A History of Ashes: An 80 Year Comparative Portrait of Smoking Initiation in American Indians and Non-Hispanic Whites—the Strong Heart Study

Abstract
:1. Introduction
2. Methods
2.1. Sample
2.2. Measures: Smoking Status and Age of Initiation
2.3. Analysis
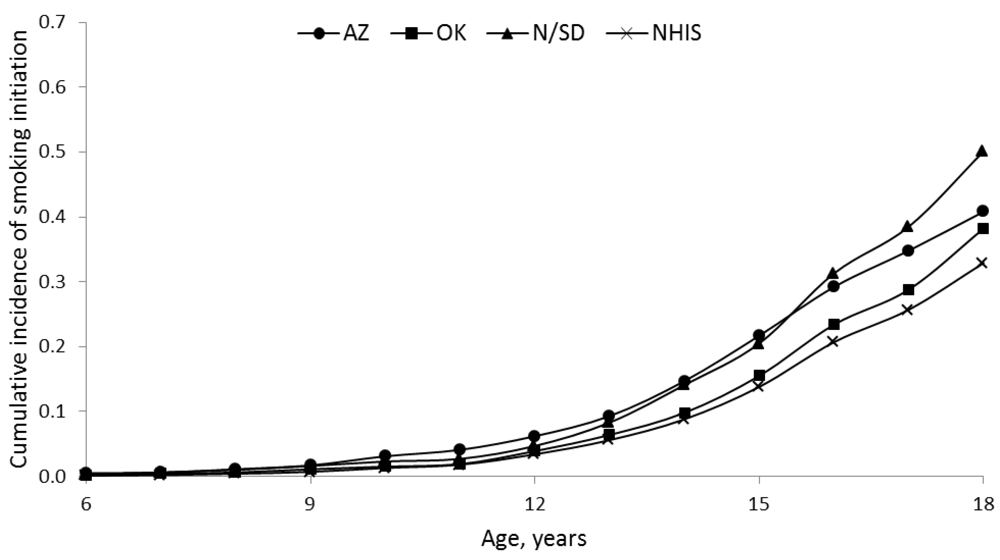
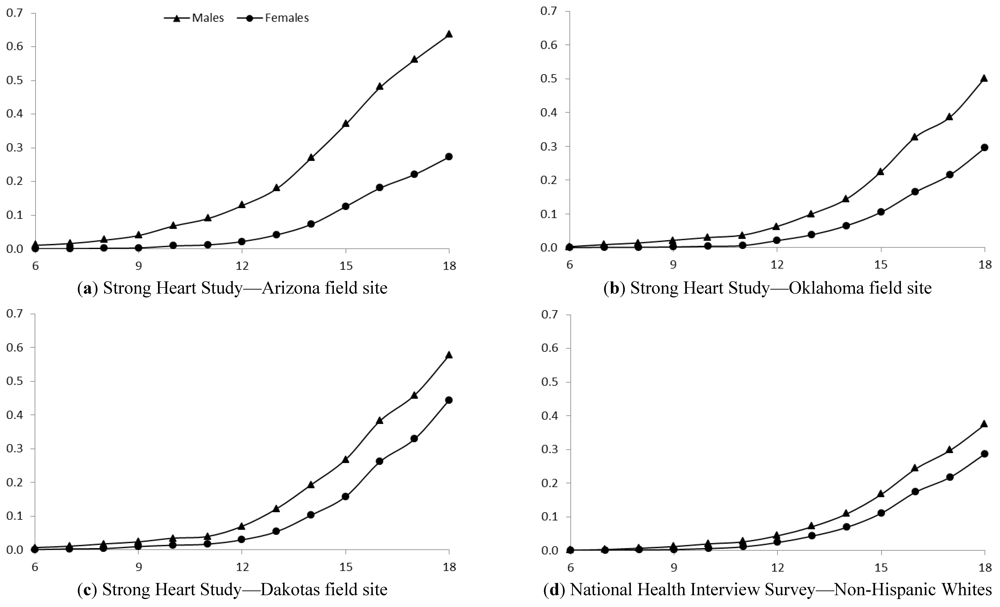
3. Results

{kind=link}
{kind=link}
{kind=link}
| American Indians | Non-Hispanic whites | |||
|---|---|---|---|---|
| Variable | SHS-AZ | SHS-OK | SHS-N/SD | NHIS |
| (n = 2,343) | (n = 2,327) | (n = 2,403) | (n = 19,747) * | |
| Age, mean years (SE) | 48 (0.3) | 51 (0.3) | 49 (0.3) | 47 (0.2) |
| Birth cohort, % | ||||
| 1910s and before | 3 | 5 | 4 | 3 |
| 1920–1929 | 14 | 17 | 15 | 8 |
| 1930–1939 | 24 | 24 | 26 | 10 |
| 1940–1949 | 23 | 23 | 22 | 15 |
| 1950–1959 | 9 | 10 | 8 | 20 |
| 1960–1969 | 11 | 11 | 11 | 19 |
| 1970–1979 | 11 | 8 | 10 | 16 |
| 1980–1985 | 6 | 3 | 5 | 9 |
| Female, % | 63 | 58 | 58 | 52 |
| High school graduate, % | 41 | 75 | 60 | 88 |
| Smoker by age 18 years, % | 41 | 38 | 50 | 33 |

| American Indians | Non-Hispanic whites | |||
|---|---|---|---|---|
| SHS-AZ% | SHS-OK% | SHS-N/SD% | NHIS% | |
| (95% CI) | (95% CI) | (95% CI) | (95% CI) | |
| Males | ||||
| Before 1920 | 50 (24–76) | 52 (37–68) | 50 (31–69) | 32 (26–39) |
| 1920–1929 | 61 (52–70) | 57 (49–65) | 50 (43–58) | 48 (44–53) |
| 1930–1939 | 65 (59–72) | 44 (38–51) | 62 (56–67) | 45 (42–49) |
| 1940–1949 | 63 (57–69) | 51 (45–58) | 63 (57–69) | 45 (42–48) |
| 1950–1959 | 67 (57–77) | 52 (41–63) | 51 (39–64) | 38 (36–41) |
| 1960–1969 | 63 (53–72) | 34 (25–44) | 46 (36–56) | 31 (29–34) |
