Neurotoxicity of Acrylamide in Exposed Workers


 ,
,  and
and
Abstract
:1. Introduction
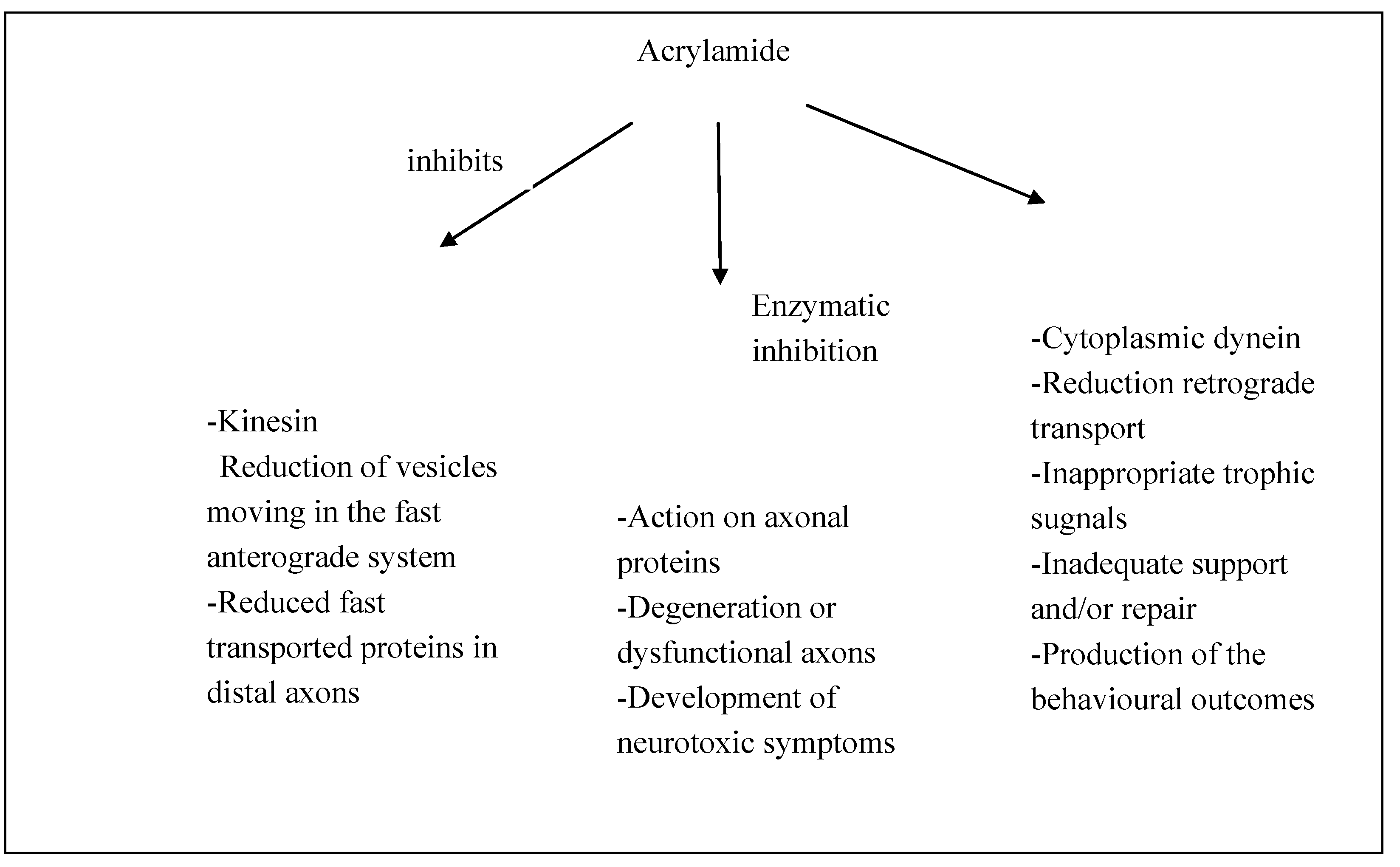
2. Experimental Research and Pathogenesis

3. Human Case Studies

{kind=link}
| Case Study | Patients | Type of Work | Exposition | Signs and Symptoms |
|---|---|---|---|---|
| Mulloy, K.B. 1996 [48] | 2 workers in the Southern West Virginia | Coal mine preparation plant workers producing acrylamide monomers | Exposure for over 10 years to acrylamide polymer flocculent contaminated with acrylamide monomer | Patient A: parkinsonism Patient B: peripheral neuropathies, neurological bladder |
| Calleman, C.J. et al. 1994 [49] | 41 workers in the city of Xinxiang | Workers heavily exposed to a mixture of acrylamide and acrylonitrile | Acrylamide and acrylonitrile | Peripheral neuropathy |
| Myers, J.E. et al. 1991 [50] | Workers at a South African factory | Factory workers producing polymer from acrylamide monomers | Acrylamide monomer | Peripheral neuropathy, abnormal gait, skin abnormalities |
| Auld, R.B. et al. 1967 [3] | A white male worker in Bathurst | Mine worker | 10% Aqueous solution of acrylamide | Peripheral neuropathy |
| Kesson, C.M. et al. 1977 [51] | 6 workers in England | Construction industry workers in the confines of a small tunnel | Acrylamide monomer | Peripheral neuropathy. Two workers affected more severely than the other ones |
| Garland, T.O. et al. 1967 [52] | 6 workers at two English factories | Polymerization of the Acrylamide monomer in the manufacture of flocculators | Acrylamide monomer | Peripheral neuropathy, midbrain disturbance |
| He, F. et al. 1989 [53] | 71 workers in China | Small factories manufacturing acrylamide workers | Aqueous solution of acrylamide monomer | Peripheral neuropathy, cerebellar involment (3 patients), skin abnormalities |
| Kjuus, H. et al. 2004 [54] | 24 workers in Norway | Tunnel workers | N-methylolacrylamide (NMA)-containing grout and water contaminated with acrylamide | Peripheral neuropathy (paresthesia, pain and weakness in the limbs), skin abnormalities |
| Goffeng, L.O. et al. 2008 [55] | 44 workers in Norway | Tunnel workers | N-methylolacrylamide (NMA)-containing grout and water contaminated with acrylamide | Slightly reduced light sensitivity and colour discrimination |
