
A Novel Technique for Basilar Invagination Treatment in a Patient with Klippel–Feil Syndrome: A Clinical Example and Brief Literature Review

 ,
,  and
and 
Abstract
:1. Introduction
2. Case Presentation
2.1. Patient History
2.2. Physical Examination
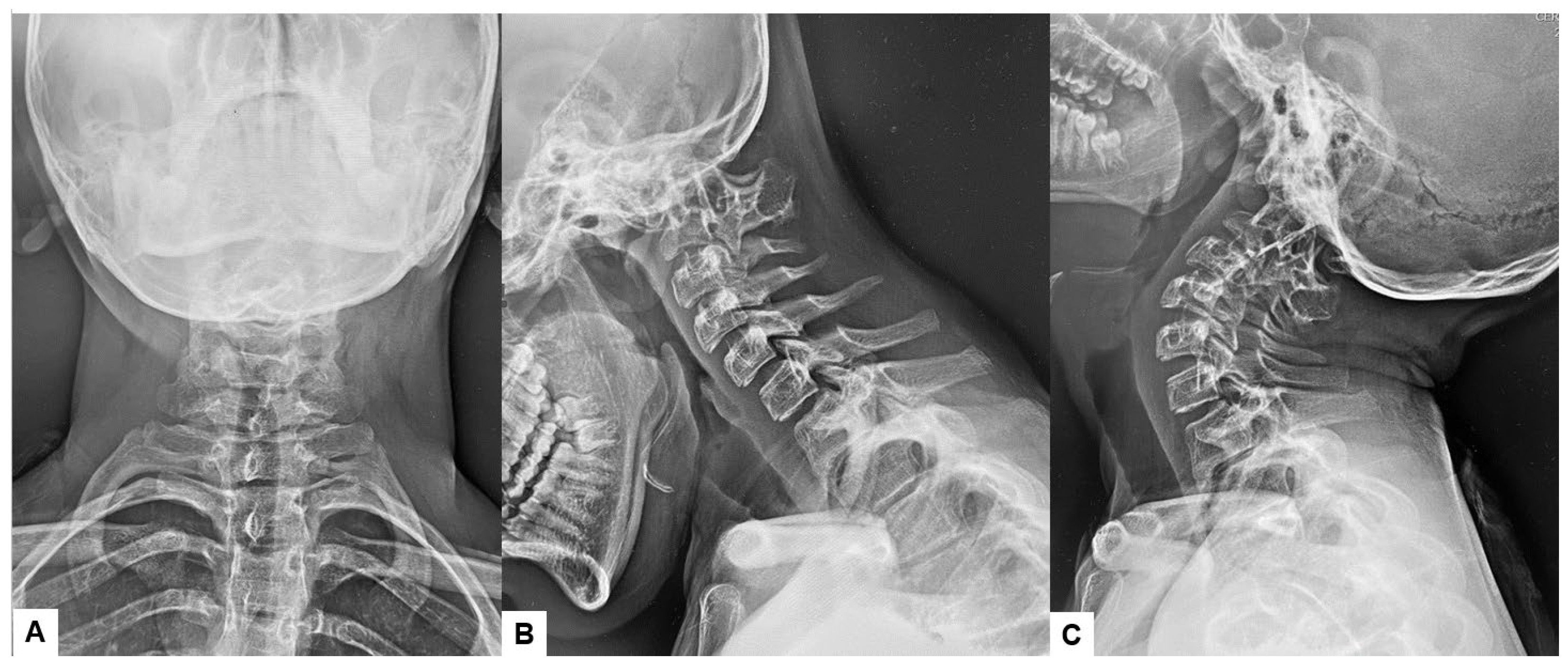
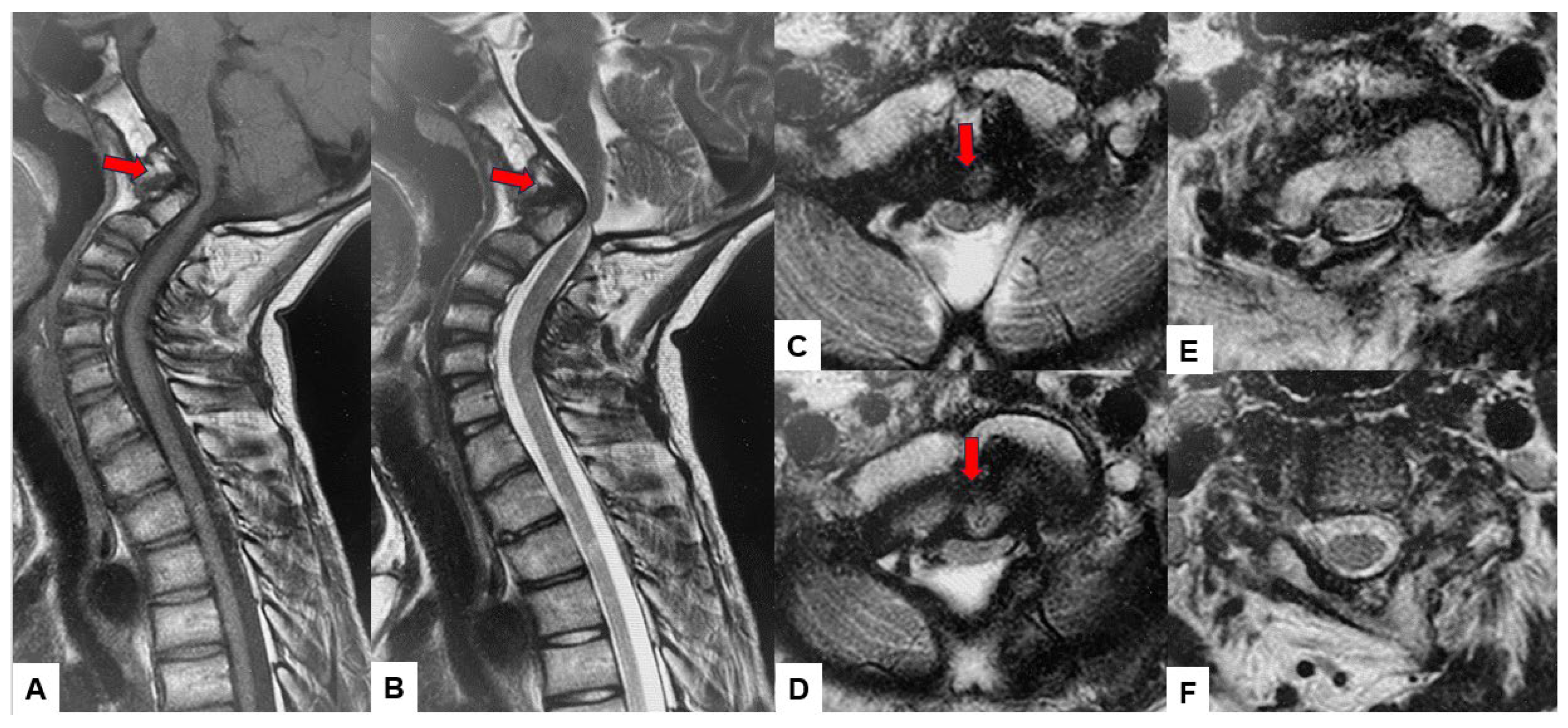
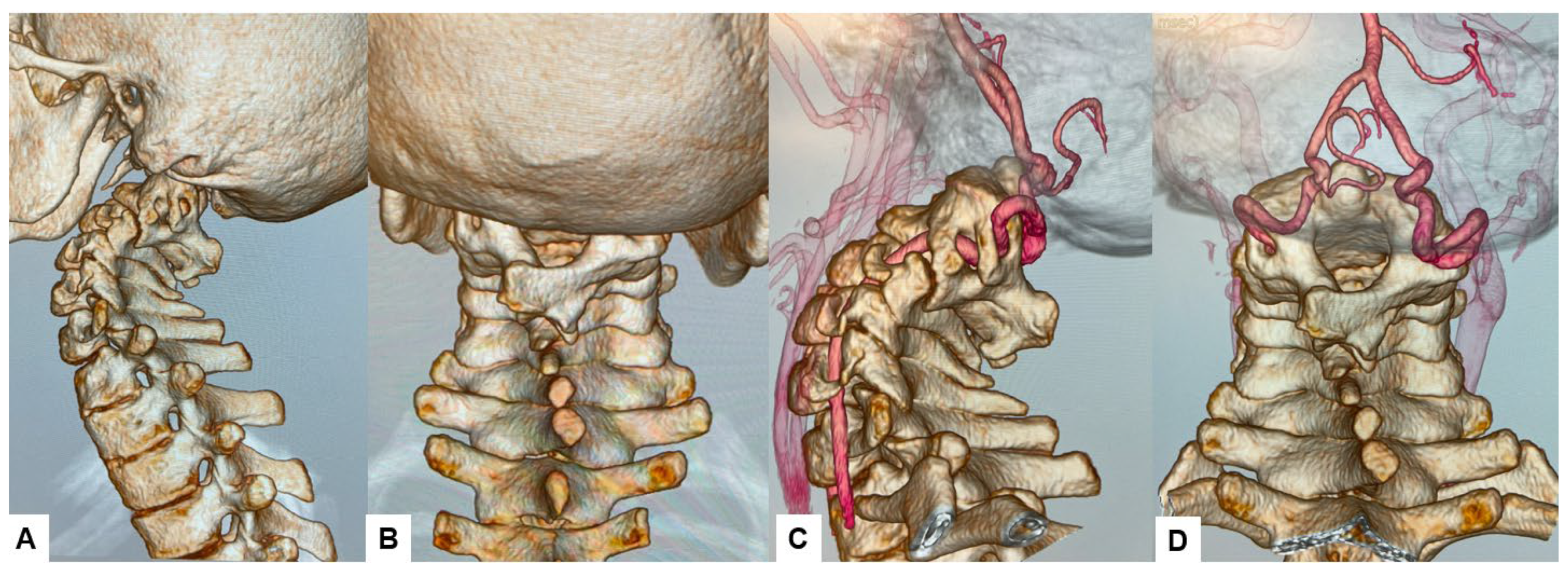
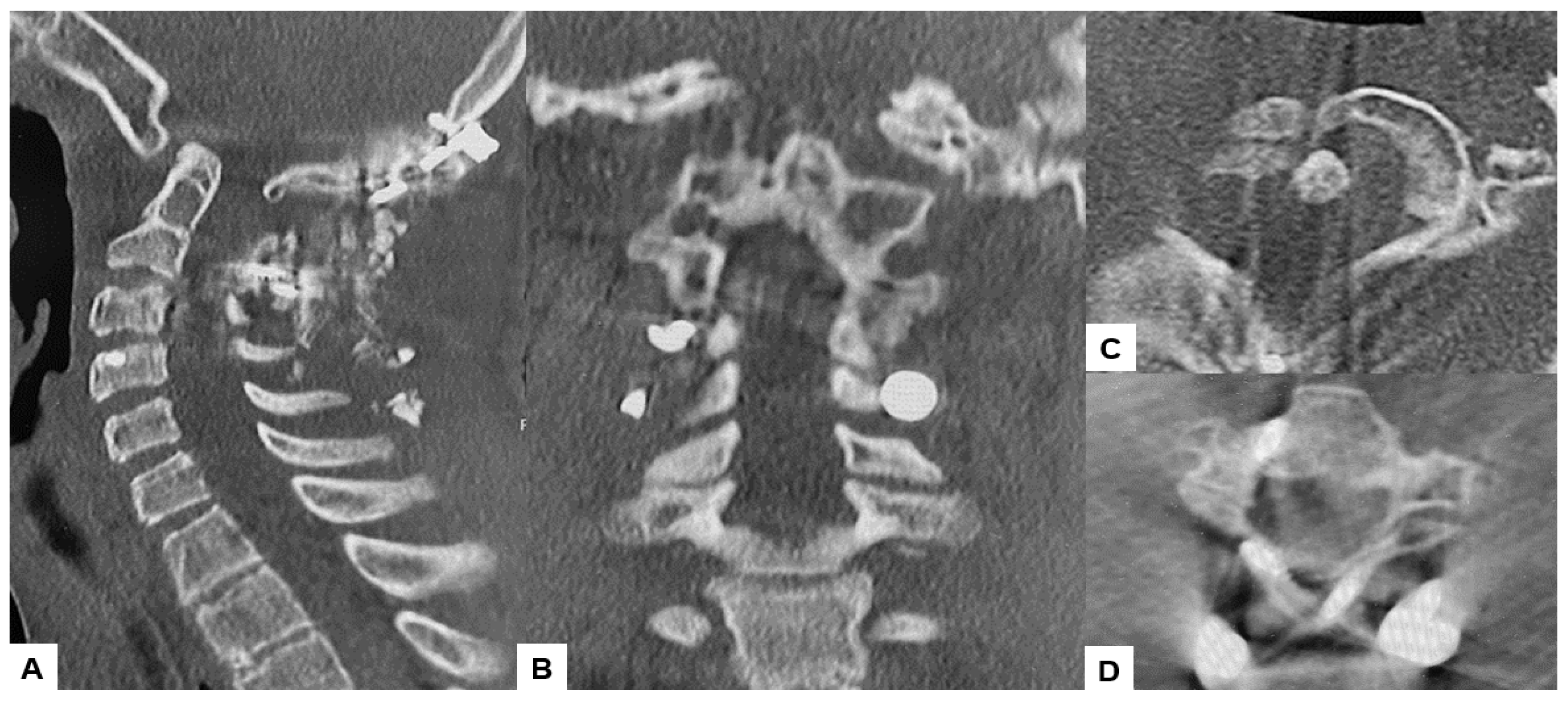
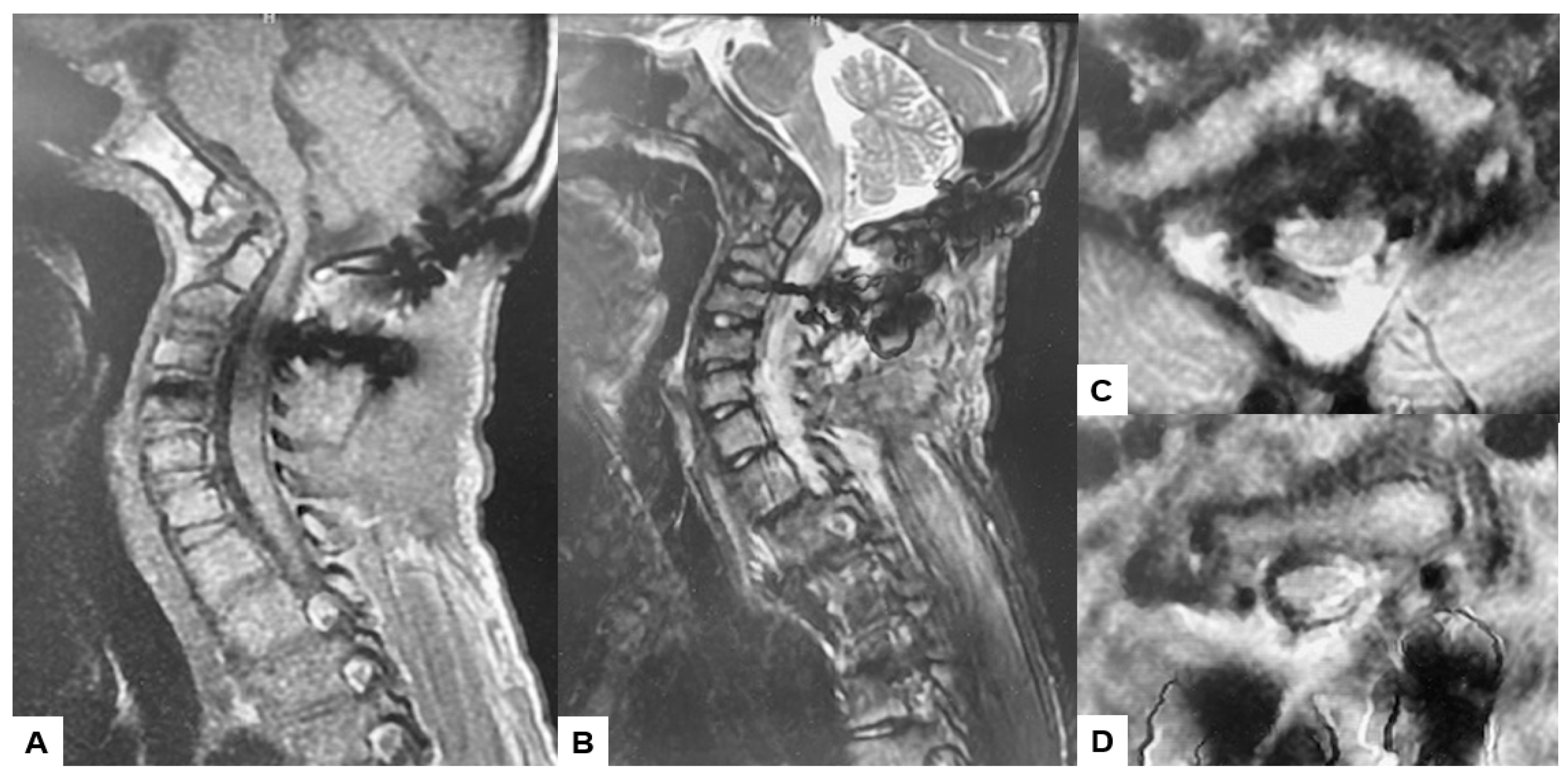
2.3. Preoperative Imaging
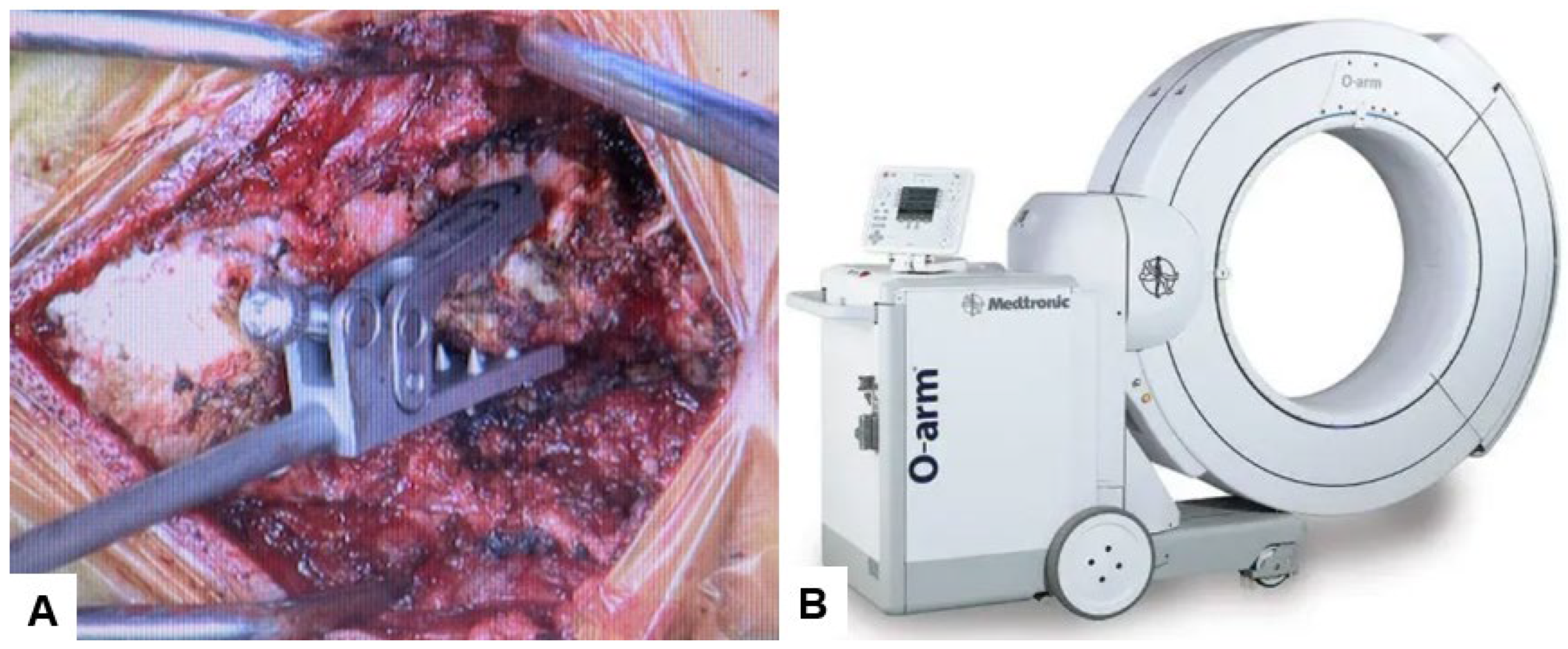
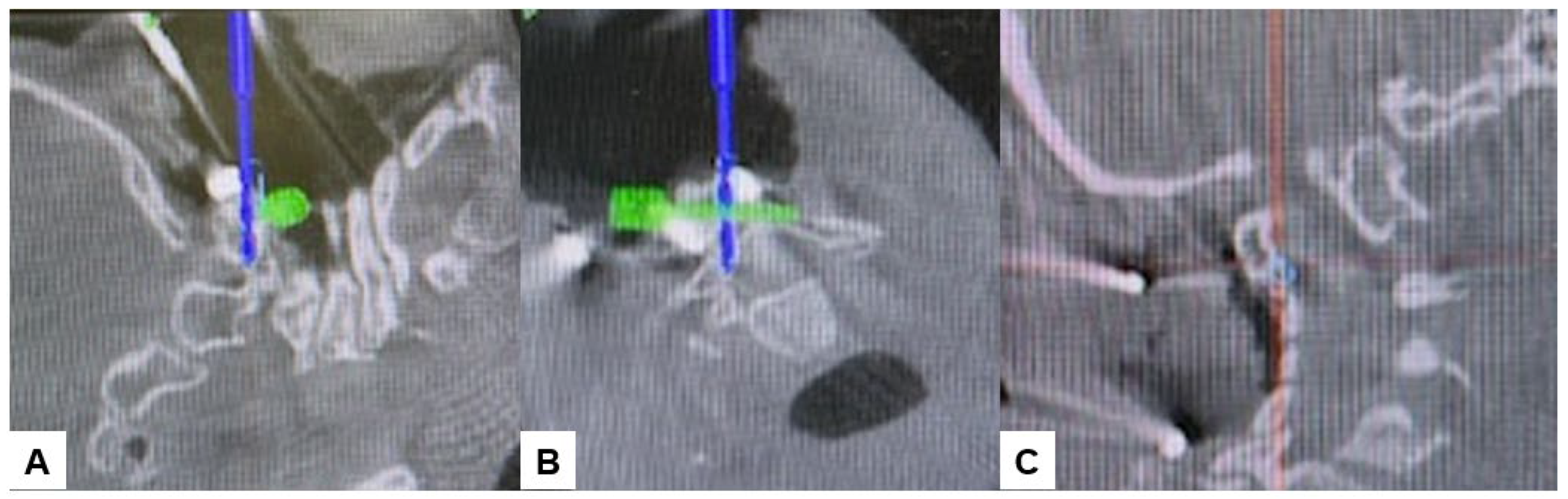
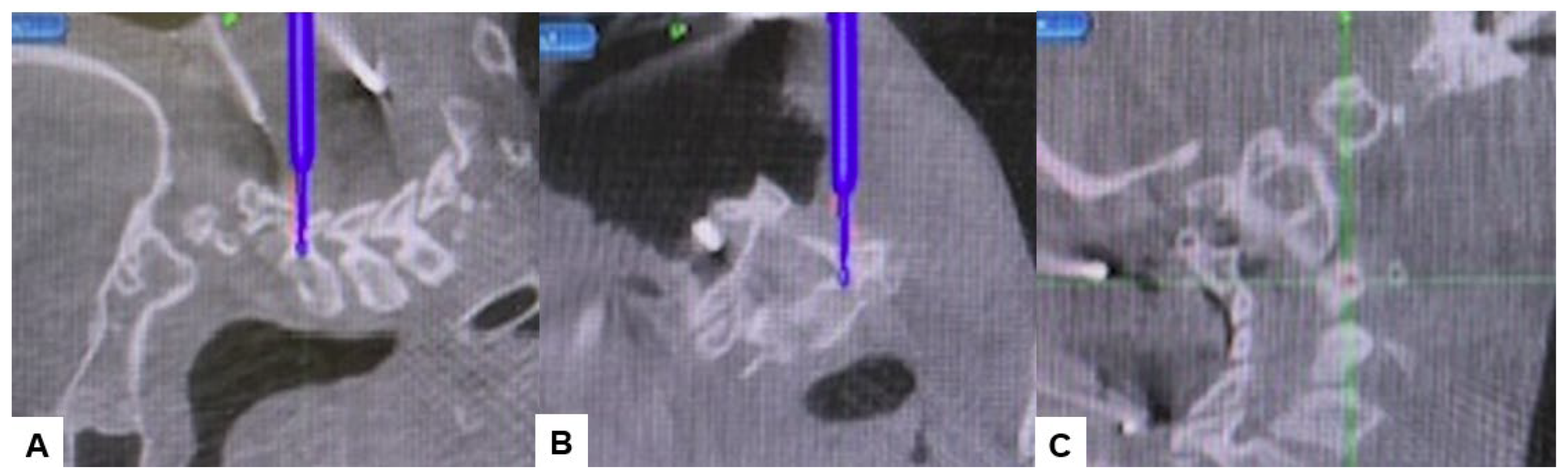
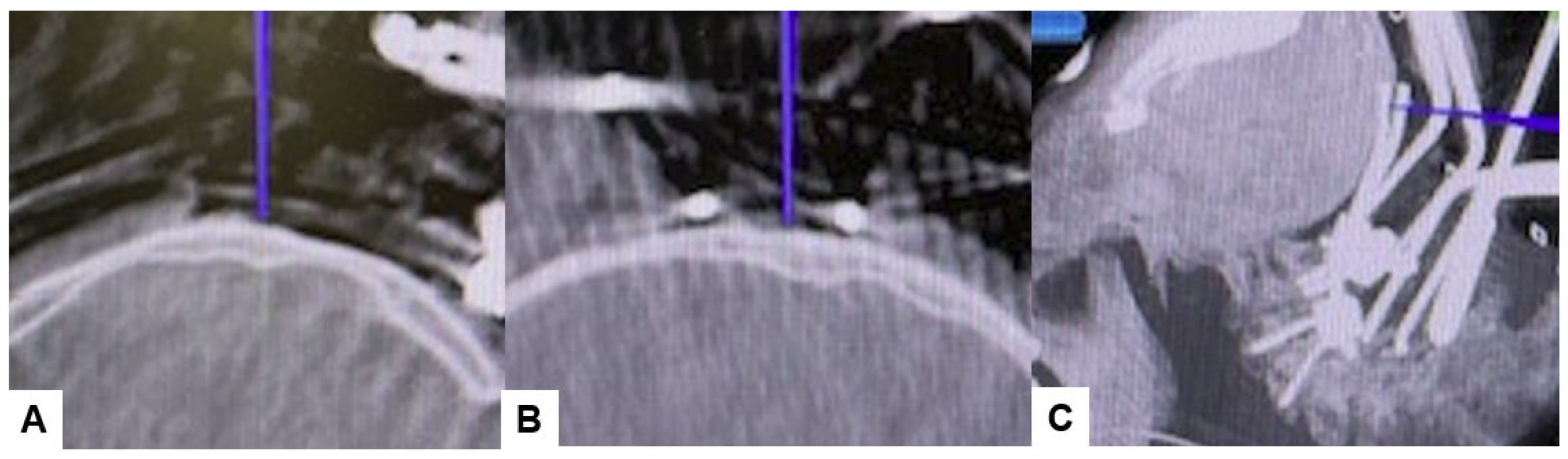
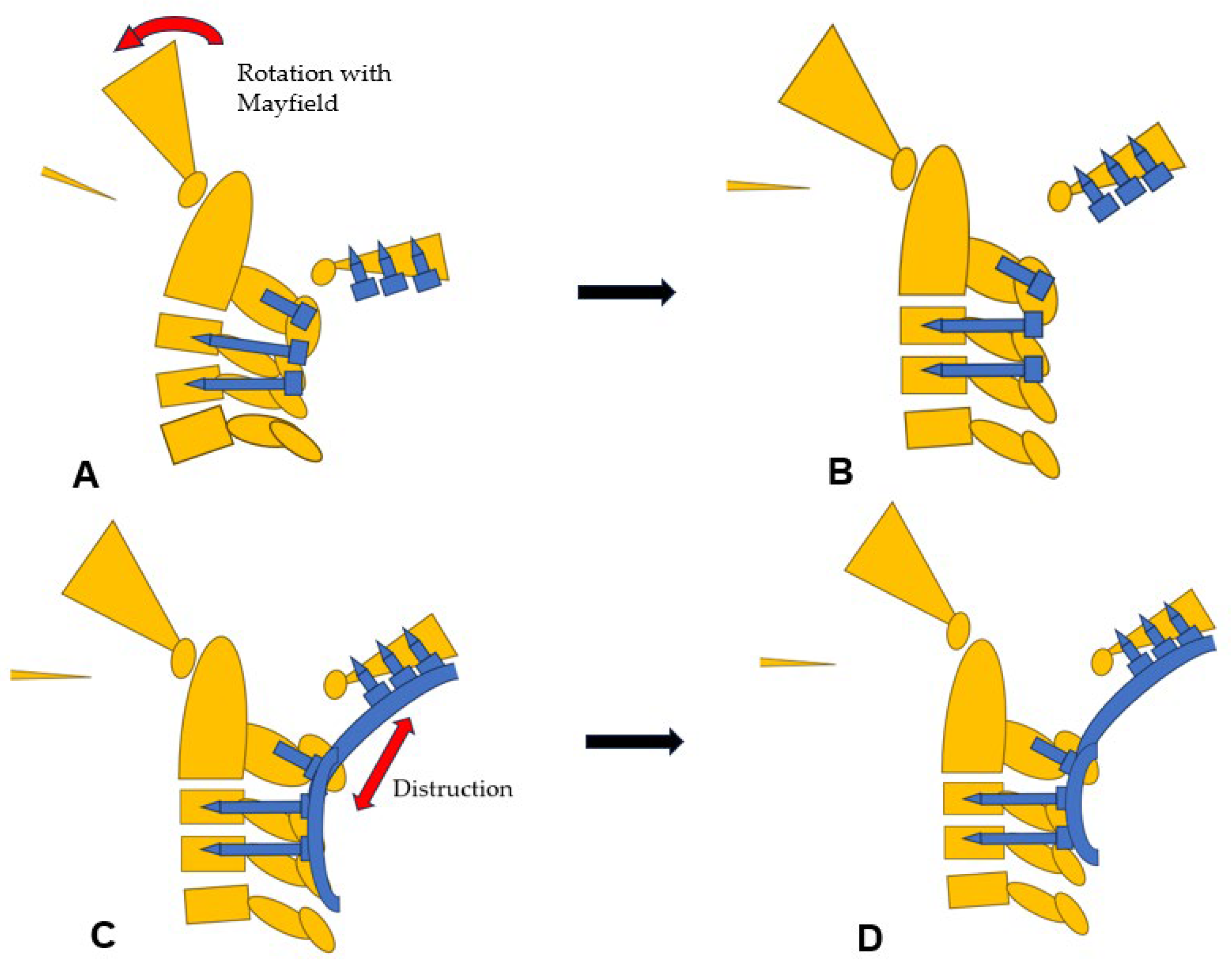
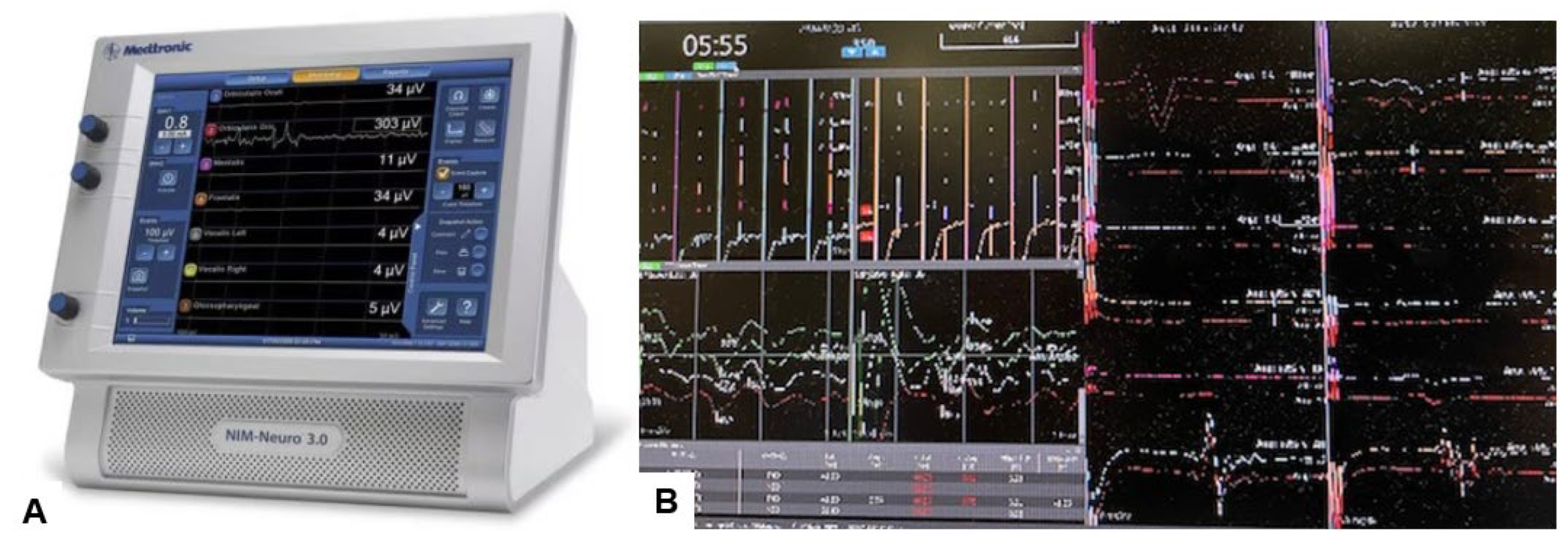
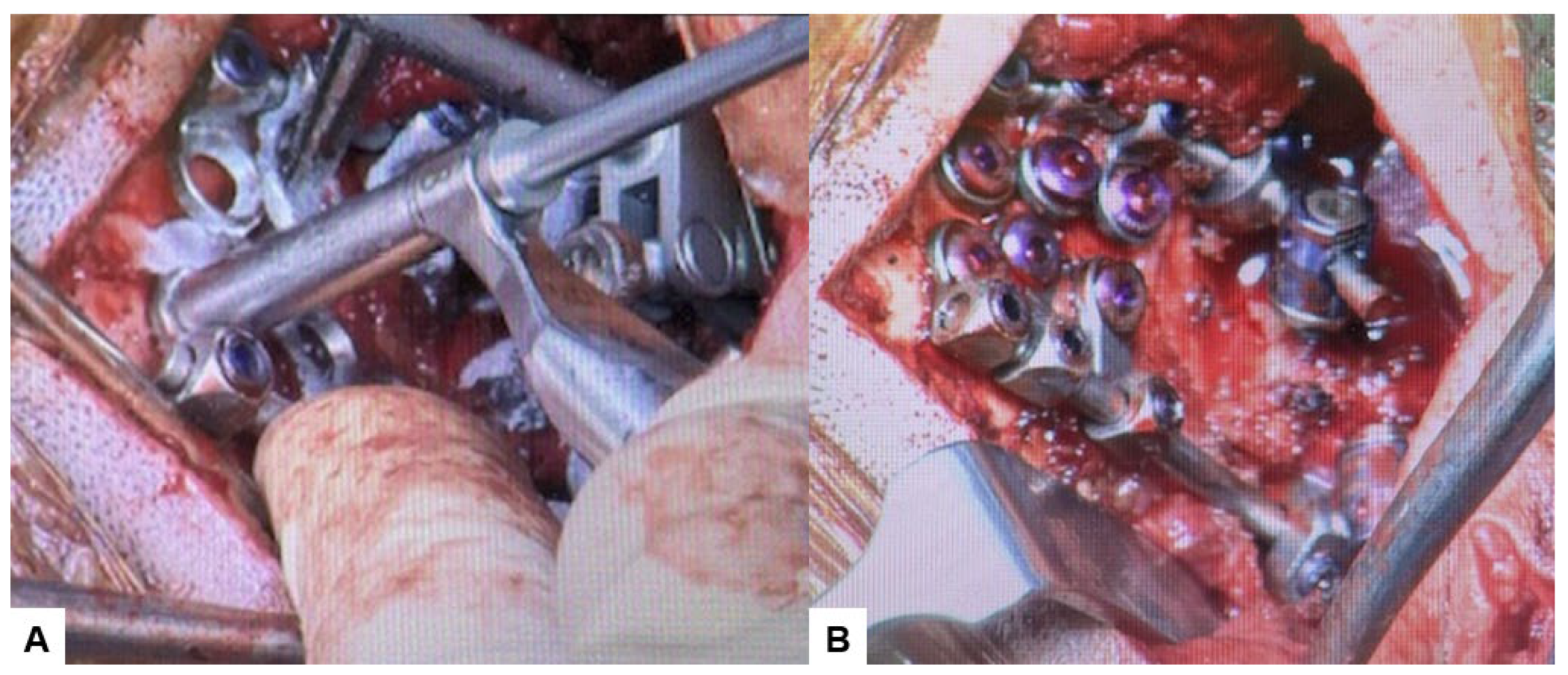
2.4. Surgery
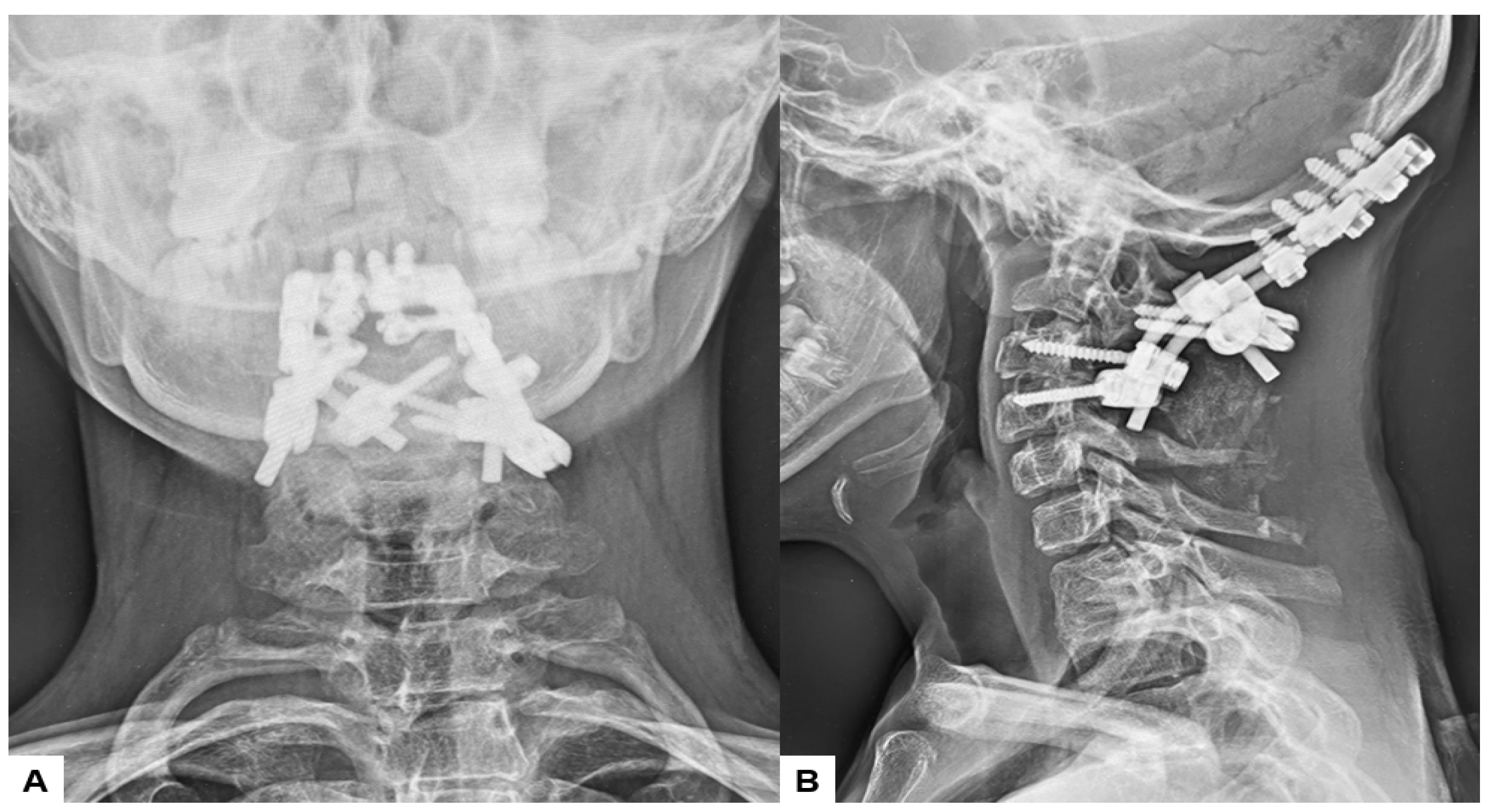
2.5. Postoperative Imaging
2.6. One Year Follow-Up
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Da Silva, E.O. Autosomal recessive Klippel-Feil syndrome. J. Med. Genet. 1982, 19, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Klippel, M.; Feil, A. Un cas d’absence des vertebres cervicales. Avec cage thoracique remontant jusqu’a la base du crane (cage thoracique cervicale). Nouv. Iconog Salpetriere 1912, 25, 223–250. [Google Scholar]
- Nagib, M.G.; Maxwell, R.E.; Chou, S.N. Identification and management of high-risk patients with Klippel-Feil syndrome. J. Neurosurg. 1984, 61, 523–530. [Google Scholar] [CrossRef]
- Ackermann, J.F. Ueber die Kretinen, einebesondereMenschenabart in den Alpen. In Gotha, in der EttingerschenBuchhandlung; Hansebooks Publisher: Norderstedt, Germany, 1790. [Google Scholar]