| 1970–1979 | 56 (46–66) | 47 (36–58) | 50 (40–59) | 34 (31–37) |
| 1980–1985 | 49 (35–63) | 48 (31–64) | 67 (54–79) | 29 (25–33) |
| ptrend | 0.17 | 0.05 | 0.68 | <0.001 |
| Females | ||||
| Before 1920 | 12 (2–22) | 14 (5–23) | 28 (16–40) | 12 (9–16) |
| 1920–1929 | 13 (9–17) | 20 (15–25) | 33 (27–40) | 19 (16–21) |
| 1930–1939 | 20 (16–24) | 20 (15–24) | 37 (32–42) | 23 (21–26) |
| 1940–1949 | 29 (24–34) | 36 (30–41) | 42 (37–48) | 27 (25–30) |
| 1950–1959 | 35 (26–43) | 30 (23–38) | 51 (42–60) | 31 (29–33) |
| 1960–1969 | 40 (32–47) | 41 (33–49) | 53 (4–60) | 33 (31–36) |
| 1970–1979 | 39 (31–47) | 38 (29–48) | 55 (46–63) | 33 (31–36) |
| 1980–1985 | 33 (23–43) | 43 (26–59) | 72 (61–84) | 31 (27–35) |
| ptrend | <0.001 | <0.001 | <0.001 | <0.001 |

| American Indians | Non-Hispanic whites | |||
|---|---|---|---|---|
| SHS-AZ | SHS-OK | SHS-N/SD | NHIS | |
| HR (95% CI) | HR (95% CI) | HR (95% CI) | HR (95% CI) | |
| Males | ||||
| Before 1920 | 1.0 | 1.0 | 1.0 | 1.0 |
| 1920–1929 | 1.1 (0.6–2.2) | 1.0 (0.6–1.6) | 1.0 (0.6–1.8) | 1.6 (1.2–2.1) |
| 1930–1939 | 1.3 (0.7–2.6) | 0.7 (0.5–1.2) | 1.3 (0.8–2.3) | 1.5 (1.1–2.1) |
| 1940–1949 | 1.2 (0.6–2.4) | 0.9 (0.6–1.4) | 1.4 (0.8–2.4) | 1.5 (1.1–2.0) |
| 1950–1959 | 1.4 (0.7–2.8) | 0.9 (0.5–1.5) | 1.1 (0.6–2.0) | 1.2 (0.9–1.6) |
| 1960–1969 | 1.1 (0.6–2.2) | 0.5 (0.3–0.9) | 0.9 (0.5–1.6) | 0.9 (0.7–1.3) |
| 1970–1979 | 0.9 (0.5–1.9) | 0.8 (0.4–1.3) | 1.1 (0.6–1.9) | 1.1 (0.8–1.4) |
| 1980–1985 | 0.8 (0.4–1.7) | 0.7 (0.4–1.3) | 1.6 (0.9–2.9) | 0.9 (0.6–1.2) |
| ptrend | 0.06 | 0.02 | 0.96 | <0.001 |
| Females | ||||
| Before 1920 | 1.0 | 1.0 | 1.0 | 1.0 |
| 1920–1929 | 1.1 (0.4–3.0) | 1.5 (0.7–3.0) | 1.3 (0.7–2.2) | 1.6 (1.1–2.3) |