4. Prevention and Health Risk Assessment
5. Medical Treatment of ACR Neurotoxicity
6. Conclusions
Acknowledgments
Conflicts of Interest
References
- Brown, L.; Rhead, M.M.; Bancroft, K.C.C.; Allen, N. Case studies of acrylamide pollution resulting from industrial use of acrylamides. Water Pollut. Control 1980, 79, 507–510. [Google Scholar]
- Kopp, E.K.; Dekant, W. Toxicokinetics of acrylamide in rats and humans following single oral administration of low doses. Toxicol. Appl. Pharmacol. 2009, 235, 135–142. [Google Scholar] [CrossRef]
- Auld, R.B.; Bedwell, S.F. Peripheral neuropathy with sympathetic overactivity from industrial contact with acrylamide. Can. Med. Assoc. J. 1967, 96, 652–654. [Google Scholar]
- Zhang, Y.; Zhang, G.; Zhang, Y. Occurrence and analytical methods of acrylamide in heat-treated foods: Review and recent developments. J. Chromatogr. A 2005, 1075, 1–21. [Google Scholar]
- Eriksson, S. Acrylamide in Food Products: Identification, Formation and Analytical Methodology. Ph.D. Thesis, Department of Environmental Chemistry, Stockholm University, Stockholm, Sweden, 2005. [Google Scholar]
- Törqvist, M. Acrylamide in Food: The Discovery and Its Implications. In Chemistry and Safety of Acrylamide in Food; Friedman, M., Mottram, D., Eds.; Springer Science, Business Media Inc.: New York, NY, USA, 2005; pp. 1–19. [Google Scholar]
- Johnson, K.A.; Gorzinski, S.J.; Bodner, K.M.; Campbell, R.A.; Wolf, C.H.; Friedman, M.A. Chronic toxicity and oncogenicity study on acrylamide incorporated in the drinking water of Fischer 344 rats. Toxicol. Appl. Pharmacol. 1986, 85, 154–168. [Google Scholar] [CrossRef]
- Smith, E.A.; Oehme, F.W. Acrylamide and polyacrylamide: A review of production, use, environmental fate and neurotoxicity. Rev. Environ. Health 1991, 9, 215–228. [Google Scholar]
- Edwards, P.M.; Parker, V.H. A simple, sensitive, and objective method for early assessment of acrylamide neuropathy in rats. Toxicol. Appl. Pharmacol. 1977, 40, 589–591. [Google Scholar] [CrossRef]
- Some Industrial Chemicals. In IRAC Monographs on the Evaluation of Carcinogenic Risk for Chemicals to Humans; International Agency for Research on Cancer (IARC): Lyon, France, 1994; Volume 60, p. 435.
