The Portrayal of Natural Environment in the Evolution of the Ecological Public Health Paradigm

Abstract
:1. Introduction
2. The Natural Environment in Increasingly Ecological Conceptions of Health
2.1. Public Health and the Environment
2.2. The Natural Environment Concept Finds Its Way into Ecological Models of Health






3. Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Field | Description |
|---|---|
| Conservation Medicine [40] | Connects ecosystem, animal, and human health, but is largely focused on infectious disease transmission exacerbated by human encroachment into animal habitat. |
| OneHealth [41] | “One Health is the collaborative effort of multiple disciplines-working locally, nationally, and globally to attain optimal health for people, animals and our environment” (p. 13). |
| EcoHealth [42] | Encompasses Conservation Medicine and OneHealth but also considers equity and development in a socio-ecological systems approach to health. |
| Human Ecology [38] | The study of human-environment interactions. Health has been considered as an outcome of these interactions. |
| Health Ecology [43] | Health ecology places health as the core concept in human ecology, the ultimate aim of which “...is the creation and maintenance of healthy people in healthy environments” (p. 17). |
| Ecotoxicology [44] | The study of the ecological products and mechanisms that have the potential to affect ecosystem functionality and cause illness. |
| Public Health Ecology [26] | Presents the natural environment as fundamental to health and denotes the reciprocal relationship between the natural and built environment. |
4. Conclusions
Conflicts of Interest
References
- Millennium Ecosystem Assessment. Ecosystems and Human Well-Being: Health Synthesis, WHO Publication: Geneva, Switzerland, 2005.
- De Groot, R.S.; Alkemade, R.; Braat, L.; Hein, L.; Willemen, L. Challenges in integrating the concept of ecosystem services and values in landscape planning, management and decision making. Ecol. Complex. 2010, 7, 260–272. [Google Scholar] [CrossRef]
- McCally, M. Life Support: The Environment and Human Health. In Environment, Health, and Risk; McCally, M., Ed.; MIT Press: Cambridge, MA, USA, 2002; pp. 1–14. [Google Scholar]
- Duhl, L.J.; Sanchez, A.K. Healthy Cities and the City Planning Process: A Background Document on Links between Health and Urban Planning; WHO Regional Office for Europe: Copenhagen, Denmark, 1999. [Google Scholar]
- Martensen, R. Landscape Designers, Doctors, and the Making of Healthy Urban Spaces in 19th Century America. In Restorative Commons: Creating Health and Well-being Through Urban Landscapes; Campbell, L., Wiesen, A., Eds.; U.S. Department of Agriculture, Forest Service, Northern Research Station: Newtown Square, PA, USA, 2009; pp. 26–37. [Google Scholar]
- Thompson, C.W. Linking landscape and health: The recurring theme. Landscape Urban Plan 2011, 99, 187–195. [Google Scholar] [CrossRef]
- Hebbert, M. A city in good shape: Town planning and public health. Town Plan. Rev. 1999, 70, 433–453. [Google Scholar]
- Ashton, J.; Ubido, B. The healthy city and the ecologic idea. J. Soc. Soc. Hist. Med. 1991, 41, 173–180. [Google Scholar] [CrossRef]
- Maslow, A.H. The Psychology of Science; Maurice Bassett: Richmond, CA, USA, 1966. [Google Scholar]
- Duhl, L.J. The Urban Condition: People and Policy in the Metropolis; Basic Books: New York, NY, USA, 1963. [Google Scholar]
- Antonovsky, A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well; Josey-Bass: Hoboken, NJ, USA, 1987. [Google Scholar]
- Ottawa Charter for Health Promotion; WHO: Geneva, Switzerland, 1986.
