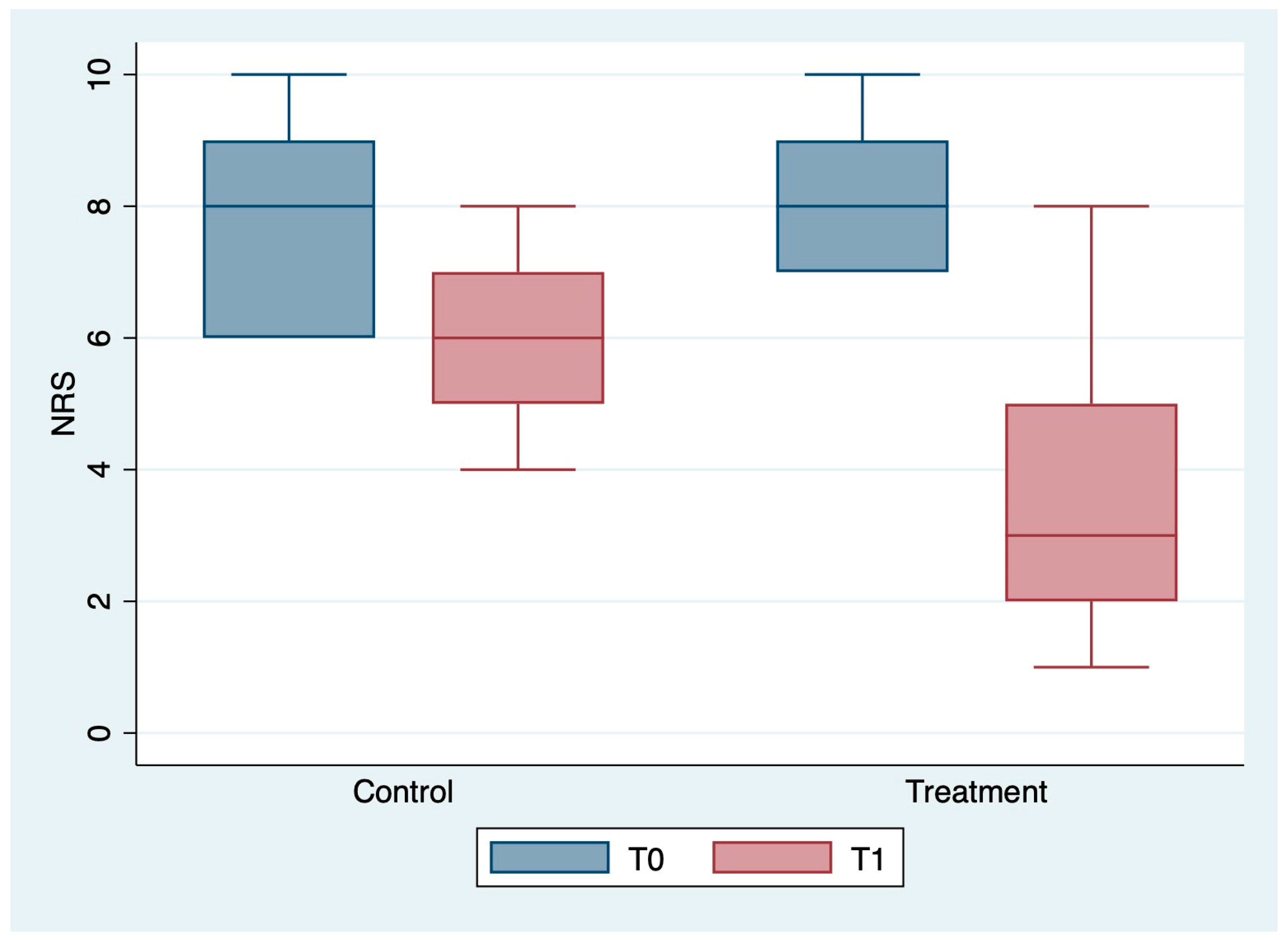
- Numeric Rating Scale (NRS): this is a one-dimensional scale that rates pain from 0, the absence of pain, to 10, the maximum perceived pain;
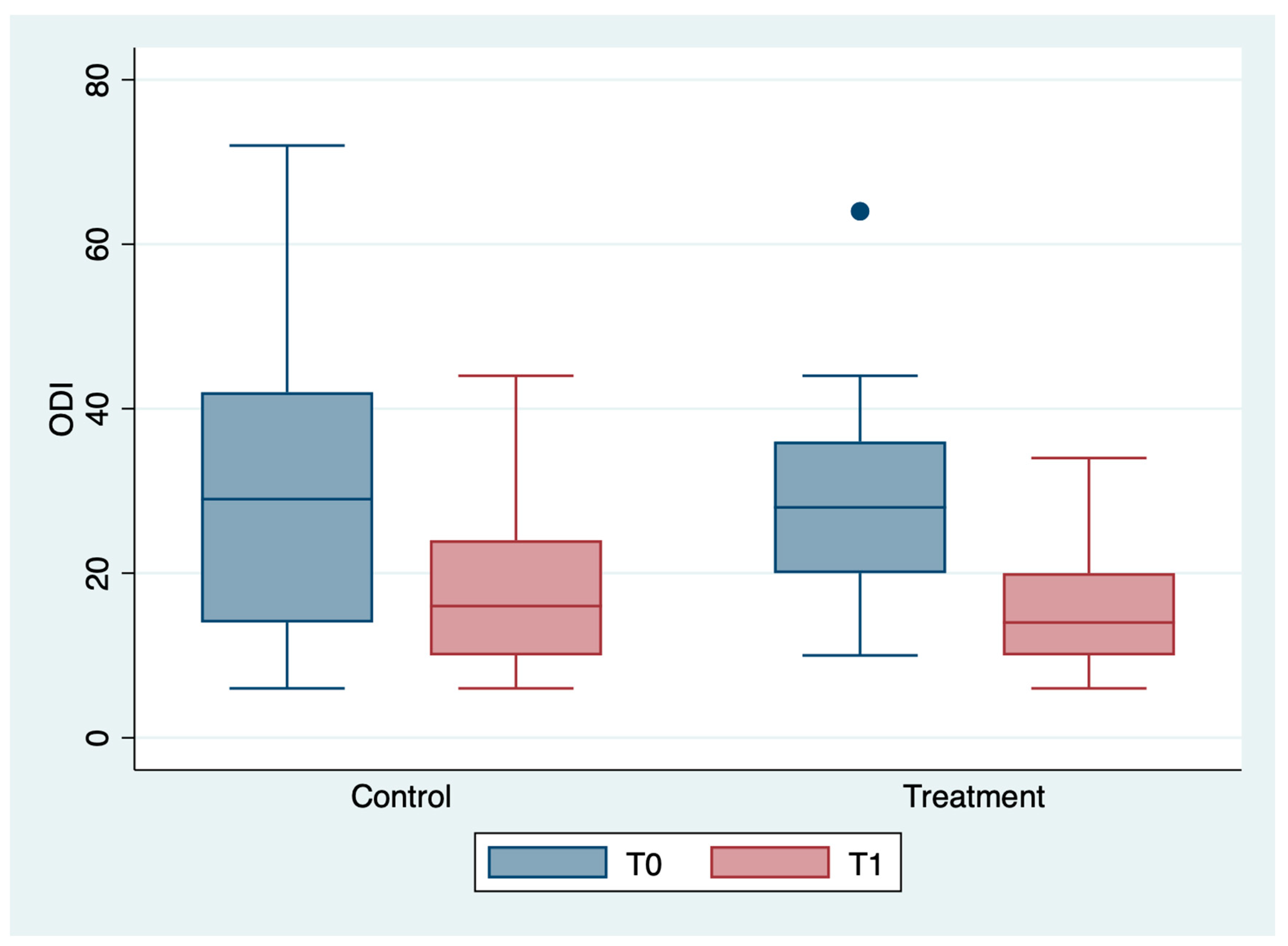
- Oswestry Disability Index (ODI): this is a scale that rates the percentage value of disability and ranges from 0%, no disability, to 100%, maximum disability;
