Antihypertensive Effect of Long-Term Oral Administration of Jellyfish (Rhopilema esculentum) Collagen Peptides on Renovascular Hypertension


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results and Discussion
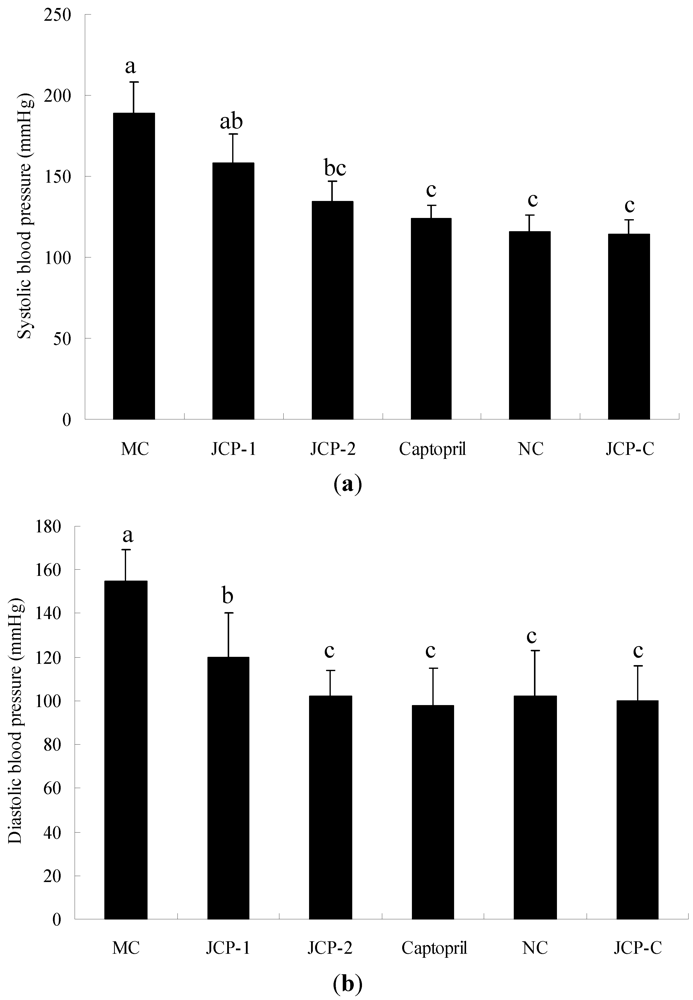
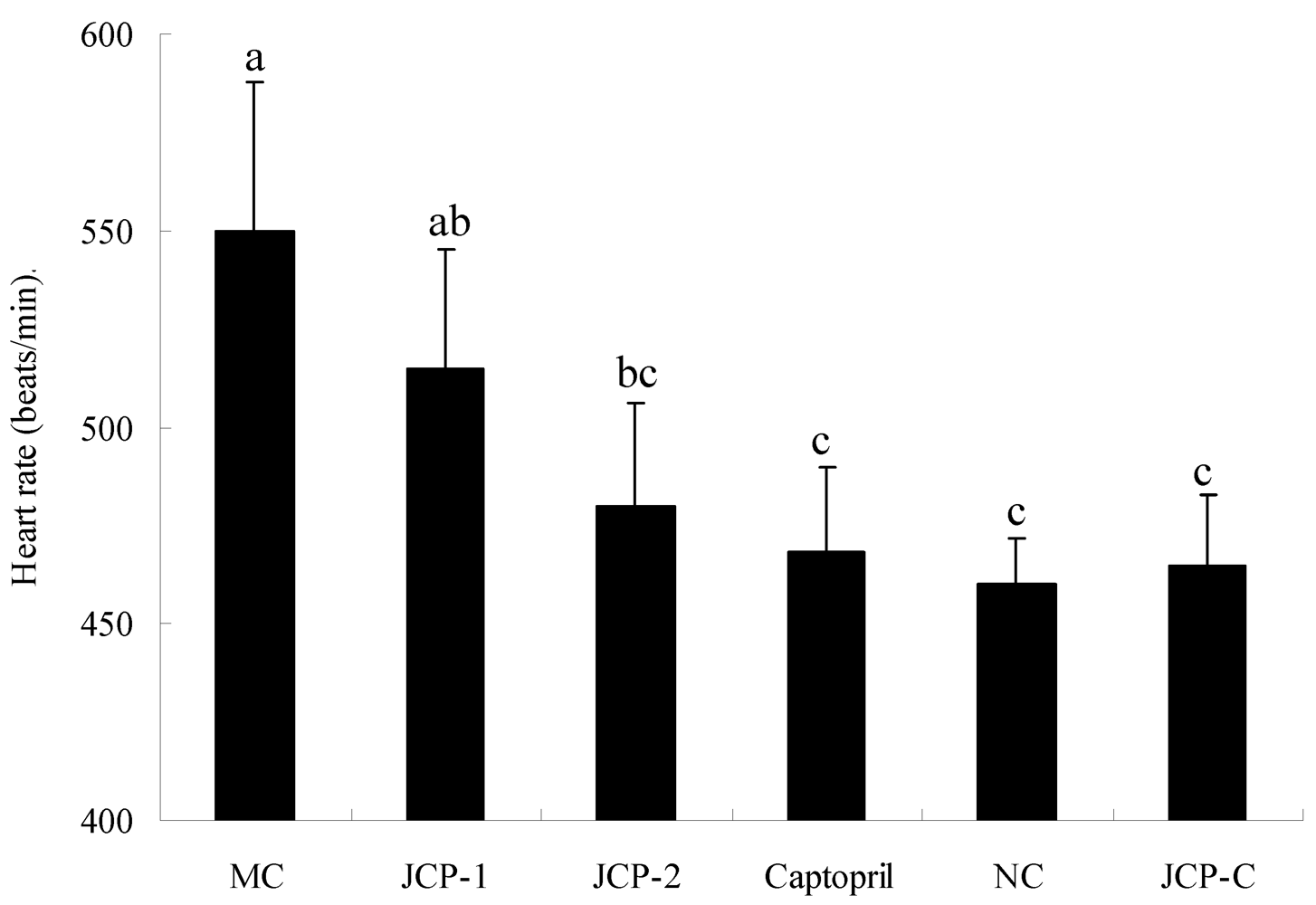
2.1. Blood Pressure and Heart Rate


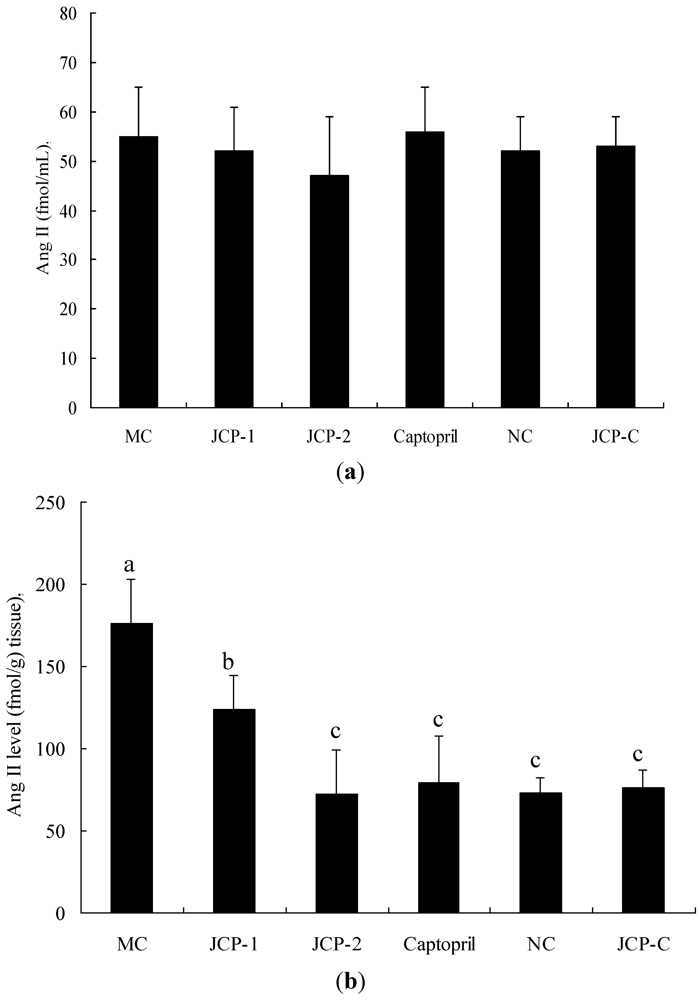
2.2. Angiotensin II Concentration

3. Experimental Section
3.1. Materials
3.2. Animal Treatment
3.3. Measurement of Blood Pressure and Heart Rate
3.4. Determination of Angiotensin-II (Ang II) Concentration
3.5. Statistical Analysis
4. Conclusions
Acknowledgements
References
- Zhuang, Y.; Sun, L.; Li, B. Production of the angiotensin-I-converting enzyme (ACE)-inhibitory peptide from hydrolysates of jellyfish (Rhopilema esculentum) collagen. Food Bioprocess Technol. 2010. [Google Scholar] [CrossRef]
- Richard, J.F.; Brain, A.M.; Daniel, J.W. The emerging role of dairy protein and bioactive peptides in nutrition and health. J. Nutr. 2004, 134, 980–988. [Google Scholar]
- Huang, W.H.; Sun, J.; He, H.; Dong, H.W.; Li, J.T. Antihypertensive effect of corn peptides, produced by a continuous production in enzymatic membrance reactor, in spontaneously hypertensive rats. Food Chem. 2011, 128, 968–973. [Google Scholar]
- Kim, S.K.; Choi, Y.R.; Park, P.J.; Choi, J.H.; Moon, S.H. Screening of biofunctional peptides from cod processing wastes. J. Korean Soc. Agric. Chem. Biotechnol. 2000, 43, 225–227. [Google Scholar]
- Zhao, Y.H.; Li, B.F.; Dong, S.Y.; Liu, Z.Y.; Zhao, X.; Wang, J.F.; Zeng, M.Y. A novel ACE inhibitory peptide isolated from Acaudina molpadioidea hydrolysate. Peptides 2009, 30, 1028–1033. [Google Scholar]
- Zhang, C.H.; Cao, W.H.; Hong, P.Z.; Ji, H.W.; Qin, X.M.; He, J.F. Angiotensin converting enzyme inhibitory activity of Acetes chinensis peptic hydrolysate and its antihypertensive effect in spontaneously hypertensive rats. Int. J. Food Sci. Technol. 2009, 44, 2042–2048. [Google Scholar]
