

Impact of Direct-Acting Antiviral Therapy on Liver Fibrosis Regression among People with Chronic HCV Infection: Results from a Real-Life Cohort in Patients Who Achieved Sustained Virological Response
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample
- (1)
- Treatment-naïve (NAÏVE): patients who had not previously received treatment for chronic HCV infection.
- (2)
- Poor tolerance to a previous IFN therapy (PTP IFN): patients who did not complete a previous IFN therapy due to severe side effects.
- (3)
- Partial response to a previous DAA therapy (PRP DAA): patients with new-onset detectable viral load after achieving SVR with a previous DAA therapy.
- (4)
- No response to a previous DAA therapy (NRP DAA): patients who did not achieve SVR after completing a previous DAA therapy.
- (5)
- Partial response to a previous IFN therapy (PRP IFN): patients with new-onset detectable viral load after achieving SVR with a previous IFN therapy.
- (6)
- No response to a previous IFN therapy (NRP IFN): patients who did not achieve SVR after completing a previous IFN therapy.
2.2. FibroScan®
2.3. HCV Viral Load and GT
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. DAA Therapy
3.3. Complications
3.4. FibroScan® Values
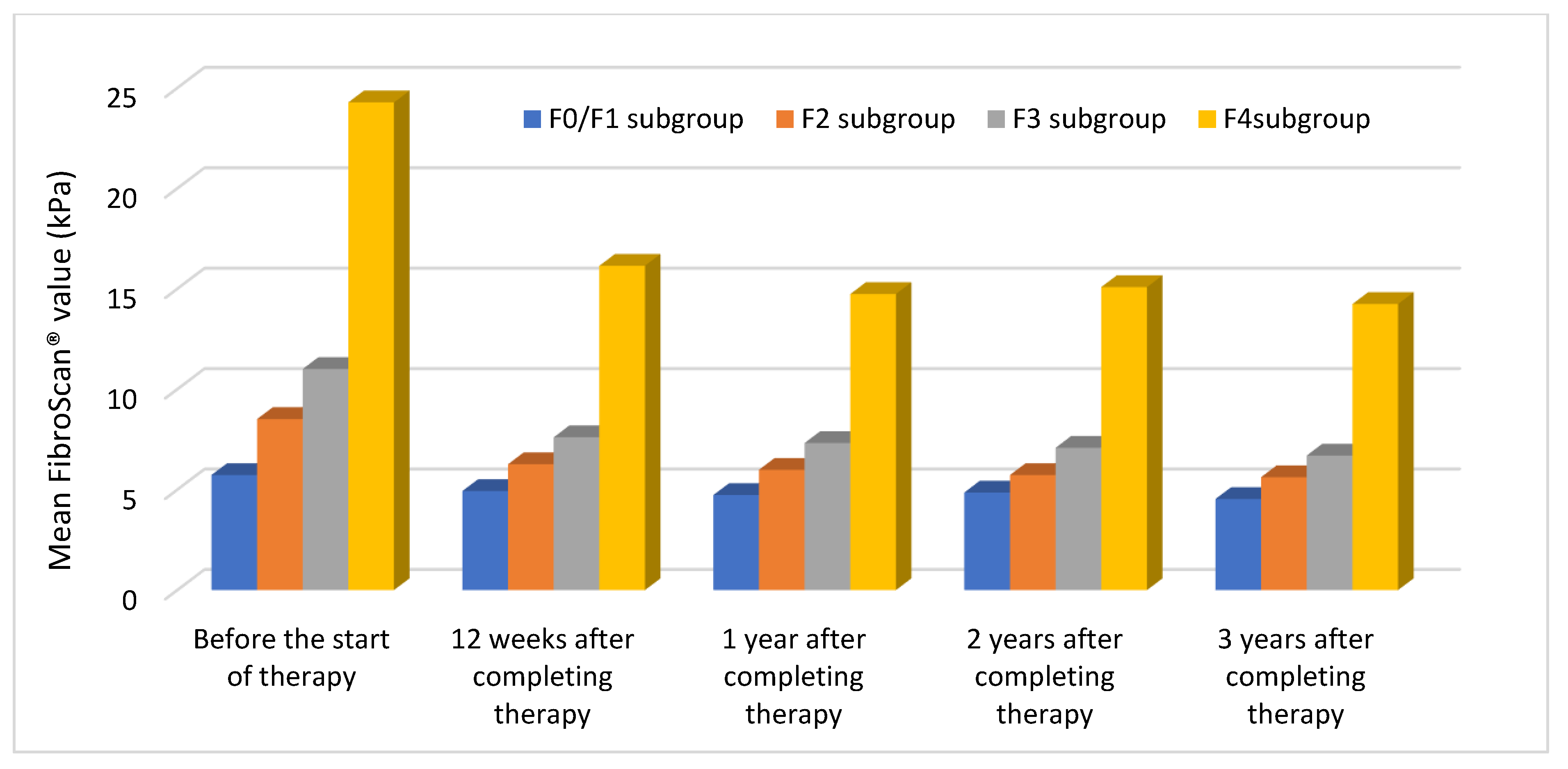
3.4.1. Mean Values in Each Subgroup
3.4.2. Success Rates
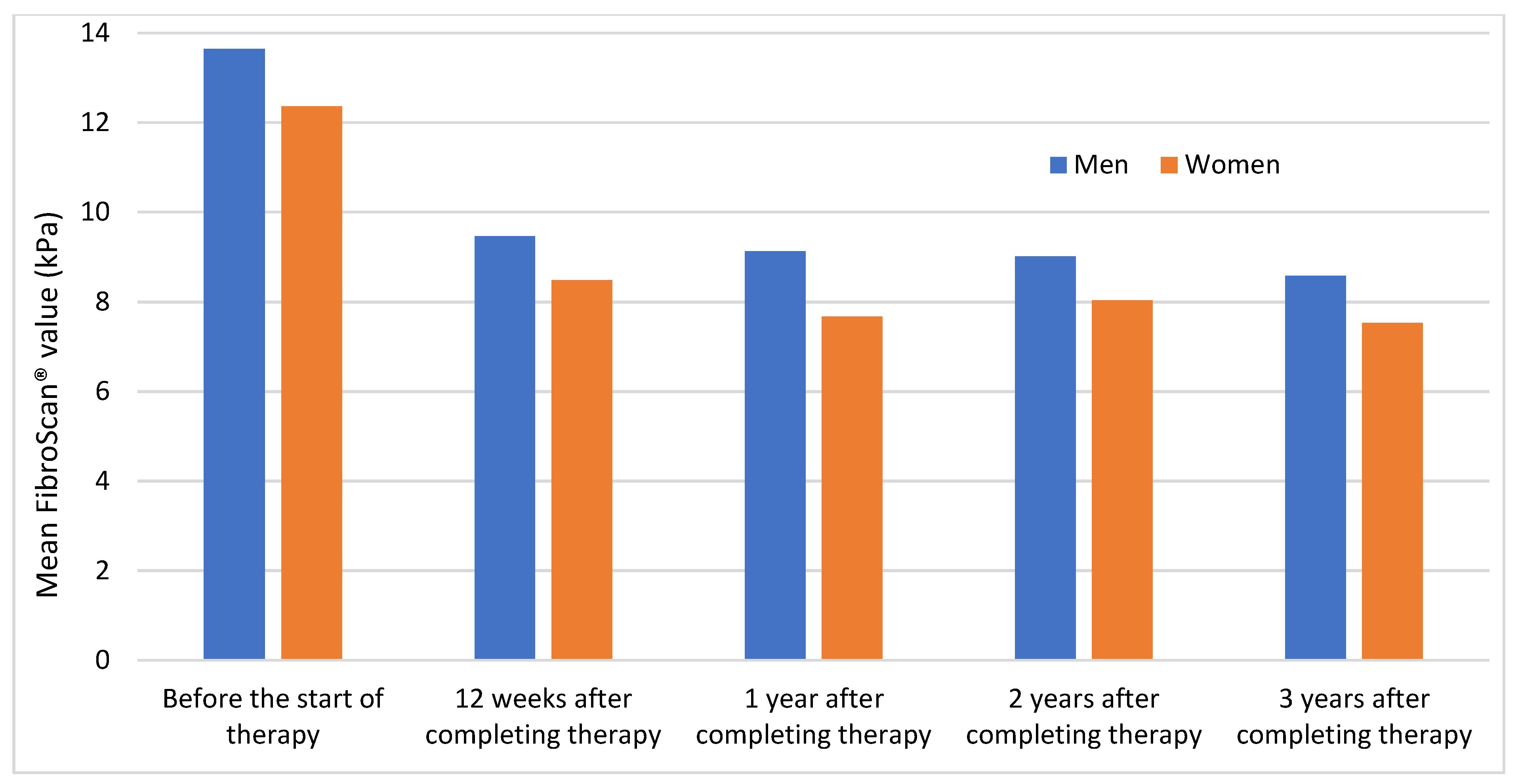
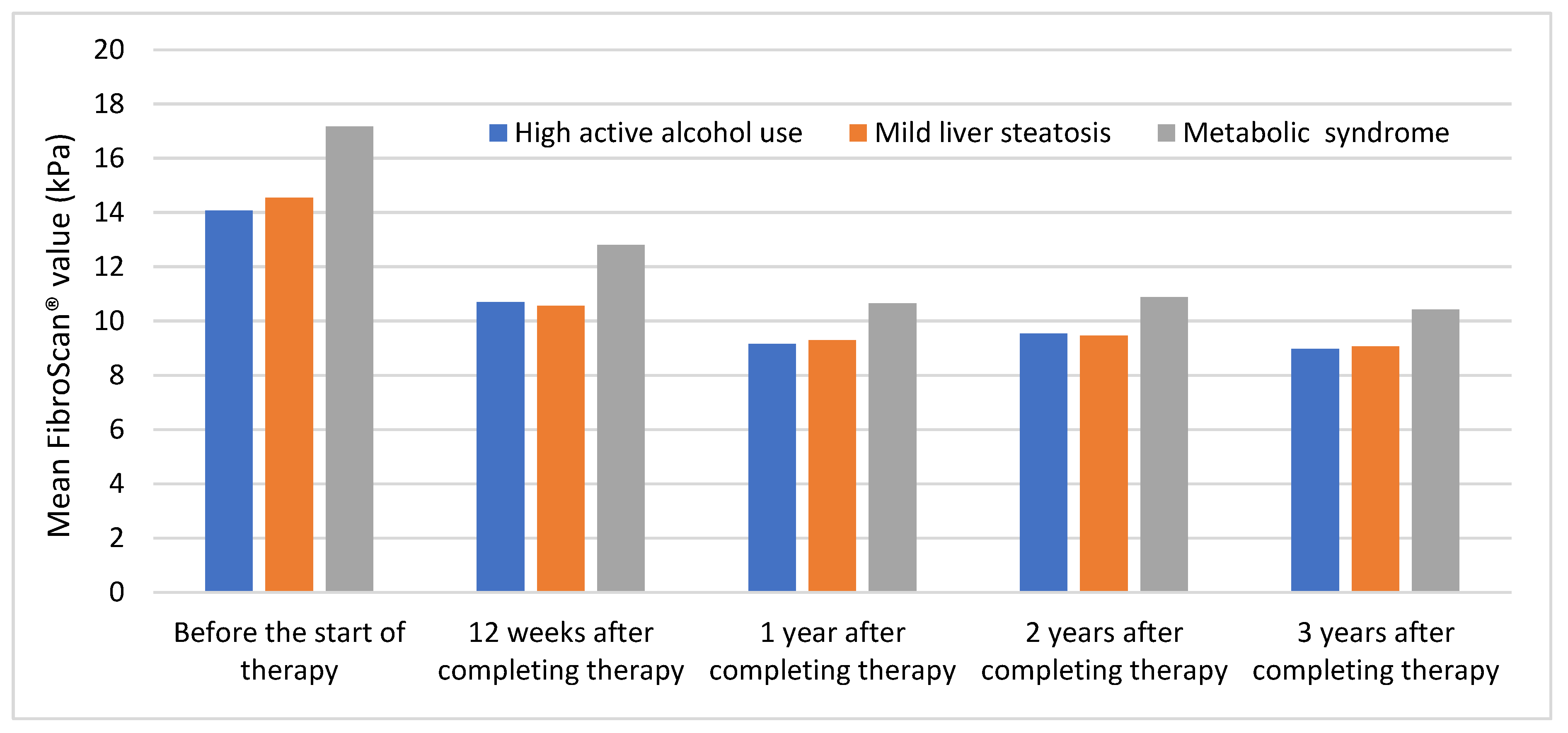
3.4.3. Patient Variables
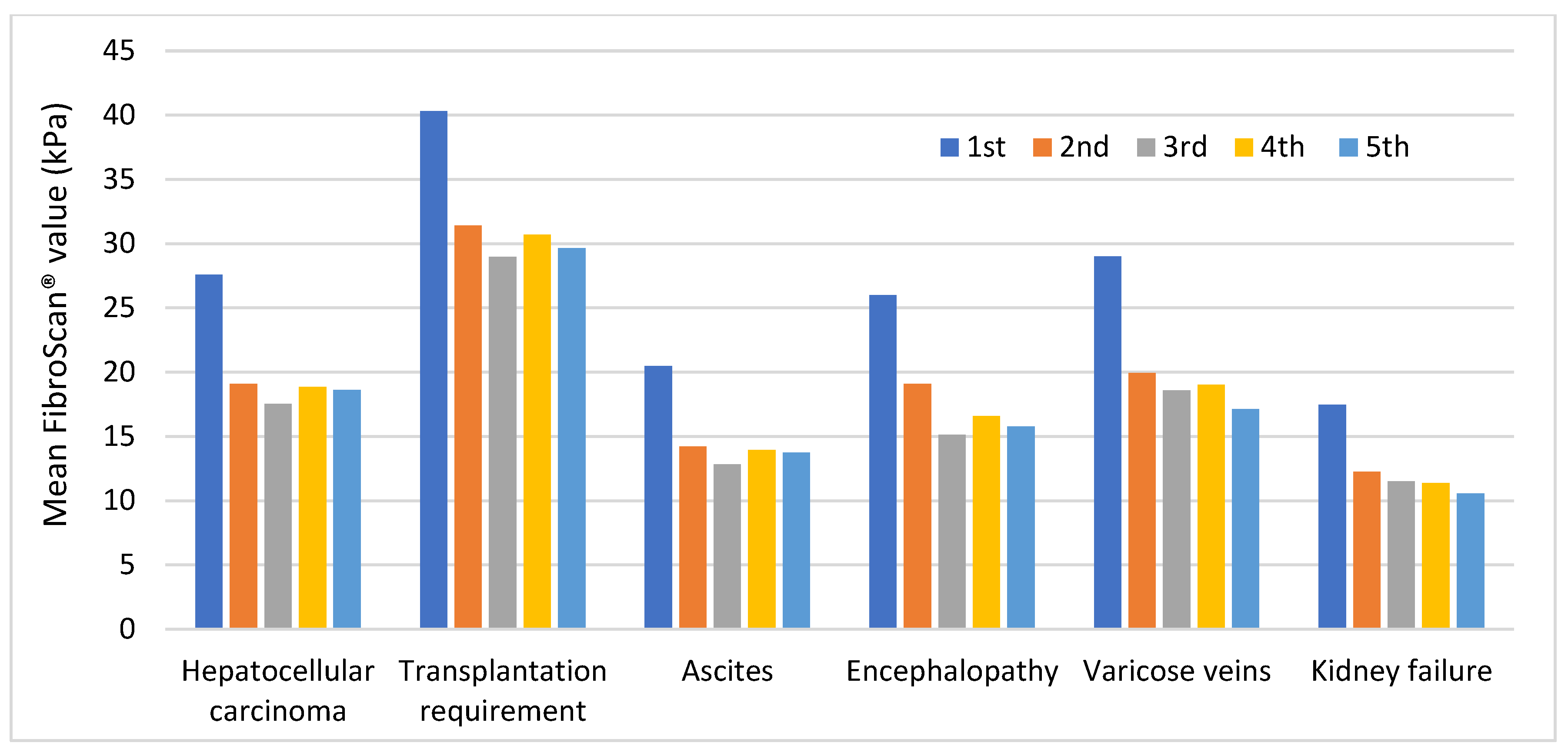
3.4.4. Complications
3.5. Distribution in Subgroups
