
Influence of the COVID-19 Outbreak in Vulnerable Patients (Pediatric Patients, Pregnant Women, and Elderly Patients) on an Emergency Medical Service System: A Pre- and Post-COVID-19 Pandemic Comparative Study Using the Population-Based ORION Registry

Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. The Emergency Medical Service (EMS) System in Japan
2.3. The ORION System
2.4. Data Collection and Quality Control
2.5. Availability of Data and Materials
2.6. Outcomes
2.7. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA-J. Am. Med. Assoc. 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Katayama, Y.; Kiyohara, K.; Kitamura, T.; Hayashida, S.; Shimazu, T. Influence of the COVID-19 pandemic on an emergency medical service system: A population-based, descriptive study in Osaka, Japan. Acute Med. Surg. 2020, 7, e534. [Google Scholar] [CrossRef]
- Ota, K.; Nishioka, D.; Katayama, Y.; Kitamura, T.; Masui, J.; Ota, K.; Nitta, M.; Matsuoka, T.; Takasu, A. Influence of the COVID-19 outbreak on transportation of pregnant women in an emergency medical service system: Population-based, ORION registry. Int. J. Gynecol. Obstet. 2022, 157, 366–374. [Google Scholar] [CrossRef]
- Ota, K.; Nishioka, D.; Katayama, Y.; Kitamura, T.; Masui, J.; Ota, K.; Nitta, M.; Matsuoka, T.; Takasu, A. Effect of the COVID-19 outbreak on emergency transport of children by an emergency medical service system: A population-based, ORION registry study. BMC Emerg. Med. 2022, 22, 206. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatr. 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- Ageta, K.; Naito, H.; Yorifuji, T.; Obara, T.; Nojima, T.; Yamada, T.; Tsukahara, K.; Yakushiji, H.; Nakao, A. Delay in Emergency Medical Service Transportation Responsiveness during the COVID-19 Pandemic in a Minimally Affected Region. Acta Med. Okayama. 2020, 74, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Aruga, Y. Emergency medical services for the elderly: Present fact and future challenge. Nihon Rinsho 2013, 71, 964–968. [Google Scholar] [PubMed]
- Salvi, F.; Morichi, V.; Grilli, A.; Giorgi, R.; De Tommaso, G.; Dessì-Fulgheri, P. The elderly in the emergency department: A critical review of problems and solutions. Intern. Emerg. Med. 2007, 2, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Shahid, Z.; Kalayanamitra, R.; McClafferty, B.; Kepko, D.; Ramgobin, D.; Patel, R.; Aggarwal, C.S.; Vunnam, R.; Sahu, N.; Bhatt, D.; et al. COVID-19 and Older Adults: What We Know. J. Am. Geriatr. Soc. 2020, 68, 926–929. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 2020, 81, e16–e25. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, J.; Katayama, Y.; Kitamura, T.; Sado, J.; Nakamura, R.; Kimura, N.; Misaki, H.; Yamao, S.; Nakao, S.; Nitta, M.; et al. Profile of the ORION (Osaka emergency information Research Intelligent Operation Network system) between 2015 and 2016 in Osaka, Japan: A population-based registry of emergency patients with both ambulance and in-hospital records. Acute Med. Surg. 2019, 6, 12–24. [Google Scholar] [CrossRef]
- Amyx, M.; Xiong, X.; Xie, Y.; Buekens, P. Racial/Ethnic Differences in Sleep Disorders and Reporting of Trouble Sleeping Among Women of Childbearing Age in the United States. Matern. Child. Health J. 2017, 21, 306–314. [Google Scholar] [CrossRef]
- WHO. International Statistical Classification of Diseases and Related Health Problems, 10th Revision ICD-10: Tabular List; World Health Organization: Geneva, Switzerland, 2016; Volume 1, pp. 332–345. Available online: http://www.who.int/classifications/icd/icdonlineversions/en/ (accessed on 5 August 2023).
- Difinition. 2017. Available online: https://www.jpn-geriat-soc.or.jp/proposal/pdf/definition_01.pdf (accessed on 5 August 2023).
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Petersen, I.; Sørensen, H.T.; von Elm, E.; Langan, S.M.; RECORD Working Committee. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) Statement. PLoS Med. 2015, 12, e1001885. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare of Japan Ambulance Service Planning Office of Fire and Service, Management Agency of Japan and Guidance of Medical Division, Health Policy Bureau, Ministry of Health L and, Disaster ASPO of F and, Service MA of J and G of M, Division HPB. A Report on the Acceptance of Emergency Patients by Medical Institutions. Volume 6. Available online: https://www.fdma.go.jp/disaster/coronavirus/items/coronavirus_kekka.pdf (accessed on 5 August 2023).
