Screening and Brief Interventions for Hazardous and Harmful Alcohol Use among University Students in South Africa: Results from a Randomized Controlled Trial


Abstract
:1. Introduction
2. Methodology
2.1. Design
2.2. Study Population and Participants
2.2.1. Principles for Recruitment
Inclusion criteria
Exclusion criteria
2.2.2. Participant Randomization
Blinding
2.2.3. Procedure
2.2.4. Interventions
Control arm: provision of health education leaflet
Experimental arm: brief intervention
2.2.5. Counsellor Training and Intervention Quality Assurance
2.3. Measures
2.4. Data Analysis
3. Results and Discussion
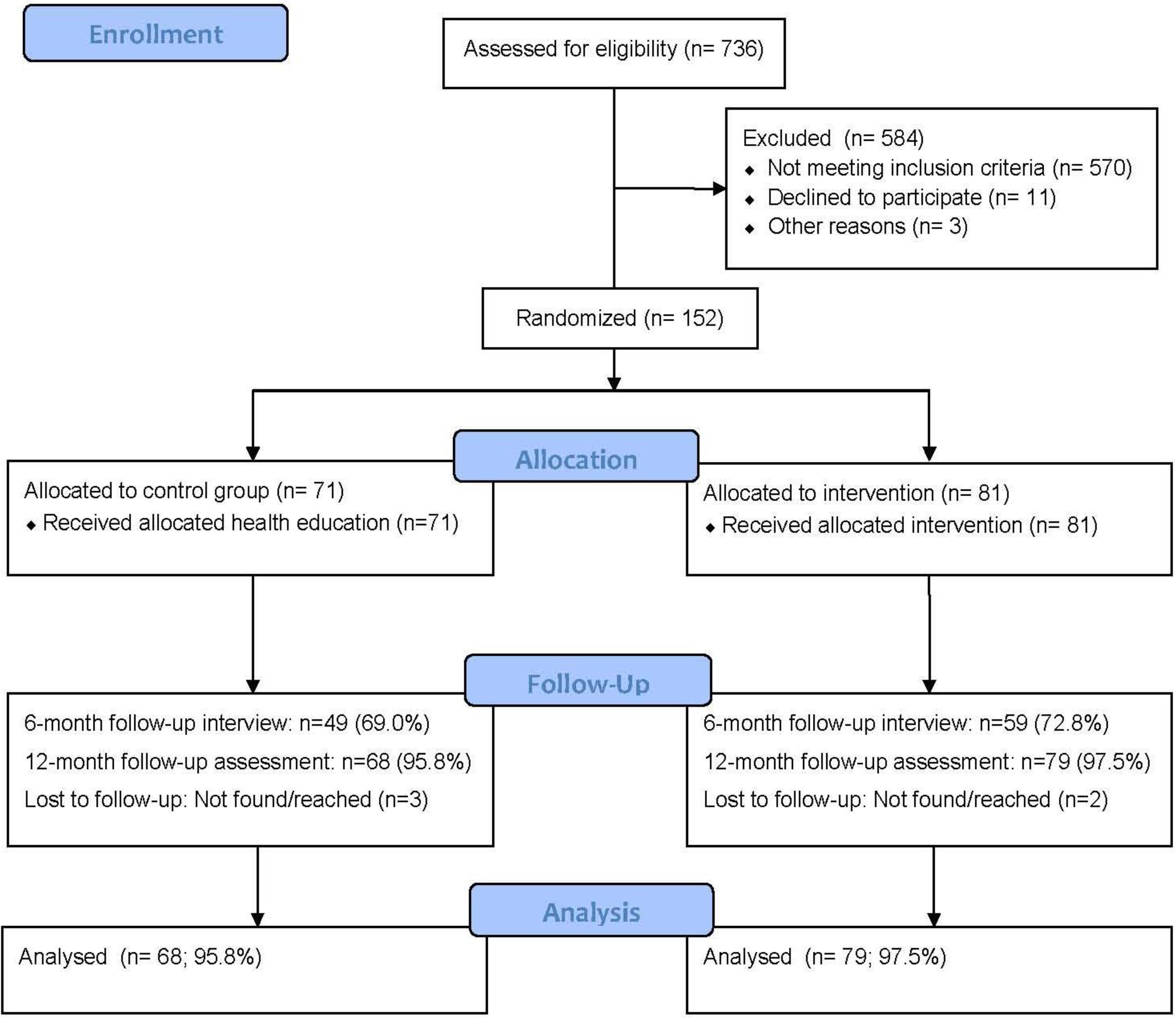
3.1. Screening and Randomization
3.2. Brief Intervention Implementation Fidelity Analysis

3.3. Participant Characteristics

{kind=link}
| Variables | Control n = 71 (%) | Intervention n = 81 (%) | t/χ2 | P-value |
|---|---|---|---|---|
| Socio-demographic variables | ||||
| Gender (N, % male) | 65 (92.9) | 66 (82.5) | χ2 3.62 | 0.057 |
| Age in years (M, SD) | 22.1 (3.7) | 21.7 (3.4) | t 0.67 | 0.503 |
| Year of study | ||||
| First year | 23 (39.7) | 27 (39.7) | χ2 0.17 | 0.920 |
| Second year | 17 (29.3) | 18 (26.5) | ||
| Third or more year | 18 (31.0) | 23 (33.8) | ||
| Family background | ||||
| Wealthier (wealthy, quite well off) | 32 (45.3) | 34 (43.0) | χ2 0.11 | 0.743 |
| Poorer (not very well off or quite poor) | 38 (54.3) | 45 (57.0) | ||
| Residence | ||||
| On campus | 57 (80.3) | 61 (75.3) | χ2 0.54 | 0.463 |
| Off campus | 14 (19.7) | 20 (24.7) | ||
| Health variables | ||||
| Alcohol use (AUDIT score) (M,SD) | 14.0 (6.1) | 18.0 (7.3) | t −3.66 | <0.001 *** |
| Drinking norms score (range 2–10) | 7.2 (1.9) | 7.1 (2.2) | t 0.35 | 0.729 |
| Importance of not drinking too much Alcohol score (range 1–10) | 7.1 (2.9) | 7.0 (2.9) | t 0.18 | 0.858 |
| Daily or almost daily tobacco use | 16 (22.5) | 20 (24.7) | χ2 0.10 | 0.755 |
| Past month cannabis use | 18 (25.4) | 27 (33.3) | χ2 1.16 | 0.282 |
| Perceived health status | ||||
| Poor/Fair/Good | 33 (46.5) | 35 (43.2) | χ2 0.16 | 0.686 |
| Very good/Excellent | 38 (53.8) | 46 (56.8) | ||
| PTSD (4 or more items) | 12 (17.6) | 23 (29.1) | χ2 2.65 | 0.104 |
| Depression (15 or more scores) | 5 (7.5) | 12 (17.6) | χ2 3.18 | 0.075 |
3.4. Alcohol Use Outcomes