3.5.1. F4 Subgroup
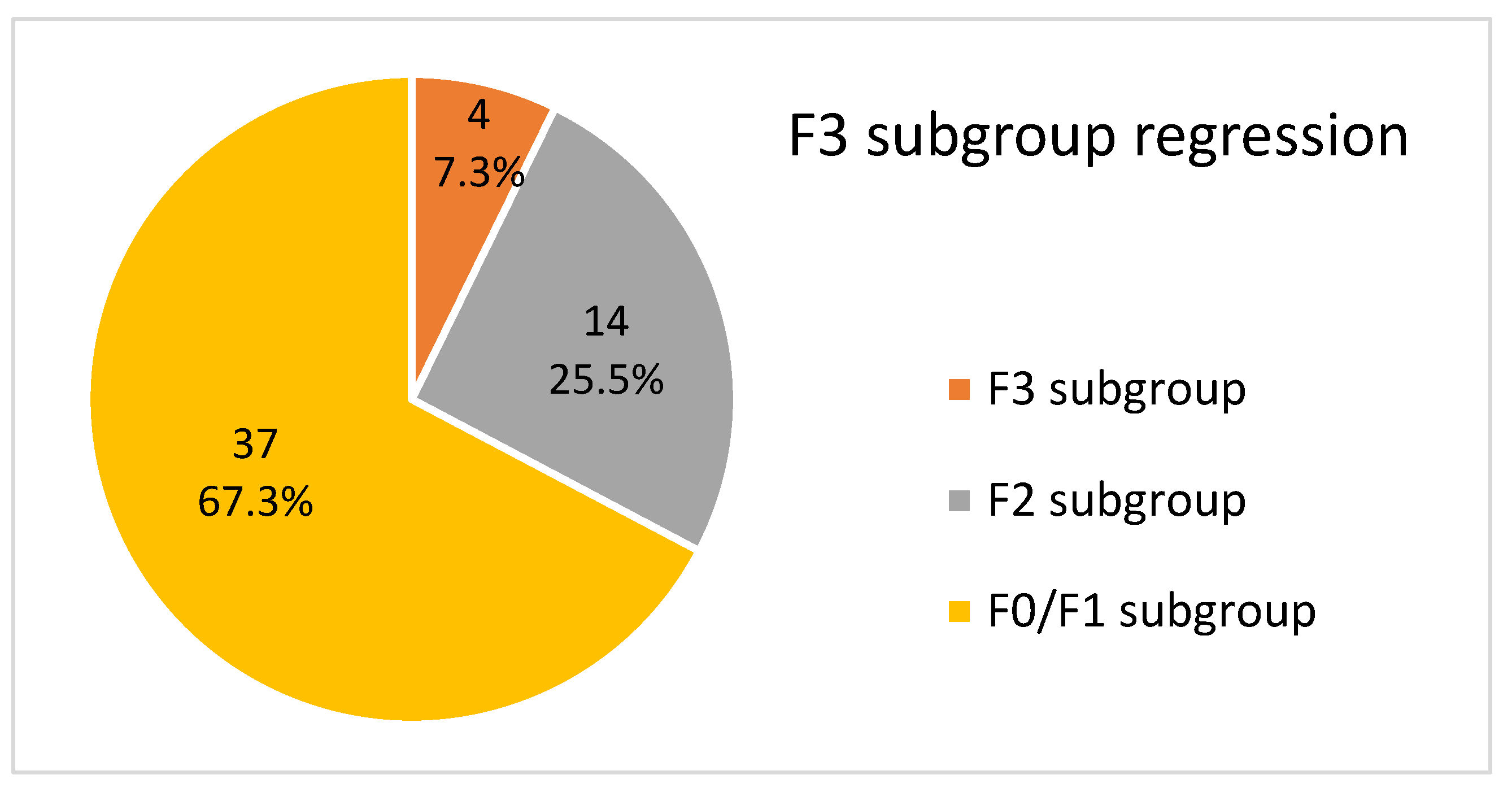
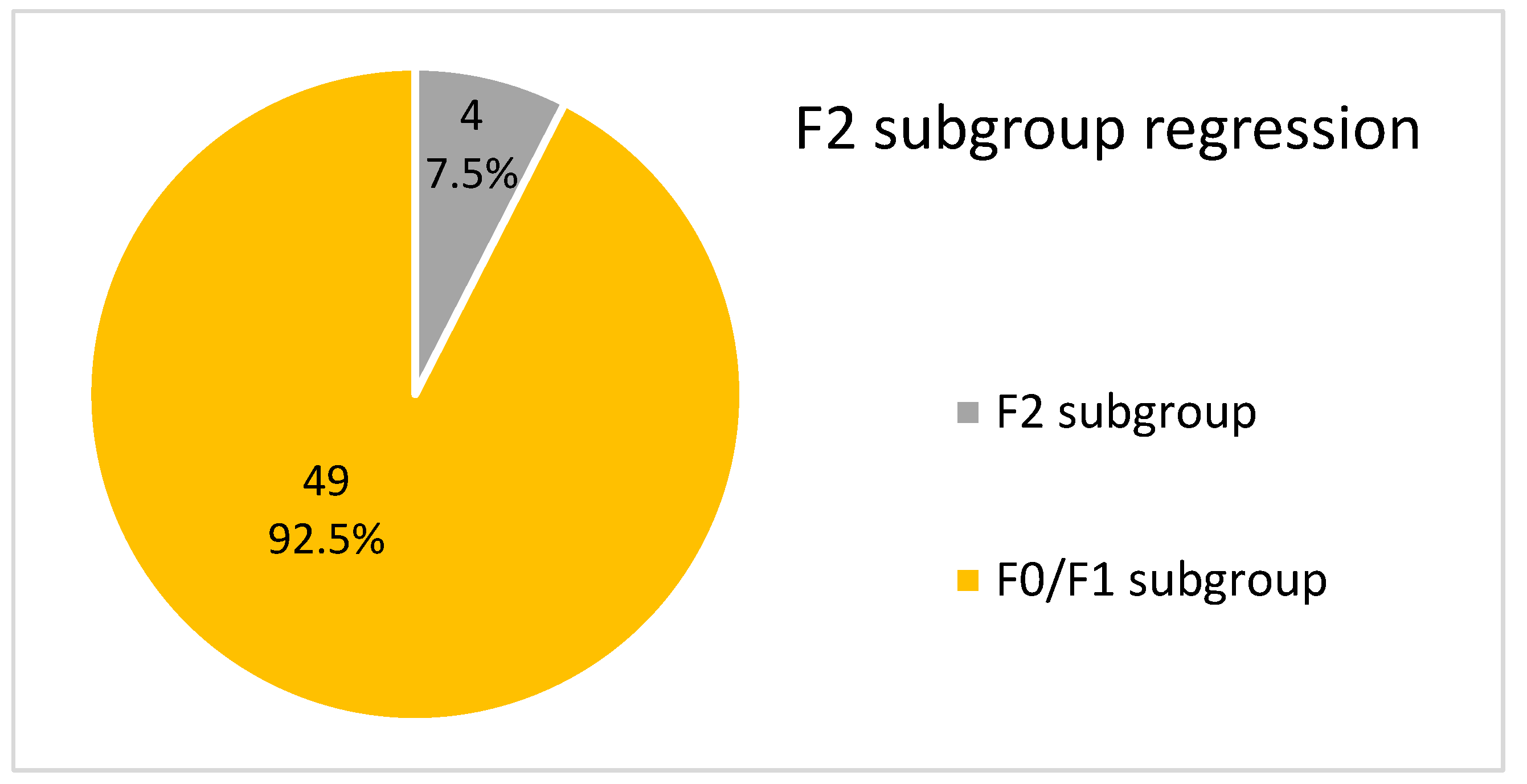
3.5.2. F3, F2 and F0/F1 Subgroups
3.6. Fibrotic Stage and Development of Hepatocellular Carcinoma
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021: Accountability for the Global Health Sector Strategies 2016–2021: Actions for Impact; WHO: Geneva, Switzerland, 2021.