- The Fire and Disaster Management Agency. White Book on Emergency System in Japan. 2020. Available online: https://www.fdma.go.jp/publication/rescue/items/kkkg_r02_01_kyukyu.pdf (accessed on 5 August 2023).
- Holmes, J.L.; Brake, S.; Docherty, M.; Lilford, R.; Watson, S. Emergency ambulance services for heart attack and stroke during UK’s COVID-19 lockdown. Lancet 2020, 395, e93–e94. [Google Scholar] [CrossRef]
- Sutherland, K.; Chessman, J.; Zhao, J.; Sara, G.; Shetty, A.; Smith, S.; Went, A.; Dyson, S.; Levesque, J.F. Impact of COVID-19 on healthcare activity in NSW, Australia. Public Health Res. Pract. 2020, 30, e3042030. [Google Scholar] [CrossRef] [PubMed]
- Grunau, B.; Helmer, J.; Lee, S.; Acker, J.; Deakin, J.; Armour, R.; Tallon, J.; Jenneson, S.; Christenson, J.; Scheuermeyer, F.X. Decrease in emergency medical services utilization during early stages of the COVID-19 pandemic in British Columbia. Can. J. Emerg. Med. 2021, 23, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Ota, K.; Nishioka, D.; Katayama, Y.; Kitamura, T.; Masui, J.; Ota, K.; Nitta, M.; Matsuoka, T.; Takasu, A. Epidemiology of patients with dizziness over a 3-year period, requiring utilization of the emergency medical serviced system—A Pre- and Post-COVID pandemic comparative study using the population-based ORION registry. J. Vestib. Res. 2023, 33, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, K.; Hibino, S.; Biros, M.H.; Irisawa, T.; Shimazu, T. Emergency medicine in Japan: Past, present, and future. Int. J. Emerg. Med. 2021, 14, 2. [Google Scholar] [CrossRef] [PubMed]
- Arai, H.; Ouchi, Y.; Toba, K.; Endo, T.; Shimokado, K.; Tsubota, K.; Matsuo, S.; Mori, H.; Yumura, W.; Yokode, M.; et al. Japan as the front-runner of super-aged societies: Perspectives from medicine and medical care in Japan. Geriatr. Gerontol. Int. 2015, 15, 673–687. [Google Scholar] [CrossRef] [PubMed]
- Pollard, C.A.; Morran, M.P.; Nestor-Kalinoski, A.L. The COVID-19 pandemic: A global health crisis. Physiol. Genom. 2020, 52, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Kurahara, Y.; Kobayashi, T.; Shintani, S.; Matsuda, Y.; Tamiya, A.; Sugawara, R.; Arai, T.; Tachibana, K.; Okishio, K.; Matsui, H.; et al. Clinical characteristics of COVID-19 in Osaka, Japan: Comparison of the first–third waves with the fourth wave. Respir. Investig. 2021, 59, 810–818. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Chubachi, S.; Namkoong, H.; Asakura, T.; Tanaka, H.; Otake, S.; Nakagawara, K.; Morita, A.; Fukushima, T.; Watase, M.; et al. Characteristics of hospitalized patients with COVID-19 during the first to fifth waves of infection: A report from the Japan COVID-19 Task Force. BMC Infect. Dis. 2022, 22, 935. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