| 1930–1939 | 1.8 (0.7–4.4) | 1.5 (0.7–2.9) | 1.4 (0.8–2.4) | 2.0 (1.4–2.9) |
| 1940–1949 | 2.9 (1.2–7.1) | 3.0 (1.5–6.0) | 1.7 (1.0–2.8) | 2.5 (1.8–3.5) |
| 1950–1959 | 3.6 (1.4–9.0) | 2.5 (1.2–5.0) | 2.1 (1.2–3.6) | 2.9 (2.1–4.0) |
| 1960–1969 | 4.0 (1.6–10.0) | 3.5 (1.7–7.0) | 2.3 (1.3–3.9 ) | 3.2 (2.3–4.5) |
| 1970–1979 | 3.9 (1.6–9.8) | 3.2 (1.6–6.6) | 2.6 (1.5–4.4) | 3.3 (2.4–4.5) |
| 1980–1985 | 3.3 (1.3–8.5) | 3.6 (1.6–8.0) | 3.9 (2.2–6.9) | 3.0 (2.1–4.2) |
| ptrend | <0.001 | <0.001 | <0.001 | <0.001 |
4. Discussion

5. Conclusions
Acknowledgments
References
- Bachman, J.G.; Wallace, J.M.; O’Malley, P.M.; Johnston, L.D.; Kurth, C.L.; Neighbors, H.W. Racial/Ethnic differences in smoking, drinking, and illicit drug use among American high school seniors, 1976–89. Am. J. Publ. Health. 1991, 81, 372–377. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. In Vital Signs: Current Cigarette Smoking Among Audlts Aged ≥18 Years—United States, 2005–2010; MMWR: Atlanta, GA, USA, 2011; pp. 1207–1212.
- Choi, W.S.; Faseru, B.; Beebe, L.A.; Greiner, A.K.; Yeh, H.W.; Shireman, T.I.; Talawyma, M.; Cully, L.; Kaur, B.; Daley, C.M. Culturally-tailored smoking cessation for American Indians: Study protocol for a randomized controlled trial. Trials 2011, 12, 1–10. [Google Scholar] [CrossRef]
- U.S. Public Health Service, Preventing Tobacco Use Among Youth and Young Adults: A Report of the Surgeon General; U.S. Department of Health and Human Services: Atlanta, GA, USA, 2012.
- Centers for Disease Control and Prevention, Cigarette Smoking among Adults—United States 1998; MMWR: Atlanta, GA, USA, 2000; 49, pp. 881–884.