- Shipp, A.; Lawrence, G.; Gentry, R.; McDonald, T.; Bartow, H.; Bounds, J.; Macdonald, N.; Clewell, H.; Allen, B.; van Landingham, C. Acrylamide: Review of toxicity data and dose-response analyses for cancer and noncancer effects. Crit. Rev. Toxicol. 2006, 36, 481–608. [Google Scholar] [CrossRef]
- Collins, J.J.; Swaen, G.M.; Marsh, G.M.; Utidjian, H.M.; Caporossi, J.C.; Lucas, L.J. Mortality patterns among workers exposed to acrylamide. J. Occup. Med. 1989, 31, 614–617. [Google Scholar] [CrossRef]
- Marsh, G.M.; Lucas, L.J.; Youk, A.O.; Schall, L.C. Mortality patterns among workers exposed to acrylamide: 1994 follow up. Occup. Environ. Med. 1999, 56, 181–190. [Google Scholar] [CrossRef]
- LoPachin, R.M., Jr.; Lehning, E.J. Acrylamide-induced distal axon degeneration: A proposed mechanism of action. Neurotoxicology 1994, 15, 247–259. [Google Scholar]
- LoPachin, R.M.; Lehning, E.J.; Opanashuk, L.A.; Jortner, B.S. Rate of neurotoxicant exposure determines morphologic manifestations of distal axonopathy. Toxicol. Appl. Pharmacol. 2000, 167, 75–86. [Google Scholar] [CrossRef]
- LoPachin, R.M.; Ross, J.F.; Lehning, E.J. Nerve terminals as the primary site of acrylamide action: A hypothesis. Neurotoxicology 2002, 23, 43–59. [Google Scholar] [CrossRef]
- Fennell, T.R.; Sumner, S.C.; Snyder, R.W.; Burgess, J.; Friedman, M.A. Kinetics of elimination of urinary metabolites of acrylamide in humans. Toxicol. Sci. 2006, 93, 256–267. [Google Scholar] [CrossRef]
- LoPachin, R.M. The changing view of acrylamide neurotoxicity. Neurotoxicology 2004, 25, 617–630. [Google Scholar] [CrossRef]
- Lehning, E.J.; Balaban, C.D.; Ross, J.F.; Reid, M.A.; LoPachin, R.M. Acrylamide neuropathy. I. Spatiotemporal characteristics of nerve cell damage in rat cerebellum. Neurotoxicology 2002, 23, 397–414. [Google Scholar] [CrossRef]
- Spencer, P.S.; Schaumburg, H.H. A review of acrylamide neurotoxicity. Part II. Experimental animal neurotoxicity and pathologic mechanisms. Can. J. Neurol. Sci. 1974, 1, 152–169. [Google Scholar]
- Schaumburg, H.H.; Wiœniewski, H.M.; Spencer, P.S. Ultrastructural studies of the dying-back process. I. Peripheral nerve terminal and axon degeneration in systemic acrylamide intoxication. J. Neuropathol. Exp. Neurol. 1974, 33, 260–284. [Google Scholar] [CrossRef]
- Cavanagh, J.B. The “dying back” process. A common denominator in many naturally occurring and toxic neuropathies. Arch. Pathol. Lab. Med. 1979, 103, 659–664. [Google Scholar]
- Cavanagh, J.B. The significance of the “dying back” process in experimental and human neurological disease. Int. Rev. Exp. Pathol. 1964, 3, 219–267. [Google Scholar]
- Jones, H.B.; Cavanagh, J.B. The evolution of intracellular responses to acrylamide in rat spinal ganglion neurons. Neuropathol. Appl. Neurobiol. 1984, 10, 101–121. [Google Scholar] [CrossRef]
