

Different Chemotherapy Regimens and Pathologic Complete Response in Triple-Negative Breast Cancer: An Updated Network Meta-Analysis of Phase 3 Trials

 ,
,  , ,
, , 

Abstract
:1. Introduction
2. Material and Methods
3. Results
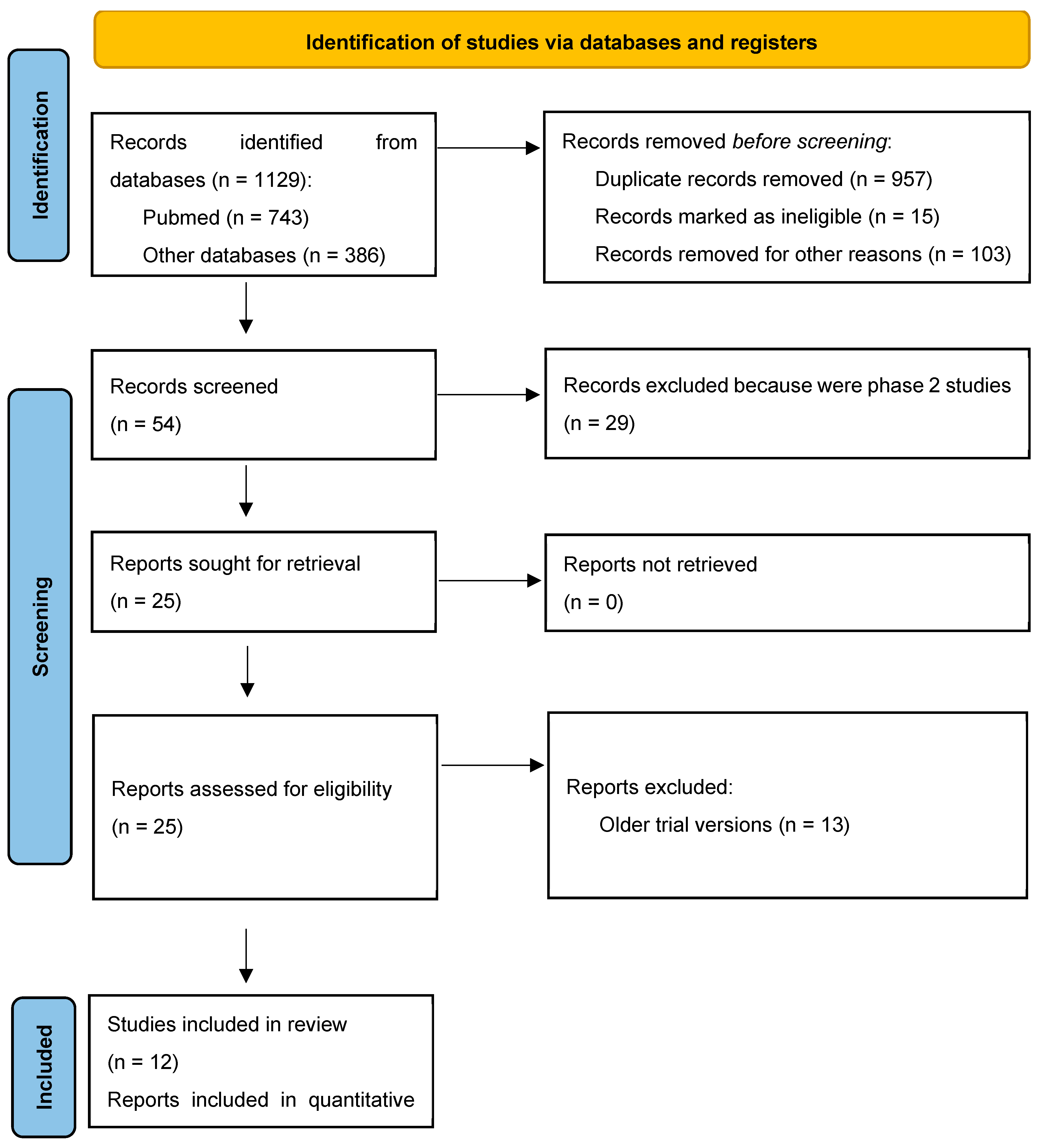
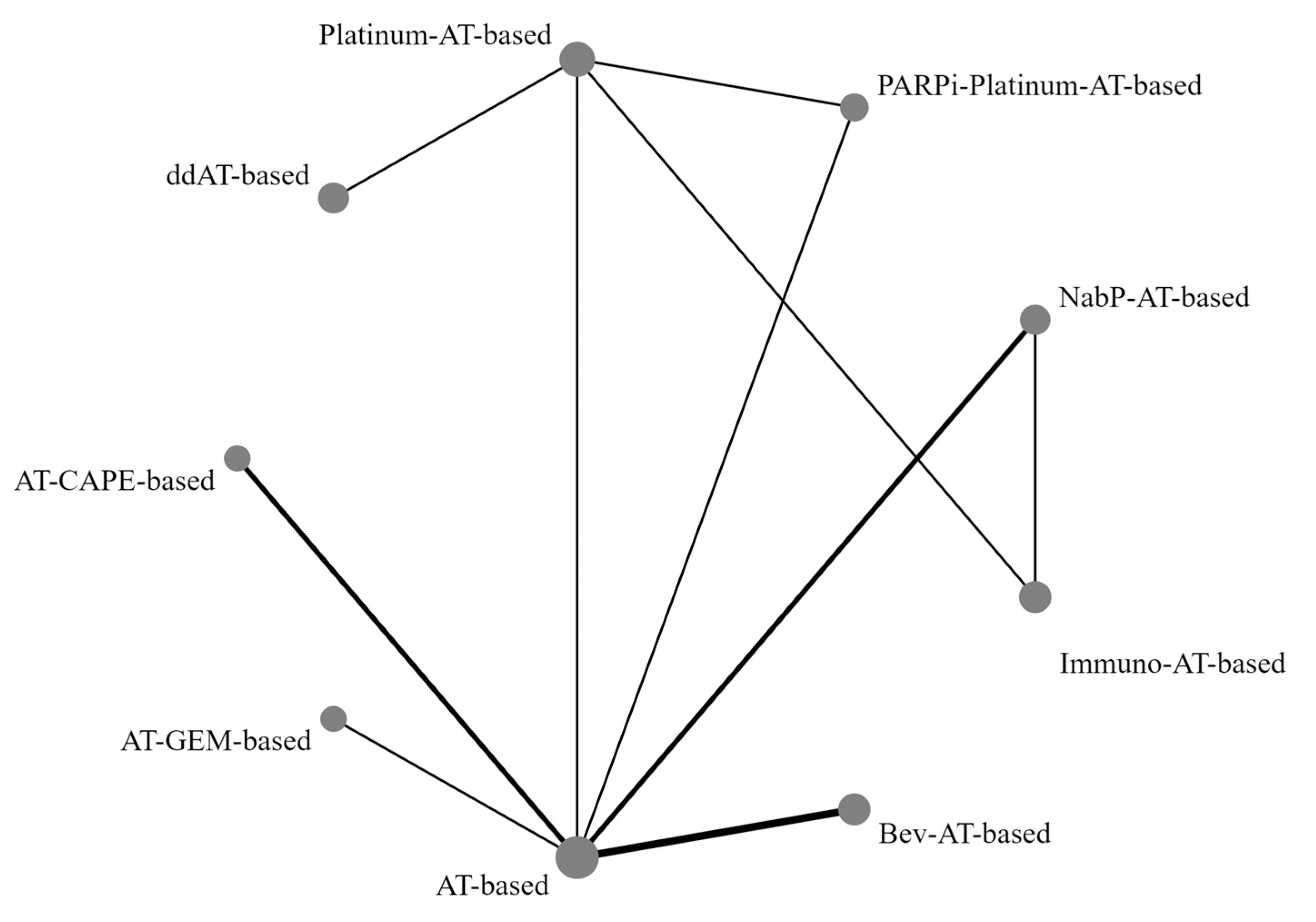
3.1. Study Characteristics
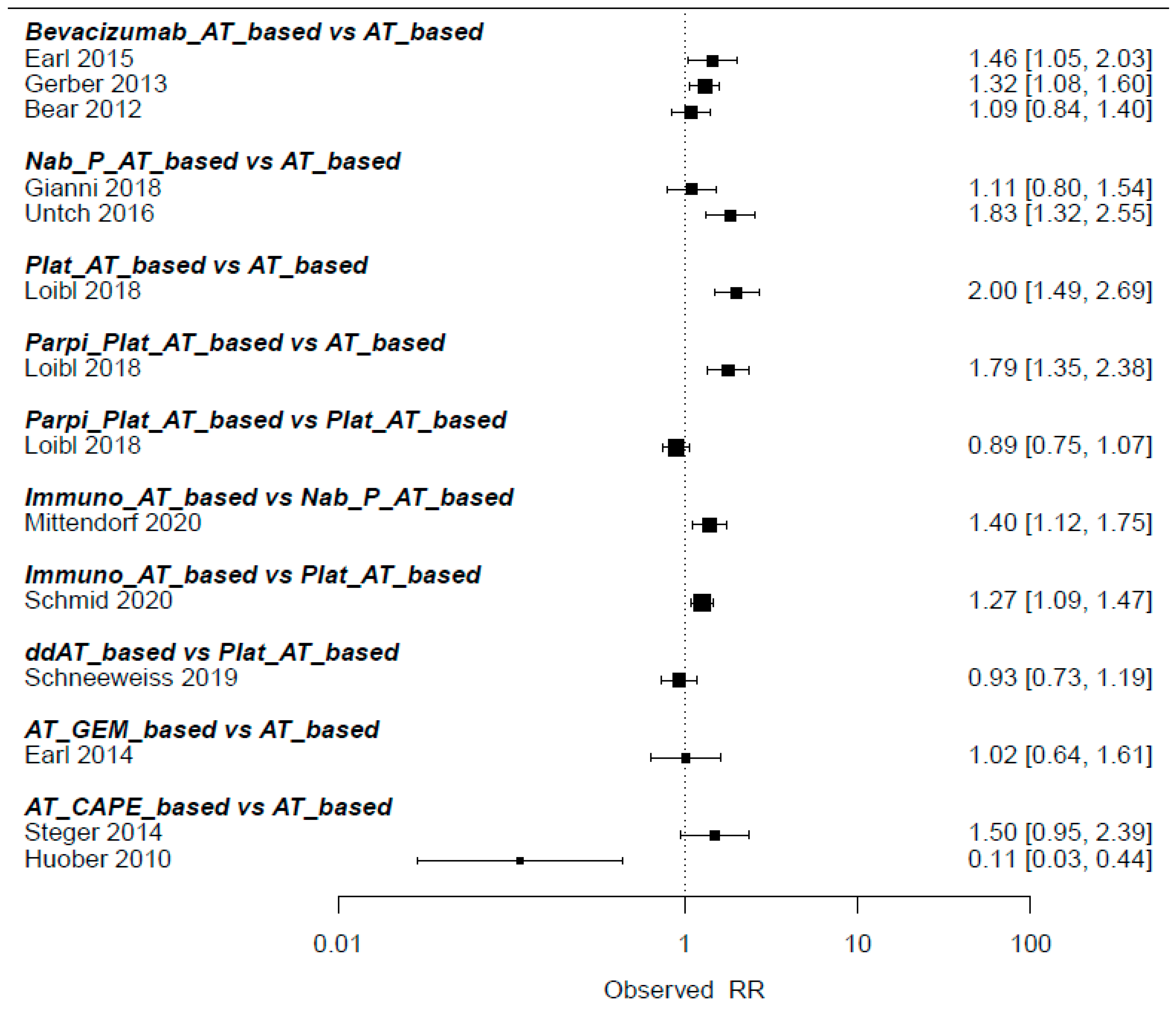
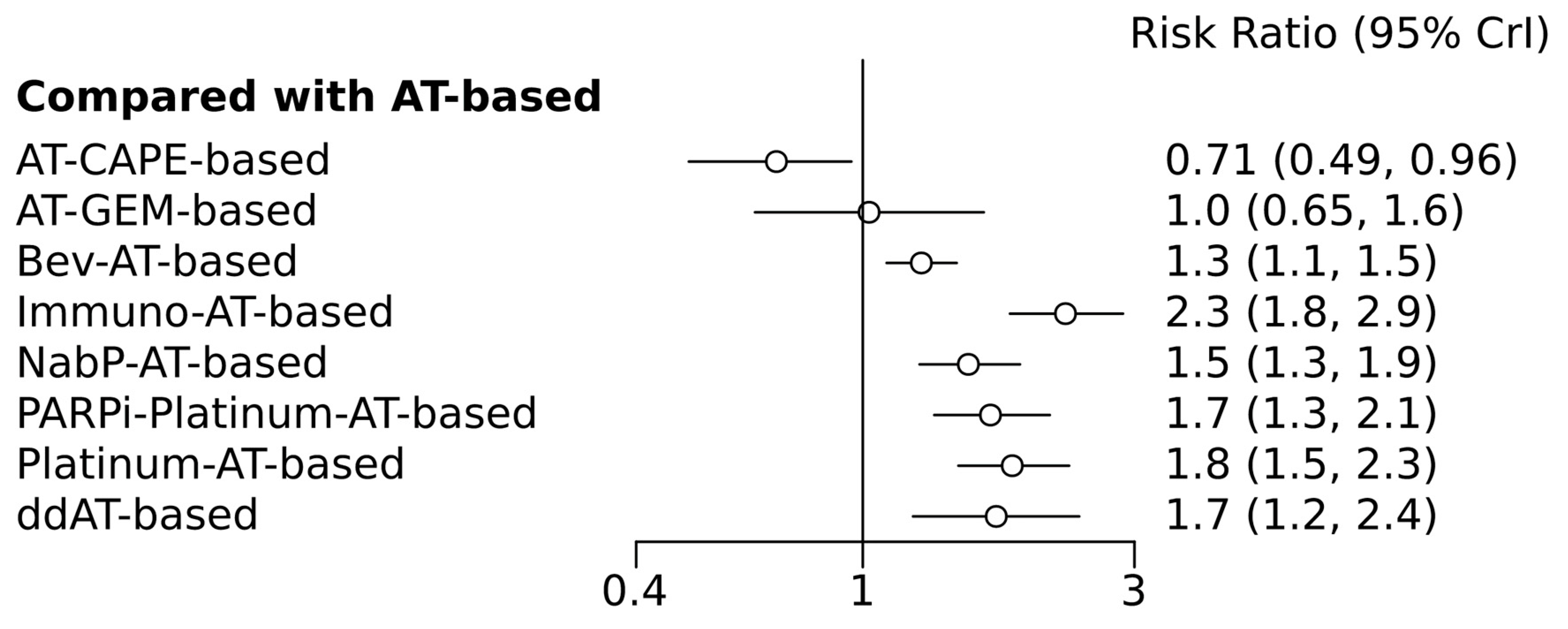
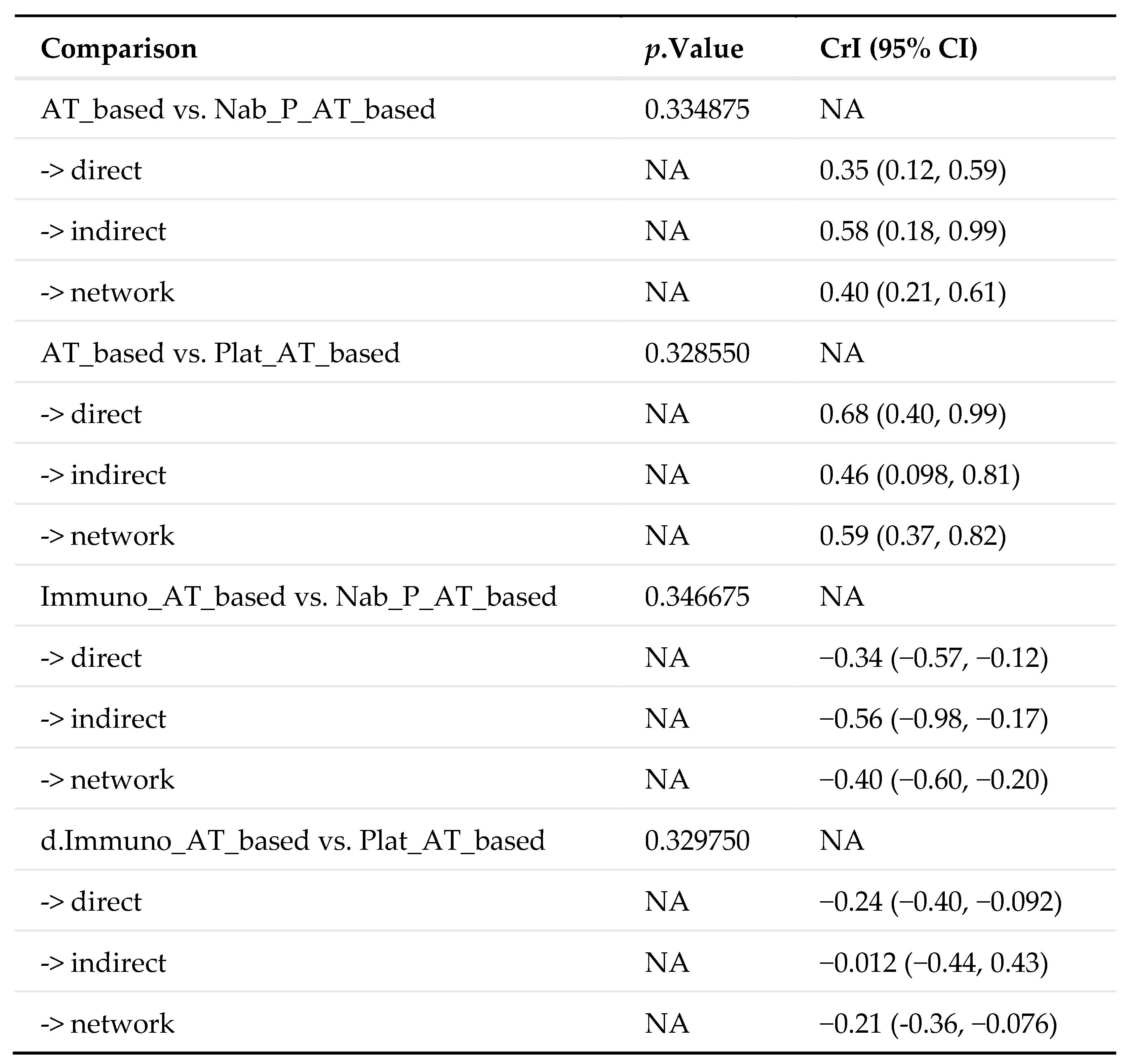