- Ono, S.; Hosokawa, M.; Miyashita, K.; Takahashi, K. Inhibition properties of dipeptides from salmon muscle hydrolysate on angiotensin I-converting enzyme. Int. J. Food Sci. Technol. 2006, 41, 383–386. [Google Scholar]
- Lin, L.; Shun, L.; Li, B.F. Angiotensin-I-converting enzyme (ACE)-inhibitory and antihypertensive properties of squid skin gelatin hydrolysates. Food Chem. 2011. [Google Scholar] [CrossRef]
- Wu, J.; Aluko, R.E.; Nakai, S. Structural requirements of angiotensin I converting enzyme inhibitory peptides: Quantitative structure-activity relationship study of di- and tripeptides. J. Agric. Food Chem. 2006, 54, 732–738. [Google Scholar]
- Herregods, G.; van Camp, J.; Morel, N.; Ghesquière, B.; Gevaert, K.; Vercruysse, L.; Dierckx, S.; Quanten, E.; Smagghe, G. Angiotensin I-converting enzyme inhibitory activity of gelatin hydrolysates and identification of bioactive peptides. J. Agric. Food Chem. 2011, 59, 552–558. [Google Scholar]
- Lee, S.H.; Qian, Z.J.; Kim, S.K. A novel angiotensin I converting enzyme inhibitory peptide from tuna frame protein hydrolysate and its antihypertensive effect in spontaneously hypertensive rats. Food Chem. 2010, 118, 96–102. [Google Scholar]
- Foltz, M.; van der Pijl, P.C.; Duchateau, G.S.M.J.E. Current in vitro testing of bioactive peptides is not valuable. J. Nutr. 2010, 140, 117–118. [Google Scholar]
- Maeno, M.; Yamamoto, N.; Takano, T. Identification of an antihypertensive peptide from casein hydrolysate produced by a proteinase from Lactobacillus helveticus CP790. J. Dairy Sci. 1996, 79, 1316–1321. [Google Scholar]
- Ondetti, M.A.; Cushman, D.W. Enzymes of the rennin angiotensin system and their inhibitors. Ann. Rev. Biochem. 1982, 51, 283–308. [Google Scholar]
- Brown, N.J.; Vaughan, D.E. Angiotensin-converting enzyme inhibitors. Circulation 1998, 97, 1411–1420. [Google Scholar]