- Sterman, A.B.; Sheppard, R.C. A correlative neurobehavioral-morphological model of acrylamide neuropathy. Neurobehav. Toxicol. Teratol. 1983, 5, 151–159. [Google Scholar]
- Sterman, A.B. The role of the neuronal cell body in neurotoxic injury. Neurobehav. Toxicol. Teratol. 1982, 4, 493–494. [Google Scholar]
- Sterman, A.B. Acrylamide induces early morphologic reorganization of the neuronal cell body. Neurology 1982, 32, 1023–1026. [Google Scholar] [CrossRef]
- Sterman, A.B.; Sposito, N. Motoneuron axosomatic synapses are altered in axonopathy. J. Neuropathol. Exp. Neurol. 1984, 43, 201–209. [Google Scholar] [CrossRef]
- Sterman, A.B. Acrylamide-induced remodelling of perikarya in rat superior cervical ganglia. Neuropathol. Appl. Neurobiol. 1984, 10, 221–234. [Google Scholar] [CrossRef]
- Sterman, A.B. The pathology of toxic axonal neuropathy: A clinical-experimental link. Neurobehav. Toxicol. Teratol. 1984, 6, 463–466. [Google Scholar]
- Sterman, A.B.; Panasci, D.J.; Persons, W. Does pyruvate prevent acrylamide neurotoxicity? Implications for disease pathogenesis. Exp. Neurol. 1983, 82, 148–158. [Google Scholar] [CrossRef]
- Tandrup, T.; Braendgaard, H. Number and volume of rat dorsal root ganglion cells in acrylamide intoxication. J. Neurocytol. 1994, 23, 242–248. [Google Scholar] [CrossRef]
- DeGrandchamp, R.L.; Lowndes, H.E. Early degeneration and sprouting at the rat neuromuscular junction following acrylamide administration. Neuropathol. Appl. Neurobiol. 1990, 16, 239–254. [Google Scholar] [CrossRef]
- DeGrandchamp, R.L.; Reuhl, K.R.; Lowndes, H.E. Synaptic terminal degeneration and remodeling at the rat neuromuscular junction resulting from a single exposure to acrylamide. Toxicol. Appl. Pharmacol. 1990, 105, 422–433. [Google Scholar] [CrossRef]
- Suzuki, K.; Pfaff, L.D. Acrylamide neuropathy in rats. An electron microscopic study of degeneration and regeneration. Acta Neuropathol. 1973, 24, 197–213. [Google Scholar] [CrossRef]
- Madrid, R.G.; Ohnishi, A.; Hachisuka, K.; Murai, Y. Axonal sprouting of motor nerve in acrylamide-intoxicated rats with progressive weakness. Environ. Res. 1993, 60, 233–241. [Google Scholar] [CrossRef]
- Schaumburg, H.H.; Spencer, P.S. The neurology and neuropathology of the occupational neuropathies. J. Occup. Med. 1976, 18, 739–742. [Google Scholar] [CrossRef]
- Rampello, L.; Vecchio, I.; Malaguarnera, M.; Rampello, L. Axonal and demyelinating motor neuropathies. Differential diagnosis. Acta Med. Mediterr. 2012, 28, 139–140. [Google Scholar]
- Sickles, D.W.; Stone, J.D.; Friedman, M.A. Fast axonal transport: A site of acrylamide neurotoxicity? Neurotoxicology 2002, 23, 223–251. [Google Scholar] [CrossRef]
- LoPachin, R.M.; Barber, D.S.; He, D.; Das, S. Acrylamide inhibits dopamine uptake in rat striatal synaptic vesicles. Toxicol. Sci. 2006, 89, 224–234. [Google Scholar] [CrossRef]