- Joaquim, A.F.; Ghizoni, E.; Giacomini, L.A.; Tedeschi, H.; Patel, A.A. Basilar invagination: Surgical results. J. Craniovertebr. Junction Spine 2014, 5, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Goel, A. Instability and basilar invagination. J. Craniovertebr. Junction Spine 2012, 3, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Schüller, A. Zur Röntgendiagnose der basilären impression des schädels. Wien. Med. Wochenschr. 1911, 61, 2594–2599. [Google Scholar]
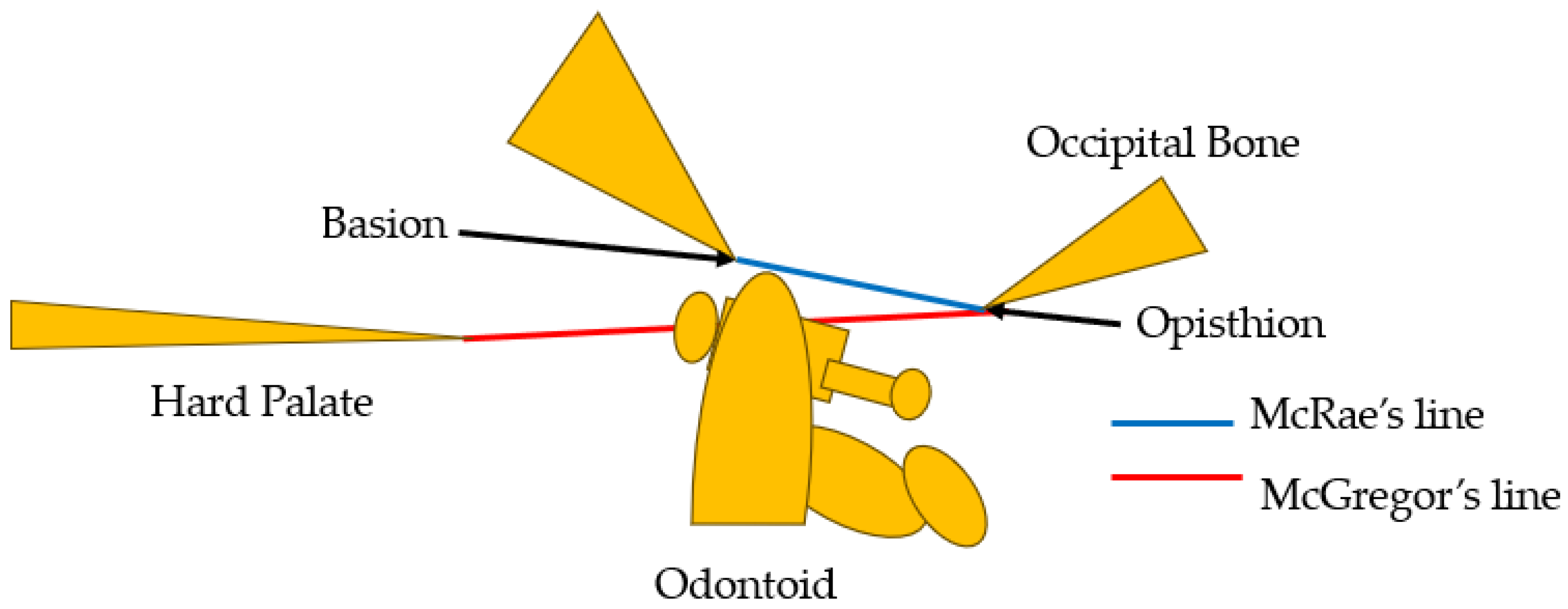
- McGregor, M. The significance of certain measurements of the skull in the diagnosis of basilar impression. Br. J. Radiol. 1948, 21, 171.e81. [Google Scholar] [CrossRef] [PubMed]
- McRae, D.L.; Barnum, A.S. Occipitalization of the atlas. AJR Am. J. Roentgenol. 1953, 70, 23. [Google Scholar]
- Brito, J.N.P.O.; Santos, B.A.D.; Nascimento, I.F.; Martins, L.A.; Tavares, C.B. Basilar invagination associated with chiari malformation type I: A literature review. Clinics 2019, 74, e653. [Google Scholar] [CrossRef]
- Kaplan, K.M.; Spivak, J.M.; Bendo, J.A. Embryology of the spine and associated congenital abnormalities. Spine J. 2005, 5, 564–576. [Google Scholar] [CrossRef]
- Greenberg, M.S. Klippel–Feil syndrome. In Handbook of Neurosurgery, 7th ed.; Greenberg, M.S., Ed.; Thieme Medical Publishers: New York, NY, USA, 2010; pp. 253–254. [Google Scholar]
- Thomsen, M.N.; Schneider, U.; Weber, M.; Johannisson, R.; Niethard, F.U. Scoliosis and congenital anomalies associated with Klippel–Feil syndrome types I–III. Spine 1997, 22, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Tracy, M.R.; Dormans, J.P.; Kusumi, K. Klippel-Feil syndrome: Clinical features and current understanding of etiology. Clin. Orthop. Relat. Res. 2004, 424, 183–190. [Google Scholar] [CrossRef]