- Ashton, J. Sanitarian becomes ecologist: The new environmental health. BMJ Br. Med. J. 1991, 302, 189–190. [Google Scholar] [CrossRef]
- Morris, G.P.; Beck, S.A.; Hanlon, P.; Robertson, R. Getting strategic about the environment and health. Public Health 2006, 120, 889–903. [Google Scholar] [CrossRef]
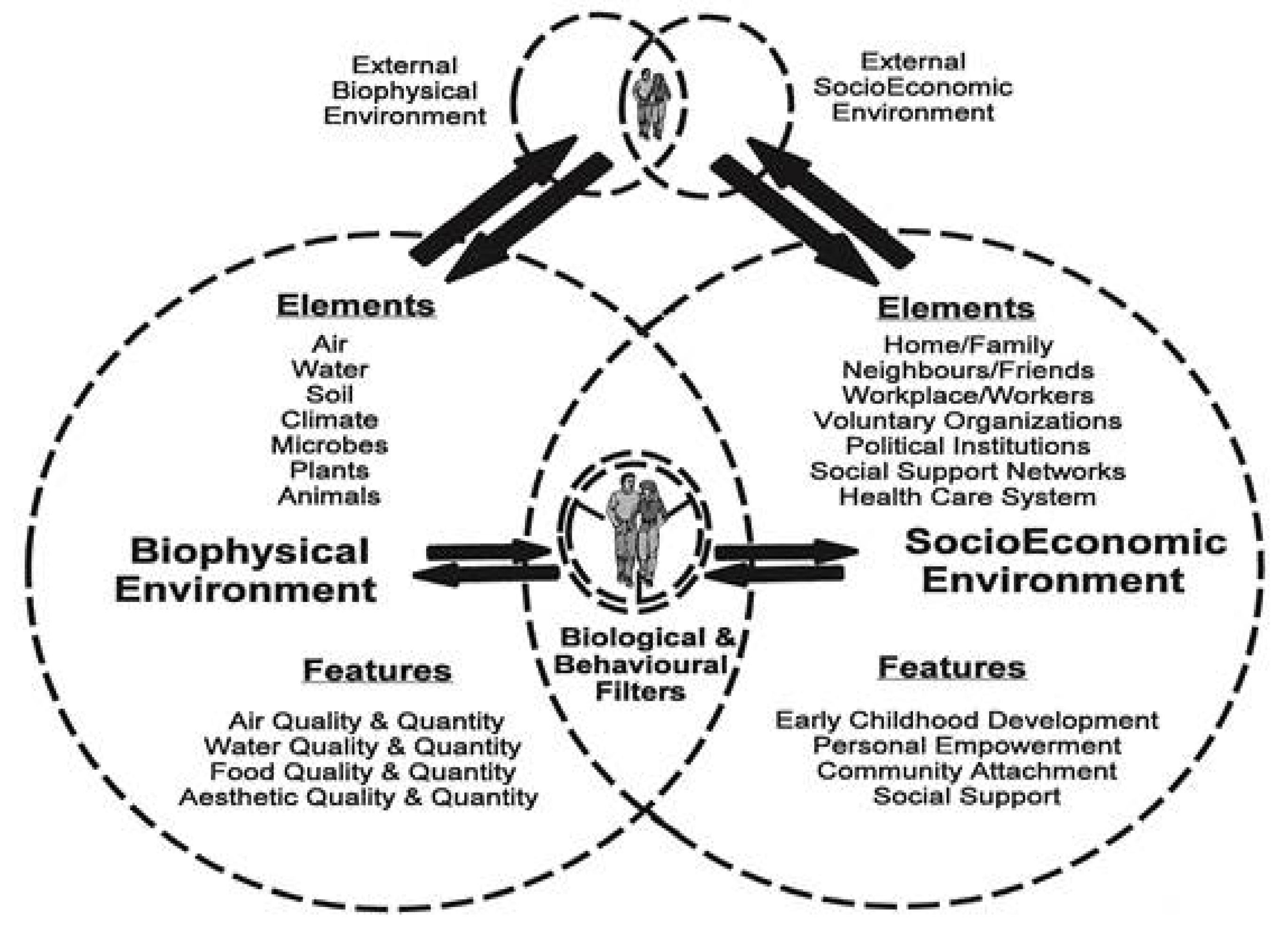
- VanLeeuwen, J.A.; Waltner-Toews, D.; Abernathy, T.; Smit, B. Evolving models of human health toward an ecosystem context. Ecosyst. Health 1999, 5, 204–219. [Google Scholar] [CrossRef]
- Green, L.W.; Richard, L.; Potvin, L. Ecological foundations of health promotion. Amer. J. Health Promot. 1996, 10, 270–281. [Google Scholar] [CrossRef]