| Variables | Time | Control | Intervention | β (95% CI) | P-value |
|---|---|---|---|---|---|
| Criterion variables | |||||
| AUDIT total (M, SD) | Baseline | 14.0 (6.1) | 18.0 (7.3) | −0.18 (−0.30, −0.06) | 0.004 ** |
| 6 months | 11.6 (7.7) | 11.3 (7.6) | |||
| 12 months | 11.0 (6.4) | 13.5 (7.3) | |||
| AUDIT (8–19) High risk (n, %) | Baseline | 59 (83.1) | 51 (63.0) | −0.18 (−0.30, −0.06) | 0.090 |
| 6 months | 23 (46.9) | 28 (47.5) | |||
| 12 months | 43 (63.2) | 48 (60.8) | |||
| AUDIT (20–40) Alcohol dependence (n, %) | Baseline | 12 (16.9) | 30 (37.0) | −0.71 (−1.29, −0.13) | 0.013 * |
| 6 months | 10 (20.4) | 11 (18.6) | |||
| 12 months | 6 (8.8) | 16 (20.3) | |||
| Heavy episodic drinking score (range 0–5) 1 (M, SD) | Baseline | 1.7 (0.9) | 2.2 (1.0) | −0.44 (−0.76, −0.12) | 0.007 ** |
| 6 months | 1.8 (1.1) | 1.7 (1.1) | |||
| 12 months | 1.8 (1.0) | 1.9 (1.2) | |||
| Mediator variables | |||||
| Drinking norms (M, SD) | Baseline | 7.2 (1.9) | 7.1 (2.2) | 0.04 (−0.03, 0.12) | 0.271 |
| 12 months | 7.1 (1.9) | 6.6 (2.2) | |||
| Importance of not drinking too much alcohol (M, SD) | Baseline | 7.3 (2.8) | 7.0 (2.8) | −0.01 (−0.10, 0.09) | 0.886 |
| 12 months | 8.2 (2.3) | 8.4 (2.6) | |||
| Other health variables | |||||
| Daily or almost daily tobacco use (n, %) | Baseline | 16 (22.5) | 20 (24.7) | −0.24 (−0.88, 0.41) | 0.469 |
| 12 months | 16 (23.5) | 24 (30.4) | |||
| Current (past month) cannabis use (n, %) | Baseline | 18 (25.4) | 27 (33.3) | −0.24 (−0.84, 0.37) | 0.445 |
| 12 months | 20 (29.9) | 25 (31.6) | |||
| Self-rated health status (rated from 1–5, with 5 being the highest) (M, SD) | Baseline | 3.6 (1.0) | 3.6 (0.9) | −0.02 (−0.09, 0.04) | 0.501 |
| 12 months | 3.6 (0.9) | 3.7 (0.9) | |||
| PTSD score (M, SD) | Baseline | 1.8 (1.7) | 2.4 (2.0) | −0.17 (−0.44, 0.10) | 0.221 |
| 12 months | 1.6 (2.0) | 1.7 (1.9) | |||
| Depression score (M, SD) | Baseline | 7.4 (4.2) | 9.7 (6.5) | −0.07 (−0.14, 0.01) | 0.074 |
| 12 months | 8.7 (6.5) | 9.1 (5.5) | |||
4. Discussion
5. Study Limitations
6. Conclusions
Acknowledgments
Conflict of Interest
References
- World Health Organtization (WHO), Global Status Report on Alcohol and Health; WHO: Geneva, Switzerland, 2011.
- Rehm, J.; Rehn, N.; Room, R.; Monteiro, M.; Gmel, G.; Jernigan, D.; Frick, U. The global distribution of average volume of alcohol consumption and patterns of drinking. Eur. Addict. Res. 2003, 9, 147–156. [Google Scholar] [CrossRef]