- Geishirt Cantrell, B.A.; Hodge, F.S.; Struthers, R.; Decora, L.H. The high incidence of cigarette smoking among American Indians of the Northern Plains. J. Cancer Educ. 2005, 20, 97–100. [Google Scholar] [CrossRef]
- Broome, C.V.; Marks, J.; Bales, V.; Eriksen, M. Tobacco Use among U.S. Racial/Ethnic Minority Groups, African Americans, American Indians and Alaska Natives, Asian Americans and Pacific Islanders, Hispanics: A Report of the Surgeon General; U.S. Department of Health and Human Services: Washington, DC, USA, 1998. [Google Scholar]
- D’Silva, J.; Schillo, B.A.; Sandman, N.R.; Leonard, T.L.; Boyle, R.G. Evaluation of a tailored approach for tobacco dependence treatment for American Indians. Am. J. Health Promot. 2011, 25, S66–S69. [Google Scholar]
- Kahende, J.W.; Malarcher, A.M.; Teplinskaya, A.; Asman, K.J. Quit attempt correlates among smokers by race/ethnicity. Int. J. Environ. Res. Public Health 2011, 8, 3871–3888. [Google Scholar]
- Lemstra, M.; Mackenbach, J.; Neudorf, C.; Nannapaneni, U.; Kunst, A. Daily smoking in Saskatoon: The independent effect of income and cultural status. C. J. Public Health 2009, 100, 51–54. [Google Scholar]
- Treiber, J. Developing culturally competent evaluation tools with tobacco control program practitioners. Health Promot. Pract. 2011, 12, 673–680. [Google Scholar] [CrossRef]
- Pego, C.M.; Hill, R.F.; Solomon, G.W.; Chisholm, R.M.; Ivey, S.E. Tobacco, culture, and health among American Indians: A historical review. Am. Indian Cult. Res. J. 1995, 19, 143–164. [Google Scholar]
- Federman, E.B.; Costello, E.J.; Angold, A.; Farmer, E.M.; Erkanli, A. Development of substance use and psychiatric comorbidity in an epidemiologic study of white and American Indian young adolescents the Great Smoky Mountains Study. Drug Alcohol Depend. 1997, 44, 69–78. [Google Scholar] [CrossRef]
- Beauvais, F.; Thurman, P.J.; Burnside, M.; Plested, B. Prevalence of American Indian adolescent tobacco use: 1993–2004. Subst. Use Misuse 2007, 42, 591–601. [Google Scholar] [CrossRef]
- Forster, J.L.; Brokenleg, I.; Rhodes, K.L.; Lamont, G.R.; Poupart, J. Cigarette smoking among American Indian youth in Minneapolis-St. Paul. Am. J. Prev. Med. 2008, 35, S449–S456. [Google Scholar] [CrossRef]
- LeMaster, P.L.; Connell, C.M.; Mitchell, C.M.; Manson, S.M. Tobacco use among American Indian adolescents: Protective and risk factors. J. Adolescent Health 2002, 30, 426–432. [Google Scholar] [CrossRef]
- Nez Henderson, P.; Kanekar, S.; Wen, Y.; Buchwald, D.; Goldberg, J.; Choi, W.; Okuyemi, K.S.; Ahluwalia, J.; Henderson, J.A. Patterns of cigarette smoking initiation in two culturally distinct American Indian tribes. Am. J. Publ. Health. 2009, 99, 2020–2025. [Google Scholar]
- Park, S.; Lee, J.Y.; Song, T.M.; Cho, S.I. Age-associated changes in nicotine dependence. Publ. Health 2012, 126, 482–489. [Google Scholar] [CrossRef]
- Duncan, A.E.; Lessov-Schlaggar, C.N.; Sartor, C.E.; Bucholz, K.K. Differences in time to onset of smoking and nicotine dependence by race/ethnicity in a Midwestern sample of adolescents and young adults from a high risk family study. Drug Alcohol Depend. 2012, 125, 140–145. [Google Scholar] [CrossRef]
- O’Loughlin, J.; DiFranza, J.; Tyndale, R.F.; Meshefedjian, G.; McMillan-Davey, E.; Clarke, P.B.; Hanley, J.; Paradis, G. Nicotine-dependence symptoms are associated with smoking frequency in adolescents. Am. J. Prev. Med. 2003, 25, 219–225. [Google Scholar] [CrossRef]