3.2. Pathologic Complete Response
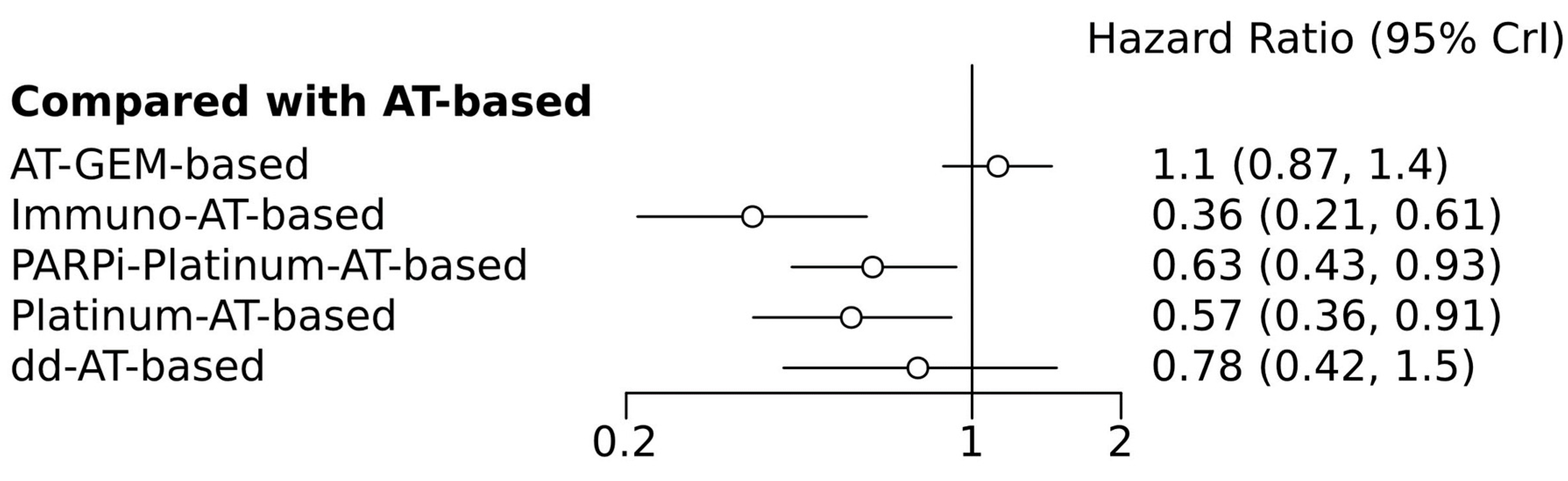
3.3. Disease-Free Survival
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Asselain, B.; Barlow, W.; Bartlett, J.; Bergh, J.; Bergsten-Nordström, E.; Bliss, J.; Boccardo, F.; Boddington, C.; Bogaerts, J.; Bonadonna, G.; et al. Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early breast cancer: Meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. 2018, 19, 27–39. [Google Scholar] [CrossRef]
