A Systematic Review of Peer-Support Programs for Smoking Cessation in Disadvantaged Groups



Abstract
:1. Introduction
2. Experimental Section
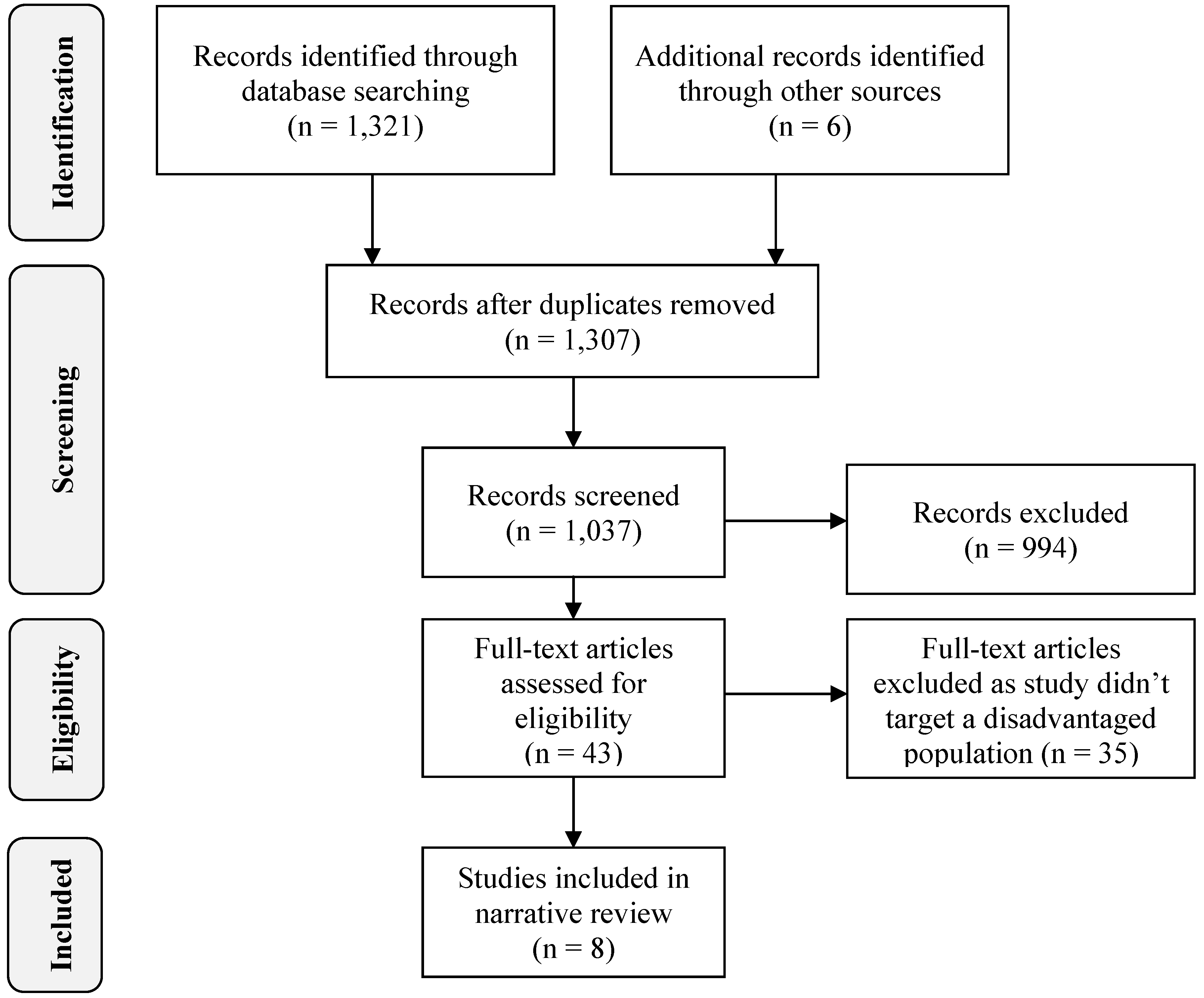
2.1. Search Strategy
2.2. Selection of Studies

2.3. Review Format and Criteria

{kind=link}
{kind=link}
| Author, Year, Country | Study Population | Intervention | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Description of smokers | n | Mean or Median Age (year) | Baseline smoking | Duration | Design | Peers/Partners | Intervention integrity | Length of follow up (% followed-up) | Behaviour change | Summary Efficacy Score | |
| Albrecht et al. 2006, USA [29] | Pregnant adolescents (14–19y) from low socio-economic areas; 53% Caucasian; 42% African American; 5% other | 142 | 17 | UC = 6.76cpd TFS = 7.04cpd TFSB = 7.31cpd | 8 weeks | Usual Care (UC) = 45–60 min individual education session and written materials Teen Fresh Start (TFS) = 8 group sessions Teen Fresh Start plus Buddy (TFSB) = TFS + participants required to identify and bring a peer supporter to sessions | Peer supporters were non-smoking females of similar age identified by the participants. No peer training. | Nurses certified in intervention delivery Participant’s attendance at meeting recorded. Intervention exposure not clearly reported. | 1year (53%) | Abstinence at 8wks: TFSB vs. UC (p = 0.01); no differences at 1year. Low power reported. OR(8 wks) = 3.730 | 1 |
| Hennrikus et al. 2010, USA [30] | Low income pregnant women who smoked aged 18+; 67% racial minority/Hispanic; 65% had a high school education or less 48% married/de facto | 82 | 24 | Median = 5cpd; 52% smoked first cigarette within 30 min of waking | Variable depending on due date (approx. 6 months) | Participants identified a woman in their social network to help them quit. Dyads were then randomized to intervention or control groups. Intervention: supporters received monthly contacts from counselor Control: supporters not contacted | Supporter session discussed activities to support participant’s quit efforts; monthly calls reviewed support efforts and planned for next month 52% of supporters were current smokers, 22% were former smokers | Participant attendance recorded Intervention exposure > 89% | 3 months pp (68%) | Abstinence at birth: intervention 13.0%; control 3.6%. Abstinence at 3 months pp: intervention 9.3%; control 0%. No statistically significant differences. Participants with friends as supporters more likely to quit (21.7%) than with relatives (6.5%); and more quits when supporters were ex-smokers (18.2%) than never (13.3%) or current (10.7%) smokers. Low power reported. OR unable to be calculated due to small numbers | 0 |