- Freedman, K.S.; Nelson, N.M.; Feldman, L.L. Smoking initiation among young adults in the United States and Canada,1998–2010: A systematic review. Prev. Chronic Dis. 2012, 9, p. E05. [CrossRef]
- Eichner, J.E.; Cravatt, K.; Beebe, L.A.; Blevins, K.S.; Stoddart, M.L.; Bursac, Z.; Yeh, F.; Lee, E.T.; Moore, W.E. Tobacco use among American Indians in Oklahoma: An epidemiologic view. Public Health Rep. 2005, 120, 192–199. [Google Scholar]
- Williams, D.; Mohammed, S. Discrimination and racial disparities in health: Evidence and needed research. J. Behav. Med. 2008, 32, 20–47. [Google Scholar] [CrossRef]
- Van De Ven, M.O.; Greenwood, P.A.; Engels, R.C.; Olsson, C.A.; Patton, G.C. Patterns of adolescent smoking and later nicotine dependence in young adults: A 10-year prospective study. Publ. Health. 2010, 124, 65–70. [Google Scholar] [CrossRef]
- Rose, J.S.; Dierker, L.C.; Donny, E. Nicotine dependence symptoms among recent onset adolescent smokers. Drug Alcohol Depend. 2010, 106, 126–132. [Google Scholar] [CrossRef]
- Rose, J.S.; Lee, C.T.; Dierker, L.C.; Selya, A.S.; Mermelstein, R.J. Adolescent nicotine dependence symptom profiles and risk for future daily smoking. Addict. Behav. 2012, 37, 1093–1100. [Google Scholar] [CrossRef]
- Branstetter, S.A.; Horn, K.; Dino, G.; Zhang, J. Beyond quitting: Predictors of teen smoking cessation, reduction and acceleration following a school-based intervention. Drug Alcohol Depend. 2009, 99, 160–168. [Google Scholar] [CrossRef]
- Hitchman, S.C.; Fong, G.T. Gender empowerment and female-to-male smoking prevalence ratios. Bull. World Health Organ. 2011, 89, 195–202. [Google Scholar] [CrossRef]
- National Clearinghouse for Smoking and Health, Use of Tobacco: Practices, Attitudes, Knowledge, and Beliefs, United States, Fall 1964 and Spring 1966; U.S. Department of Health Education, and Welfare: Washington, DC, USA, 1969.
- Waldron, I. Patterns and causes of gender differences in Smoking. Soc. Sci. Med. 1991, 32, 989–1005. [Google Scholar] [CrossRef]
- Ernster, V.L. Mixed messages for women. A social history of cigarette smoking and advertising. New York State J. Med. 1985, 85, 335–340. [Google Scholar]
- Howe, H. Advertising and Women’s Changing Smoking Habits: A Historical Perspective. In Proceedings of Fifth World Conference on Smoking and Health, Winnipeg, Canada, 10–15 July 1983.
- Toll, B.A.; Ling, P.M. The Virginia Slims identity crisis: An inside look at tobacco industry marketing to women. Tob. Control 2005, 14, 172–180. [Google Scholar] [CrossRef]
- Charlton, A.; Wald, N.; Kiryluk, S.; Darby, S.; Doll, R.; Pike, M.; Peto, R. U.K. Smoking Statistics; Oxford University Press: Oxford, UK, 1988; Volume 8. [Google Scholar]
- O’Keefe, A.M.; Pollay, R.W. Deadly targeting of women in promoting cigarettes. J. Am. Med. Womens Assoc. 1996, 51, 67–69. [Google Scholar]
- Hodge, F.S.; Struthers, R. Persistent smoking among northern plains Indians: Lenient attitudes, low harm value, and partiality toward cigarette smoking. J. Cult. Divers. 2006, 13, 181–185. [Google Scholar]
- Schissel, C. Traditional Tobacco Use in Plains Indian Societies; Canadian Cancer Society, Alberta, N.W.T. Division: Calgary, Canada, 1994. [Google Scholar]
- Ogunwole, S.U. We the People: American Indians and Alaska Natives in the United States; U.S. Census Bureau: Washington, DC, USA, 2006. [Google Scholar]
- Kim, Y.N.; Cho, Y.G.; Kim, C.H.; Kang, J.H.; Park, H.A.; Kim, K.W.; Hur, Y.I.; Lee, S.H.; Na, Y.M.; Park, N.Y. Socioeconomic indicators associated with initiation and cessation of smoking among women in Seoul. Korean J. Fam. Med. 2012, 33, 1–8. [Google Scholar] [CrossRef]