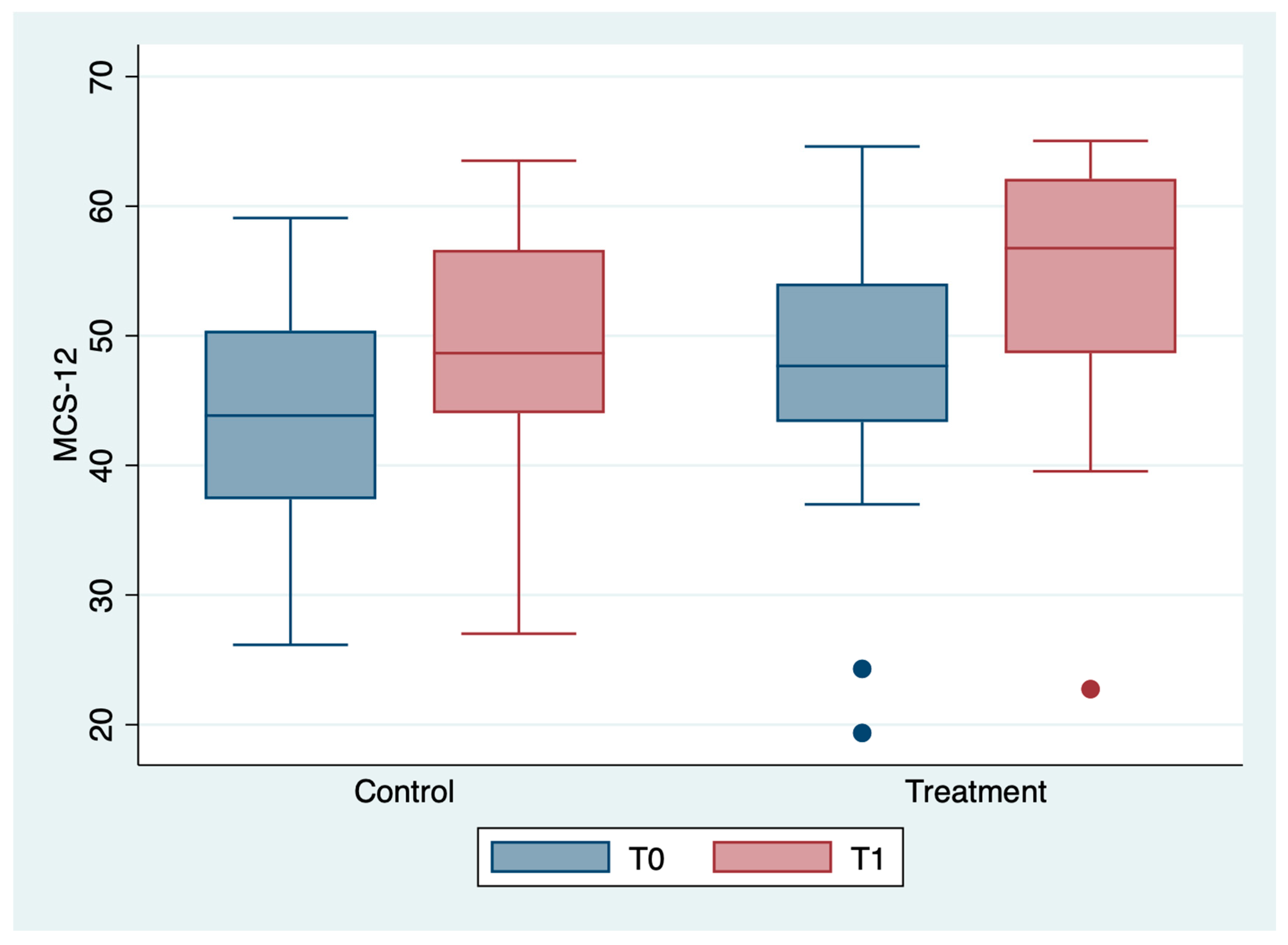
- Short Form 12 (SF-12): this is a quality of life assessment scale. It is divided into physical domain (PCS) and mental domain (MCS). The higher the score, the better the patients’ quality of life;
- Knee Injury and Osteoarthritis Outcome Score (KOOS): this is a percentage value that quantifies clinical symptoms, disability, and quality