The Effect of Eating Sea Cucumber Jelly on Candida Load in the Oral Cavity of Elderly Individuals in a Nursing Home

Abstract
:1. Introduction
2. Results
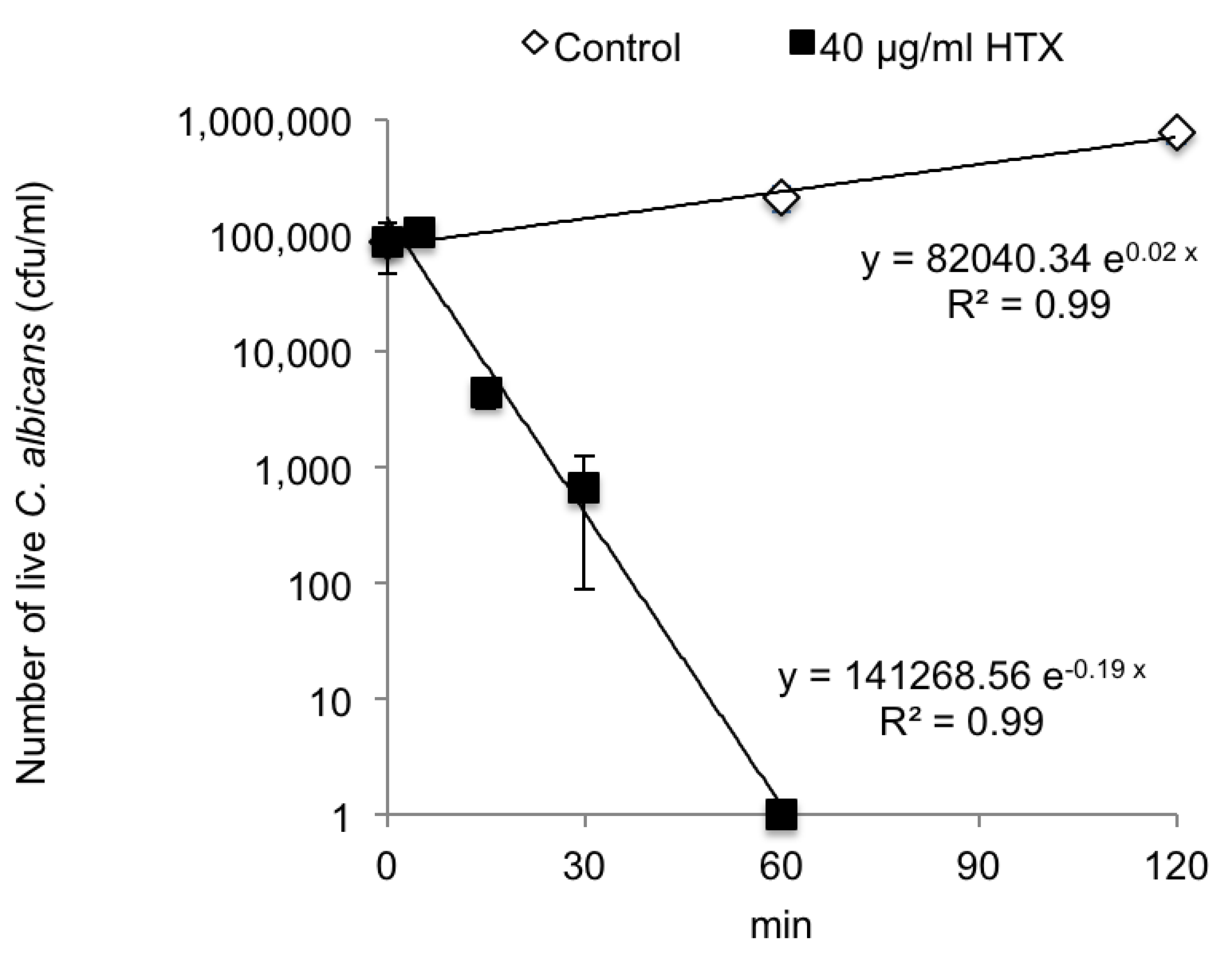
2.1. Antifungal Activities of S. japonicus Holotoxins

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Strain | MIC (µg/mL) |
|---|---|
| Candida albicans SC5314 | 7.0 ± 2.0 |
| C. albicans JCM1542 | 7.0 ± 2.0 |
| C. tropicalis JCM1541 | 14.0 ± 4.0 |
| C. glabrata JCM3761 | 7.0 ± 2.0 |
| C. parapsilosis JCM1612 | 8.0 ± 0.0 |
| C. krusei JCM1609 | 16.0 ± 0.0 |

| Strain | MIC (µg/mL) |
|---|---|
| Candida albicans | |
| SI_1 | 4.0 ± 0.0 |
| SI_2 | 4.0 ± 0.0 |
| SI_3 | 4.0 ± 0.0 |
| SI_4 | 4.0 ± 0.0 |
| SI_5 | 2.7 ± 2.3 |
| SI_6 | 5.7 ± 4.0 |
| Candida glabrata | |
| SI_11 | 10.7 ± 4.6 |
| SI_12 | 8.0 ± 0.0 |
| SI_13 | 10.7 ± 4.6 |
| SI_14 | 10.7 ± 4.6 |
| SI_15 | 13.3 ± 4.6 |
| SI_16 | 8.0 ± 0.0 |

| HTX Fraction a | MIC of Each Fraction (µg/mL) b | A Compound Detected in Each Peak (Molecular Mass) c |
|---|---|---|
| Containing peak 1 | 4.0 ± 0.0 | 1431.63 |
| Containing peak 2 | 4.0 ± 0.0 | 1445.65 |
| Containing peak 3 | 2.7 ± 1.2 | 1415.64 |
2.2. Antifungal Activity of the Hydrolysate of S. japonicus
| Deduced Concentration of Each Peak Fraction in the Hydrolysate (µg/mL) a | A Compound Detected in the Peak of the Hydrolysate (Molecular Mass) b | |
|---|---|---|
| Peak 1 | 44.0 | 1431.63 |
| Peak 2 | 51.0 | 1445.65 |
| Peak 3 | 263 | 1415.64 |
| Sample | MIC (µg/mL) |
|---|---|
| The hydrolysate | 6.25 ± 0.0 (×103) |
| The jelly | 12.5 ± 0.0 (×103) |
| HTX | 7.0 ± 2.0 |
| Amphotericin B | 0.4 ± 0.1 |
| Miconazole | 0.3 ± 0.2 |
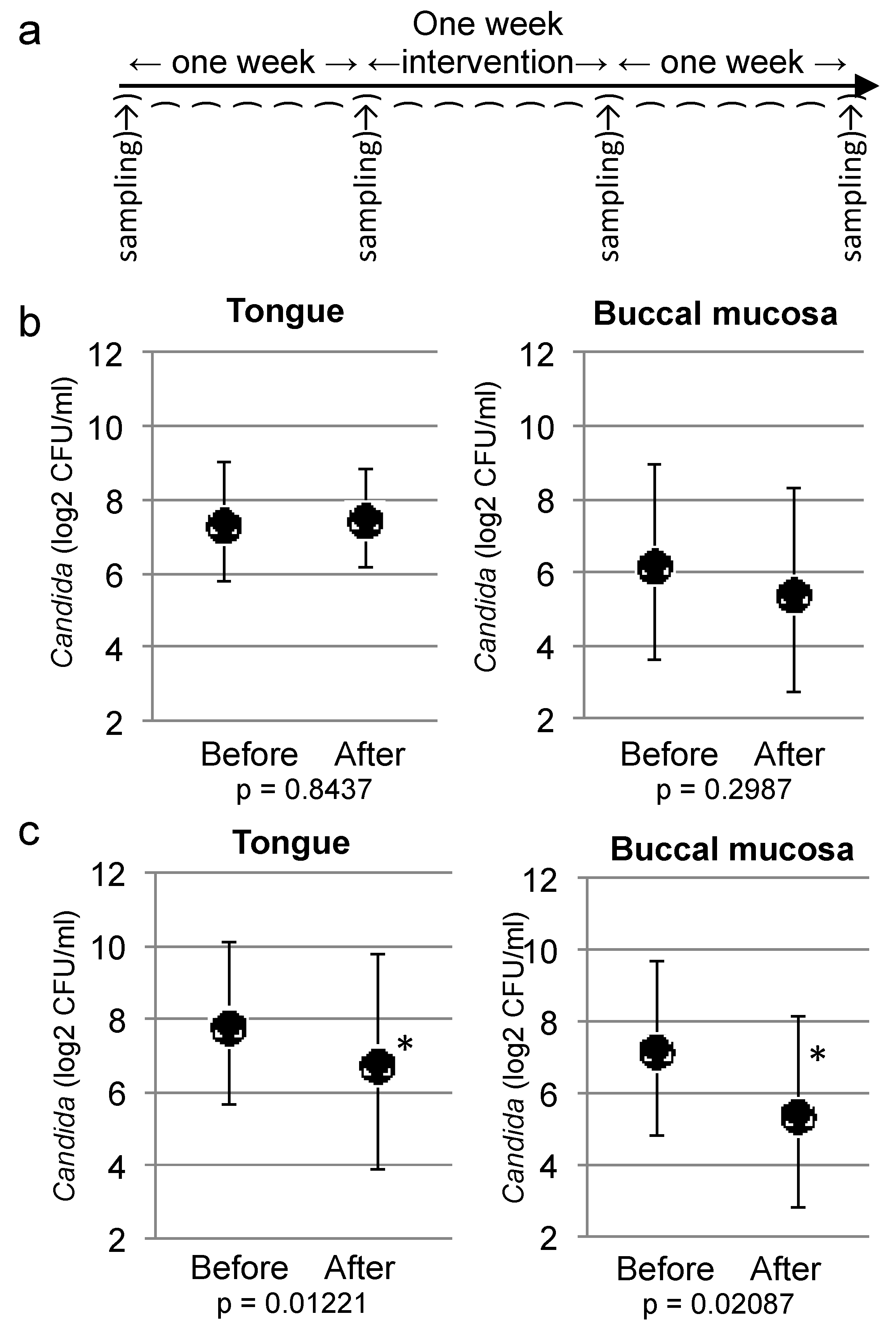
2.3. Double-Blind Randomized Controlled Study


3. Discussion
4. Experimental Section
4.1. Fungal Strains
4.2. Antifungal Activities of Holotoxin
4.3. Preparation and Analysis of S. japonicus Hydrolysate
4.4. S. japonicus Jelly
4.5. Participants
4.6. Sampling and Measurement of Oral Candida
4.7. Interventions
4.8. Statistical Analysis
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Cheng, S.C.; Joosten, L.A.B.; Kullberg, B.J.; Netea, M.G. Interplay between Candida albicans and the mammalian innate host defense. Infect. Immun. 2012, 80, 1304–1313. [Google Scholar] [CrossRef]