- De Brito, R.J.V.C.; da Silva, L.F.; Santos, M.B.; de Moura, P.M.M.F.; de Souza, C.D.F.; do Carmo, R.F. A time series analysis of detection and mortality of hepatitis C in Brazil, 2008–2018. BMC Infect. Dis. 2022, 22, 81. [Google Scholar] [CrossRef] [PubMed]
- CDC. Hepatitis C. Centers for Disease Control and Prevention. 2021. Available online: https://www.cdc.gov/hepatitis/hcv/index.htm (accessed on 13 April 2023).
- ICTV. Table 1—Confirmed HCV Genotypes/Subtypes. International Committee on Taxonomy of Viruses. 2022. Available online: https://ictv.global/sg_wiki/flaviviridae/hepacivirus/table1 (accessed on 13 April 2023).
- Trickey, A.; Fraser, H.; Lim, A.G.; Peacock, A.; Colledge, S.; Walker, J.G.; Leung, J.; Grebely, J.; Larney, S.; Martin, N.K.; et al. The contribution of injection drug use to hepatitis C virus transmission globally, regionally, and at country level: A modelling study. Lancet Gastroenterol. Hepatol. 2019, 4, 435–444. [Google Scholar] [CrossRef] [PubMed]
- AASLD/IDSA HCV Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C. Clin. Liver Dis. 2018, 12, 117. [CrossRef]
- Westbrook, R.H.; Dusheiko, G. Natural history of hepatitis C. J. Hepatol. 2014, 61 (Suppl. 1), S58–S68. [Google Scholar] [CrossRef]
- Migdal, A.L.; Jagannathan, R.; Qayed, E.; Cusi, K.; McCoy, R.G.; Pasquel, F.J.; Miller, L.S. Association of Obesity, Diabetes, and Alcohol Use with Liver Fibrosis Among US Adults with Hepatitis C Virus Infection. JAMA Netw. Open 2022, 5, e2142282. [Google Scholar] [CrossRef]
- Bang, C.S.; Song, I.H. Impact of antiviral therapy on hepatocellular carcinoma and mortality in patients with chronic hepatitis C: Systematic review and meta-analysis. BMC Gastroenterol. 2017, 17, 46. [Google Scholar] [CrossRef]
- Calvaruso, V.; Cabibbo, G.; Cacciola, I.; Petta, S.; Madonia, S.; Bellia, A.; Tinè, F.; Distefano, M.; Licata, A.; Giannitrapani, L.; et al. Incidence of Hepatocellular Carcinoma in Patients with HCV-Associated Cirrhosis Treated with Direct-Acting Antiviral Agents. Gastroenterology 2018, 155, 411–421.e4. [Google Scholar] [CrossRef]
- Van der Meer, A.J.; Feld, J.J.; Hofer, H.; Almasio, P.L.; Calvaruso, V.; Fernández-Rodríguez, C.M.; Aleman, S.; Ganne-Carrié, N.; D’Ambrosio, R.; Pol, S.; et al. Risk of cirrhosis-related complications in patients with advanced fibrosis following hepatitis C virus eradication. J. Hepatol. 2017, 66, 485–493. [Google Scholar] [CrossRef]
- Mauro, E.; Crespo, G.; Montironi, C.; Londoño, M.C.; Hernández-Gea, V.; Ruiz, P.; Sastre, L.; Lombardo, J.; Mariño, Z.; Díaz, A.; et al. Portal pressure and liver stiffness measurements in the prediction of fibrosis regression after sustained virological response in recurrent hepatitis C. Hepatology 2018, 67, 1683–1694. [Google Scholar] [CrossRef]
- Malin, J.J.; Boesecke, C.; Schwarze-Zander, C.; Wasmuth, J.C.; Schlabe, S.; Trebicka, J.; Spengler, U.; Llibre, J.M.; Jou, T.; Vasylyev, M.; et al. Liver stiffness regression after successful Hepatitis C treatment is independent of HIV coinfection. HIV Med. 2019, 20, 230–236. [Google Scholar] [CrossRef]
- Yuri, Y.; Nishikawa, H.; Enomoto, H.; Yoh, K.; Iwata, Y.; Sakai, Y.; Kishino, K.; Ikeda, N.; Takashima, T.; Aizawa, N.; et al. Impact of Sustained Virological Response for Gastroesophageal Varices in Hepatitis-C-Virus-Related Liver Cirrhosis. J. Clin. Med. 2019, 9, 95. [Google Scholar] [CrossRef] [PubMed]
- Smith-Palmer, J.; Cerri, K.; Valentine, W. Achieving sustained virologic response in hepatitis C: A systematic review of the clinical, economic and quality of life benefits. BMC Infect. Dis. 2015, 15, 19. [Google Scholar] [CrossRef] [PubMed]
- Chevaliez, S.; Asselah, T. Mechanisms of non-response to antiviral treatment in chronic hepatitis C. Clin. Res. Hepatol. Gastroenterol. 2011, 35 (Suppl. 1), S31–S41. [Google Scholar] [CrossRef] [PubMed]