| McBride et al. 2004, USA [31] | Pregnant women who smoked and recent quitters at an army medical centre living with a partner; 77% Caucasian; 50% employed; 52% more than high school education | 583 | 24 | Mean = 13cpd; 33% smoked first cigarette within 30 min of waking | Variable depending on due date (approx. 10 months) | Usual Care (UC): advice at prenatal visit to quit smoking + self-help guide; Woman Only (WO): UC + late pregnancy relapse prevention kit and six counseling calls completed by 4 moths postpartum; Partner Assisted (PA): WO + partner adjunct in which partner advised how to be a quit coach. | Partner training covered helpful/unhelpful behaviours, partners also given assistance to quit if they smoked. | Intervention exposure = Number of counselling calls reported Self-report of partner interaction by woman and support partner Intervention exposure not clearly reported. | 1year pp (75%) | Abstinence at 28 weeks of pregnancy UC 60%, WO 59%, PA 61%; Abstinence at 2 months pp UC 38%, WO 37%, PA 42%; Abstinence at 6 months pp UC 33%, WO 36%, PA 37%; Abstinence at 12 months pp UC 29%, WO 32%, PA 35%; Sustained abstinence: UC 15%, WO 20%, PA 21%. No statistically significant differences. No power analysis reported. OR(2 months pp) = 1.186 | 0 |
| Solomon et al. 2000a, USA [32] | Pregnant women, mostly Caucasian, English speaking, low income, low education | 151 | 23.5 | Mean = 10.5cpd (intervention); 9.8cpd (control) | Variable depending on due date (approx. 6 months) | Control: brief advice at first 3 pre-natal visits + printed materials. Intervention: Control + offer of telephone peer support for women with moderate or high intentions to quit during pregnancy | Peer supporter (woman ex-smoker) received 8h training | Number and duration of support calls recorded Quality control checks conducted on women in intervention group Intervention exposure > 80% | End of pregnancy (approx. 6 months) (73%) | Abstinence at end of pregnancy: intervention 19%; control 17%. No statistically significant differences. Low power reported. OR(pp) = 1.273 | 0 |
| Solomon et al. 2000b, USA [33] | Low income women | 214 | 33 | Mean = 23.7cpd | 3 months | Control: free nicotine patches Intervention: free nicotine patches + pro-active telephone peer support | Peer supporter (woman ex-smoker) received 7 h training | Phone support personnel trained Intervention exposure = 53% | 6 months (90%) | Abstinence at 3 months: intervention 42%; control 28% (p = 0.03). At 6 months, no significant difference. No power analysis reported. OR(3 months) = 1.845 | 2 |
| Solomon et al. 2005, USA [34] | Low income women | 330 | 33.7 (intervention) 34.8 (control) | Mean = 23.6cpd | 4 months | Control: free nicotine patches Intervention: free nicotine patches + pro-active telephone peer support | Peer supporter (woman ex-smoker) received 8h training | Number and duration of support calls recorded Intervention exposure~70% | 6 months (87%) | Abstinence at 3 months: intervention 42.7%; control 26.4% (p = 0.002). At 6 months, no significant difference. Power = 0.40. OR(3 months) = 2.075 | 2 |