- Heemskerk, M. Conceptual models as tools for communication across disciplines. Cons. Ecol. 2003, 7. Available online: http://www.consecol.org/vol7/iss3/art8 (accessed on 24 December 2013). [Google Scholar]
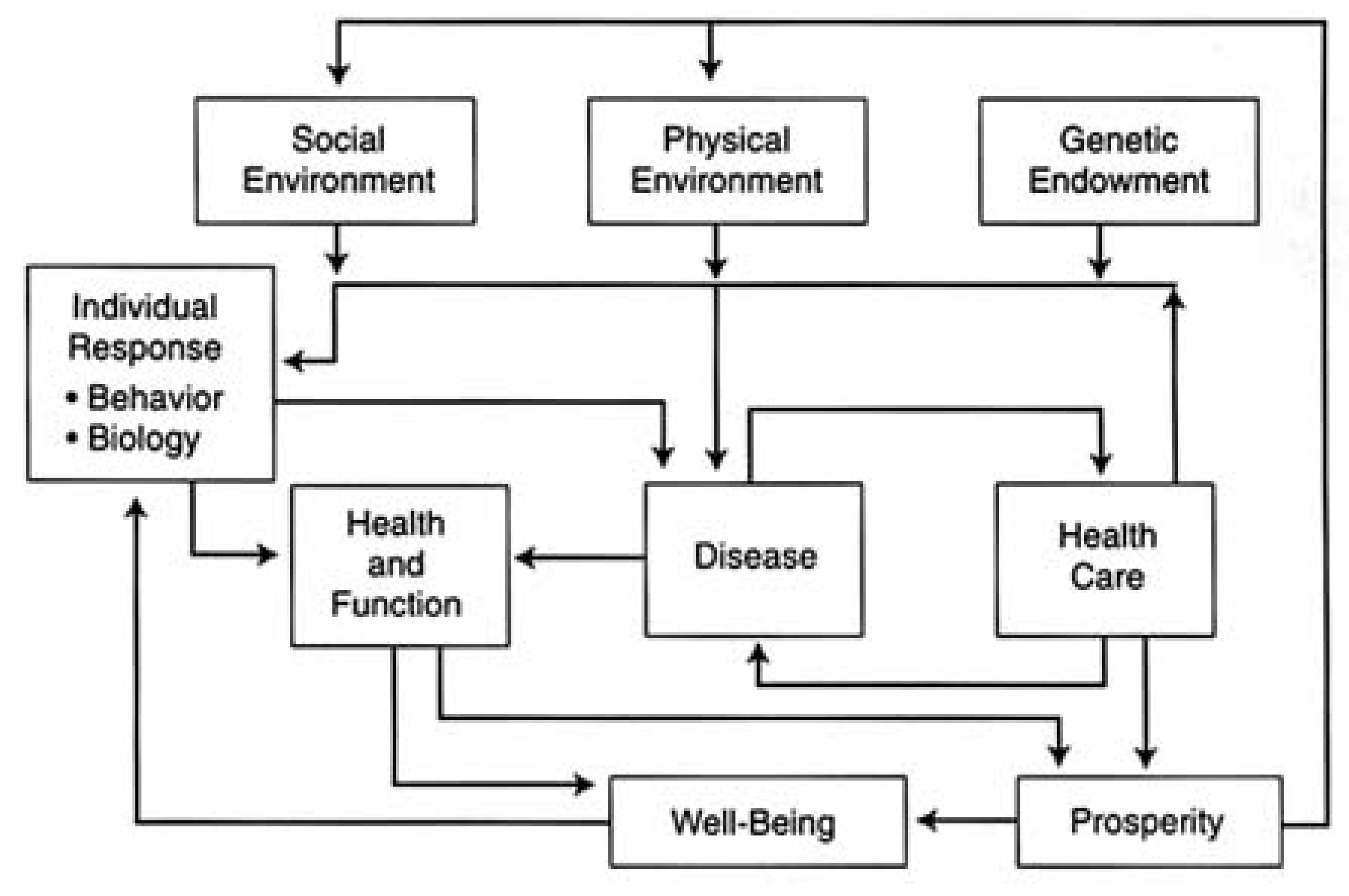
- Evans, R.; Stoddart, G. Producing health, consuming health care. Soc. Sci. Med. 1990, 31, 1347–1363. [Google Scholar] [CrossRef]
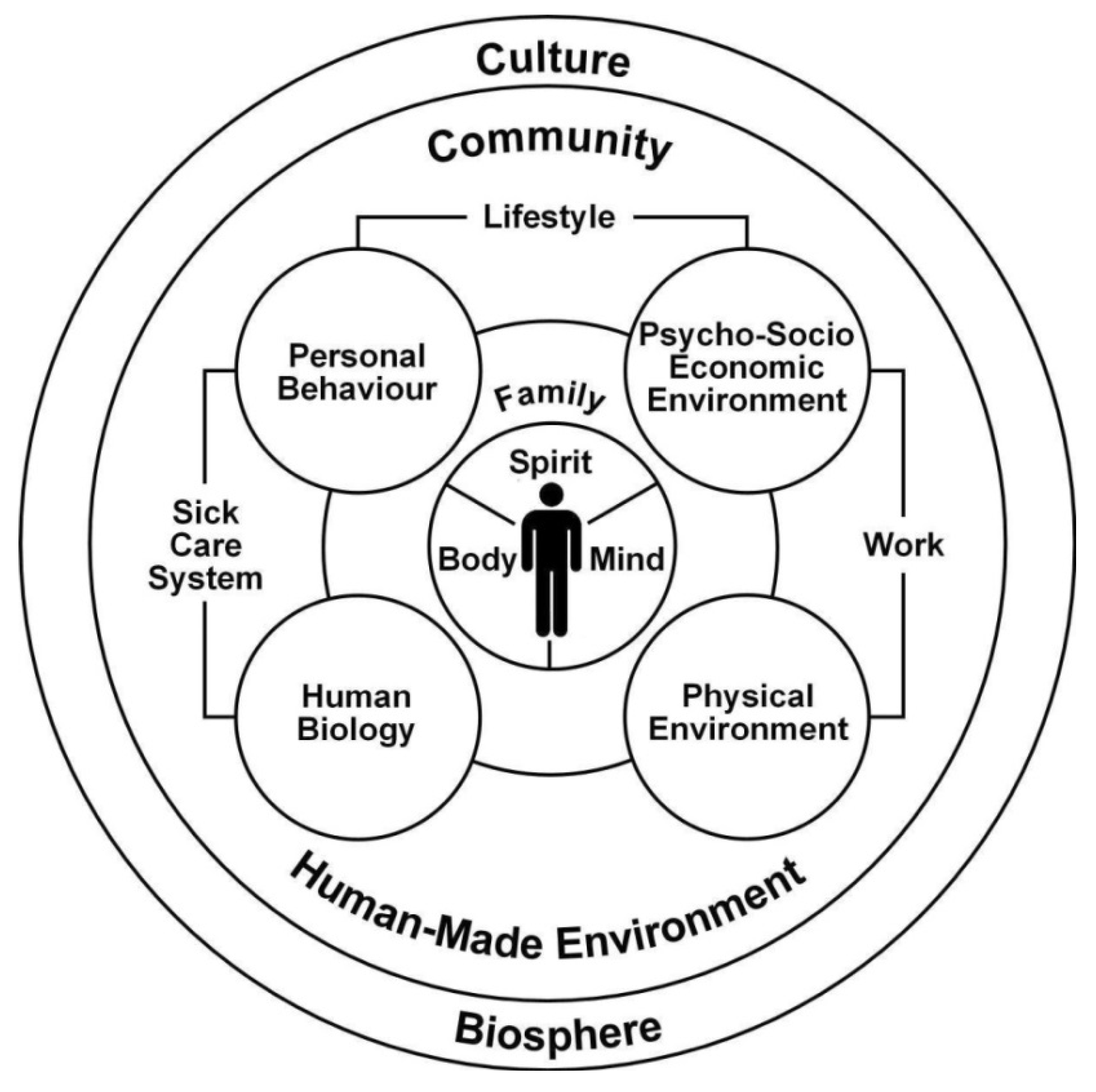
- Hancock, T.; Perkins, F. The mandala of health: A conceptual model and teaching tool. Health Educ. 1985, 24, 8–10. [Google Scholar]