of life in patients suffering from knee diseases. It ranges from 0% (severe disability) to 100% (optimal condition);
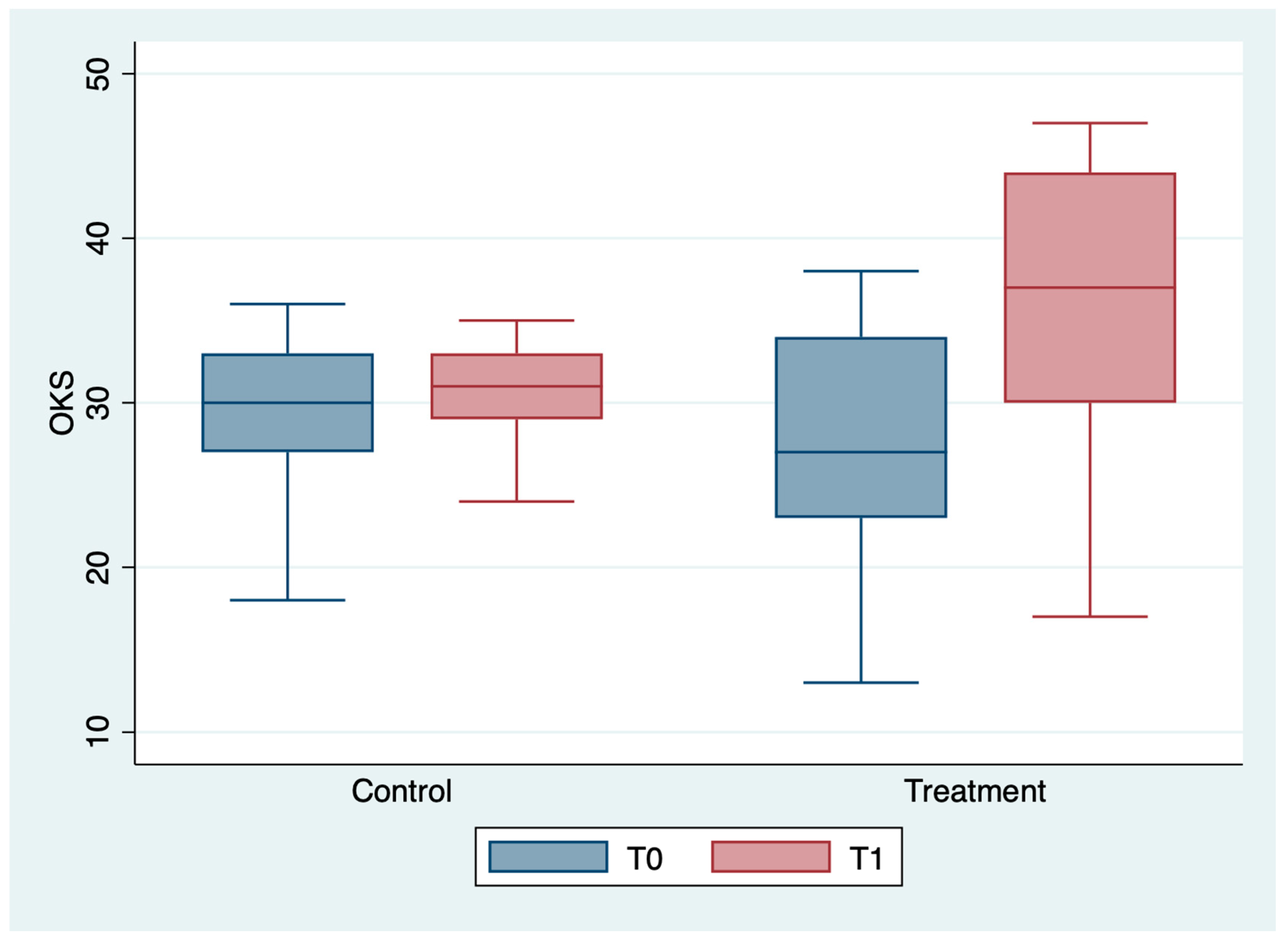
- Oxford Knee Score (OKS): this assesses the severity of osteoarthritis from 0 to 48 (severe osteoarthritis 0–19; moderate-severe osteoarthritis 20–29; mild-moderate osteoarthritis 30–39; no sign of osteoarthritis 40–48).