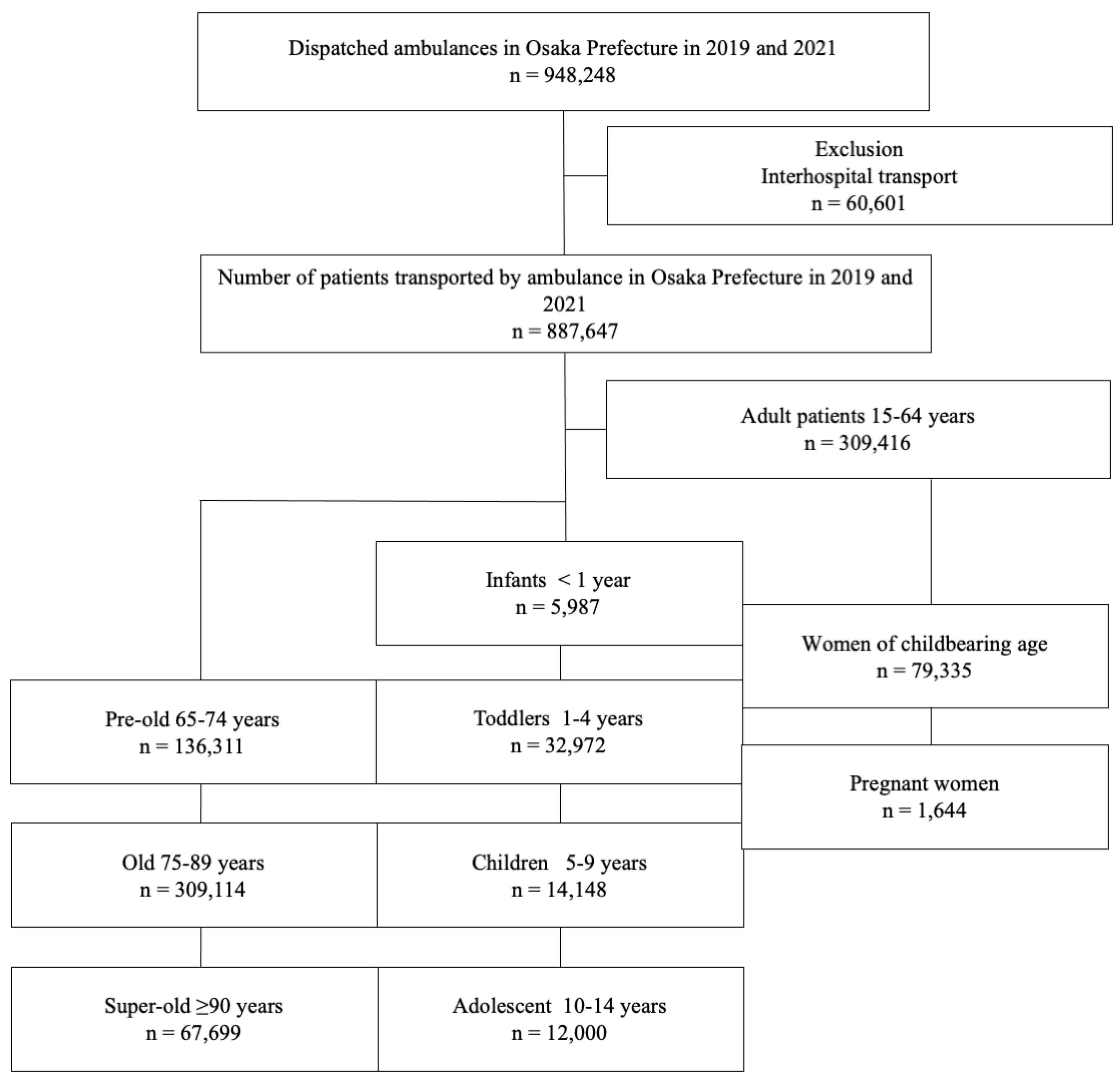
| Year | 2019 | 2021 | Total | p-Value |
|---|---|---|---|---|
| Number of patients | 468,697 | 418,950 | 887,647 | <0.001 |
| Age, median (IQR) | 70.0 (38) | 72.0 (37) | <0.001 | |
| Sex (male), % | 236,661 (50.5) | 212,458 (50.7) | 449,119 (50.6) | 0.04 |
| Pediatric patients, % | 37,547 (8.0) | 27,560 (6.6) | 65,107 (7.3) | <0.001 |
| Age category of children | <0.001 | |||
| Infants (0 y), % | 3375 (9.0) | 2612 (9.5) | 5987 (9.2) | |
| Toddlers (1–4 y), % | 18,891 (50.3) | 14,081 (51.1) | 32,972 (50.6) | |
| Children (5–9 y), % | 8480 (22.6) | 5668 (20.6) | 14,148 (21.7) | |
| Adolescents (10–14 y), % | 6801 (18.1) | 5199 (18.9) | 12,000 (18.4) | |
| Adult patients (15–64 y), % | 164,722 (35.1) | 144,694 (34.5) | 309,416 (34.9) | <0.001 |
| Women of childbearing age (15–44 y), % | 43,105 (9.2) | 36,230 (8.6) | 79,335 (8.9) | <0.001 |
| Pregnant women, % | 943 (0.2) | 701 (0.2) | 1644 (0.2) | <0.001 |
| Elderly patients, % | 266,428 (56.8) | 246,550 (59.4) | 513,124 (57.8) | <0.001 |
| Age category of elderly | <0.001 | |||
| Pre-old (65–74 y), % | 73,062 (27.4) | 63,249 (25.6) | 136,311 (26.6) | |
| Old (75–89 y), % | 160,666 (60.3) | 148,448 (60.2) | 309,114 (60.2) | |
| Super-old (≥90 y), % | 32,700 (12.3) | 34,999 (14.2) | 67,699 (13.2) |
| 2019 | Not Difficult-to-Transport Cases | Difficult-to-Transport Cases | All |
|---|---|---|---|
| Infants (0 y), % | 3349 (99.2) | 26 (0.8) | 3375 (9.0) |
| Toddlers (1–4 y), % | 18,751 (99.3) | 140 (0.7) | 18,891 (50.3) |
| Children (5–9 y), % | 8338 (98.3) | 142 (1.7) | 8,480 (22.6) |
| Adolescents (10–14 y), % | 6676 (98.2) | 125 (1.8) | 6801 (18.1) |
| Total | 37,114 (98.9) | 433 (1.2) | 37,547 |
| 2021 | Not difficult-to-transport cases | Difficult-to-transport cases | All |
| Infants (0 y), % | 2572 (98.5) | 40 (1.5) | 2612 (9.5) |
| Toddlers (1–4 y), % | 13,901 (98.7) | 180 (1.3) | 14,081 (51.1) |
| Children (5–9 y), % | 5548 (97.9) | 120 (2.1) | 5668 (20.6) |
| Adolescents (10–14 y), % | 5071 (97.5) | 128 (2.5) | 5199 (18.9) |
| Total | 27,092 (98.3) | 468 (1.7) | 27,560 |
| Women of childbearing age (15–44 y), % | 41,602 (96.5) | 1503 (3.5) | 43,105 (9.2) |
| Pregnant women, % | 931 (98.7) | 12 (1.3) | 943 (0.2) |
| 2021 | Not difficult-to-transport cases | Difficult-to-transport cases | All |
| Women of childbearing age (15–44 y), % | 34,123 (94.2) | 2107 (5.8) | 36,230 (8.6) |
