Adaptive Tele-Therapies Based on Serious Games for Health for People with Time-Management and Organisational Problems: Preliminary Results




Abstract
:1. Introduction
2. Background
2.1. Serious Games for Health and ADHD
2.1.1. Diagnosis and Evaluation
2.1.2. Treatment

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Game Name | Year | Country | Type | Goal | Technologies |
|---|---|---|---|---|---|---|
| Pope and Bogart [36] | - | 1994 | US | Development | Fostering attention | EEG, PC |
| Peter Freer [45] | Play Attention | 2000 | US | Development/In Use | Fostering attention | EEG, PC |
| Kerns [32] | Cyber-Cruiser | 2000 | CA | Development | Evaluating executive functioning and prospective memory | PC |
| Pope and Palsson [37] | 2001 | US | Commercial videogame adaptation | Fostering attention | Play Station, EEG | |
| Bell, Smith et al. [38] | The Journey to Wild Divine | 2003 | US | Commercial | Relaxation, Mindfulness | Biofeedback, PC |
| Rizzo, Bewerly et al. [30] | - | 2004 | US | Development | ADHD diagnosis | 3D virtual classroom, PC |
| Coyle, Sharry et al. [43] | Personal Investigator | 2005 | IE | Development | Focused Solution Therapies | Virtual world, PC |