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Argenson, J.N.; Parratte, S.; Ollivier, M. Approches thérapeutiques de la gonarthrose [Therapeutic approaches to gonarthrosis]. Rev. Infirm. 2016, 223, 25–27. [Google Scholar] [CrossRef] [PubMed]
- Farì, G.; Pignatelli, G.; Macchiarola, D.; Bernetti, A.; Agostini, F.; Fornaro, M.; Mariconda, C.; Megna, M.; Ranieri, M. Cartilage damage: Clinical approach. Minerva Orthop. 2022, 73, 20–27. [Google Scholar] [CrossRef]
- Della Tommasa, S.; Winter, K.; Seeger, J.; Spitzbarth, I.; Brehm, W.; Troillet, A. Evaluation of Villus Synovium From Unaffected Metacarpophalangeal Joints of Adult and Juvenile Horses. J. Equine Vet. Sci. 2021, 102, 103637. [Google Scholar] [CrossRef]
- Kwiatkowski, K. Choroba zwyrodnieniowa stawu kolanowego—epidemiologia i czynniki ryzyka [Gonarthrosis—epidemiology and risk factors]. Pol. Merkur. Lekarski. 2004, 17, 410–414. [Google Scholar] [PubMed]
- Pape, D.; Tischer, T. Kniearthrose des jungen Patienten [Osteoarthritis of the knee in young patients]. Orthopade 2021, 50, 345. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.; Lee, K.; Ju, J.H. Recent Updates of Diagnosis, Pathophysiology, and Treatment on Osteoarthritis of the Knee. Int. J. Mol. Sci. 2021, 22, 2619. [Google Scholar] [CrossRef]
- Michael, J.W.; Schlüter-Brust, K.U.; Eysel, P. The epidemiology, etiology, diagnosis, and treatment of osteoarthritis of the knee. Dtsch. Arztebl. Int. 2010, 107, 152–162. [Google Scholar] [CrossRef]
- Hussain, S.M.; Neilly, D.W.; Baliga, S.; Patil, S.; Meek, R. Knee osteoarthritis: A review of management options. Scott. Med. J. 2016, 61, 7–16. [Google Scholar] [CrossRef]
- Mariconda, C.; Megna, M.; Farì, G.; Bianchi, F.P.; Puntillo, F.; Correggia, C.; Fiore, P. Therapeutic exercise and radiofrequency in the rehabilitation project for hip osteoarthritis pain. Eur. J. Phys. Rehabil. Med. 2020, 56, 451–458. [Google Scholar] [CrossRef]
- Farì, G.; de Sire, A.; Fallea, C.; Albano, M.; Grossi, G.; Bettoni, E.; Di Paolo, S.; Agostini, F.; Bernetti, A.; Puntillo, F.; et al. Efficacy of Radiofrequency as Therapy and Diagnostic Support in the Management of Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Diagnostics 2022, 12, 600. [Google Scholar] [CrossRef]
- Notarnicola, A.; Maccagnano, G.; Farì, G.; Bianchi, F.P.; Moretti, L.; Covelli, I.; Ribatti, P.; Mennuni, C.; Tafuri, S.; Pesce, V.; et al. Extracorporeal shockwave therapy for plantar fasciitis and gastrocnemius muscle: Effectiveness of a combined treatment. J. Biol. Regul. Homeost. Agents 2020, 34, 285–290. [Google Scholar] [PubMed]
- Vicenti, G.; Solarino, G.; Carrozzo, M.; De Giorgi, S.; Moretti, L.; De Crescenzo, A.; Moretti, B. Major concern in the multiligament injuried knee treatment: A systematic review. Injury 2019, 50 (Suppl. 2), S89–S94. [Google Scholar] [CrossRef] [PubMed]
- Sachdeva, V.; Roy, A.; Bharadvaja, N. Current Prospects of Nutraceuticals: A Review. Curr. Pharm. Biotechnol. 2020, 21, 884–896. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Browne, H.; Mobasheri, A.; Rayman, M.P. What is the evidence for a role for diet and nutrition in osteoarthritis? Rheumatology 2018, 57 (suppl. 4), iv61–iv74. [Google Scholar] [CrossRef] [Green Version]
- Iftikhar, A.; Zafar, U.; Ahmed, W.; Shabbir, M.A.; Sameen, A.; Sahar, A.; Bhat, Z.F.; Kowalczewski, P.Ł.; Jarzębski, M.; Aadil, R.M. Applications of Cannabis Sativa L. in Food and Its Therapeutic Potential: From a Prohibited Drug to a Nutritional Supplement. Molecules 2021, 26, 7699. [Google Scholar] [CrossRef]