- Salomone, S.; Waeber, C. Selectivity and specificity of sphingosine-1-phosphate receptor ligands: Caveats and critical thinking in characterizing receptor-mediated effects. Front. Pharmacol. 2011, 2, 9. [Google Scholar] [CrossRef]
- Yu, S.; Zhao, X.; Zhang, T.; Yu, L.; Li, S.; Cui, N.; Han, X.; Zhu, Z.; Xie, K. Acrylamide-induced changes in the neurofilament protein of rat cerebrum fractions. Neurochem. Res. 2005, 30, 1079–1085. [Google Scholar] [CrossRef]
- Zhang, L.; Gavin, T.; Barber, D.; LoPachin, R.M. Role of the Nrf2-ARE pathway in acrylamide neurotoxicity. Toxicol. Lett. 2011, 205, 1–7. [Google Scholar] [CrossRef]
- Zhu, Y.J.; Zeng, T.; Zhu, Y.B.; Yu, S.F.; Wang, Q.S.; Zhang, L.P.; Guo, X.; Xie, K.Q. Effects of acrylamide on the nervous tissue antioxidant system and sciatic nerve electrophysiology in the rat. Neurochem. Res. 2008, 33, 2310–2317. [Google Scholar] [CrossRef]
- Halliwell, B.; Gutteridge, J.M.C. Free Radicals in Biology and Medicine, 4th ed.; Clarendon Press: Oxford, UK, 2006. [Google Scholar]
- Maiese, K. Metabolic clues: Novel directives for broad treatment strategies. Oxid. Med. Cell. Longev. 2010, 3, 289. [Google Scholar] [CrossRef]
- Chen, J.C.; Schwartz, J. Neurobehavioral effects of ambient air pollution on cognitive performance in U.S. adults. Neurotoxicology 2009, 30, 231–239. [Google Scholar] [CrossRef]
- Mulloy, K.B. Two case reports of neurological disease in coal mine preparation plant workers. Am. J. Ind. Med. 1996, 30, 56–61. [Google Scholar] [CrossRef]
- Calleman, C.J.; Wu, Y.; He, F.; Tian, G.; Bergmark, E.; Zhang, S.; Deng, H.; Wang, Y.; Crofton, K.M.; Fennell, T.; Costa, L.G. Relationships between biomarkers of exposure and neurological effects in a group of workers exposed to acrylamide. Toxicol. Appl. Pharmacol. 1994, 126, 361–371. [Google Scholar] [CrossRef]
- Myers, J.E.; Macun, I. Acrylamide neuropathy in a South African factory: An epidemiologic investigation. Am. J. Ind Med. 1991, 19, 487–493. [Google Scholar] [CrossRef]
- Kesson, C.M.; Baird, A.W.; Lawson, D.H. Acrylamide poisoning. Postgrad. Med. J. 1977, 53, 16–17. [Google Scholar] [CrossRef]
- Garland, T.O.; Patterson, M.W. Six cases of acrylamide poisoning. Br. Med. J. 1967, 4, 134–138. [Google Scholar] [CrossRef]
- He, F.S.; Zhang, S.L.; Wang, H.L.; Li, G.; Zhang, Z.M.; Li, F.L.; Dong, X.M.; Hu, F.R. Neurological and electroneuromyographic assessment of the adverse effects of acrylamide on occupationally exposed workers. Scand. J. Work Environ. Health 1989, 15, 125–129. [Google Scholar] [CrossRef]
- Kjuus, H.; Goffeng, L.O.; Heier, M.S.; Sjöholm, H.; Ovrebø, S.; Skaug, V.; Paulsson, B.; Törnqvist, M.; Brudal, S. Effects on the peripheral nervous system of tunnel workers exposed to acrylamide and N-methylolacrylamide. Scand. J. Work Environ. Health 2004, 30, 21–29. [Google Scholar] [CrossRef]