- Schneider, M.; Norman, R.; Parry, C.; Bradshawm, D.; Plüddemann, A. South African comparison risk assessment collaborating group: Estimating the burden of disease attributable to alcohol use in South Africa in 2000. S. Afr. Med. J. 2007, 97, 664–672. [Google Scholar]
- Reid, M.C.; Fiellin, D.A.; O’Connor, P.G. Harzardous and harmful alcohol consumption in primary care. Arch. Intern. Med. 1999, 159, 1681–1689. [Google Scholar] [CrossRef]
- Zverev, Y. Problem drinking among university students in Malawi. Coll. Anthropol. 2008, 32, 27–31. [Google Scholar]
- Young, C.; de Klerk, V. Patterns of alcohol usage on a South African university campus: The findings of two annual drinking surveys. Afr. J. Drug Alcohol Stud. 2008, 7, 101–112. [Google Scholar]
- Young, C.; Mayson, T. The Alcohol Use Disorders Identification Scale (AUDIT) normative scores for a multiracial sample of Rhodes University residence students. J. Child Adol. Men. Health 2010, 22, 15–23. [Google Scholar] [CrossRef]
- Alexandre, E.; Bowen, A. Excessive drinking in college: Behavioral outcome, not binge, as a basis for prevention. Addict. Behav. 2004, 29, 1199–1205. [Google Scholar] [CrossRef]
- Simão, M.O.; Kerr-Corrêa, F.; Smaira, S.I.; Trinca, L.A.; Floripes, T.M.; Dalben, I.; Martins, R.A.; Oliveira, J.B.; Cavariani, M.B.; Tucci, A.M. Prevention of “risky” drinking among students at a Brazilian university. Alcohol Alcohol. 2008, 43, 470–476. [Google Scholar] [CrossRef]
- Wicki, M.; Kuntsche, E.; Gmel, G. Drinking at European universities? A review of students’ alcohol use. Addict. Behav. 2010, 35, 913–924. [Google Scholar] [CrossRef]
- Borsari, B.; Carey, K.B. Peer influences in college drinking: A review of the research. J. Subst. Abuse. 2001, 13, 391–424. [Google Scholar] [CrossRef]
- Deressa, W.; Azazh, A. Substance use and its predictors among undergraduate medical students of Addis Ababa University in Ethiopia. BMC Public Health. 2011, 11, 660. [Google Scholar] [CrossRef]
- John, B.; Alwyn, T. Alcohol Related Social Norm Perceptions in University Students: Effective Interventions for Change. 2010. Available online: http://alcoholresearchuk.org/downloads/finalReports/AERC_FinalReport_0072.pdf (accessed on 15 March 2013).