- Farì, G.; Santagati, D.; Pignatelli, G.; Scacco, V.; Renna, D.; Cascarano, G.; Vendola, F.; Bianchi, F.P.; Fiore, P.; Ranieri, M.; et al. Collagen Peptides, in Association with Vitamin C, Sodium Hyaluronate, Manganese and Copper, as Part of the Rehabilitation Project in the Treatment of Chronic Low Back Pain. Endocr. Metab. Immune Disord. Drug Targets 2022, 22, 108–115. [Google Scholar] [CrossRef]
- Koppel, B.S.; Brust, J.C.; Fife, T.; Bronstein, J.; Youssof, S.; Gronseth, G.; Gloss, D. Systematic review: Efficacy and safety of medical marijuana in selected neurologic disorders: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2014, 82, 1556–1563. [Google Scholar] [CrossRef]
- Russo, E.B.; Marcu, J. Cannabis pharmacology: The usual suspects and a few promising leads. Adv Pharmacol. 2017, 80, 67–134. [Google Scholar]
- Hill, K.P. Medical marijuana for treatment of chronic pain and other medical and psychiatric problems: A clinical review. JAMA 2015, 313, 2474–2483. [Google Scholar] [CrossRef]
- Romero-Sandoval, E.A.; Fincham, J.E.; Kolano, A.L.; Sharpe, B.N.; Alvarado-Vazquez, P.A. Cannabis for chronic pain: Challenges and considerations. Pharmacotherapy 2018, 38, 651–662. [Google Scholar] [CrossRef]
- Weston-Green, K. The United Chemicals of Cannabis: Beneficial effects of Cannabis phytochemicals on the brain and cognition. In Recent Advances in Cannabinoid Research; Costain, W., Laprairie, R.B., Eds.; IntechOpen: London, UK, 2018; pp. 83–100. [Google Scholar]
- Liktor-Busa, E.; Keresztes, A.; LaVigne, J.; Streicher, J.M.; Largent-Milnes, T.M. Analgesic Potential of Terpenes Derived from Cannabis sativa. Pharmacol. Rev. 2021, 73, 98–126. [Google Scholar] [CrossRef] [PubMed]
- Sharma, C.; Al Kaabi, J.M.; Nurulain, S.M.; Goyal, S.N.; Kamal, M.A.; Ojha, S. Polypharmacological properties and therapeutic potential of b-caryophyllene: A dietary phytocannabinoid of pharmaceutical promise. Curr. Pharm. Des. 2016, 22, 3237–3264. [Google Scholar] [CrossRef] [PubMed]
- Gertsch, J.; Leonti, M.; Raduner, S.; Racz, I.; Chen, J.Z.; Xie, X.Q.; Altmann, K.H.; Karsak, M.; Zimmer, A. Beta-caryophyllene is a dietary cannabinoid. Proc. Natl. Acad. Sci. USA 2008, 105, 9099–9104. [Google Scholar] [CrossRef] [Green Version]
- Whiteside, G.; Lee, G.; Valenzano, K. The Role of the Cannabinoid CB2 Receptor in Pain Transmission and Therapeutic Potential of Small Molecule CB2 Receptor Agonists. Curr. Med. Chem. 2007, 14, 917–936. [Google Scholar] [CrossRef] [PubMed]
- Rufino, A.T.; Ribeiro, M.; Sousa, C.; Judas, F.; Salgueiro, L.; Cavaleiro, C.; Mendes, A.F. Evaluation of the anti-inflammatory, anti-catabolic and pro-anabolic effects of E-caryophyllene, myrcene and limonene in a cell model of osteoarthritis. Eur. J. Pharmacol. 2015, 750, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Phan, P.V.; Sohrabi, A.; Polotsky, A.; Hungerford, D.S.; Lindmark, L.; Frondoza, C.G. Ginger extract components suppress induction of chemokine expression in human synoviocytes. J. Altern. Complement. Med. 2005, 11, 149–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, J.Y.; Wang, Q.; Wang, Y.C.; Xiang, F.; Tian, X.C.; Liu, D.H.; Dong, Z. [β-caryophyllene alleviates cerebral ischemia/ reperfusion injury in mice by activating autophagy]. Zhongguo Zhong Yao Za Zhi 2020, 45, 932–936. [Google Scholar]
- Mattiuzzo, E.; Faggian, A.; Venerando, R.; Benetti, A.; Belluzzi, E.; Abatangelo, G.; Ruggieri, P.; Brun, P. In Vitro Effects of Low Doses of β-Caryophyllene, Ascorbic Acid and d-Glucosamine on Human Chondrocyte Viability and Inflammation. Pharmaceuticals 2021, 14, 286. [Google Scholar] [CrossRef]
- Irrera, N.; D’Ascola, A.; Pallio, G.; Bitto, A.; Mazzon, E.; Mannino, F.; Squadrito, V.; Arcoraci, V.; Minutoli, L.; Campo, G.M.; et al. β-Caryophyllene Mitigates Collagen Antibody Induced Arthritis (CAIA) in Mice Through a Cross-Talk between CB2 and PPAR-γ Receptors. Biomolecules 2019, 9, 326. [Google Scholar] [CrossRef] [Green Version]