- Fujita, H.; Yokoyama, K.; Yoshikawa, M. Classification and antihypertensive activity of angiotensin I-converting enzyme inhibitory peptides derived from food proteins. J. Food Sci. 2000, 65, 564–569. [Google Scholar]
- Vercruysse, L.; Smagghe, G.; Herregods, G.; van Camp, J. ACE inhibitory activity in enzymatic hydrolysates of insect protein. J. Agric Food. Chem. 2005, 53, 5207–5211. [Google Scholar]
- Vercruysse, L.; Van Camp, J.; Morel, N.; Rougé, P.; Herregods, G.; Smagghe, G. Ala-Val-Phe and Val-Phe: ACE inhibitory peptides derived from insect protein with antihypertensive activity in spontaneously hypertensive rats. Peptides 2010, 31, 482–488. [Google Scholar]
- Dostal, D.E.; Baker, K.M. The cardiac rennin-angiotensin system conceptual, or a regulator of cardiac function? Circ. Res. 1999, 85, 643–650. [Google Scholar]
- Vermeirssen, V.; van Camp, J.; Verstraete, W. Optimisation and validation of an angiotensin-converting enzyme inhibition assay for the screening of bioactive peptides. J. Biochem. Biophys. Meth. 2002, 51, 75–87. [Google Scholar]
- Fang, H.; Luo, M.; Sheng, Y.; Li, Z.X.; Wu, Y.Q.; Liu, C. The antihypertensive effect of peptides: A novel alternative to drugs? Peptides 2008, 20, 1062–1071. [Google Scholar]
- Masuda, O.; Nakamura, Y.; Takano, T. Antihypertensive peptides are present in aorta after oral administration of sour milk containing these peptides to spontaneously hypertensive rats. Nutrition 1996, 126, 3063–3068. [Google Scholar]
- Van der Pijl, P.C.; Kies, A.K.; Ten Have, G.A.; Duchateau, G.S.; Deutz, N.E. Pharmacokinetics of proline-rich tripeptides in the pig. Peptides 2008, 29, 2196–2202. [Google Scholar]
- Unger, T.H.; Ganten, D.; Lang, R.E.; Schölkens, B.A. Persistent tissue converting enzyme inhibition following chronic treatment with Hoe498 and MK421 in spontaneously hypertensive rats. J. Cardiovasc. Pharmacol. 1985, 7, 36–41. [Google Scholar]