- Steyl, T.; Phillips, J. Actual and perceived substance use of health science students at a university in the Western Cape, South Africa. Afr. Health Sci. 2011, 11, 329–333. [Google Scholar]
- Utpala-Kumar, R.; Deane, F.P. Heavy episodic drinking among university students: Drinking status and perceived normative comparisons. Subst. Use Misuse. 2012, 47, 278–285. [Google Scholar] [CrossRef]
- Vantamay, S. Alcohol consumption among university students: Applying a social ecological approach for multi-level preventions. Southeast Asian J. Trop. Med. Publ. Health 2009, 40, 354–369. [Google Scholar]
- Adewuya, A.O.; Ola, B.A.; Aloba, O.O.; Mapayi, B.M.; Oginni, O.O. Depression amongst Nigerian university students. Prevalence and sociodemographic correlates. Soc. Psychiatry Psychiatr. Epidemiol. 2006, 41, 674–678. [Google Scholar] [CrossRef]
- Atwoli, L.; Mungla, P.A.; Ndung’u, M.N.; Kinoti, K.C.; Ogot, E.M. Prevalence of substance use among college students in Eldoret, Western Kenya. BMC Psychiatry 2011, 11, 34. [Google Scholar] [CrossRef]
- O’Donnell, K.; Wardle, J.; Dantzer, C.; Steptoe, A. Alcohol consumption and symptoms of depression in young adults from 20 countries. J. Stud. Alcohol. 2006, 67, 837–840. [Google Scholar]
- Peltzer, K. Depressive symptoms in relation to alcohol and tobacco use in South African University students. Psychol. Rep. 2003, 92, 1097–1098. [Google Scholar]
- Bachrach, R.L.; Read, J.P. The role of posttraumatic stress and problem alcohol involvement in university academic performance. J. Clin. Psychol. 2012. [Google Scholar] [CrossRef]
- Carey, K.B.; Scott-Sheldon, L.A.; Carey, M.P.; DeMartini, K.S. Individual-level interventions to reduce college student drinking: A meta-analytic review. Addict. Behav. 2007, 32, 2469–2494. [Google Scholar] [CrossRef]
- Seigers, D.K.; Carey, K.B. Screening and brief interventions for alcohol use in college health centers: A review. J. Am. Coll. Health 2011, 59, 151–158. [Google Scholar] [CrossRef]
- The Physicians’ Guide to Helping Patients with Alcohol Problems; National Institute on Alcohol Abuse and Alcoholism (NIAAA): Rockville, MD, USA, 2012.
- Pensuksan, W.C.; Taneepanichskul, S.; Williams, M.A. A peer-drinking group motivational intervention among Thai male undergraduate students. Int. J. Drug Policy 2010, 21, 432–436. [Google Scholar] [CrossRef]
- Babor, T.F.; Higgins-Biddle, J.C. Brief Intervention for Hazardous and Harmful Drinking. A Manual for Use in Primary Care Settings; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Fisher, W.A.; Fisher, J.D.; Harman, J. The information-motivation-behavioural skills model: A general social psychological approach to understanding and promoting health behavior. In Social Psychological Foundations of Health and Illness; Suls, J., Wallston, K., Eds.; Wiley-Blackwell: London, UK, 2003; pp. 87–106. [Google Scholar]
- Raistrick, D.; Heather, N.; Godfrey, C. Review of the Effectiveness of Treatment for Alcohol Problems; National Treatment Agency for Drug Abuse: London, UK, 2006. [Google Scholar]
- Raistrick, D.; Tober, G. Psychosocial interventions. Psychiatry 2004, 3, 36–39. [Google Scholar] [CrossRef]
- Pengpid, S.; Peltzer, K.; Skaal, L.; van der Heever, H.; van Hal, G. Screening and brief intervention for alcohol problems in Dr George Mukhari Hospital out-patients in Gauteng, South Africa: A single-blinded randomized controlled trial protocol. BMC Public Health 2012, 12, 127. [Google Scholar] [CrossRef]
- Babor, T.F.; Higgins-Biddle, J.C.; Saunders, J.B.; Monteiro, M.G. AUDIT: The Alcohol Use Disorders Identification Test. Guidelines for Use in Primary Care; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Freeborn, D.K.; Polen, M.R.; Hollis, J.F.; Senft, R.A. Screening and brief intervention for hazardous drinking in an HMO: Effects on medical care utilization. J. Behav. Health Serv. Res. 2000, 27, 446–453. [Google Scholar] [CrossRef]
- Wing, K. Drinking Norms Questionnaire. 2010. Available online: http://www.afcrossroads.com/Drinking_Norms_Questionnaire2.pdf (accessed on 15 March 2013).