- Bernetti, A.; Agostini, F.; Alviti, F.; Giordan, N.; Martella, F.; Santilli, V.; Paoloni, M.; Mangone, M. New Viscoelastic Hydrogel Hymovis MO.RE. Single Intra-articular Injection for the Treatment of Knee Osteoarthritis in Sportsmen: Safety and Efficacy Study Results. Front. Pharmacol. 2021, 12, 673988. [Google Scholar] [CrossRef]
- Scandiffio, R.; Geddo, F.; Cottone, E.; Querio, G.; Antoniotti, S.; Gallo, M.P.; Maffei, M.E.; Bovolin, P. Protective Effects of (E)-β-Caryophyllene (BCP) in Chronic Inflammation. Nutrients 2020, 12, 3273. [Google Scholar] [CrossRef] [PubMed]
- Ou, M.C.; Hsu, T.F.; Lai, A.C.; Lin, Y.T.; Lin, C.C. Pain relief assessment by aromatic essential oil massage on outpatients with primary dysmenorrhea: A randomized, double-blind clinical trial. J. Obstet. Gynaecol. Res. 2012, 38, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Shim, H.I.; Song, D.J.; Shin, C.M.; Yoon, H.; Park, Y.S.; Kim, N.; Lee, D.H. [Inhibitory Effects of β-caryophyllene on Helicobacter pylori Infection: A Randomized Double-blind, Placebo-controlled Study]. Korean J. Gastroenterol. 2019, 74, 199–204. [Google Scholar] [CrossRef] [Green Version]
- Fidyt, K.; Fiedorowicz, A.; Strządała, L.; Szumny, A. Β-Caryophyllene and Β-Caryophyllene Oxide—Natural compounds of anticancer and analgesic properties. Cancer Med. 2016, 5, 3007–3017. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, M.M.; Porreca, F.; Lai, J.; Albrecht, P.J.; Rice, F.L.; Khodorova, A.; Davar, G.; Makriyannis, A.; Vanderah, T.W.; Mata, H.P.; et al. CB2 cannabinoid receptor activation produces antinociception by stimulating peripheral release of endogenous opioids. Proc. Natl. Acad. Sci. USA 2005, 102, 3093–3098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandes, E.S.; Passos, G.F.; Medeiros, R.; da Cunha, F.M.; Ferreira, J.; Campos, M.M.; Pianowski, L.F.; Calixto, J.B. Anti-inflammatory effects of compounds alpha-humulene and (-)-trans-caryophyllene isolated from the essential oil of Cordia verbenacea. Eur. J. Pharmacol. 2007, 569, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Paula-Freire, L.I.G.; Andersen, M.L.; Gama, V.S.; Molska, G.R.; Carlini, E.L.A. The oral administration of trans-caryophyllene attenuates acute and chronic pain in mice. Phytomedicine 2014, 21, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Islam, A.U.S.; Hellman, B.; Nyberg, F.; Amir, N.; Jayaraj, R.L.; Petroianu, G.; Adem, A. Myrcene Attenuates Renal Inflammation and Oxidative Stress in the Adrenalectomized Rat Model. Molecules 2020, 25, 4492. [Google Scholar] [CrossRef]
- Jansen, C.; Shimoda, L.M.N.; Kawakami, J.K.; Ang, L.; Bacani, A.J.; Baker, J.D.; Badowski, C.; Speck, M.; Stokes, A.J.; Small-Howard, A.L.; et al. Myrcene and terpene regulation of TRPV1. Channels 2019, 13, 344–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, S.J.; Wang, Y.H.; Huang, L.C. The effect of oral low molecular weight liquid hyaluronic acid combination with glucosamine and chondroitin on knee osteoarthritis patients with mild knee pain: An 8-week randomized double-blind placebo-controlled trial. Medicine 2021, 100, e24252. [Google Scholar] [CrossRef]
- Brien, S.; Prescott, P.; Coghlan, B.; Bashir, N.; Lewith, G. Systematic review of the nutritional supplement Perna Canaliculus (green-lipped mussel) in the treatment of osteoarthritis. QJM 2008, 101, 167–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verrico, C.D.; Wesson, S.; Konduri, V.; Hofferek, C.J.; Vazquez-Perez, J.; Blair, E.; Dunner, K., Jr.; Salimpour, P.; Decker, W.K.; Halpert, M.M. A randomized, double-blind, placebo-controlled study of daily cannabidiol for the treatment of canine osteoarthritis pain. Pain 2020, 161, 2191–2202. [Google Scholar] [CrossRef] [PubMed]