- Korde, L.A.; Somerfield, M.R.; Carey, L.A.; Crews, J.R.; Denduluri, N.; Hwang, E.S.; Khan, S.A.; Loibl, S.; Morris, E.A.; Perez, A.; et al. Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer: ASCO Guideline. J. Clin. Oncol. 2021, 39, 1485–1505. [Google Scholar] [CrossRef]
- Sikov, W.M.; Polley, M.-Y.; Twohy, E.; Perou, C.M.; Singh, B.; Berry, D.A.; Tolaney, S.M.; Somlo, G.; Port, E.R.; Ma, C.X.; et al. CALGB (Alliance) 40603: Long-term outcomes (LTOs) after neoadjuvant chemotherapy (NACT) +/− carboplatin (Cb) and bevacizumab (Bev) in triple-negative breast cancer (TNBC). J. Clin. Oncol. 2019, 37, 591. [Google Scholar] [CrossRef]
- Untch, M.; Schneeweiss, A.; Salat, C.; Rezai, M.; Zahm, D.-M.; Klare, P.; Blohmer, J.-U.; Tesch, H.; Khandan, F.; Fasching, P.; et al. Long-term survival analysis of the randomized phase II trial investigating the addition of carboplatin to neoadjuvant therapy for triple-negative (TNBC) and HER2-positive early breast cancer (GeparSixto). Ann. Oncol. 2017, 28, v49. [Google Scholar] [CrossRef]
- Schmid, P.; Cortes, J.; Pusztai, L.; McArthur, H.; Kümmel, S.; Bergh, J.; Denkert, C.; Park, Y.H.; Hui, R.; Harbeck, N.; et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N. Engl. J. Med. 2020, 382, 810–821. [Google Scholar] [CrossRef] [PubMed]
- Bayesian Evidence Synthesis. Available online: https://gemtc.drugis.org (accessed on 21 December 2023).