- Donnally, I.I.I.C.J.; Munakomi, S.; Varacallo, M. Basilar Invagination; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Ferreira, J.A.; Botelho, R.V. The odontoid process invagination in normal subjects, Chiari malformation and Basilar invagination patients: Pathophysiologic correlations with angular craniometry. Surg. Neurol. Int. 2015, 6, 118. [Google Scholar] [CrossRef] [PubMed]
- Chamnan, R.; Chantarasirirat, K.; Paholpak, P.; Wiley, K.; Buser, Z.; Wang, J.C. Occipitocervical measurements: Correlation and consistency between multi-positional magnetic resonance imaging and dynamic radiographs. Eur. Spine J. 2020, 29, 2795–2803. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.P.; Zhang, R.J.; Zhang, H.Q.; Jiang, Z.F.; Shang, J.; Shen, C.L. Effect of High-Riding Vertebral Artery on the Accuracy and Safety of C2 Pedicle Screw Placement in Basilar Invagination and Related Risk Factors. Glob. Spine J. 2024, 14, 458–469. [Google Scholar] [CrossRef] [PubMed]
- Su, C.; Chen, Z.; Wu, H.; Jian, F. Computed tomographic angiography to analyze dangerous vertebral artery anomalies at the craniovertebral junction in patients with basilar invagination. Clin. Neurol. Neurosurg. 2021, 200, 106309. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.P.; Zhang, R.J.; Jiang, Z.F.; Tao, E.X.; Shang, J.; Shen, C.L. Ideal entry point and trajectory for C2 pedicle screw placement in basilar invagination patients with high-riding vertebral artery based on 3D computed tomography. Spine J. 2022, 22, 1281–1291. [Google Scholar] [CrossRef] [PubMed]
- Joaquim, A.F.; Tedeschi, H.; Chandra, P.S. Controversies in the surgical management of congenital craniocervical junction disorders—A critical review. Neurol. India 2018, 66, 1003–1015. [Google Scholar] [PubMed]