| West et al. 1998, UK [35] | Economically and socially disadvantaged | 172 | 42.6 (intervention) 44.5 (control) | FTND = 4.9 (intervention); 5.1 (control) | 5 weeks | Control: brief intervention + NRT Intervention: brief intervention + NRT + buddy (paired with another smoker participant) | No peer training (participants were paired with each other) | Level of buddy interaction and use of pharmacotherapy self-reported Intervention exposure = 85% | 5 weeks (nr) | Abstinence at end of intervention: intervention 27%; control 12% (p < 0.01). Low power reported. OR(5 weeks) = 2.794 | 1 |
| Williams et al. 2011 [36] | People with mental illness (outpatients) | 102 | 43.5 | Mean = 19cpd | One off 20 min brief intervention | Pre post study design. Intervention: 20min brief intervention with peer counsellor | Peer counselors are mental health consumers with a min 1year tobacco-free period who receive 30 h intensive training and a detailed training manual. | Weekly phone and face to face supervision and feedback to peer counsellours. Monitoring of number of visits, events and smokers receiving intervention. Intervention exposure = 100% | 6 months (59%) | Reduction in cpd at 1 month (p < 0.001) compared with baselineReduction in cpd at 6 months (p = 0.001) compared with baseline | 2 |
3. Results and Discussion
3.1. Study Populations
3.2. Efficacy
3.3. Intervention Design
3.4. Peer Selection and Training
3.5. Theoretical Frameworks
3.6. Methodological Quality

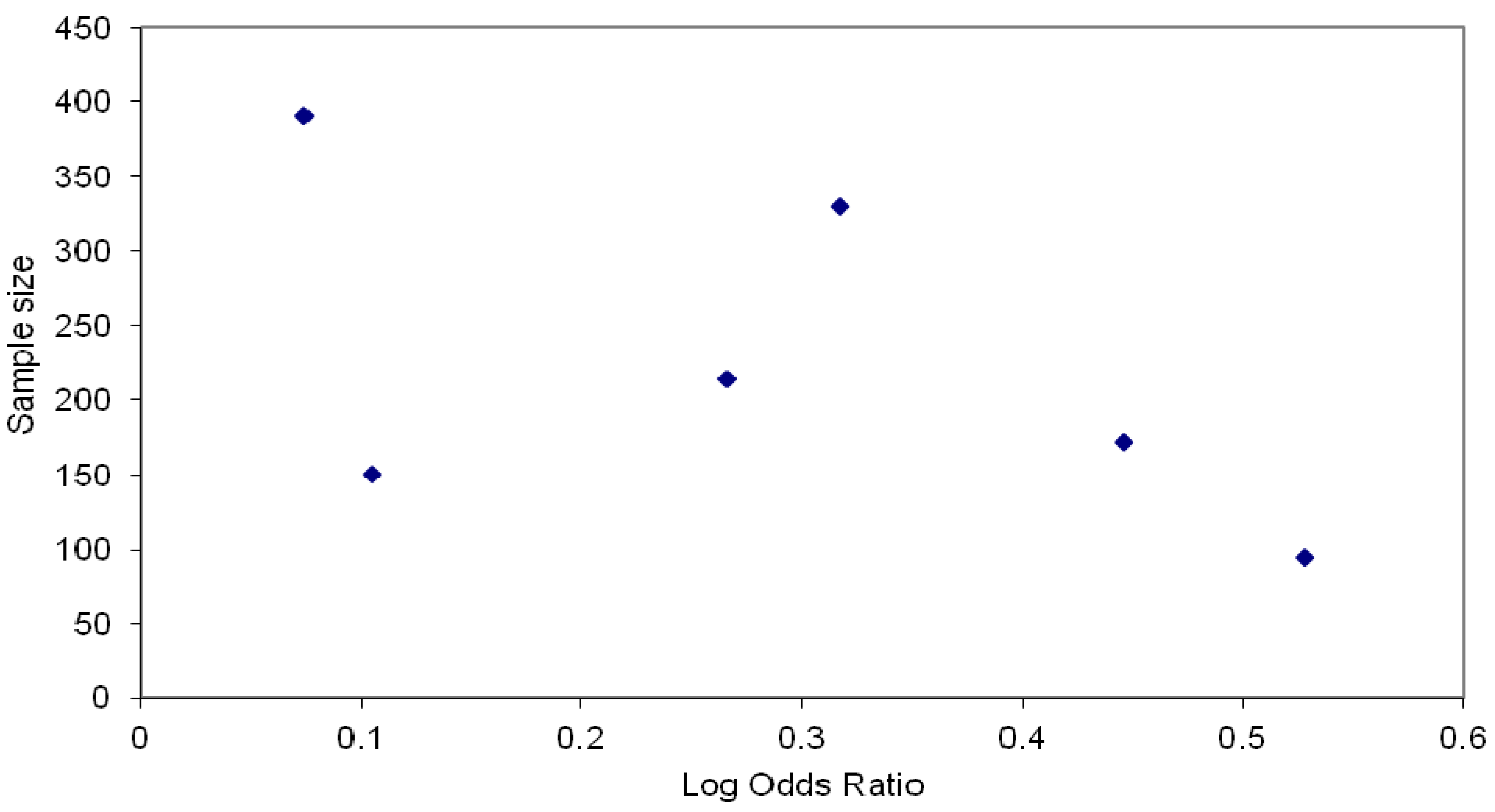
3.7. Publication Bias
4. Conclusions
Conflicts of Interest
Appendix 1
- smoking.ti,ab
- tobacco.ti,ab.
- 1 OR 2
- cessation.ti,ab
- peer*.ti,ab.
- social support*.ti,ab.
- social network*.ti,ab.
- 5 OR 6 OR 7
- 3 AND 4 AND 8
- smoking cessation/
- social support/
- 9 AND 10 AND 11
References
- Stockings, E.; Bowman, J.; McElwaine, K.; Baker, A.; Terry, M.; Clancy, R.; Bartlem, K.; Wye, P.; Bridge, P.; Knight, J.; et al. Readiness to quit smoking and quit attempts among Australian mental health inpatients. Nicotine Tob. Res. 2013, 15, 942–949. [Google Scholar] [CrossRef]
- Thomas, D. National trends in Aboriginal and Torres Strait Islander smoking and quitting, 1994–2008. Aust. N. Z. J. Public Health 2012, 36, 24–29. [Google Scholar] [CrossRef]
- Tsai, J.; Rosenheck, R.A. Smoking among chronically homeless adults: Prevalence and correlates. Psychiatr. Serv. 2012, 63, 569–576. [Google Scholar] [CrossRef]
- Apollonio, D.E.; Malone, R.E. Marketing to the marginalised: Tobacco industry targeting of the homeless and mentally ill. Tob. Control 2005, 14, 409–415. [Google Scholar] [CrossRef]
- DiGiacomo, M.; Davidson, P.M.; Abbott, P.A.; Davison, J.; Moore, L.; Thompson, S.C. Smoking cessation in indigenous populations of Australia, New Zealand, Canada, and the United States: Elements of effective interventions. Int. J. Environ. Res. Public Health 2011, 8, 388–410. [Google Scholar] [CrossRef]