- Hancock, T. The mandala of health: A model of the human ecosystem. Fam. Community Health 1985, 8, 1–10. [Google Scholar] [CrossRef]
- Hancock, T. Lalonde and beyond: Looking back at “A new perspective on the health of Canadians”. Health Promot. 1986, 1, 93–100. [Google Scholar] [CrossRef]
- Hancock, T. Health, human development and the community ecosystem: Three ecological models. Health Promot. Int. 1993, 8, 41–47. [Google Scholar]
- Kickbusch, I. Approaches to an ecological base for public health. Health Promot. Int. 1989, 4, 265–268. [Google Scholar] [CrossRef]
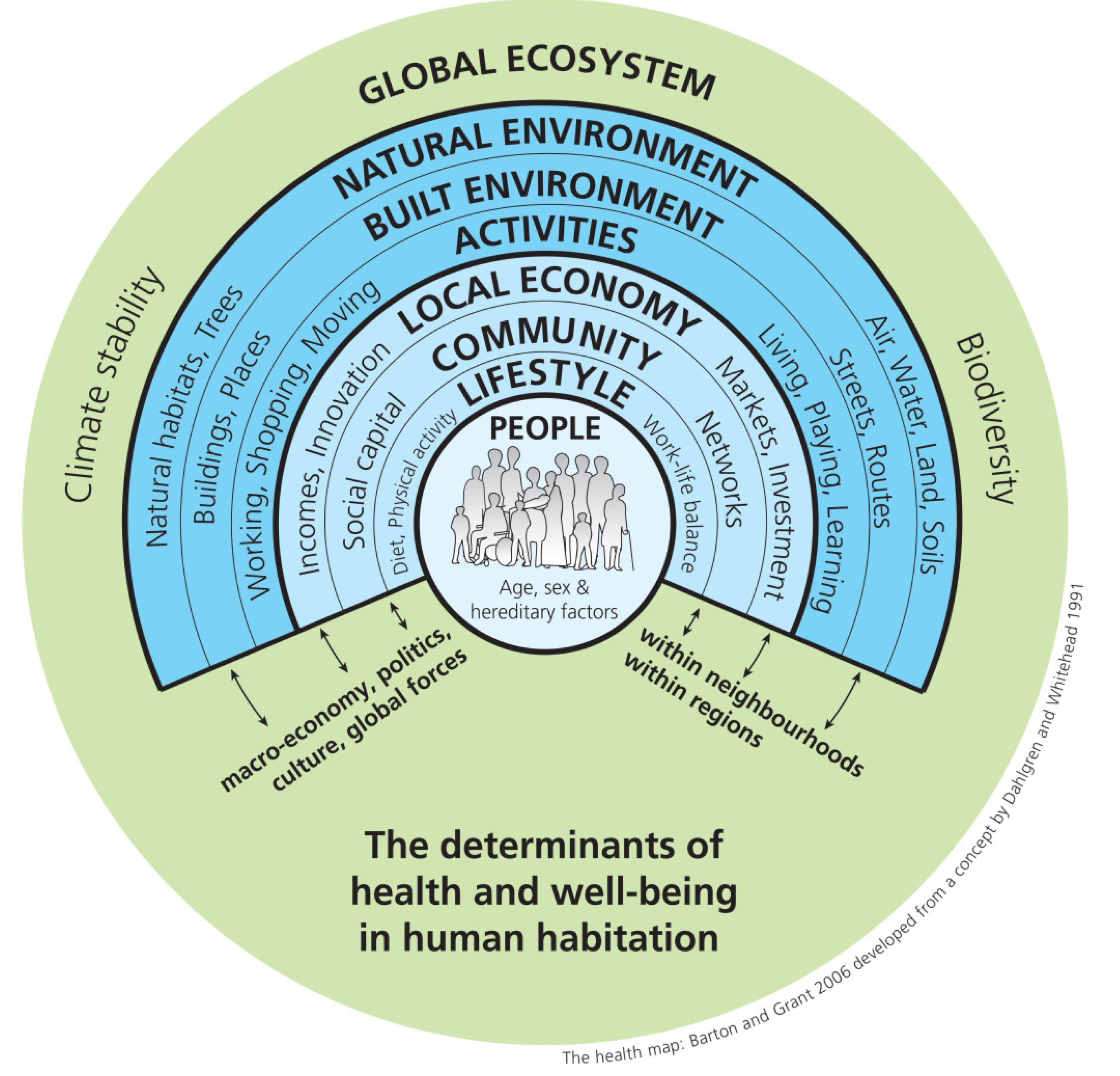
- Barton, H.; Grant, M. A health map for the local human habitat. J. R. Soc. Promot. Health 2006, 126, 252–253. [Google Scholar] [CrossRef]