- Al Jishi, A. Commentary: Comprehensive Drilling of C1-2 Facets in Congenital Atlanto-Axial Dislocation and Basilar Invagination: Critical Review. Oper. Neurosurg. 2019, 16, 58–59. [Google Scholar] [CrossRef]
- Goel, A. Basilar invagination, Chiari malformation, syringomyelia: A review. Neurol. India 2009, 57, 235–246. [Google Scholar] [CrossRef]
- Garfin, S.R.; Botte, M.J.; Waters, R.L.; Nickel, V.L. Complications in the use of the halo fixation device. J. Bone Jt. Surg. 1986, 68, 320–325. [Google Scholar] [CrossRef]
- Abumi, K.; Takada TShono, Y.; Kaneda, K.; Fujiya, M. Posterior occipitocervical reconstruction using cervical pedicle screws and plate-rod systems. Spine 1999, 24, 1425–1434. [Google Scholar] [CrossRef]
- Menezes, A.H.; VanGilder, J.C.; Graf, C.J.; McDonnell, D.E. Craniocervical abnormalities. A comprehensive surgical approach. J. Neurosurg. 1980, 53, 444–455. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Serchi, E. Management of basilar invagination: A historical perspective. J. Craniovertebr. Junction Spine 2016, 7, 96–100. [Google Scholar] [CrossRef]
- Bharucha, E.P.; Dastur, H.M. Craniovertebral anomalies. (A report on 40 cases). Brain 1964, 87, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Menezes, A.H. Primary craniovertebral anomalies and hindbrain herniation syndrome (Chiari I): Database analysis. Pediatr. Neurosurg. 1995, 23, 260–269. [Google Scholar] [CrossRef]
- Crockard, H.A. Anterior approaches to lesions of the upper cervical spine. Clin. Neurosurg. 1988, 34, 389–416. [Google Scholar] [PubMed]
- Goel, A. Craniovertebral junction instability: A review of facts about facets. Asian Spine J. 2015, 9, 636–644. [Google Scholar] [CrossRef] [PubMed]