- Backus, L.I.; Belperio, P.S.; Shahoumian, T.A.; Mole, L.A. Direct-acting antiviral sustained virologic response: Impact on mortality in patients without advanced liver disease. Hepatology 2018, 68, 827–838. [Google Scholar] [CrossRef] [PubMed]
- Kalidindi, Y.; Jung, J.; Feldman, R.; Riley, T., 3rd. Association of Direct-Acting Antiviral Treatment with Mortality Among Medicare Beneficiaries with Hepatitis C. JAMA Netw. Open 2020, 3, e2011055. [Google Scholar] [CrossRef]
- Zoratti, M.J.; Siddiqua, A.; Morassut, R.E.; Zeraatkar, D.; Chou, R.; van Holten, J.; Xie, F.; Druyts, E. Pangenotypic direct acting antivirals for the treatment of chronic hepatitis C virus infection: A systematic literature review and meta-analysis. EClinicalMedicine 2020, 18, 100237. [Google Scholar] [CrossRef]
- Mar, J.; Ibarrondo, O.; Martínez-Baz, I.; Juanbeltz, R.; San Miguel, R.; Casado, I.; Arrospide, A.; Castilla, J. Economic evaluation of a population strategy for the treatment of chronic hepatitis C with direct-acting antivirals. Rev. Esp. Enferm. Dig. 2018, 110, 621–628. [Google Scholar] [CrossRef]
- EASL. Recommendations on Treatment of Hepatitis C 2018. J. Hepatol. 2018, 69, 461–511. [Google Scholar] [CrossRef]
- Keelan, C.G.; Sanabria, D. The liver biopsy in viral hepatitis C. Puerto Rico Health Sci. J. 2004, 23 (Suppl. 2), 29–34. [Google Scholar] [PubMed]
- Florea, M.; Serban, T.; Tirpe, G.R.; Tirpe, A.; Lupsor-Platon, M. Noninvasive Assessment of Hepatitis C Virus Infected Patients Using Vibration-Controlled Transient Elastography. J. Clin. Med. 2021, 10, 2575. [Google Scholar] [CrossRef]
- Afdhal, N.H.; Bacon, B.R.; Patel, K.; Lawitz, E.J.; Gordon, S.C.; Nelson, D.R.; Challies, T.L.; Nasser, I.; Garg, J.; Wei, L.J.; et al. Accuracy of fibroscan, compared with histology, in analysis of liver fibrosis in patients with hepatitis B or C: A United States multicenter study. Clin. Gastroenterol. Hepatol. 2015, 13, 772–779.e1–3. [Google Scholar] [CrossRef] [PubMed]
- Calleja, J.L.; Macias, J.; Forns, X.; Garcia, F.; Berenguer, M.; Garcia Deltoro, M.; Buti, M.; Granados, R.; Carrion, J.A.; Morano, L.; et al. Guidelines on treatment of hepatitis C virus infection. Spanish Association for the Study of the Liver (AEEH). Gastroenterol. Hepatol. 2018, 41, 597–608, (In English & Spanish). [Google Scholar] [CrossRef] [PubMed]
- Bedossa, P.; Poynard, T. An algorithm for the grading of activity in chronic hepatitis C. Hepatology 1996, 24, 289–293. [Google Scholar] [CrossRef]
- Fernandes, F.F.; Piedade, J.; Guimaraes, L.; Nunes, E.P.; Chaves, U.; Goldenzon, R.V.; Cardoso, S.W.; Duarte, J.; Grinsztejn, B.; Veloso, V.G.; et al. Effectiveness of direct-acting agents for hepatitis C and liver stiffness changing after sustained virological response. J. Gastroenterol. Hepatol. 2019, 34, 2187–2195. [Google Scholar] [CrossRef]
- Toyoda, H.; Tada, T.; Yasuda, S.; Mizuno, K.; Ito, T.; Kumada, T. Dynamic Evaluation of Liver Fibrosis to Assess the Risk of Hepatocellular Carcinoma in Patients with Chronic Hepatitis C Who Achieved Sustained Virologic Response. Clin. Infect. Dis. 2020, 70, 1208–1214. [Google Scholar] [CrossRef]
- Horsley-Silva, J.L.; Vargas, H.E. New Therapies for Hepatitis C Virus Infection. Gastroenterol. Hepatol. 2017, 13, 22–31. [Google Scholar] [PubMed]
- Badia Aranda, E.; Fernández Marcos, C.; Puebla Maestu, A.; Gozalo Marín, V.; Vinuesa Campo, R.; Calvo Simal, S.; Gómez Camarero, J. Evolution of patients with chronic hepatitis C infection with advanced fibrosis or cirrhosis cured with direct-acting antivirals. Long-term follow-up. Gastroenterol. Hepatol. 2022, 45, 767–779. [Google Scholar] [CrossRef]