- Christakis, N.A.; Fowler, J.H. The spread of obesity in a large social network over 32 years. N. Engl. J. Med. 2007, 357, 370–379. [Google Scholar] [CrossRef]
- Hammond, R.A. Social influence and obesity. Curr. Opin. Endocrinol. Diabetes Obes. 2010, 17, 467–471. [Google Scholar] [CrossRef]
- Christakis, N.A.; Fowler, J.H. The collective dynamics of smoking in a large social network. N. Engl. J. Med. 2008, 358, 2249–2258. [Google Scholar] [CrossRef]
- Johnston, V.; Thomas, D. Smoking behaviours in a remote Australian Indigenous community: The influence of family and other factors. Soc. Sci. Med. 2008, 67, 1708–1716. [Google Scholar] [CrossRef]
- Bond, C.; Brough, M.; Spurling, G.; Hayman, N. ‘It had to be my choice’ Indigenous smoking cessation and negotiations of risk, resistance and resilience. Health Risk Soc. 2012, 14, 565–581. [Google Scholar] [CrossRef] [Green Version]
- Clay, S.; Schell, B.; Corrigan, P.W.; Ralph, R.O. On Our Own, Together: Peer Programs for People with Mental Illness; Vanderbilt University Press: Nashville, TN, USA, 2005; pp. 141–178. [Google Scholar]
- Solomon, P. Peer support/peer provided services underlying process, benefits, and critical ingredients. Psychiatr. Rehabil. J. 2004, 27, 392–401. [Google Scholar] [CrossRef]
- Davidson, L.; Chinman, M.; Kloos, B.; Weingarten, R.; Stayner, D.; Tebes, J.K. Peer support among individuals with severe mental illness: A review of the evidence. Clin. Psychol. 1999, 6, 165–187. [Google Scholar]
- Heisler, M. Overview of peer support models to improve diabetes self-management and clinical outcomes. Diabetes Spectr. 2007, 20, 214–221. [Google Scholar] [CrossRef]
- Dale, J.R.; Williams, S.M.; Bowyer, V. What is the effect of peer support on diabetes outcomes in adults? A systematic review. Diabet Med. 2012, 29, 1361–1377. [Google Scholar] [CrossRef]
- Boisvert, R.A.; Martin, L.M.; Grosek, M.; Clarie, A.J. Effectiveness of a peer-support community in addiction recovery: Participation as intervention. Occup. Ther. Int. 2008, 15, 205–220. [Google Scholar] [CrossRef]
- Webel, A.R.; Okonsky, J.; Trompeta, J.; Holzemer, W.L. A systematic review of the effectiveness of peer-based interventions on health-related behaviors in adults. Am. J. Public Health 2010, 100, 247–253. [Google Scholar] [CrossRef]
- Paasse, G.; Adams, K. Working together as a catalyst for change: The development of a peer mentoring model for the prevention of chronic disease in Australian Indigenous communities. Aust. J. Primary Health 2011, 17, 214–219. [Google Scholar] [CrossRef]
- Salzer, M.S.; Shoshanna, S.L. Identifying consumer-provider benefits in evaluations of consumer-delivered services. Psychiatr. Rehabil. J. 2002, 25, 281–288. [Google Scholar] [CrossRef]