| Andrade et al. [28,29] | Supermarket game | 2006 | BR | Development | ADHD diagnosis | PC |
| Conconi, Jiménez et al. [41,42] | Play Mancer | 2007 | EU | Development | Creating a common framework for Serious Games-based therapies | Virtual world, PC |
| Van Dijk, Hunneman et al. [40] | Self-City | 2008 | NL | Development | Fostering social skills | PC |
| Bartle [34,35] | Cognitive Carnival | 2012 | CA | Development | Executive memory | PC |
| Bartle [34,35] | Caribbean Quest | 2012 | CA | Development | Executive memory | PC |
| Rubia et al. [39] | - | 2012 | GB | Development | Self-control | MRI, Virtual helicopter |
| Díaz-Orueta, García-López et al. [31] | AULA Nesplora | 2013 | ES | Development/In Use | Testing attention: Conners’ CPT | 3D virtual classroomPC |
| Authors | Year | Country | Participants | Method | Assessment | Result |
|---|---|---|---|---|---|---|
| Abikoff, Gallagher
et al. [46] | 2013 | US | 158 Children: 64 Organisational Skills Training 61 Precluded Skills training 33 Wait-List Control | 20 individual clinic-based sessions 10–12 weeks | 1 month post-treatment 2 in the following school year Measures: Organizational Skills Training (OST) Children’s Organisational Skills Scale for Parents (COSS-Parent) Children’s Organisational Skills Scale for Teachers (COSS-Teacher) | Promises clinical utility in children with ADHD and organisational deficits |