- Goffeng, L.O.; Kjuus, H.; Heier, M.S.; Alvestrand, M.; Ulvestad, B.; Skaug, V. Colour vision and light sensitivity in tunnel workers previously exposed to acrylamide and N-methylolacrylamide containing grouting agents. Neurotoxicology 2008, 29, 31–39. [Google Scholar] [CrossRef]
- Rampello, L.; Vecchio, I.; Migliore, M.; Malaguarnera, M.; Malaguarnera, G.; Rampello, L. The most frequent medical and surgical neuralgias: Physiopathology and clinical pictures. Acta Med. Mediterr. 2012, 28, 109–111. [Google Scholar]
- Rampello, L.; Vecchio, I.; Malaguarnera, M.; Rampello, L. Restless legs sindrome. Acta Med. Mediterr. 2012, 28, 153. [Google Scholar] [CrossRef]
- Frazzetto, P.M.; Malaguarnera, G.; Gagliano, C.; Lucca, F.; Giordano, M.; Rampello, L.; Rampello, L.; Malaguarnera, M. Biohumoral tests in chronic pesticides exposure. Acta Med. Mediterr. 2011, 28, 237–246. [Google Scholar]
- Sayre, L.M.; Autilio-Gambetti, L.; Gambetti, P. Pathogenesis of experimental giant neurofilamentous axonopathies: A unified hypothesis based on chemical modification of neurofilaments. Brain Res. 1985, 357, 69–83. [Google Scholar]
- LoPachin, R.M.; Balaban, C.D.; Ross, J.F. Acrylamide axonopathy revisited. Toxicol. Appl. Pharmacol. 2003, 188, 135–153. [Google Scholar] [CrossRef]
- Godin, A.C.; Dubielzig, R.R.; Giuliano, E.; Ekesten, B. Retinal and optic nerve degeneration in cattle after accidental acrylamide intoxication. Vet. Ophthalmol. 2000, 3, 235–239. [Google Scholar] [CrossRef]
- Paulsson, B.; Larsen, K.O.; Törnqvist, M. Hemoglobin adducts in the assessment of potential occupational exposure to acrylamides—Three case studies. Scand. J. Work Environ. Health 2006, 32, 154–159. [Google Scholar] [CrossRef]
- Ahmed, H.H.; Elmegeed, G.A.; El Sayed, S.M.; Abd-Elhalim, M.M.; Shousha, W.G.; Shafic, R.W. Potent neuroprotective role of novel melatonin derivatives for management of central neuropathy induced by acrylamide in rats. Eur. J. Med. Chem. 2010, 45, 5452–5459. [Google Scholar] [CrossRef]
- Tareke, E.; Rydberg, P.; Karlsson, P.; Eriksson, S.; Törnqvist, M. Acrylamide: A cooking carcinogen? Chem. Res. Toxicol. 2000, 13, 517–522. [Google Scholar]
- Xi, C.Z. Long-term exposure to various types of dietary fat modulates acrylamide-induced preneoplastic lesions of colon mucosa through Wnt/beta-catenin signaling in rats. Toxicol. Mech. Meth. 2009, 19, 285–291. [Google Scholar] [CrossRef]
- Malaguarnera, M. Carnitine derivatives: Clinical usefulness. Curr. Opin. Gastroenterol. 2012, 28, 166–176. [Google Scholar] [CrossRef]
- Malaguarnera, M. Acetyl-l-carnitine in hepatic encephalopathy. Metab. Brain Dis. 2013, 28, 193–199. [Google Scholar] [CrossRef]
- Bucolo, C.; Marrazzo, G.; Platania, C.B.; Drago, F.; Leggio, G.M.; Salomone, S. Fortified extract of red berry, Ginkgo biloba, and white willow bark in experimental early diabetic retinopathy. J. Diabetes Res. 2013, 2013, 432695. [Google Scholar] [CrossRef]