- Zileli, M.; Akıntürk, N. Complications of occipitocervical fixation: Retrospective review of 128 patients with 5-year mean follow-up. Eur. Spine J. 2022, 31, 311–326. [Google Scholar] [CrossRef]
- Das, K.K.; Pattankar, S.; Srivastava, A.K. Arterial Fencing: A Challenge During Complex Craniovertebral Junction Surgery. World Neurosurg. 2022, 161, 147–148. [Google Scholar] [CrossRef]
- Chibbaro, S.; Ganau, M.; Cebula, H.; Nannavecchia, B.; Todeschi, J.; Romano, A.; Debry, C.; Proust, F.; Olivi, A.; Gaillard, S.; et al. The Endonasal Endoscopic Approach to Pathologies of the Anterior Craniocervical Junction: Analytical Review of Cases Treated at Four European Neurosurgical Centres. Acta Neurochir. Suppl. 2019, 125, 187–195. [Google Scholar] [PubMed]
- Jain, V.K.; Mittal, P.; Banerji, D.; Behari, S.; Acharya, R.; Chhabra, D.K. Posterior occipitoaxial fusion for atrantoaxial dislocation associated with occipitalizedatlas. J. Neurosurg. 1996, 84, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Sheshadri, V.; Moga, R.; Manninen, P.; Goldstein, C.L.; Rampersaud, Y.R.; Massicotte, E.M.; Fehlings, M.G.; Venkatraghavan, L. Airway adverse events following posterior occipito-cervical spinal fusion. J. Clin. Neurosci. 2017, 39, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Huang, F.; Zhong, Q.; Wang, Y.; Weng, Y. Failed reintubation during resuscitation after posterior occipito-cervical spinal fusion: A case report. Medicine 2023, 102, e35427. [Google Scholar] [CrossRef] [PubMed]