- Steger, G.G.; Greil, R.; Lang, A.; Rudas, M.; Fitzal, F.; Mlineritsch, B.; Hartmann, B.L.; Bartsch, R.; Melbinger, E.; Hubalek, M.; et al. Epirubicin and docetaxel with or without capecitabine as neoadjuvant treatment for early breast cancer: Final results of a randomized phase III study (ABCSG-24). Ann. Oncol. 2014, 25, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Bear, H.D.; Tang, G.; Rastogi, P.; Geyer, C.E., Jr.; Robidoux, A.; Atkins, J.N.; Baez-Diaz, L.; Brufsky, A.M.; Mehta, R.S.; Fehrenbacher, L.; et al. Bevacizumab Added to Neoadjuvant Chemotherapy for Breast Cancer. N. Engl. J. Med. 2012, 366, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Mittendorf, E.A.; Zhang, H.; Barrios, C.H.; Saji, S.; Jung, K.H.; Hegg, R.; Koehler, A.; Sohn, J.; Iwata, H.; Telli, M.L.; et al. Neoadjuvant atezolizumab in combination with sequential nab-paclitaxel and anthracycline-based chemotherapy versus placebo and chemotherapy in patients with early-stage triple-negative breast cancer (IMpassion031): A randomised, double-blind, phase 3 trial. Lancet 2020, 396, 1090–1100. [Google Scholar] [CrossRef] [PubMed]
- Earl, H.M.; Vallier, A.-L.; Hiller, L.; Fenwick, N.; Young, J.; Iddawela, M.; Abraham, J.; Hughes-Davies, L.; Gounaris, I.; McAdam, K.; et al. Effects of the addition of gemcitabine, and paclitaxel-first sequencing, in neoadjuvant sequential epirubicin, cyclophosphamide, and paclitaxel for women with high-risk early breast cancer (Neo-tAnGo): An open-label, 2 × 2 factorial randomised phase 3 trial. Lancet Oncol. 2014, 15, 201–212. [Google Scholar] [CrossRef] [PubMed]
- Untch, M.; Jackisch, C.; Schneeweiss, A.; Conrad, B.; Aktas, B.; Denkert, C.; Eidtmann, H.; Wiebringhaus, H.; Kümmel, S.; Hilfrich, J.; et al. Nab-paclitaxel versus solvent-based paclitaxel in neoadjuvant chemotherapy for early breast cancer (GeparSepto—GBG 69): A randomised, phase 3 trial. Lancet Oncol. 2016, 17, 345–356. [Google Scholar] [CrossRef] [PubMed]
- Earl, H.M.; Hiller, L.; Dunn, J.A.; Blenkinsop, C.; Grybowicz, L.; Vallier, A.-L.; Abraham, J.; Thomas, J.; Provenzano, E.; Hughes-Davies, L.; et al. Efficacy of neoadjuvant bevacizumab added to docetaxel followed by fluorouracil, epirubicin, and cyclophosphamide, for women with HER2-negative early breast cancer (ARTemis): An open-label, randomised, phase 3 trial. Lancet Oncol. 2015, 16, 656–666. [Google Scholar] [CrossRef] [PubMed]
- Schneeweiss, A.; Michel, L.L.; Möbus, V.; Tesch, H.; Klare, P.; Hahnen, E.; Denkert, C.; Kast, K.; Pohl-Rescigno, E.; Hanusch, C.; et al. Survival analysis of the randomised phase III GeparOcto trial comparing neoadjuvant chemotherapy of intense dose-dense epirubicin, paclitaxel, cyclophosphamide versus weekly paclitaxel, liposomal doxorubicin (plus carboplatin in triple-negative breast cancer) for patients with high-risk early breast cancer. Eur. J. Cancer 2022, 160, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Gerber, B.; Loibl, S.; Eidtmann, H.; Rezai, M.; Fasching, P.A.; Tesch, H.; Eggemann, H.; Schrader, I.; Kittel, K.; Hanusch, C.; et al. Neoadjuvant bevacizumab and anthracycline–taxane-based chemotherapy in 678 triple-negative primary breast cancers; results from the geparquinto study (GBG 44). Ann. Oncol. 2013, 24, 2978–2984. [Google Scholar] [CrossRef] [PubMed]