- Ranney, L.; Melvin, C.; Lux, L.; McClain, E.; Lohr, K.N. Systematic review: Smoking cessation intervention strategies for adults and adults in special populations. Ann. Intern. Med. 2006, 145, 845–856. [Google Scholar] [CrossRef]
- May, S.; West, R. Do social support interventions (“buddy systems”) aid smoking cessation? A review. Tob. Control 2000, 9, 415–422. [Google Scholar] [CrossRef]
- Westmaas, J.L.; Bontemps-Jones, J.; Bauer, J.E. Social support in smoking cessation: Reconciling theory and evidence. Nicotine Tob. Res. 2010, 12, 695–707. [Google Scholar] [CrossRef]
- Park, E.W.; Tudiver, F.; Schultz, J.K.; Campbell, T. Does enhancing partner support and interaction improve smoking cessation? A meta-analysis. Ann. Family Med. 2004, 2, 170–174. [Google Scholar] [CrossRef]
- McKay, C.E.; Dickerson, F. Peer supports for tobacco cessation for adults with serious mental illness: A review of the literature. J. Dual. Diagn. 2012, 8, 104–112. [Google Scholar] [CrossRef]
- Flaskerud, J.H.; Lesser, J.; Dixon, E.; Anderson, N.; Conde, F.; Kim, S.; Koniak-Griffin, D.; Strehlow, A.; Tullmann, D.; Verzemnieks, I. Health disparities among vulnerable populations: Evolution of knowledge over five decades in Nursing Research publications. Nurs. Res. 2002, 51, 74–85. [Google Scholar] [CrossRef]
- Najman, J.M.; Lanyon, A.; Andersen, M.; Williams, G.; Bor, W.; O’Callaghan, M. Socioeconomic status and maternal cigarette smoking before, during and after a pregnancy. Aust. N. Z. J. Public Health 1998, 22, 60–66. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef]
- Jackson, N. Handbook: Systematic Reviews of Health Promotion and Public Health Interventions; Cochrane Health Promotion and Public Health Field and the Victorian Health Promotion Foundation: Melbourne, Australia, 2007. [Google Scholar]
- Albrecht, S.A.; Caruthers, D.; Patrick, T.; Reynolds, M.; Salamie, D.; Higgins, L.W.; Braxter, B.; Kim, Y.; Mlynarchek, S. A randomized controlled trial of a smoking cessation intervention for pregnant adolescents. Nurs. Res. 2006, 55, 402–410. [Google Scholar] [CrossRef]
- Hennrikus, D.; Pirie, P.; Hellerstedt, W.; Lando, H.A.; Steele, J.; Dunn, C. Increasing support for smoking cessation during pregnancy and postpartum: Results of a randomized controlled pilot study. Prev. Med. 2010, 50, 134–137. [Google Scholar] [CrossRef]
- McBride, C.M.; Baucom, D.H.; Peterson, B.L.; Pollak, K.I.; Palmer, C.; Westman, E.; Lyna, P. Prenatal and postpartum smoking abstinence—A partner-assisted approach. Am. J. Prev. Med. 2004, 27, 232–238. [Google Scholar]
- Solomon, L.J.; Secker-Walker, R.H.; Flynn, B.S.; Skelly, J.M.; Capeless, E.L. Proactive telephone peer support to help pregnant women stop smoking. Tob. Control 2000, 9 (Suppl. 3), III72–III74. [Google Scholar]
- Solomon, L.J.; Scharoun, G.M.; Flynn, B.S.; Secker-Walker, R.H.; Sepinwall, D. Free nicotine patches plus proactive telephone peer support to help low-income women stop smoking. Prev. Med. 2000, 31, 68–74. [Google Scholar] [CrossRef]