- Wisplinghoff, H.; Bischoff, T.; Tallent, S.M.; Seifert, H.; Wenzel, R.P.; Edmond, M.B. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Clin. Infect. Dis. 2004, 39, 309–317. [Google Scholar] [CrossRef]
- Vazquez, J.A. Optimal management of oropharyngeal and esophageal candidiasis in patients living with HIV infection. HIV AIDS 2010, 2, 89–101. [Google Scholar]
- Dongari-Bagtzoglou, A.; Dwivedi, P.; Ioannidou, E.; Shaqman, M.; Hull, D.; Burleson, J. Oral Candia infection and colonization in solid organ transplant recipients. Oral Microbiol. Immunol. 2009, 24, 249–254. [Google Scholar] [CrossRef]
- Lalla, R.V.; Latortue, M.C.; Hong, C.H.; Ariyawardana, A.; D’Amato-Palumbo, S.; Fischer, D.J.; Martof, A.; Nicolatou-Galitis, O.; Patton, L.L.; Elting, L.S.; et al.; Fungal Infections Section, Oral Care Study Group, Multinational Association of Supportive Care in Cancer (MASCC)/International Society of Oral Oncology (ISOO) A systematic review of oral fungal infections in patients receiving cancer therapy. Support. Care Cancer 2010, 18, 985–992. [Google Scholar] [CrossRef]
- Liu, L.J.; Xiao, W.; He, Q.B.; Jiang, W.W. Generic and oral quality of life is affected by oral mucosal diseases. BMC Oral Health 2012, 12, 1–6. [Google Scholar] [CrossRef]
- Maza, J.L.; Elguezabal, N.; Prado, C.; Ellacuria, J.; Soler, I.; Ponton, J. Candida albicans adherence to resin-composite restorative dental material: Influence of whole human saliva. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 94, 589–592. [Google Scholar] [CrossRef]
- Narhi, T.O.; Ainamo, A.; Meurman, J.H. Salivary yeasts, saliva, and oral mucosa in the elderly. J. Dent. Res. 1993, 72, 1009–1014. [Google Scholar] [CrossRef]
- Torres, S.R.; Peixoto, C.B.; Caldas, D.M.; Silva, E.B.; Akiti, T.; Nucci, M.; Uzeda, M. Relationship between salivary flow rates and Candida counts in subjects with xerostomia. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 93, 149–154. [Google Scholar] [CrossRef]
- Ueda, K.; Toyosato, A.; Nomura, S. A study on the effects of short-, medium- and long-term professional oral care in elderly persons requiring long-term nursing care at a chronic or maintenance stage of illness. Gerodontology 2003, 20, 50–56. [Google Scholar]