| Pregnant women, % | 681 (97.2) | 20 (2.9) | 701 (0.2) |
| Pre-old (65–74 y), % | 71,158 (97.4) | 1904 (2.6) | 73,062 (27.4) |
| Old (75–89 y), % | 156,936 (97.7) | 3730 (2.3) | 160,666 (60.3) |
| Super-old (≥90 y), % | 31,806 (97.3) | 894 (2.7) | 32,700 (12.3) |
| Total | 259,900 (97.6) | 6528 (2.5) | 266,428 |
| 2021 | Not difficult-to-transport cases | Difficult-to-transport cases | All |
| Pre-old (65–74 y), % | 60,320 (95.4) | 2929 (4.6) | 63,249 (25.6) |
| Old (75–89 y), % | 140,982 (95.0) | 7466 (5.0) | 148,448 (60.2) |
| Super-old (≥90 y), % | 32,838 (93.8) | 2161 (6.2) | 34,999 (14.2) |
| Total | 234,140 (94.9) | 12,556 (5.1) | 246,696 |
| Pediatric Patients | |||||
|---|---|---|---|---|---|
| 2019 | Infants (0 y), % | Toddlers (1–4 y), % | Children (5–9 y), % | Adolescents (10–14 y), % | Total, % |
| Admission, % | 650 (19.3) | 3103 (16.4) | 1410 (16.6) | 1023 (15.0) | 6186 (16.5) |
| Home, % | 2682 (79.5) | 15,719 (83.2) | 7020 (82.8) | 5722 (84.1) | 31,143 (82.9) |
| Transfer, % | 21 (0.6) | 55 (0.3) | 48 (0.6) | 48 (0.7) | 172 (0.5) |
| Death, % | 21 (0.6) | 14 (0.1) | 2 (0) | 8 (0.1) | 45 (0.1) |
| No show, % | 1 (0) | 0 | 0 | 0 | 1 (0) |
| Total | 3375 | 18,891 | 8480 | 6801 | 37,547 |
| 2021 | Infants (0 y), % | Toddlers (1–4 y), % | Children (5–9 y), % | Adolescents (10–14 y), % | Total, % |
| Admission, % | 498 (19.3) | 2429 (17.3) | 929 (16.4) | 908 (17.5) | 4764 (17.3) |
| Home, % | 2074 (79.4) | 11,595 (82.4) | 4702 (83.0) | 4245 (81.7) | 22,616 (82.1) |
| Transfer, % | 27 (1.0) | 53 (0.4) | 36 (0.6) | 41 (0.8) | 157 (0.6) |
| Death, % | 12 (0.5) | 4 (0) | 1 (0) | 5 (0) | 22 (0.1) |
| No show, % | 1 (0) | 0 | 0 | 0 | 1 (0) |
| Total | 2612 | 14,081 | 5668 | 5199 | 27,560 |
| Women of childbearing age and pregnant women | |||||
| 2019 | Pregnant women, % | Women of childbearing age (15–44 y), % | |||
| Admission, % | 547 (58.0) | 6938 (16.1) | |||
| Home, % | 391 (41.5) | 35,807 (83.1) | |||
| Transfer, % | 5 (0.5) | 283 (0.7) | |||
| Death, % | 0 | 66 (0.2) | |||
| No show, % | 0 | 11 (0.0) | |||
| Total | 943 | 43,105 | |||
| 2021 | Pregnant women, % | Women of childbearing age (15–44 y), % | |||
| Admission, % | 418 (59.6) | 6086 (16.8) | |||
| Home, % | 274 (39.1) | 29,777 (82.2) | |||
| Transfer, % | 9 (1.3) | 250 (0.7) | |||
| Death, % | 0 | 111 (0.3) | |||
| No show, % | 0 | 6 (0.0) | |||
| Total | 943 | 36,230 | |||
| Elderly patients | |||||
| 2019 | Pre-old (65–74 y), % | Old (75–89 y), % | Super-old (≥90 y), % | Total, % | |
| Admission, % | 31,161 (42.7) | 80,713 (50.2) | 20,128 (61.6) | 132,002 (49.6) | |