| Langberg, Becker et al. [47] | 2013 | US | 23 Children | Homework, Organisation and Planning Skills Intervention (HOPS) Included demographic and child characteristics | Parent-rated materials organisation and planning skills | Importance of teaching students with ADHD to use structured organisation systems |
| Pfiffner, Villodas
et al. [48] | 2013 | US | 57 Children (mean age 8.1 years) 17 girls 40 boys | Collaborative Life Skills Programme (CLS Programme) 10 schools 3 integrated components over 12 weeks | - | Support the focus of CLS on both ADHD symptom reduction and organisational skills improvement |
| Parker, Hoffman et al. [49] | 2013 | US | 19 students | 10 different US campuses One-on-one interviews | Learning and Strategies Inventory | ADHD helped participants to enhance their self-control |
| Field, Parker et al. [50] | 2013 | US | 160 college students: 70 Female 90 Male | Weekly phone-based coaching interviews | Learning and Study Strategies Inventory (LASSI) College Well-Being Scale | Statistically significant higher total scores in both scales |
| Hart, Radua
et al. [51] | 2012 | UK | 150 patients 145 healthy controls | Peak coordinates extracted from: Case-control activation differences Demographic, clinical and methodological variables | Meta regression analyses | Suggests potential normalisation effects on the function of the pre-frontal region with long-term psycho-stimulant treatment |
| Bioulac, Lallemand et al. [52] | 2012 | US | 36 boys 20 ADHD 16 controls | Virtual classroom task | Continuous Performance Test (CPT) | Children with ADHD are vulnerable to time-on-task effect on performance |
| Langberg, Epstein
et al. [53] | 2012 | US | 37 middle school students with ADHD 24 HOPS intervention 13 wait-list control | HOPS Intervention 3-month follow-up | Parent and teacher ratings of organisational skills and homework problems were collected. School grades were also collected | Intervention participants did not make significant improvements relative to the comparison group according to teacher ratings |
| Gureasko-Moore, DuPaul et al. [54] | 2008 | US | 3 male students enrolled in a public secondary school | Training in self-management procedures. | - | Results were consistent across the 3 participants. |
2.2. Time Management and Organisational Skills in ADHD