- Izeki, M.; Neo, M.; Takemoto, M.; Fujibayashi, S.; Ito, H.; Nagai, K.; Matsuda, S. The O-C2 angle established at occipito-cervical fusion dictates the patient’s destiny in terms of postoperative dyspnea and/or dysphagia. Eur. Spine J. 2014, 23, 328–336. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, Y.; Kanemura, T.; Yoshida, G.; Matsumoto, A.; Ito, Z.; Tauchi, R.; Muramoto, A.; Ohno, S.; Nishimura, Y. Intraoperative, full-rotation, three-dimensional image (O-arm)-based navigation system for cervical pedicle screw insertion. J. Neurosurg. Spine 2011, 15, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Wada, K.; Tamaki, R.; Yui, M.; Numaguchi, D.; Murata, Y. C1 lateral mass screw insertion caudally from C2 nerve root —An alternate method for insertion of C1 screws: A technical note and preliminary clinical results. J. Orthop. Sci. 2017, 22, 213–217. [Google Scholar] [CrossRef] [PubMed]
- La Marca, F.; Zubay, G.; Morrison, T.; Karahalios, D. Cadaveric study for placement of occipital condyle screws: Technique and effects on surrounding anatomic structures. J. Neurosurg. Spine 2008, 9, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Uribe, J.S.; Ramos, E.; Vale, F. Feasibility of occipital condyle screw placement for occipitocervical fixation: A cadaveric study and description of a novel technique. J. Spinal Disord. Tech. 2008, 21, 540–546. [Google Scholar] [CrossRef]
- El-Gaidi, M.A.; Eissa, E.M.; El-Shaarawy, E.A. Free hand placement of occipital condyle screws: A cadaveric study. Eur. Spine J. 2014, 23, 2182–2188. [Google Scholar] [CrossRef]
- Bosco, A.; Venugopal, P.; Shetty, A.P.; Shanmuganathan, R.; Kanna, R.M. Morphometric evaluation of occipital condyles: Defining optimal trajectories and safe screw lengths for occipital condyle-based occipitocervical fixation in Indian population. Asian Spine J. 2018, 12, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Helgeson, M.D.; Lehman, R.A.; Sasso, R.C., Jr.; Dmitriev, A.E.; Mack, A.W.; Riew, K.D. Biomechanical analysis of occipitocervical stability afforded by three fixation techniques. Spine J. 2011, 11, 245–250. [Google Scholar] [CrossRef]