| Home, % | 39,904 (54.6) | 74,514 (46.4) | 11,162 (34.1) | 125,580 (47.1) | |
| Transfer, % | 1163 (1.6) | 2991 (1.9) | 593 (1.8) | 4747 (1.8) | |
| Death, % | 827 (1.1) | 2443 (1.5) | 816 (2.5) | 4086 (1.5) | |
| No show, % | 7 (0) | 5 (0) | 1 (0) | 13 (0) | |
| Total | 73,062 | 160,666 | 32,700 | 266,428 | |
| 2021 | Pre-old (65–74 y), % | Old (75–89 y), % | Super-old (≥90 y), % | Total, % | |
| Admission, % | 29,369 (46.4) | 77,541 (52.2) | 21,529 (61.5) | 128,439 (52.1) | |
| Home, % | 31,761 (50.2) | 64,981 (43.8) | 11,677 (33.4) | 108,419 (44.0) | |
| Transfer, % | 1163 (1.8) | 2991 (2.0) | 733 (2.1) | 4887 (2.0) | |
| Death, % | 952 (1.5) | 2927 (2.0) | 1057 (3.0) | 4936 (2.0) | |
| No show, % | 4 (0) | 8 (0) | 3 (0) | 15 (0) | |
| Total | 63,249 | 148,448 | 34,999 | 246,696 | |
| 2021 vs. 2019 (Reference) | |||||
|---|---|---|---|---|---|
| Odds Ratio | 95%CI | p-Value | |||
| Infants (0 y) | 1.42 | 1.10 | – | 1.81 | 0.006 |
| Toddlers (1–4 y) | 1.32 | 1.18 | – | 1.47 | <0.001 |
| Children (5–9 y) | 1.13 | 1.00 | – | 1.27 | 0.056 |
| Adolescents (10–14 y) | 1.16 | 1.03 | – | 1.32 | 0.019 |
| Women of childbearing age (15–44 y) | 1.31 | 1.26 | – | 1.35 | <0.001 |
| Pregnant women | 1.51 | 1.05 | – | 2.17 | 0.025 |
| Pre-old (65–74 y) | 1.35 | 1.31 | – | 1.39 | <0.001 |
| Old (75–89 y) | 1.49 | 1.46 | – | 1.52 | <0.001 |
| Super-old (≥90 y) | 1.53 | 1.47 | – | 1.59 | <0.001 |
| Non-vulnerable patients | 1.28 | 1.26 | – | 1.30 | <0.001 |
| Vulnerable patients | 1.46 | 1.44 | – | 1.48 | <0.001 |
| Pediatric Patients as a Variable | |||||
|---|---|---|---|---|---|
| Odds Ratio | 95%CI | p-Value | |||
| Year | |||||
| 2019 | Reference | ||||
| 2021 | 1.39 | 1.37 | – | 1.40 | <0.001 |
| Female (compared with male) | 0.91 | 0.89 | – | 0.93 | <0.001 |
| Month | |||||
| June | Reference | ||||
| January | 1.87 | 1.78 | – | 1.98 | <0.001 |
| February | 1.52 | 1.44 | – | 1.61 | <0.001 |
| March | 1.24 | 1.17 | – | 1.32 | <0.001 |
| April | 1.64 | 1.56 | – | 1.74 | <0.001 |
| May | 1.59 | 1.50 | – | 1.68 | <0.001 |
| July | 1.00 | 0.94 | – | 1.06 | 0.963 |
| August | 1.28 | 1.21 | – | 1.35 | <0.001 |
| September | 1.27 | 1.20 | – | 1.35 | <0.001 |
| October | 1.01 | 0.95 | – | 1.07 | 0.851 |
| November | 1.01 | 0.95 | – | 1.07 | 0.773 |
| December | 1.06 | 1.00 | – | 1.13 | 0.04 |
| Weekends (compared with weekdays) | 1.19 | 1.16 | – | 1.22 | <0.001 |
| Nighttime (17:00–09:00) (compared with daytime) | 2.55 | 2.49 | – | 2.61 | <0.001 |
| Children (compared with adult > 15 y) | 0.33 | 0.31 | – | 0.35 | <0.001 |
| COVID-19 (including suspected cases) | 1.38 | 1.29 | – | 1.46 | <0.001 |