3. Materials and Methods
3.1. Participants
3.2. Methods
| Section | Interpretation |
|---|---|
| F1 | This section describes students’ willingness to prioritise and select tasks, in order to obtain specific goals. High scores in this section show an effective task prioritisation. |
| F2 | Area 2 contains the items related to the use of specific techniques associated with effective time management. High scores on this section indicate effective time management skills using specific techniques. |
| F3 | This section evaluates the way subjects organise their time, and how their study environment is structured. High scores in this section indicate a preference for a disorganised environment. |
| F4 | This area shows the degree of control users perceive to have over their own time. High scores in this area indicate a high control over their time. |
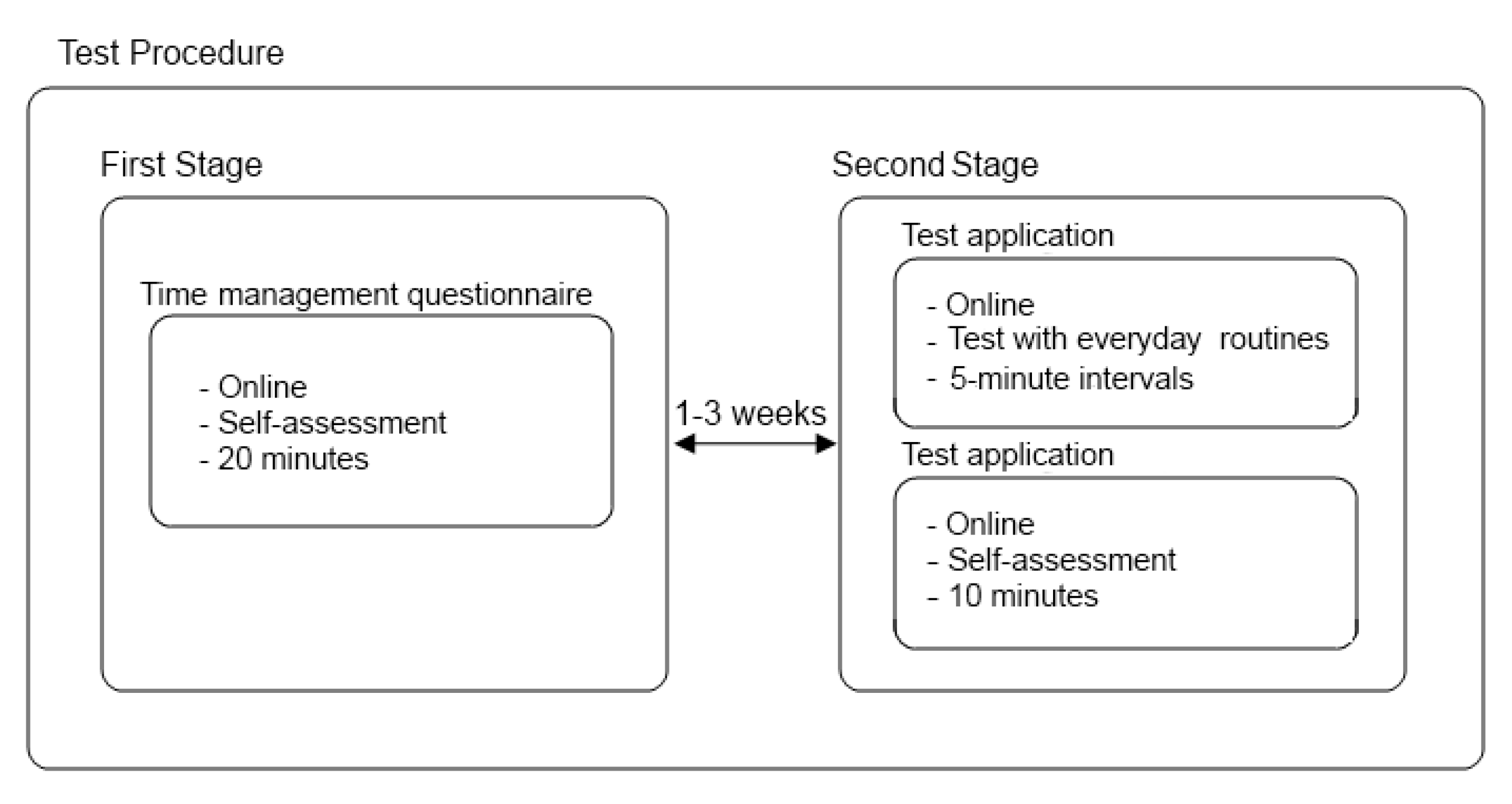
3.3. Experiment Description

4. Results
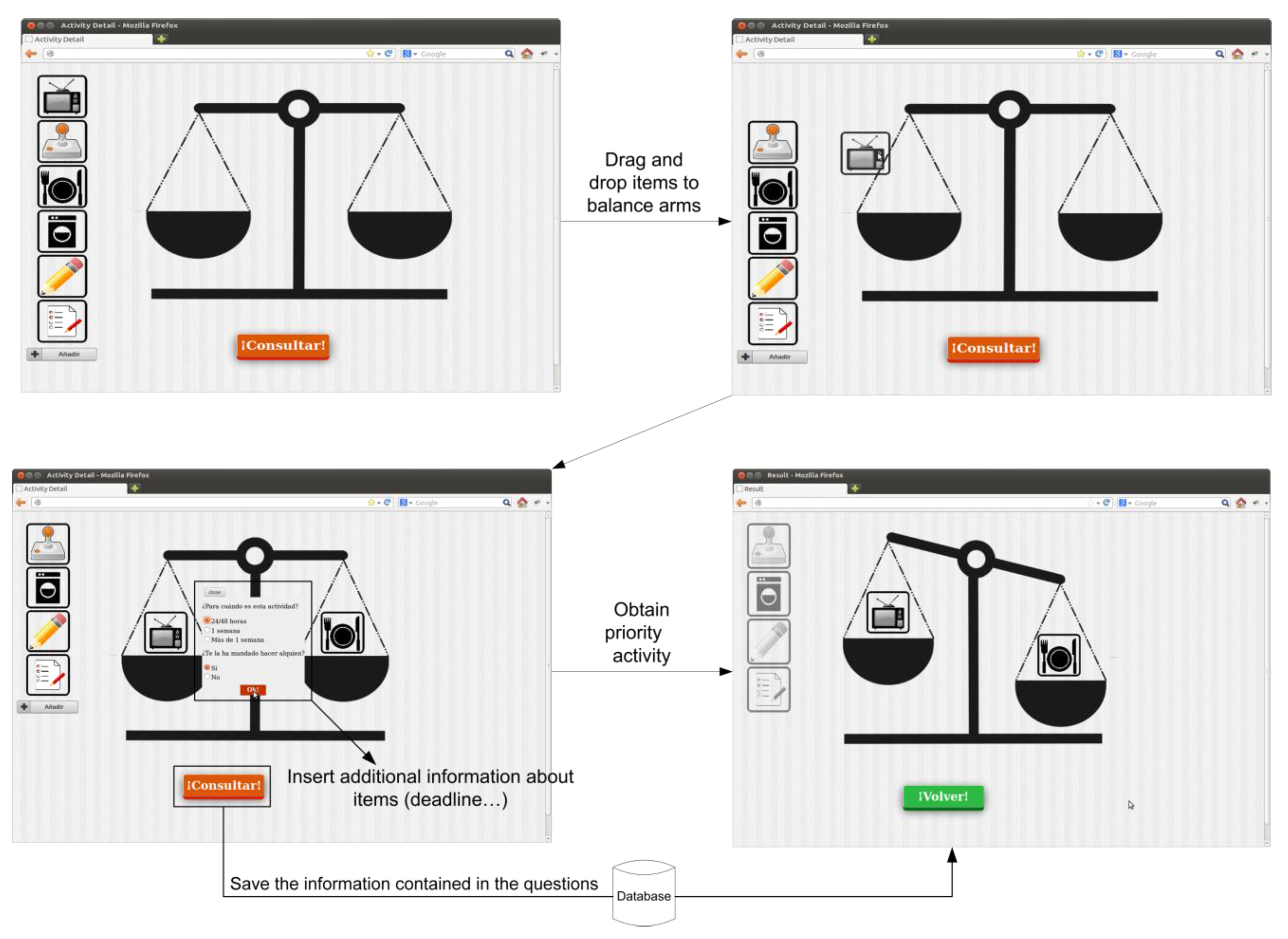
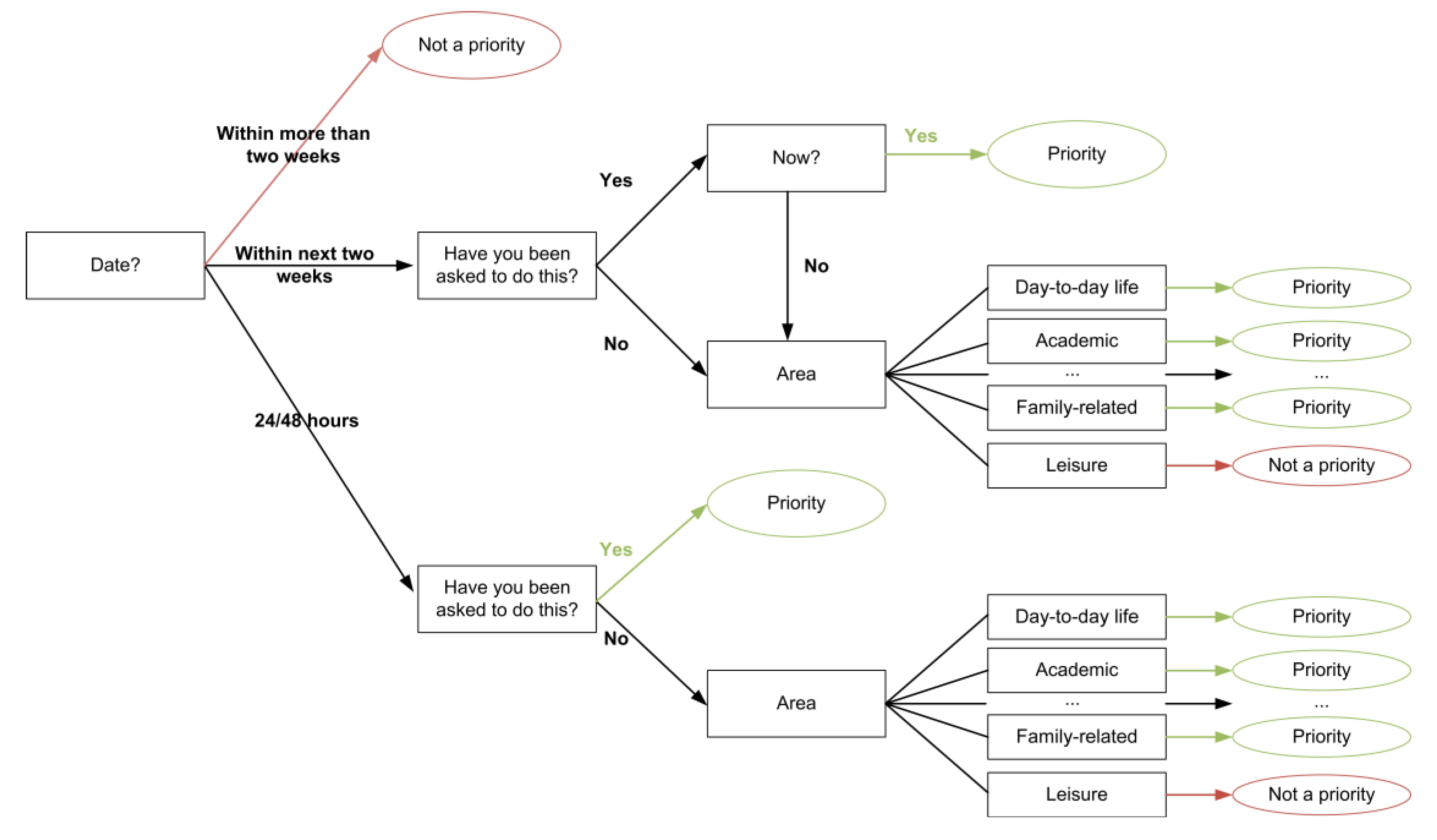
4.1. Technological Results: Tele-Therapy System




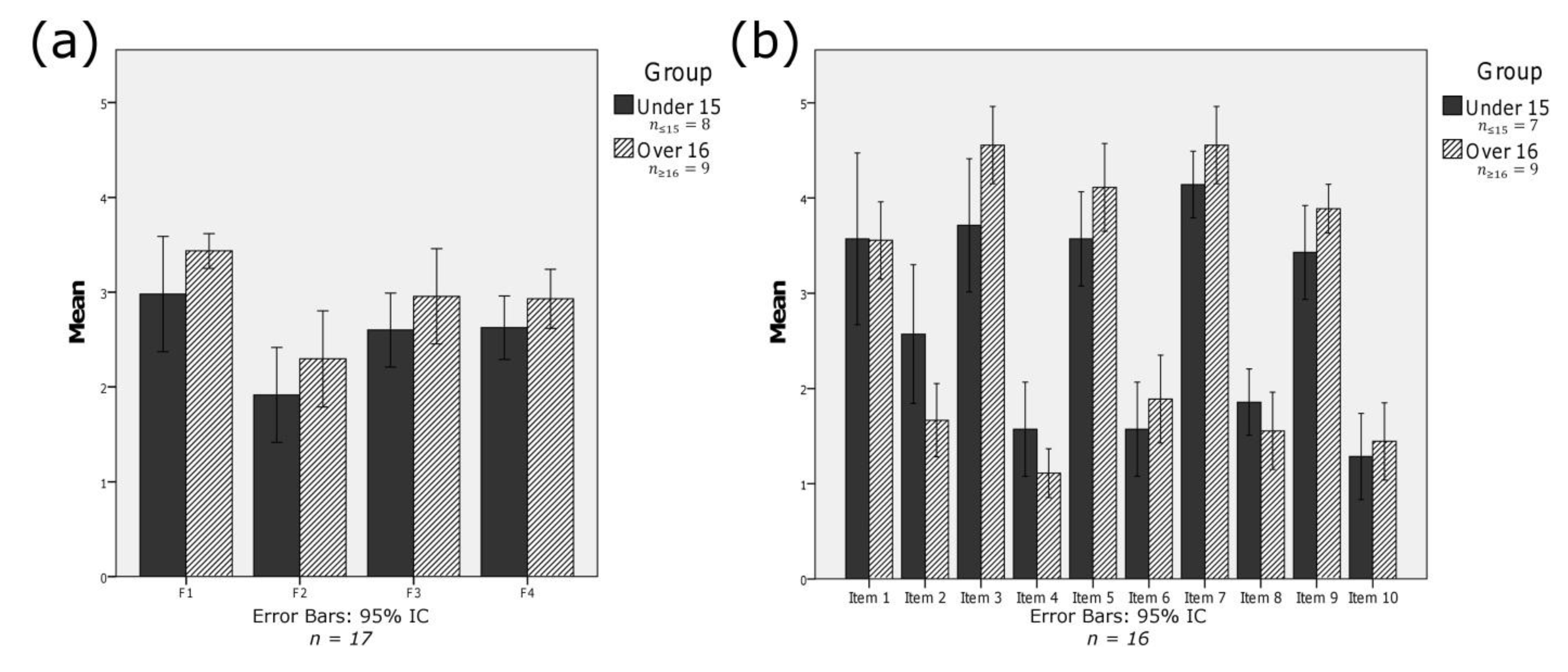
4.2. User Experience Evaluation



5. Discussion and Conclusions
- With a higher number of users.