- Miguel, M.; Contreras, M.M.; Recio, I.; Aleixandre, A. ACE-inhibitory and antihypertensive properties of a bovine casein hydrolysate. Food Chem. 2009, 112, 211–214. [Google Scholar]
- Matsui, T.; Imamura, M.; Oka, H.; Osajima, K.; Kimoto, K.I.; Kawasaki, T.; Matsumoto, K. Tissue distribution of antihypertensive dipeptide, Val-Tyr, after its single oral administration to spontaneously hypertensive rats. J. Peptide Sci. 2004, 10, 535–545. [Google Scholar]
- Sadjadi, J.; Kramer, G.L.; Yu, C.H.; Welborn, M.B.; Chappell, M.C.; Modrall, J.G. Angiotensin converting enzyme-independent angitotensin II production by chymase is up-regulated in the ischemic kidney in renovascular hypertension. J. Surg. Res. 2005, 127, 65–69. [Google Scholar]
- Samples Availability: Available from the authors.
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Zhuang, Y.; Sun, L.; Zhang, Y.; Liu, G. Antihypertensive Effect of Long-Term Oral Administration of Jellyfish (Rhopilema esculentum) Collagen Peptides on Renovascular Hypertension. Mar. Drugs 2012, 10, 417-426. https://doi.org/10.3390/md10020417
Zhuang Y, Sun L, Zhang Y, Liu G. Antihypertensive Effect of Long-Term Oral Administration of Jellyfish (Rhopilema esculentum) Collagen Peptides on Renovascular Hypertension. Marine Drugs. 2012; 10(2):417-426. https://doi.org/10.3390/md10020417
Chicago/Turabian StyleZhuang, Yongliang, Liping Sun, Yufeng Zhang, and Gaoxiang Liu. 2012. "Antihypertensive Effect of Long-Term Oral Administration of Jellyfish (Rhopilema esculentum) Collagen Peptides on Renovascular Hypertension" Marine Drugs 10, no. 2: 417-426. https://doi.org/10.3390/md10020417
APA StyleZhuang, Y., Sun, L., Zhang, Y., & Liu, G. (2012). Antihypertensive Effect of Long-Term Oral Administration of Jellyfish (Rhopilema esculentum) Collagen Peptides on Renovascular Hypertension. Marine Drugs, 10(2), 417-426. https://doi.org/10.3390/md10020417