| Pregnant women as a variable | |||||
| Odds ratio | 95%CI | p-value | |||
| Year | |||||
| 2019 | Reference | ||||
| 2021 | 1.39 | 1.38 | – | 1.41 | <0.001 |
| Female (compared with male) | 0.93 | 0.91 | – | 0.95 | <0.001 |
| Month | |||||
| June | Reference | ||||
| January | 1.91 | 1.81 | – | 2.01 | <0.001 |
| February | 1.55 | 1.47 | – | 1.65 | <0.001 |
| March | 1.27 | 1.20 | – | 1.34 | <0.001 |
| April | 1.66 | 1.57 | – | 1.75 | <0.001 |
| May | 1.60 | 1.51 | – | 1.69 | <0.001 |
| July | 1.01 | 0.95 | – | 1.07 | 0.752 |
| August | 1.31 | 1.23 | – | 1.38 | <0.001 |
| September | 1.29 | 1.22 | – | 1.37 | <0.001 |
| October | 1.02 | 0.96 | – | 1.09 | 0.448 |
| November | 1.03 | 0.97 | – | 1.09 | 0.365 |
| December | 1.08 | 1.02 | – | 1.15 | 0.008 |
| Weekends (compared with weekdays) | 1.18 | 1.16 | – | 1.21 | <0.001 |
| Nighttime (17:00–09:00) (compared with daytime) | 2.53 | 2.47 | – | 2.59 | <0.001 |
| Pregnant women | 0.48 | 0.34 | – | 0.69 | <0.001 |
| COVID-19 (including suspected cases) | 1.44 | 1.35 | – | 1.53 | <0.001 |
| Elderly patients as a variable | |||||
| Odds ratio | 95%CI | p-value | |||
| Year | |||||
| 2019 | Reference | ||||
| 2021 | 1.39 | 1.38 | – | 1.41 | <0.001 |
| Female (compared with male) | 0.93 | 0.91 | – | 0.95 | <0.001 |
| Month | |||||
| June | Reference | ||||
| January | 1.91 | 1.81 | – | 2.01 | <0.001 |
| February | 1.55 | 1.47 | – | 1.65 | <0.001 |
| March | 1.27 | 1.20 | – | 1.34 | <0.001 |
| April | 1.66 | 1.57 | – | 1.75 | <0.001 |
| May | 1.60 | 1.51 | – | 1.69 | <0.001 |
| July | 1.01 | 0.95 | – | 1.07 | 0.755 |
| August | 1.31 | 1.23 | – | 1.38 | <0.001 |
| September | 1.29 | 1.22 | – | 1.37 | <0.001 |
| October | 1.02 | 0.96 | – | 1.09 | 0.453 |
| November | 1.03 | 0.97 | – | 1.09 | 0.373 |
| December | 1.08 | 1.02 | – | 1.15 | 0.008 |
| Weekends (compared with weekdays) | 1.18 | 1.16 | – | 1.21 | <0.001 |
| Nighttime (17:00–09:00) (compared with daytime) | 2.53 | 2.47 | – | 2.59 | <0.001 |
| Old (compared with young <65 y) | 1.01 | 0.99 | – | 1.03 | 0.403 |
| COVID-19 (including suspected cases) | 1.44 | 1.35 | – | 1.53 | <0.001 |
| Vulnerable patients as a variable | |||||
| Odds ratio | 95%CI | p-value | |||
| Year | |||||
| 2019 | Reference | ||||
| 2021 | 1.40 | 1.38 | – | 1.41 | <0.001 |
| Female (compared with male) | 0.94 | 0.92 | – | 0.96 | <0.001 |
| Month | |||||
| June | Reference | ||||
| January | 1.93 | 1.83 | – | 2.03 | <0.001 |
| February | 1.56 | 1.48 | – | 1.65 | <0.001 |
| March | 1.27 | 1.20 | – | 1.35 | <0.001 |
| April | 1.66 | 1.57 | – | 1.75 | <0.001 |