- Nagelhout, G.E.; de Korte-de Boer, D.; Kunst, A.E.; van der Meer, R.M.; de Vries, H.; van Gelder, B.M.; Willemsen, M.C. Trends in socioeconomic inequalities in smoking prevalence, consumption, initiation, and cessation between 2001 and 2008 in the Netherlands. Findings from a national population survey. BMC Publ. Health. 2012, 12, 303. [Google Scholar] [CrossRef]
- Giskes, K.; Kunst, A.E.; Benach, J.; Borrell, C.; Costa, G.; Dahl, E.; Dalstra, J.A.; Federico, B.; Helmert, U.; Judge, K.; et al. Trends in smoking behaviour between 1985 and 2000 in nine European countries by education. J. Epidemiol. Community Health 2005, 59, 395–401. [Google Scholar] [CrossRef] [Green Version]
- Hosseinpoor, A.R.; Parker, L.A.; Tursan d’Espaignet, E.; Chatterji, S. Socioeconomic inequality in smoking in low-income and middle-income countries: Results from the world health survey. PLos One 2012, 7, e42843. [Google Scholar] [CrossRef]
- Peretti-Watel, P.; Seror, V.; Constance, J.; Beck, F. Poverty as a smoking trap. Int. J. Drug Policy 2009, 20, 230–236. [Google Scholar] [CrossRef]
- Simantov, E.; Schoen, C.; Klein, J.D. Health-compromising behaviors: Why do adolescents smoke or drink?: Identifying underlying risk and protective factors. Arch. Pediatr. Adolesc. Med. 2000, 154, 1025–1033. [Google Scholar] [CrossRef]
- Stanton, W.R.; McClelland, M.; Elwood, C.; Ferry, D.; Silva, P.A. Prevalence, reliability and bias of adolescents’ reports of smoking and quitting. Addiction 1996, 91, 1705–1714. [Google Scholar] [CrossRef]
- Ellickson, P.L.; Tucker, J.S.; Klein, D.J. High-risk behaviors associated with early smoking: Results from a 5-year follow-up. J. Adolesc. Health 2001, 28, 465–473. [Google Scholar] [CrossRef]
- Bricker, J.B.; Peterson, A.V., Jr.; Leroux, B.G.; Andersen, M.R.; Rajan, K.B.; Sarason, I.G. Prospective prediction of children’s smoking transitions: role of parents’ and older siblings’ smoking. Addiction 2006, 101, 128–136. [Google Scholar] [CrossRef]
- Bricker, J.B.; Peterson, A.V.; Robyn Andersen, M.; Leroux, B.G.; Bharat Rajan, K.; Sarason, I.G. Close friends’, parents’, and older siblings’ smoking: Reevaluating their influence on children’s smoking. Nicotine Tob. Res. 2006, 8, 217–226. [Google Scholar] [CrossRef]
- Hruba, D.; Zaloudikova, I. Where do our children learn to smoke? Cent. Eur. J. Publ. Health 2008, 16, 178–181. [Google Scholar]
- Briggs, V.L.; Lindorff, K.J.; Ivers, R.G. Aboriginal and Torres Strait Islander Australians and tobacco. Tob. Control 2003, 12, ii5–ii8. [Google Scholar]
- Motyka, A.; Adamek, R.; Kurzepa-Hasan, E.; Bochenek, K. Motives, awareness of danger and prevalence of tobacco smoking among students of Poznan University of Medical Sciences in Poznan and High School of Country Economy in Kutno. Przegl.Lek. 2008, 65, 562–564. [Google Scholar]
- Youssef, R.M.; Abou-Khatwa, S.A.; Fouad, H.M. Current and never smokers: Differentials in characteristics, knowledge and perceptions. East Mediterr. Health J. 2003, 9, 923–934. [Google Scholar]
- Moe v. Salish and Kootenai Tribes—425 U.S. 463 (1976). Available online: supreme.justia.com/cases/federal/us/425/463/case.html (accessed on 10 Febuary 2013).
- Washington v. Confederated Tribes of the Colville Indian Reservation. Available online: supreme.justia.com/cases/federal/us/425/463/case.html (accessed on 14 January 2013).