- Dahlgren, G.; Whitehead, M. European Strategies for Tackling Social Inequities in Health: Levelling up Part 2; WHO Regional Office for Europe: Copenhagen, Denmark, 2007. [Google Scholar]
- Coutts, C. Public health ecology. J. Environ. Health 2010, 72, 53–55. [Google Scholar]
- McLeroy, K.; Bibeau, D.; Steckler, A.; Glanz, K. An ecological perspective on health promotion programs. Health Educ. Quart. 1988, 15, 351–377. [Google Scholar] [CrossRef]
- Liu, J.; Dietz, T.; Carpenter, S.R.; Alberti, M.; Folke, C.; Moran, E.; Pell, A.N.; Deadman, P.; Kratz, T.; Lubchenco, J.; et al. Complexity of coupled human and natural systems. Science 2007, 317, 1513–1516. [Google Scholar] [CrossRef]
- Liu, J.; Dietz, T.; Carpenter, S.; Folke, C. Coupled human and natural systems. Ambio 2007, 36, 639–649. [Google Scholar] [CrossRef]
- McConnell, W.J.; Millington, J.D.A.; Reo, N.J.; Alberti, M.; Asbjornsen, H.; Baker, L.A.; Brozović, N.; Drinkwater, L.E.; Drzyzga, S.A.; Fragoso, J.; et al. Research on coupled human and natural systems (CHANS): Approach, challenges, and strategies. Bull. Ecol. Soc. Am. 2011, 92, 218–228. [Google Scholar] [CrossRef]
- Millennium Ecosystem Assessment. Ecosystems and Human Well-being, Synthesis, Island Press: Washington DC, USA, 2005.