- Solomon, L.J.; Marcy, T.W.; Howe, K.D.; Skelly, J.M.; Reinier, K.; Flynn, B.S. Does extended proactive telephone support increase smoking cessation among low-income women using nicotine patches? Prev. Med. 2005, 40, 306–313. [Google Scholar] [CrossRef]
- West, R.; Edwards, M.; Hajek, P. A randomized controlled trial of a “buddy” system to improve success at giving up smoking in general practice. Addiction 1998, 93, 1007–1011. [Google Scholar]
- Williams, J.M.; Dwyer, M.; Verna, M.; Zimmermann, M.H.; Gandhi, K.K.; Galazyn, M.; Szkodny, N.; Molnar, M.; Kley, R.; Steinberg, M.L. Evaluation of the CHOICES program of peer-to-peer tobacco education and advocacy. Community Ment. Health J. 2011, 47, 243–251. [Google Scholar] [CrossRef]
- Su, A.; Buttenheim, A.M. Maintenance of smoking cessation in the postpartum period: Which interventions work best in the long-term? Matern. Child Health J. 2013. [Google Scholar] [CrossRef]
- Mermelstein, R.; Lichtenstein, E.; McIntyre, K. Partner support and relapse in smoking-cessation programs. J. Consult. Clin. Psychol. 1983, 51, 465–466. [Google Scholar] [CrossRef]
- Drummond, M.F. Methods for the Economic Evaluation of Health Care Programmes, 3rd ed.; Oxford University Press: Oxford, UK, 2005; pp. 6–7. [Google Scholar]
- Warburton, J.; Chambers, B. Older Indigenous Australians: Their integral role in culture and community. Aust. J. Ageing 2007, 26, 3–7. [Google Scholar] [CrossRef]
- Adams, K.; Paasse, G.; Clinch, D. Peer-support preferences and readiness-to-change behaviour for chronic disease prevention in an urban indigenous population. Aust. Soc. Work 2011, 64, 55–67. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Ford, P.; Clifford, A.; Gussy, K.; Gartner, C. A Systematic Review of Peer-Support Programs for Smoking Cessation in Disadvantaged Groups. Int. J. Environ. Res. Public Health 2013, 10, 5507-5522. https://doi.org/10.3390/ijerph10115507
Ford P, Clifford A, Gussy K, Gartner C. A Systematic Review of Peer-Support Programs for Smoking Cessation in Disadvantaged Groups. International Journal of Environmental Research and Public Health. 2013; 10(11):5507-5522. https://doi.org/10.3390/ijerph10115507
Chicago/Turabian StyleFord, Pauline, Anton Clifford, Kim Gussy, and Coral Gartner. 2013. "A Systematic Review of Peer-Support Programs for Smoking Cessation in Disadvantaged Groups" International Journal of Environmental Research and Public Health 10, no. 11: 5507-5522. https://doi.org/10.3390/ijerph10115507
APA StyleFord, P., Clifford, A., Gussy, K., & Gartner, C. (2013). A Systematic Review of Peer-Support Programs for Smoking Cessation in Disadvantaged Groups. International Journal of Environmental Research and Public Health, 10(11), 5507-5522. https://doi.org/10.3390/ijerph10115507