- Schneeweiss, A.; Möbus, V.; Tesch, H.; Hanusch, C.; Denkert, C.; Lübbe, K.; Huober, J.; Klare, P.; Kümmel, S.; Untch, M.; et al. Intense dose-dense epirubicin, paclitaxel, cyclophosphamide versus weekly paclitaxel, liposomal doxorubicin (plus carboplatin in triple-negative breast cancer) for neoadjuvant treatment of high-risk early breast cancer (GeparOcto—GBG 84): A randomised phase III trial. Eur. J. Cancer 2019, 106, 181–192. [Google Scholar] [CrossRef]
- Gianni, L.; Mansutti, M.; Anton, A.; Calvo, L.; Bisagni, G.; Bermejo, B.; Semiglazov, V.; Thill, M.; Chacon, J.I.; Chan, A.; et al. Comparing neoadjuvant nab-paclitaxel vs paclitaxel both followed by anthracycline regimens in women with ERBB2/HER2-negative breast cancer—the evaluating treatment with neoadjuvant abraxane (ETNA) trial: A randomized phase 3 clinical trial. JAMA Oncol. 2018, 4, 302–308. [Google Scholar] [CrossRef]
- Loibl, S.; O’Shaughnessy, J.; Untch, M.; Sikov, W.M.; Rugo, H.S.; McKee, M.D.; Huober, J.; Golshan, M.; von Minckwitz, G.; Maag, D.; et al. Addition of the PARP inhibitor veliparib plus carboplatin or carboplatin alone to standard neoadjuvant chemotherapy in triple-negative breast cancer (BrighTNess): A randomised, phase 3 trial. Lancet Oncol. 2018, 19, 497–509. [Google Scholar] [CrossRef]
- Huober, J.; von Minckwitz, G.; Denkert, C.; Tesch, H.; Weiss, E.; Zahm, D.M.; Belau, A.; Khandan, F.; Hauschild, M.; Thomssen, C.; et al. Effect of neoadjuvant anthracycline-taxane-based chemotherapy in different biological breast cancer phenotypes: Overall results from the GeparTrio study. Breast Cancer Res. Treat. 2010, 124, 133–140. [Google Scholar] [CrossRef]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Diéras, V.; Hegg, R.; Im, S.-A.; Shaw Wright, G.; et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N. Engl. J. Med. 2018, 379, 2108–2121. [Google Scholar] [CrossRef]
- Lin, Y.-Y.; Gao, H.-F.; Yang, X.; Zhu, T.; Zheng, X.-X.; Ji, F.; Zhang, L.-L.; Yang, C.-Q.; Yang, M.; Li, J.-Q.; et al. Neoadjuvant therapy in triple-negative breast cancer: A systematic review and network meta-analysis. Breast 2022, 66, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Chen, X.; Li, H.; Li, Y. Immune checkpoint inhibitors in first-line therapies of metastatic or early triple-negative breast cancer: A systematic review and network meta-analysis. Front. Endocrinol. 2023, 14, 1137464. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.; Cescon, D.W.; Rugo, H.S.; Nowecki, Z.; Im, S.-A.; Yusof, M.M.; Gallardo, C.; Lipatov, O.; Barrios, C.H.; Holgado, E.; et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): A randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet 2020, 396, 1817–1828. [Google Scholar] [CrossRef] [PubMed]
- Elmakaty, I.; Abdo, R.; Elsabagh, A.; Elsayed, A.; Malki, M.I. Comparative efficacy and safety of PD-1/PD-L1 inhibitors in triple negative breast cancer: A systematic review and network meta-analysis of randomized controlled trials. Cancer Cell Int. 2023, 23, 90. [Google Scholar] [CrossRef] [PubMed]
- Loibl, S.; Schneeweiss, A.; Huober, J.; Braun, M.; Rey, J.; Blohmer, J.-U.; Furlanetto, J.; Zahm, D.-M.; Hanusch, C.; Thomalla, J.; et al. Neoadjuvant durvalumab improves survival in early triple-negative breast cancer independent of pathological complete response. Ann. Oncol. 2022, 33, 1149–1158. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year | Type of Study | N° pts/Median Follow Up (Months) | Stage | Definition of TN Status | Treatment Arms (ctr vs. exp) | pCR % (ctr vs. exp) | Risk of Bias |
|---|---|---|---|---|---|---|---|