- Li Volti, G.; Salomone, S.; Sorrenti, V.; Mangiameli, A.; Urso, V.; Siarkos, I.; Galvano, F.; Salamone, F. Effect of silibinin on endothelial dysfunction and ADMA levels in obese diabetic mice. Cardiovasc. Diabetol. 2011, 10, 62. [Google Scholar] [CrossRef]
- Levine, R.A.; Smith, R.E. Sources of variability of acrylamide levels in cracker model. J. Agric. Food Chem. 2005, 53, 4410–4416. [Google Scholar] [CrossRef]
- Casado, F.J.; Sanchez, A.H.; Montano, A. Reduction of acrylamide content of ripe olives by selected additives. Food Chem. 2010, 119, 161–166. [Google Scholar] [CrossRef]
- Mustafa, A.; Andersson, R.; Rosen, J.; Kamal-Eldin, A.; Aman, P. Factors influencing acrylamide content and color in rye crisp bread. J. Agric. Food Chem. 2005, 53, 5985–5989. [Google Scholar] [CrossRef]
- Keramat, J.; LeBail, A.; Prost, C.; Jafari, M. Acrylamide in baking products: A review article. Food Bioprocess. Technol. 2011, 4, 530–543. [Google Scholar] [CrossRef]
- Loeb, A.L.; Anderson, R.J. Antagonism of acrylamide neurotoxicity by supplementation with vitamin B6. Neurotoxicology 1981, 2, 625–633. [Google Scholar]
- Kemplay, S.; Martin, P.; Wilson, S. The effects of thioctic acid on motor nerve terminals in acrylamide-poisoned rats. Neuropathol. Appl. Neurobiol. 1988, 14, 275–288. [Google Scholar] [CrossRef]
- Sabri, M.I.; Dairman, W.; Fenton, M.; Juhasz, L.; Ng, T.; Spencer, P.S. Effect of exogenous pyruvate on acrylamide neuropathy in rats. Brain Res. 1989, 483, 1–11. [Google Scholar] [CrossRef]
- Saita, K.; Ohi, T.; Hanaoka, Y.; Furukawa, S.; Furukawa, Y.; Hayashi, K.; Matsukura, S. A catechol derivative (4-methylcatechol) accelerates the recovery from experimental acrylamide-induced neuropathy. J. Pharmacol. Exp. Ther. 1996, 276, 231–237. [Google Scholar]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Pennisi, M.; Malaguarnera, G.; Puglisi, V.; Vinciguerra, L.; Vacante, M.; Malaguarnera, M. Neurotoxicity of Acrylamide in Exposed Workers. Int. J. Environ. Res. Public Health 2013, 10, 3843-3854. https://doi.org/10.3390/ijerph10093843
Pennisi M, Malaguarnera G, Puglisi V, Vinciguerra L, Vacante M, Malaguarnera M. Neurotoxicity of Acrylamide in Exposed Workers. International Journal of Environmental Research and Public Health. 2013; 10(9):3843-3854. https://doi.org/10.3390/ijerph10093843
Chicago/Turabian StylePennisi, Manuela, Giulia Malaguarnera, Valentina Puglisi, Luisa Vinciguerra, Marco Vacante, and Mariano Malaguarnera. 2013. "Neurotoxicity of Acrylamide in Exposed Workers" International Journal of Environmental Research and Public Health 10, no. 9: 3843-3854. https://doi.org/10.3390/ijerph10093843
APA StylePennisi, M., Malaguarnera, G., Puglisi, V., Vinciguerra, L., Vacante, M., & Malaguarnera, M. (2013). Neurotoxicity of Acrylamide in Exposed Workers. International Journal of Environmental Research and Public Health, 10(9), 3843-3854. https://doi.org/10.3390/ijerph10093843