- Vela, J.; Dreyer, L.; Petersen, K.K.; Arendt-Nielsen, L.; Duch, K.S.; Kristensen, S. Cannabidiol treatment in hand osteoarthritis and psoriatic arthritis: A randomized, double-blind, placebo-controlled trial. Pain 2022, 163, 1206–1214. [Google Scholar] [CrossRef] [PubMed]
- Fairbank, J.C.; Pynsent, P.B. The Oswestry Disability Index. Spine 2000, 25, 2940–2952. [Google Scholar] [CrossRef]
- Lera, L.; Márquez, C.; Saguez, R.; Moya, M.O.; Angel, B.; Albala, C. Calidad de vida en personas mayores con depresión y dependencia funcional: Validez del cuestionario SF-12 [Quality of life of older people with depression and dependence: Validity of the SF-12 (short form health survey) questionnaire]. Rev. Med. Chil. 2021, 149, 1292–1301. [Google Scholar] [CrossRef]
- Werner, S. Anterior knee pain: An update of physical therapy. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2286–2294. [Google Scholar] [CrossRef]
- Bahr, T.; Allred, K.; Martinez, D.; Rodriguez, D.; Winterton, P. Effects of a massage-like essential oil application procedure using Copaiba and Deep Blue oils in individuals with hand arthritis. Complement. Ther. Clin. Pract. 2018, 33, 170–176. [Google Scholar] [CrossRef]
- Topp, R.; Brosky, J.A., Jr.; Pieschel, D. The effect of either topical menthol or a placebo on functioning and knee pain among patients with knee OA. J. Geriatr. Phys. Ther. 2013, 36, 92–99. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Wang, Z.; Fu, X.; Lin, Z.; Yu, K. Geraniol-mediated osteoarthritis improvement by down-regulating PI3K/Akt/NF-κB and MAPK signals: In vivo and in vitro studies. Int. Immunopharmacol. 2020, 86, 106713. [Google Scholar] [CrossRef] [PubMed]
- Leach, M.J.; Kumar, S. The clinical effectiveness of Ginger (Zingiber Officinale) in adults with osteoarthritis. JBI Libr. Syst. Rev. 2008, 6, 310–323. [Google Scholar] [CrossRef]
- Tenti, S.; Mondanelli, N.; Bernetti, A.; Mangone, M.; Agostini, F.; Capassoni, M.; Cheleschi, S.; De Chiara, R.; Farì, G.; Frizziero, A.; et al. Impact of Covid-19 pandemic on injection-based practice: Report from an Italian multicenter and multidisciplinary survey. Ann. Ig. 2022, 34, 501–514. [Google Scholar] [PubMed]
- Bernetti, A.; Farì, G.; Mangone, M.; Fiore, P.; Santilli, V.; Paoloni, M.; Agostini, F. Medical management of osteoarthritis during the COVID-19 pandemic: A challenge for the present and the future. Ann. Di Ig. Med. Prev. E Di Comunita 2022, 34, 184–189. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Control (n = 19) | Treatment (n = 19) | Total (n = 38) | p-Value |
|---|---|---|---|---|
| Females; n (%) | 10 (52.6) | 10 (52.6) | 20 (52.6) | 1.000 |
| Age(years); mean ± SD (range) | 59.7 ± 6.6 (47–69) | 54.5 ± 4.6 (48–65) | 57.1 ± 6.2 (47–69) | 0.008 |
| BMI; mean ± SD (range) | 27.9 ± 3.8 (20.4–33.4) | 29.6 ± 6.3 (20.0–49.3) | 28.7 ± 5.2 (20.0–49.3) | 0.376 |
| Variable | Control (n = 19) | Treatment (n = 19) | Total (n = 38) | Group Comparison | Time Comparison | Time and Group Interaction |
|---|---|---|---|---|---|---|
| NRS T0 | 7.6 ± 1.4 (6–10) | 8.3 ± 1.1 (7–10) | 7.9 ± 1.3 (6–10) | 0.080 | <0.0001 | <0.0001 |
| NRS T1 | 5.7 ± 1.2 (4–8) | 3.5 ± 2.1 (1–8) | 4.6 ± 2.0 (1–8) | |||
| ODI T0 | 31.3 ± 18.9 (6–72) | 29.8 ± 12.8 (10–64) | 30.6 ± 15.9 (6–72) | 0.687 | <0.0001 | 0.963 |
| ODI T1 | 17.2 ± 9.3 (6–44) | 15.9 ± 7.2 (6–34) | 16.6 ± 8.2 (6–44) | |||
| PCS12 T0 | 36.5 ± 8.4 (21.7–50.6) | 37.6 ± 7.7 (22.8–51.8) | 37.1 ± 8.0 (21.7–51.8) | 0.045 | <0.0001 | 0.066 |
| PCS12 T1 | 42.6 ± 6.9 (30.2–52.6) | 50.2 ± 10.0 (26.7–64.6) | 46.4 ± 9.3 (26.7–64.6) | |||
| MCS12 T0 | 43.3 ± 10.1 (26.2–59.1) | 46.5 ± 10.7 (19.4–64.6) | 44.9 ± 10.4 (19.4–64.6) | 0.138 | <0.0001 | 0.190 |