- Ishihara, K.; Adachi, M.; Eguchi, J.; Washizu, M.; Kosugi, M.; Okuda, K. Prevalence of Staphylococcus species and Candida albicans in the oral cavities of elderly who require daily care in a nursing home. Bull. Tokyo dent. Coll. 2000, 41, 169–174. [Google Scholar] [CrossRef]
- de Rsende, M.A.; de Sousa, L.V.; de Oliveira, R.C.; Koga-Ito, C.Y.; Lyon, J.P. Prevalence and antifungal susceptibility of yeasts obtained from the oral cavity of elderly individuals. Mycopathologia 2006, 162, 39–44. [Google Scholar] [CrossRef]
- Annual Report on the Aging Society: 2012; Cabinet Office: Tokyo, Japan, 2012.
- Akamine, J. The status of the sea cucumber fisheries and trade in Japan: past and present. In Advances in Sea Cucumber Aquaculture and Management; Lovatelli, A., Ed.; Food Agriculture Organization United Nations: Rome, Italy, 2004; pp. 39–47. [Google Scholar]
- Bordbar, S.; Anwar, F.; Saari, N. High-value components and bioactives from sea cucumbers for functional foods—a review. Mar. Drugs 2011, 9, 1761–1805. [Google Scholar] [CrossRef]
- Shimada, S. Antifungal steroid glycoside from sea cucumber. Science 1969, 163, 1462. [Google Scholar]
- Kalinin, V.I.; Aminin, D.L.; Avilov, S.A.; Silchenko, A.S.; Stonik, V.A. Triterpene glycosides from sea cucumbers (holothurioidea, echinodermata). Biological activities and functions. Stud. Nat. Prod. Chem. 2008, 35, 135–196. [Google Scholar] [CrossRef]
- Shin, J.H.; Nolte, F.S.; Holloway, B.P.; Morrison, C.J. Rapid identification of up to three Candida species in a single reaction tube by 5′ exonuclease assay using fluorescent DNA probes. J. Clin. Microbiol. 1999, 37, 165–170. [Google Scholar]
- Shinozaki, S.; Moriyama, M.; Hayashida, J.N.; Tanaka, A.; Maehara, T.; Ieda, S.; Nakamura, S. Close association between oral Candida species and oral mucosal disorders in patients with xerostomia. Oral Dis. 2012, 18, 667–672. [Google Scholar] [CrossRef]
- Kitagawa, I.; Yamanaka, H.; Kobayashi, M.; Nishino, T.; Yoshioka, I.; Sugawara, T. Saponin and sapogenol. XXVII. Revised structures of holotoxin A and holotoxin B, two antifungal oligoglycosides from the sea cucumber Stichopus japonicas SELENKA. Chem. Pharm. Bull. 1978, 26, 3722–3731. [Google Scholar] [CrossRef]