- Takigawa, T.; Simon, P.; Espinoza Orias, A.A.; Hong, J.T.; Ito, Y.; Inoue, N.; An, H.S. Biomechanical comparison of occiput-C1-C2 fixation techniques: C0-C1 transarticular screw and direct occiput condyle screw. Spine 2012, 37, E696–E701. [Google Scholar] [CrossRef] [PubMed]
- Van de Kelft, E.; Costa, F.; Van der Planken, D.; Schils, F. A prospective multicenter registry on the accuracy of pedicle screw placement in the thoracic, lumbar, and sacral levels with the use of the O-arm imaging system and Stealth Station navigation. Spine 2012, 37, E1580–E1587. [Google Scholar] [CrossRef]
- Weinstein, J.N.; Spratt, K.F.; Spengler, D.; Brick, C.; Reid, S. Spinal pedicle fixation: Reliability and validity of roentgenogram-based assessment and surgical factors on successful screw placement. Spine 1988, 13, 1012–1018. [Google Scholar] [CrossRef] [PubMed]
- Vaccaro, A.R.; Rizzolo, S.J.; Balderston, R.A. Placement of pedicle screws in the thoracic spine. Part II: An anatomical and radiographic assessment. J. Bone Jt. Surg. 1995, 77, 1200–1206. [Google Scholar] [CrossRef]
- Giordano, B.D.; Baumhauer, J.F.; Morgan, T.L.; Rechtine, G.R. Cervical spine imaging using standard C-arm fluoroscopy: Patient and surgeon exposure to ionizing radiation. Spine 2008, 33, 1970–1976. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Safe Permissible Sagittal Plane Angulation (Degrees) | Medial Plane Angulation (Degrees) | Screw Length (mm) | Screw Diameter (mm) |
|---|---|---|---|---|