| May | 1.60 | 1.51 | – | 1.69 | <0.001 |
| July | 1.01 | 0.95 | – | 1.07 | 0.867 |
| August | 1.29 | 1.22 | – | 1.37 | <0.001 |
| September | 1.29 | 1.22 | – | 1.37 | <0.001 |
| October | 1.02 | 0.96 | – | 1.09 | 0.457 |
| November | 1.03 | 0.97 | – | 1.10 | 0.328 |
| December | 1.09 | 1.02 | – | 1.15 | 0.006 |
| Weekends (compared with weekdays) | 1.18 | 1.16 | – | 1.21 | <0.001 |
| Nighttime (17:00–09:00) (compared with daytime) | 2.47 | 2.41 | – | 2.53 | <0.001 |
| Vulnerable patients (compared with non-vulnerable) | 0.81 | 0.80 | – | 0.83 | <0.001 |
| COVID-19 (including suspected cases) | 1.41 | 1.32 | – | 1.50 | <0.001 |
| Odds Ratio | 95%CI | p-Value | |||
| Year | |||||
| 2019 | Reference | ||||
| 2021 | 1.17 | 1.15 | – | 1.19 | <0.001 |
| Female (compared with male) | 0.76 | 0.73 | – | 0.79 | <0.001 |
| Month | |||||
| June | Reference | ||||
| January | 1.62 | 1.47 | – | 1.78 | <0.001 |
| February | 1.52 | 1.38 | – | 1.68 | <0.001 |
| March | 1.24 | 1.12 | – | 1.37 | <0.001 |
| April | 1.30 | 1.18 | – | 1.44 | <0.001 |
| May | 1.32 | 1.20 | – | 1.46 | <0.001 |
| July | 0.92 | 0.82 | – | 1.02 | 0.103 |
| August | 0.99 | 0.89 | – | 1.10 | 0.845 |
| September | 1.05 | 0.94 | – | 1.16 | 0.387 |
| October | 1.02 | 0.92 | – | 1.14 | 0.659 |
| November | 1.19 | 1.08 | – | 1.32 | 0.001 |
| December | 1.37 | 1.24 | – | 1.50 | <0.001 |
| Weekends (compared with weekdays) | 0.98 | 0.93 | – | 1.02 | 0.242 |
| Nighttime (17:00–09:00) (compared with daytime) | 1.60 | 1.54 | – | 1.66 | <0.001 |
| Old (compared with young <65 y) | 4.04 | 3.83 | – | 4.25 | <0.001 |
| COVID-19 (including suspected cases) | 0.25 | 0.19 | – | 0.32 | <0.001 |
| 2019 | |||||
| Odds ratio | 95% confidence interval | p-value | |||
| Female (compared with male) | 0.74 | 0.70 | – | 0.78 | <0.001 |
| Month | |||||
| June | Reference | ||||
| January | 1.54 | 1.35 | – | 1.76 | <0.001 |
| February | 1.51 | 1.31 | – | 1.73 | <0.001 |
| March | 1.27 | 1.10 | – | 1.47 | 0.001 |
| April | 1.17 | 1.01 | – | 1.35 | 0.039 |
| May | 1.06 | 0.91 | – | 1.23 | 0.446 |
| July | 0.88 | 0.76 | – | 1.03 | 0.115 |
| August | 0.85 | 0.73 | – | 0.99 | 0.041 |
| September | 1.02 | 0.87 | – | 1.18 | 0.821 |
| October | 0.99 | 0.85 | – | 1.16 | 0.938 |
| November | 1.17 | 1.01 | – | 1.35 | 0.038 |
| December | 1.32 | 1.15 | – | 1.52 | <0.001 |
| Weekends (compared with weekdays) | 0.94 | 0.88 | – | 1.00 | 0.046 |
| Nighttime (17:00–09:00) (compared with daytime) | 1.54 | 1.46 | – | 1.64 | <0.001 |
| Old (compared with young <65 y) | 4.03 | 3.74 | – | 4.34 | <0.001 |
| COVID-19 (including suspected cases) | (omitted) | ||||