- Maltsev, I.I.; Stonik, V.A.; Kalinovsky, A.I.; Elyakov, G.B. Triterpene glycosides from sea cucumber Stichopus japonicus SELENKA. Comp. Biochem. Physiol. 1984, 78, 421–426. [Google Scholar]
- Hancock, P.J.; Epstein, J.B.; Sadler, G.R. Oral and dental management related to radiation therapy for head and neck cancer. J. Can. Dent. Assoc. 2003, 69, 585–590. [Google Scholar]
- Peterson, D.E.; Bensadoun, R.J.; Roila, F. Management of oral and gastrointestinal mucositis: ESMO clinical practice guidelines. Ann. Oncol. 2011, 22, vi78–vi84. [Google Scholar]
- Yamaguchi, H.; Enomoto, S.; Kaku, M.; Sakamaki, H.; Tanaka, K.; Yoshida, M. An open randomized parallel-comparison study of itraconazole oral solution versus itraconazole capsules in treatment of patients with oropharyngeal candidiasis. Jpn. J. Chemother. 2006, 54, 18–31. [Google Scholar]
- Lee, H.E.; Li, C.Y.; Chang, H.W.; Yang, Y.H.; Wu, J.H. Effects of different denture cleaning methods to remove Candida albicans from acrylic resine denture based material. J. Dent. Sci. 2011, 6, 216–220. [Google Scholar]
- Bergsson, G.; Arnfinnsson, J.; Steingrimsson, O.; Thormar, H. In vitro killing of Candida albicans by fatty acids and monoglycerides. Antimicrob. Agents Chemother. 2001, 45, 3209–3212. [Google Scholar] [CrossRef]
- Pfaller, M.A.; Sheehan, D.J.; Rex, J.H. Determination of fungicidal activities against yeasts and molds: Lessons learned from bactericidal testing and the need for standardization. Clin. Microbiol. Rev. 2004, 17, 268–280. [Google Scholar] [CrossRef]
- Saito, M.; Kunisaki, N.; Urano, N.; Kimura, S. Collagen as the major component of sea cucumber (Stichopus japonicus). J. Food Sci. 2002, 67, 1319–1322. [Google Scholar] [CrossRef]
- Okawa, T.; Yamaguchi, Y.; Takada, S.; Sakai, Y.; Numata, N.; Nakamura, F.; Nagashima, Y.; Ikezawa, Z.; Aihara, M. Oral administration of collagen tripeptide improves the dryness and pruritus in the acetone-induced dry skin model. J. Dematol. Sci. 2012, 66, 136–143. [Google Scholar]