| MCS12 T1 | 47.9 ± 10.7 (27.0–63.5) | 54.3 ± 10.3 (22.7–65.0) | 51.2 ± 10.8 (22.7–65.0) | |||
| KOOS T0 | 62.9 ± 9.2 (45–76) | 59.8 ± 7.1 (45–72) | 61.4 ± 8.2 (45–76) | 0.403 | <0.0001 | <0.001 |
| KOOS T1 | 66.4 ± 8.6 (51–76) | 74.0 ± 11.0 (48–89) | 70.2 ± 10.5 (58–89) | |||
| OKS T0 | 29.4 ± 4.8 (18–36) | 27.4 ± 6.3 (13–38) | 28.4 ± 5.6 (13–38) | 0.278 | <0.0001 | <0.0001 |
| OKS T1 | 30.6 ± 3.1 (24–35) | 36.6 ± 8.2 (17–47) | 33.6 ± 6.8 (17–47) |
| Determinants | Coef. | 95%CI | p-Value |
|---|---|---|---|
| Group (treatment vs. control) | −2.8 | −4.0–1.6 | <0.0001 |
| Sex (male vs. female) | 0.04 | −1.08–1.17 | 0.938 |
| Age (years) | 0.04 | −0.06–0.14 | 0.404 |
| BMI | 0.04 | −0.07–0.15 | 0.486 |
| Determinants | Coef. | 95%CI | p-Value |
|---|---|---|---|
| Group (treatment vs. control) | 0.89 | −9.0–10.8 | 0.856 |
| Sex (male vs. female) | −4.70 | −13.8–4.4 | 0.303 |
| Age (years) | −0.19 | −0.98–0.61 | 0.640 |
| BMI | −0.97 | −1.88–−0.07 | 0.036 |
| Determinants | Coef. | 95%CI | p-Value |
|---|---|---|---|
| Group (treatment vs. control) | 8.5 | 0.6–16.3 | 0.036 |
| Sex (male vs. female) | 0.6 | −6.6–7.8 | 0.864 |
| Age (years) | 0.2 | −0.4–0.9 | 0.409 |
| BMI | −0.4 | −1.1–0.3 | 0.036 |
| Determinants | Coef. | 95%CI | p-Value |
|---|---|---|---|
| Group (treatment vs. control) | 3.7 | −2.3–9.6 | 0.218 |
| Sex (male vs. female) | −0.03 | −5.50–5.44 | 0.992 |
| Age (years) | 0.10 | −0.38–0.58 | 0.674 |
| BMI | 0.08 | −0.46–0.62 | 0.769 |
| Determinants | Coef. | 95%CI | p-Value |
|---|---|---|---|
| Group (treatment vs. control) | 11.9 | 5.8–18.0 | <0.0001 |
| Sex (male vs. female) | 0.7 | −4.9–6.3 | 0.792 |
| Age (years) | 0.2 | −0.3–0.6 | 0.515 |
| BMI | −0.2 | −0.8–0.3 | 0.402 |
| Determinants | Coef. | 95%CI | p-Value |
|---|---|---|---|
| Group (treatment vs. control) | 8.5 | 5.4–11.7 | <0.0001 |
| Sex (male vs. female) | 0.4 | −2.5–3.3 | 0.796 |
| Age (years) | 0.1 | −0.2–0.3 | 0.511 |
| BMI | −0.1 | −0.4–0.2 | 0.537 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farì, G.; Megna, M.; Scacco, S.; Ranieri, M.; Raele, M.V.; Chiaia Noya, E.; Macchiarola, D.; Bianchi, F.P.; Carati, D.; Panico, S.; et al. Hemp Seed Oil in Association with β-Caryophyllene, Myrcene and Ginger Extract as a Nutraceutical Integration in Knee Osteoarthritis: A Double-Blind Prospective Case-Control Study. Medicina 2023, 59, 191. https://doi.org/10.3390/medicina59020191
Farì G, Megna M, Scacco S, Ranieri M, Raele MV, Chiaia Noya E, Macchiarola D, Bianchi FP, Carati D, Panico S, et al. Hemp Seed Oil in Association with β-Caryophyllene, Myrcene and Ginger Extract as a Nutraceutical Integration in Knee Osteoarthritis: A Double-Blind Prospective Case-Control Study. Medicina. 2023; 59(2):191. https://doi.org/10.3390/medicina59020191
Chicago/Turabian StyleFarì, Giacomo, Marisa Megna, Salvatore Scacco, Maurizio Ranieri, Maria Vittoria Raele, Enrica Chiaia Noya, Dario Macchiarola, Francesco Paolo Bianchi, Davide Carati, Simona Panico, and et al. 2023. "Hemp Seed Oil in Association with β-Caryophyllene, Myrcene and Ginger Extract as a Nutraceutical Integration in Knee Osteoarthritis: A Double-Blind Prospective Case-Control Study" Medicina 59, no. 2: 191. https://doi.org/10.3390/medicina59020191
APA StyleFarì, G., Megna, M., Scacco, S., Ranieri, M., Raele, M. V., Chiaia Noya, E., Macchiarola, D., Bianchi, F. P., Carati, D., Panico, S., Di Campi, E., Gnoni, A., Scacco, V., Inchingolo, A. D., Qorri, E., Scarano, A., & Rapone, B. (2023). Hemp Seed Oil in Association with β-Caryophyllene, Myrcene and Ginger Extract as a Nutraceutical Integration in Knee Osteoarthritis: A Double-Blind Prospective Case-Control Study. Medicina, 59(2), 191. https://doi.org/10.3390/medicina59020191