- Glaser, M.; Christie, P.; Diele, K.; Dsikowitzky, L.; Ferse, S.; Nordhaus, I.; Schlüter, A.; Mañez, K.S.; Wild, C. Measuring and understanding sustainability—Enhancing processes in tropical coastal and marine social-ecological systems. Curr. Opin. Environ. Sustain. 2012, 4, 300–308. [Google Scholar] [CrossRef]
- Pavao-Zuckerman, M. The conceptual utility of models in human ecology. J. Ecol. Anthropol. 2000, 4, 31–56. [Google Scholar] [CrossRef]
- Niemelä, J. Is there a need for a theory of urban ecology? Urban Ecosyst. 1999, 3, 57–65. [Google Scholar]
- Pickett, S.; Cadenasso, M.; Grove, J. Urban ecological systems: Linking terrestrial ecological, physical, and socioeconomic components of metropolitan areas. Rev. Ecol. 2001, 32, 127–157. [Google Scholar] [CrossRef]
- Tomalak, M.; Rossi, E.; Ferrini, F.; Moro, P. Negative Aspects and Hazardous Effects of Forest Environment on Human Health. In Forests, Trees and Human Health; Nilsson, K., Sangster, M., Gallis, C., Sartig, T., de Vries, S., Seeland, K., Schipperijn, J., Eds.; Springer Verlag: New York, NY, USA, 2011; pp. 77–124. [Google Scholar]
- Frumkin, H. Beyond toxicity: Human health and the natural environment. Amer. J. Prev. Med. 2001, 20, 234–240. [Google Scholar] [CrossRef]
- Parkes, M.; Panelli, R.; Weinstein, P. Converging paradigms for environmental health theory and practice. Environ. Health Perspect. 2003, 111, 669–675. [Google Scholar] [CrossRef]
- Coutts, C.; Taylor, C. Putting the capital “E” environment into ecological models of health. J. Environ. Health 2011, 74, 26–29. [Google Scholar]
- Aguirre, A.; Ostfeld, R.; Tabor, G.; House, C.; Pearl, M. Conservation Medicine: Ecological Health in Practice; Oxford University Press: New York, NY, USA, 2002. [Google Scholar]
- American Veterinary Medical Association. One Health: A New Professional Imperative. 2008. Available online: https://www.avma.org/KB/Resources/Reports/Documents/onehealth_final.pdf (accessed on 26 December 2013).
- Wilcox, B.A.; Aguirre, A.; Daszak, P.; Horwitz, P.; Martens, P.; Parkes, M.; Patz, J.A.; Waltner-Toews, D. EcoHealth: A transdisciplinary imperative for a sustainable future. Ecohealth 2004, 1, 3–5. [Google Scholar] [CrossRef]
- Honari, M.; Boleyn, T. Health Ecology: Health, Culture, and Human-environment Interaction; Routledge: London, UK/New York, NY, USA, 1999. [Google Scholar]
- DiGiulio, R.T.; Monosson, E. Interconnections between Ecosystem and Human Health; Chapman & Hall: London, UK, 1996. [Google Scholar]
- Benedict, M.; McMahon, E.T. Green Infrastructure: Smart Conservation for the 21st Century; Sprawl Watch Clearinghouse: Washington DC, USA, 2002. [Google Scholar]
- Sloane, D.C. From congestion to sprawl. J. Amer. Plan. Assn. 2006, 72, 10–18. [Google Scholar] [CrossRef]
- Brundtland, G. Our Common Future. Available online: http://www.un-documents.net/our-common-future.pdf (accessed December 27 2013).
- Secretariat of the Convention on Biological Diversity. Global Biodiversity Outlook 3. Available online: www.cbd.int/GBO3 (accessed on 14 December 2013).
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Coutts, C.; Forkink, A.; Weiner, J. The Portrayal of Natural Environment in the Evolution of the Ecological Public Health Paradigm. Int. J. Environ. Res. Public Health 2014, 11, 1005-1019. https://doi.org/10.3390/ijerph110101005
Coutts C, Forkink A, Weiner J. The Portrayal of Natural Environment in the Evolution of the Ecological Public Health Paradigm. International Journal of Environmental Research and Public Health. 2014; 11(1):1005-1019. https://doi.org/10.3390/ijerph110101005
Chicago/Turabian StyleCoutts, Christopher, Annet Forkink, and Jocelyn Weiner. 2014. "The Portrayal of Natural Environment in the Evolution of the Ecological Public Health Paradigm" International Journal of Environmental Research and Public Health 11, no. 1: 1005-1019. https://doi.org/10.3390/ijerph110101005
APA StyleCoutts, C., Forkink, A., & Weiner, J. (2014). The Portrayal of Natural Environment in the Evolution of the Ecological Public Health Paradigm. International Journal of Environmental Research and Public Health, 11(1), 1005-1019. https://doi.org/10.3390/ijerph110101005