| La Marca et al. [41] | 30 caudal | 10 medial | 22 (intraosseous) | 3.5 |
| Uribe et al. [42] | Zero to 5 cranial | 15 medial | 20 (intraosseous) | 3.5 |
| El-Gaidi et al. [43] | 4 ± 6.2 caudad angulation (range, from 5 cranially to 12 caudally) | 30 ± 6.7 (range, 20–40) medial | 22 ± 3.1 (intraosseous) | 3.5 |
| Bosco et al. [44] | From 0 to 5 cranial | 23–38 medial | 19.9 ± 2.3 (intraosseous) | 3.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanaka, M.; Askar, A.E.K.A.; Kumawat, C.; Arataki, S.; Komatsubara, T.; Taoka, T.; Uotani, K.; Oda, Y. A Novel Technique for Basilar Invagination Treatment in a Patient with Klippel–Feil Syndrome: A Clinical Example and Brief Literature Review. Medicina 2024, 60, 616. https://doi.org/10.3390/medicina60040616
Tanaka M, Askar AEKA, Kumawat C, Arataki S, Komatsubara T, Taoka T, Uotani K, Oda Y. A Novel Technique for Basilar Invagination Treatment in a Patient with Klippel–Feil Syndrome: A Clinical Example and Brief Literature Review. Medicina. 2024; 60(4):616. https://doi.org/10.3390/medicina60040616
Chicago/Turabian StyleTanaka, Masato, Abd El Kader Al Askar, Chetan Kumawat, Shinya Arataki, Tadashi Komatsubara, Takuya Taoka, Koji Uotani, and Yoshiaki Oda. 2024. "A Novel Technique for Basilar Invagination Treatment in a Patient with Klippel–Feil Syndrome: A Clinical Example and Brief Literature Review" Medicina 60, no. 4: 616. https://doi.org/10.3390/medicina60040616
APA StyleTanaka, M., Askar, A. E. K. A., Kumawat, C., Arataki, S., Komatsubara, T., Taoka, T., Uotani, K., & Oda, Y. (2024). A Novel Technique for Basilar Invagination Treatment in a Patient with Klippel–Feil Syndrome: A Clinical Example and Brief Literature Review. Medicina, 60(4), 616. https://doi.org/10.3390/medicina60040616