- Kimerling, R.; Ouimette, P.; Prins, A.; Nisco, P.; Lawler, C.; Cronkite, R.; Moos, R.H. Brief report: Utility of a short screening scale for DSM-IV PTSD in primary care. J. Gen. Intern. Med. 2006, 21, 65–67. [Google Scholar] [CrossRef]
- Sikkema, K.J.; Watt, M.H.; Meade, C.S.; Ranby, K.W.; Kalichman, S.C.; Skinner, D.; Pieterse, D. Mental health and HIV sexual risk behavior among patrons of alcohol serving venues in Cape Town, South Africa. J. Acquir. Immune Defic. Syndr. 2011, 57, 230–237. [Google Scholar] [CrossRef]
- Andresen, E.M.; Malmgren, J.A.; Carter, W.B.; Patrick, D.L. Screening for depression in well older adults: Evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale). Am. J. Prev. Med. 1994, 10, 77–84. [Google Scholar]
- Mulrow, C.D.; Williams, J.W., Jr.; Gerety, M.B.; Ramirez, G.; Montiel, O.M.; Kerber, C. Case-finding instruments for depression in primary care settings. Ann. Intern. Med. 1995, 122, 913–921. [Google Scholar] [CrossRef]
- Molenberghs, G.; Kenward, M.G. Missing Data in Clinical Studies; John Wiley & Sons: Chichester, UK, 2007. [Google Scholar]
- Baer, J.S.; Kivlahan, D.R.; Blume, A.W.; McKnight, P.; Marlatt, G.A. Brief intervention for heavy-drinking college students: 4-year follow-up and natural history. Am. J. Public Health. 2001, 91, 1310–1316. [Google Scholar] [CrossRef]
- McCambridge, J.; Kypri, K. Can simply answering research questions change behaviour? Systematic review and meta analyses of brief alcohol intervention trials. PLoS One 2011, 6, e23748. [Google Scholar] [CrossRef]
- Murphy, J.G.; Duchnick, J.J.; Vuchinich, R.E.; Davison, J.W.; Karg, R.S.; Olson, A.M.; Smith, A.F.; Coffey, T.T. Relative efficacy of a brief motivational intervention for college student drinkers. Psychol. Addict. Behav. 2001, 15, 373–379. [Google Scholar]
- Scott-Sheldon, L.J.; Demartini, K.S.; Carey, K.B.; Carey, M.P. Alcohol interventions for college students improves antecedents of behavioural change: Results from a meta-analysis of 34 randomized controlled trials. J. Soc. Clin. Psychol. 2009, 28, 799–823. [Google Scholar] [CrossRef]
- Borsari, B.; Carey, K.B. Effects of a brief motivational intervention with college student drinkers. J. Consult. Clin. Psychol. 2000, 68, 728–733. [Google Scholar] [CrossRef]
- McCambridge, J.; Jenkins, R.J. Do brief interventions which target alcohol consumption also reduce cigarette smoking? Systematic review and meta-analysis. Drug Alcohol Depend. 2008, 96, 263–270. [Google Scholar] [CrossRef]
- Noknoy, S.; Rangsin, R.; Saengcharnchai, P.; Tantibhaedhyangkul, U.; McCambridge, J. RCT of effectiveness of motivational enhancement therapy delivered by nurses for hazardous drinkers in primary care units in Thailand. Alcohol Alcohol. 2010, 45, 263–270. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Pengpid, S.; Peltzer, K.; Van der Heever, H.; Skaal, L. Screening and Brief Interventions for Hazardous and Harmful Alcohol Use among University Students in South Africa: Results from a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2013, 10, 2043-2057. https://doi.org/10.3390/ijerph10052043
Pengpid S, Peltzer K, Van der Heever H, Skaal L. Screening and Brief Interventions for Hazardous and Harmful Alcohol Use among University Students in South Africa: Results from a Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2013; 10(5):2043-2057. https://doi.org/10.3390/ijerph10052043
Chicago/Turabian StylePengpid, Supa, Karl Peltzer, Hendry Van der Heever, and Linda Skaal. 2013. "Screening and Brief Interventions for Hazardous and Harmful Alcohol Use among University Students in South Africa: Results from a Randomized Controlled Trial" International Journal of Environmental Research and Public Health 10, no. 5: 2043-2057. https://doi.org/10.3390/ijerph10052043
APA StylePengpid, S., Peltzer, K., Van der Heever, H., & Skaal, L. (2013). Screening and Brief Interventions for Hazardous and Harmful Alcohol Use among University Students in South Africa: Results from a Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 10(5), 2043-2057. https://doi.org/10.3390/ijerph10052043