- Clinical and Laboratory Standards Institute (CLSI). Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeast; Approved Standard, 3rd ed.; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2008. [Google Scholar]
- Dyck, S.V.; Caulier, G.; Todesco, M.; Gerbaux, P.; Fournier, I.; Wisztoeski, M.; Flammang, P. The triterpene glycosides of Holothuria forskali: usefulness and efficiency as a chemical defense mechanism against predatory fish. J. Exp. Biol. 2011, 214, 1347–1356. [Google Scholar] [CrossRef]
- Dyck, S.V.; Gerbaux, P.; Flammang, P. Qualitative and quantitative saponin contents in five sea cucumbers from the Indian ocean. Mar. Drugs 2010, 8, 173–189. [Google Scholar] [CrossRef]
- Madl, T.; Sterk, H.; Mittelbach, M.; Rechberger, G.N. Tandem mass spectrometric analysis of a complex triterpene saponin mixture of Chenopodium quinoa. J. Am. Soc. Mass Spectrom. 2006, 17, 795–806. [Google Scholar] [CrossRef]
- R: A language and environment for statistical computing. Available online: http://www.lsw.uni-heidelberg.de/users/christlieb/teaching/UKStaSS10/R-refman.pdf (accessed on 31 May 2010).
Supplementary Files
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Yano, A.; Abe, A.; Aizawa, F.; Yamada, H.; Minami, K.; Matsui, M.; Kishi, M. The Effect of Eating Sea Cucumber Jelly on Candida Load in the Oral Cavity of Elderly Individuals in a Nursing Home. Mar. Drugs 2013, 11, 4993-5007. https://doi.org/10.3390/md11124993
Yano A, Abe A, Aizawa F, Yamada H, Minami K, Matsui M, Kishi M. The Effect of Eating Sea Cucumber Jelly on Candida Load in the Oral Cavity of Elderly Individuals in a Nursing Home. Marine Drugs. 2013; 11(12):4993-5007. https://doi.org/10.3390/md11124993
Chicago/Turabian StyleYano, Akira, Akiko Abe, Fumie Aizawa, Hidetoshi Yamada, Kentaro Minami, Miki Matsui, and Mitsuo Kishi. 2013. "The Effect of Eating Sea Cucumber Jelly on Candida Load in the Oral Cavity of Elderly Individuals in a Nursing Home" Marine Drugs 11, no. 12: 4993-5007. https://doi.org/10.3390/md11124993
APA StyleYano, A., Abe, A., Aizawa, F., Yamada, H., Minami, K., Matsui, M., & Kishi, M. (2013). The Effect of Eating Sea Cucumber Jelly on Candida Load in the Oral Cavity of Elderly Individuals in a Nursing Home. Marine Drugs, 11(12), 4993-5007. https://doi.org/10.3390/md11124993