| Bear/2012 | Prospective RCT | 244/- | I–III | NA | D × 4 → AC × 4 DX × 4 → AC × 4 DG × 4 → AC × 4 ±Bevacizumab | 47.1 vs. 51.2 | Low |
| Earl/2014 | Prospective RCT | 157/47 | I–III | ER/PR NA; HER2 = -, 1+, 2+/ISH- | EC × 4 → PAC × 4 PAC × 4 → EC × 4 EC × 4 → TG × 4 TG × 4 → EC × 4 | 31.5 vs. 32.1 | Low |
| Earl/2015 | Prospective RCT | 241/- | I–III | ER/PR score = 0–2/8; HER2 = -, 1+, 2+/ISH- | D × 3 → FEC × 3 ±Bevacizumab | 31.1 vs. 45.3 | Low |
| Gerber/2013 | Prospective RCT | 663/- | I–III | ER/PR < 10%; HER2 = -, 1+, 2+/ISH- | EC × 4 → D × 4 ±Bevacizumab | 32.9 vs. 43.3 | Low |
| Gianni/2018 | Prospective RCT | 219/- | I–III | ER/PR < 1%; HER2 = -, 1+, 2+/ISH- | PAC × 4 → A regimen nabPAC × 4 → A regimen | 37.2 vs. 41.2 | Low |
| Huober/2010 | Prospective RCT | 89/- | I–III | ER/PR < 10%; HER2 = -, 1+, 2+/ISH- | TAC × 2 → TAC × 4-6 TAC × 2 → NX × 4 | 43.3 vs. 4.8 | Moderate |
| Loibl/2018 and Geyer/2022 | Prospective RCT | 634/- | I–III | ER/PR < 1%; HER2 = -, 1+, 2+/ISH- | PAC + Carbo × 4 + Veliparib → AC × 4 PAC + Carbo × 4 + placebo → AC × 4 PAC + placebo → AC × 4 | 58.8 vs. 52.5 | Low |
| Mittendorf/2020 | Prospective RCT | 333/20.2 | II–III | NA | nabPAC × 12w → AC q14 × 4 ±Atezolizumab | 41.0 vs. 57.5 | Low |
| Schmid/2020 and Schmid/2022 | Prospective RCT | 602/15.5 | II–III | ASCO guidelines | PAC + Carbo × 4 ± Pembrolizumab → AC/EC × 4 ± Pembrolizumab | 51.2 vs. 64.8 | Low |
| Schneeweiss/2019 and Schneeweiss/2022 | Prospective | 403/- | I–III | ER/PR < 1%; HER2 = -, 1+, 2+/ISH- | iddEPC PAC + M + Carbo × 18w | 20.6 vs. 22.1 | Moderate |
| Steger/2014 | Prospective RCT | 127/- | I–III * | ER/PR < 10%; HER2 = -, 1+, 2+/ISH- | ED × 6 EDX × 6 | 30.1 vs. 45.3 | Moderate |
| Untch/2016 | Prospective RCT | 276/- | I–III | ER/PR < 1%; HER2 = -, 1+, 2+/ISH- | nabPAC × 4 → EC PAC × 4 → EC | 26.2 vs. 48.2 | Low |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrelli, F.; Tomasello, G.; Parati, M.C.; Ghidini, A.; Ghidini, M.; Borgonovo, K.; Cabiddu, M.; Ghilardi, M.; Reduzzi, R.; Gambini, D.; et al. Different Chemotherapy Regimens and Pathologic Complete Response in Triple-Negative Breast Cancer: An Updated Network Meta-Analysis of Phase 3 Trials. Medicina 2024, 60, 341. https://doi.org/10.3390/medicina60020341
Petrelli F, Tomasello G, Parati MC, Ghidini A, Ghidini M, Borgonovo K, Cabiddu M, Ghilardi M, Reduzzi R, Gambini D, et al. Different Chemotherapy Regimens and Pathologic Complete Response in Triple-Negative Breast Cancer: An Updated Network Meta-Analysis of Phase 3 Trials. Medicina. 2024; 60(2):341. https://doi.org/10.3390/medicina60020341
Chicago/Turabian StylePetrelli, Fausto, Gianluca Tomasello, Maria Chiara Parati, Antonio Ghidini, Michele Ghidini, Karen Borgonovo, Mary Cabiddu, Mara Ghilardi, Roberto Reduzzi, Donatella Gambini, and et al. 2024. "Different Chemotherapy Regimens and Pathologic Complete Response in Triple-Negative Breast Cancer: An Updated Network Meta-Analysis of Phase 3 Trials" Medicina 60, no. 2: 341. https://doi.org/10.3390/medicina60020341
APA StylePetrelli, F., Tomasello, G., Parati, M. C., Ghidini, A., Ghidini, M., Borgonovo, K., Cabiddu, M., Ghilardi, M., Reduzzi, R., Gambini, D., Zaniboni, A., Faustinelli, G., & Garrone, O. (2024). Different Chemotherapy Regimens and Pathologic Complete Response in Triple-Negative Breast Cancer: An Updated Network Meta-Analysis of Phase 3 Trials. Medicina, 60(2), 341. https://doi.org/10.3390/medicina60020341