- Ding, A. Curbing adolescent smoking: A review of the effectiveness of various policies. Yale J. Biol. Med. 2005, 78, 37–44. [Google Scholar]
- Zhang, B.; Cohen, J.; Ferrence, R.; Rehm, J. The impact of tobacco tax cuts on smoking initiation among Canadian young adults. Am. J. Prev. Med. 2006, 30, 474–479. [Google Scholar] [CrossRef]
- Lee, J.; Halpern-Felsher, B.L. What does it take to be a smoker? Adolescents’ characterization of different smoker types. Nicotine Tob. Res. 2011, 13, 1106–1113. [Google Scholar] [CrossRef]
- Pomerleau, C.S.; Pomerleau, O.F.; Snedecor, S.M.; Mehringer, A.M. Defining a never-smoker: Results from the nonsmokers survey. Addict. Behav. 2004, 29, 1149–1154. [Google Scholar] [CrossRef]
- McGee, R.; Williams, S.; Stanton, W. Smoking among New Zealand adolescents 1960–93. New Zeal Med. J. 1995, 108, 85–87. [Google Scholar]
- Harris, J.B.; Schwartz, S.M.; Thompson, B. Characteristics associated with self-identification as a regular smoker and desire to quit among college students who smoke cigarettes. Nicotine Tob. Res. 2008, 10, 69–76. [Google Scholar] [CrossRef]
- Levinson, A.H.; Campo, S.; Gascoigne, J.; Jolly, O.; Zakharyan, A.; Tran, Z.V. Smoking, but not smokers: Identity among college students who smoke cigarettes. Nicotine Tob.Res. 2007, 9, 845–852. [Google Scholar] [CrossRef]
- Brook, J.S.; Balka, E.; Zhang, C.; Pahl, K.; Brook, D.W. Adolescent academic adjustment factors and the trajectories of cigarette smoking from adolescence to the mid-thirties. Int. J. Ment. Health 2011, 40, 7–21. [Google Scholar] [CrossRef]
- Fidler, J.A.; West, R.; Jarvis, M.J.; Wardle, J. Early dating predicts smoking during adolescence: A prospective study. Addiction 2006, 101, 1805–1813. [Google Scholar] [CrossRef]
- Langlois, M.A.; Petosa, R.; Hallam, J.S. Why do effective smoking prevention programs work? Student changes in social cognitive theory constructs. J. Sch. Health 1999, 69, 326–331. [Google Scholar] [CrossRef]
- Kim, S.; Nam, K.A.; Seo, M.; Lee, H.H. Effectiveness of a smoking cessation program for adolescents. TaehanKanho Hakhoe Chi 2004, 34, 646–654. [Google Scholar]
- Chen, H.H.; Yeh, M.L. Developing and evaluating a smoking cessation program combined with an Internet-assisted instruction program for adolescents with smoking. Patient Educ. Couns. 2006, 61, 411–418. [Google Scholar] [CrossRef]
- Cornell, S.; Kalt, J.P. American Indian Self-Determination: The Political Economy of a Policy that Works; Harvard Kennedy School: Cambridge, MA, USA, 2010. [Google Scholar]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Orr, R.; Calhoun, D.; Noonan, C.; Whitener, R.; Henderson, J.; Goldberg, J.; Henderson, P.N. A History of Ashes: An 80 Year Comparative Portrait of Smoking Initiation in American Indians and Non-Hispanic Whites—the Strong Heart Study. Int. J. Environ. Res. Public Health 2013, 10, 1747-1762. https://doi.org/10.3390/ijerph10051747
Orr R, Calhoun D, Noonan C, Whitener R, Henderson J, Goldberg J, Henderson PN. A History of Ashes: An 80 Year Comparative Portrait of Smoking Initiation in American Indians and Non-Hispanic Whites—the Strong Heart Study. International Journal of Environmental Research and Public Health. 2013; 10(5):1747-1762. https://doi.org/10.3390/ijerph10051747
Chicago/Turabian StyleOrr, Raymond, Darren Calhoun, Carolyn Noonan, Ron Whitener, Jeff Henderson, Jack Goldberg, and Patrica Nez Henderson. 2013. "A History of Ashes: An 80 Year Comparative Portrait of Smoking Initiation in American Indians and Non-Hispanic Whites—the Strong Heart Study" International Journal of Environmental Research and Public Health 10, no. 5: 1747-1762. https://doi.org/10.3390/ijerph10051747
APA StyleOrr, R., Calhoun, D., Noonan, C., Whitener, R., Henderson, J., Goldberg, J., & Henderson, P. N. (2013). A History of Ashes: An 80 Year Comparative Portrait of Smoking Initiation in American Indians and Non-Hispanic Whites—the Strong Heart Study. International Journal of Environmental Research and Public Health, 10(5), 1747-1762. https://doi.org/10.3390/ijerph10051747