- Probst, A.; Dang, T.; Bochud, M.; Egger, M.; Negro, F.; Bochud, P.Y. Role of hepatitis C virus genotype 3 in liver fibrosis progression—A systematic review and meta-analysis. J. Viral Hepat. 2011, 18, 745–759. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| METAVIR Scale | Liver Fibrosis (kPa) |
|---|---|
| F0/F1 subgroup | ≤7.4 |
| F2 subgroup | 7.5–9.4 |
| F3 subgroup | 9.5–12.4 |
| F4 subgroup | ≥12.5 |
| Parameter | HCV Infected (n = 248) | p = |
|---|---|---|
| Males/females, n (%) | 175 (70.6)/73 (29.4) | 0.011 |
| Age (years) mean (SD) | 54.6 (10.2) | 0.000 |
| High active alcohol use, n (%) | 24 (9.7) | 0.007 |
| Mild liver steatosis, n (%) | 33 (13.3) | 0.087 |
| Metabolic syndrome, n (%) | 24 (9.7) | 0.042 |
| HIV, n (%) | 30 (12.1) | 0.065 |
| NAÏVE, n (%) | 159 (64.1) | 0.029 |
| PTP IFN, n (%) | 8 (3.2) | |
| PRP DAA, n (%) | 11 (4.5) | |
| NRP DAA, n (%) | 6 (2.4) | |
| PRP IFN, n (%) | 28 (11.3) | |
| NRP IFN, n (%) | 36 (14.5) | |
| Subtype 1a | 80 (32.2) | 0.018 |
| Subtype 1b | 108 (43.6) | |
| GT 2 | 3 (1.3) | |
| GT 3 | 36 (14.5) | |
| GT 4 | 21 (8.4) | |
| F4 subgroup, n (%) | 77 (31.0) | 0.667 |
| F3 subgroup, n (%) | 55 (22.2) | |
| F2 subgroup, n (%) | 53 (21.4) | |
| F0/F1 subgroup, n (%) | 63 (25.4) |
| F4 Subgroup (n = 77) | F3 Subgroup (n = 55) | F2 Subgroup (n = 53) | F0/F1 Subgroup (n = 63) | |
|---|---|---|---|---|
| At least one HCV complication | 27 (35.1%) | 5 (9.1%) | 6 (11.3%) | 2 (3.2%) |
| Death from HCV complications | 4 (5.2%) | 1 (1.8%) | 0 (0%) | 0 (0%) |
| Hepatocellular carcinoma | 12 (15.6%) | 1 (1.8%) | 0 (0%) | 0 (0%) |
| Ascites | 9 (11.7%) | 3 (5.4%) | 2 (3.8%) | 0 (0%) |
| Varicose veins | 17 (22.1%) | 1 (1.8%) | 1 (1.9%) | 0 (0%) |
| Encephalopathy | 4 (5.2%) | 1 (1.8%) | 0 (0%) | 0 (0%) |
| Kidney failure | 5 (6.5%) | 0 (0%) | 4 (7.6%) | 2 (3.2%) |
| Liver transplantation requirement | 6 (7.8%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Measurements | F4 Subgroup | F3 Subgroup | F2 Subgroup | F0/F1 Subgroup |
|---|---|---|---|---|
| 1st | 77 (31.0%) | 55 (22.2%) | 53 (21.4%) | 63 (25.4%) |
| 2nd | 44 (17.8%) | 30 (12.1%) | 41 (16.5%) | 133 (53.6%) |
| 3rd | 38 (15.3%) | 29 (11.7%) | 26 (10.5%) | 155 (62.5%) |
| 4th | 39 (15.7%) | 25 (10.1%) | 34 (13.7%) | 150 (60.5%) |
| 5th | 33 (13.3%) | 25 (10.1%) | 26 (10.5%) | 164 (66.1%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Ros, A.; Morán, S.; Núñez, V.; García-Ros, G.; Ruiz, G.; García-Solano, J. Impact of Direct-Acting Antiviral Therapy on Liver Fibrosis Regression among People with Chronic HCV Infection: Results from a Real-Life Cohort in Patients Who Achieved Sustained Virological Response. Medicina 2023, 59, 814. https://doi.org/10.3390/medicina59040814
García-Ros A, Morán S, Núñez V, García-Ros G, Ruiz G, García-Solano J. Impact of Direct-Acting Antiviral Therapy on Liver Fibrosis Regression among People with Chronic HCV Infection: Results from a Real-Life Cohort in Patients Who Achieved Sustained Virological Response. Medicina. 2023; 59(4):814. https://doi.org/10.3390/medicina59040814
Chicago/Turabian StyleGarcía-Ros, Alejandro, Senador Morán, Virginia Núñez, Gonzalo García-Ros, Guadalupe Ruiz, and José García-Solano. 2023. "Impact of Direct-Acting Antiviral Therapy on Liver Fibrosis Regression among People with Chronic HCV Infection: Results from a Real-Life Cohort in Patients Who Achieved Sustained Virological Response" Medicina 59, no. 4: 814. https://doi.org/10.3390/medicina59040814
APA StyleGarcía-Ros, A., Morán, S., Núñez, V., García-Ros, G., Ruiz, G., & García-Solano, J. (2023). Impact of Direct-Acting Antiviral Therapy on Liver Fibrosis Regression among People with Chronic HCV Infection: Results from a Real-Life Cohort in Patients Who Achieved Sustained Virological Response. Medicina, 59(4), 814. https://doi.org/10.3390/medicina59040814