| 2021 | |||||
| Odds ratio | 95% confidence interval | p-value | |||
| Female (compared with male) | 0.78 | 0.74 | – | 0.83 | <0.001 |
| Month | |||||
| June | Reference | ||||
| January | 1.68 | 1.48 | – | 1.91 | <0.001 |
| February | 1.54 | 1.34 | – | 1.76 | <0.001 |
| March | 1.21 | 1.06 | – | 1.39 | 0.006 |
| April | 1.42 | 1.24 | – | 1.63 | <0.001 |
| May | 1.59 | 1.38 | – | 1.82 | <0.001 |
| July | 0.94 | 0.82 | – | 1.09 | 0.432 |
| August | 1.12 | 0.97 | – | 1.29 | 0.11 |
| September | 1.07 | 0.93 | – | 1.24 | 0.345 |
| October | 1.05 | 0.91 | – | 1.21 | 0.512 |
| November | 1.22 | 1.06 | – | 1.40 | 0.005 |
| December | 1.41 | 1.24 | – | 1.61 | <0.001 |
| Weekends (compared with weekdays) | 1.00 | 0.95 | – | 1.06 | 0.974 |
| Nighttime (17:00–09:00) (compared with daytime) | 1.64 | 1.56 | – | 1.73 | <0.001 |
| Old (compared with young <65 y) | 4.05 | 3.77 | – | 4.34 | <0.001 |
| COVID-19 (including suspected cases) | 0.24 | 0.19 | 0.32 | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ota, K.; Nitta, M.; Komeya, T.; Matsuoka, T.; Takasu, A. Influence of the COVID-19 Outbreak in Vulnerable Patients (Pediatric Patients, Pregnant Women, and Elderly Patients) on an Emergency Medical Service System: A Pre- and Post-COVID-19 Pandemic Comparative Study Using the Population-Based ORION Registry. Medicina 2024, 60, 345. https://doi.org/10.3390/medicina60020345
Ota K, Nitta M, Komeya T, Matsuoka T, Takasu A. Influence of the COVID-19 Outbreak in Vulnerable Patients (Pediatric Patients, Pregnant Women, and Elderly Patients) on an Emergency Medical Service System: A Pre- and Post-COVID-19 Pandemic Comparative Study Using the Population-Based ORION Registry. Medicina. 2024; 60(2):345. https://doi.org/10.3390/medicina60020345
Chicago/Turabian StyleOta, Koshi, Masahiko Nitta, Tomonobu Komeya, Tetsuya Matsuoka, and Akira Takasu. 2024. "Influence of the COVID-19 Outbreak in Vulnerable Patients (Pediatric Patients, Pregnant Women, and Elderly Patients) on an Emergency Medical Service System: A Pre- and Post-COVID-19 Pandemic Comparative Study Using the Population-Based ORION Registry" Medicina 60, no. 2: 345. https://doi.org/10.3390/medicina60020345
APA StyleOta, K., Nitta, M., Komeya, T., Matsuoka, T., & Takasu, A. (2024). Influence of the COVID-19 Outbreak in Vulnerable Patients (Pediatric Patients, Pregnant Women, and Elderly Patients) on an Emergency Medical Service System: A Pre- and Post-COVID-19 Pandemic Comparative Study Using the Population-Based ORION Registry. Medicina, 60(2), 345. https://doi.org/10.3390/medicina60020345