- With users with and without an ADHD diagnosis.
- With the segmentation of participants into two age groups.
- Developing a bilingual or trilingual tool that allows the study to be replicated in other national and international territories in where reported diagnosis of ADHD is significantly different from the Basque Country, Spain.
- Performing a longitudinal study on the impact of online game-based tools on time management skills in teenagers with and without ADHD.
Acknowledgments
Conflicts of Interest
References
- Polanczyk, G.; de Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Amer. J. Psychiat. 2007, 164, 942–948. [Google Scholar] [CrossRef]
- Guía de Práctica Clínica sobre el Trastorno por Déficit de Atención con Hiperactividad (TDAH) en Niños y Adolescentes; Ministry of Health, Social Policy and Equality: Madrid, Spain, 2010.
- Pardey, M.C.; Kumar, N.N.; Goodchild, A.K.; Clemens, K.J.; Homewood, J.; Cornish, J.L. Long-term effects of chronic oral Ritalin administration on cognitive and neural development in adolescent Wistar Kyoto rats. Brain Sci. 2012, 2, 375–404. [Google Scholar] [CrossRef]
- Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Arlington, VA, USA, 2000; Volume 4, p. 943.
- Houghton, S.; Durkin, K.; Ang, R.P.; Taylor, M.F.; Brandtman, M. Measuring temporal self-regulation in children with and without attention deficit hyperactivity disorder: Sense of time in everyday contexts. Eur. J. Psychol. Assess. 2011, 27, 88–94. [Google Scholar] [CrossRef]
- Barkley, R.A. Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychol. Bull. 1997, 121, 65–94. [Google Scholar] [CrossRef]
- Barkley, R.A.; Koplowitz, S.; Anderson, T.; McMurray, M.B. Sense of time in children with ADHD: Effects of duration, distraction, and stimulant medication. J. Int. Neuropsychol. Soc. 1997, 3, 359–369. [Google Scholar]
- Barkley, R.A.; Murphy, K.R.; Bush, T. Time perception and reproduction in young adults with attention deficit hyperactivity disorder. Neuropsychology 2001, 15, 351–360. [Google Scholar] [CrossRef]
- Toplak, M.E.; Rucklidge, J.J.; Hetherington, R.; John, S.C.F.; Tannock, R. Time perception deficits in attention-deficit/hyperactivity disorder and comorbid reading difficulties in child and adolescent samples. J. Child Psychol. Psychiat. 2003, 44, 888–903. [Google Scholar] [CrossRef]
- Carelli, M.G.; Forman, H.; Mäntylä, T. Sense of time and executive functioning in children and adults. Child Neuropsychol. 2007, 14, 1–15. [Google Scholar] [CrossRef]
- Toplak, M.E.; Dockstader, C.; Tannock, R. Temporal information processing in ADHD: Findings to date and new methods. J. Neurosci. Meth. 2006, 151, 15–29. [Google Scholar] [CrossRef]
- González-Garrido, A.A.; Gómez-Velázquez, F.R.; Zarabozo, D.; López-Elizalde, R.; Ontiveros, A.; Madera-Carrillo, H.; Vega, O.L.; de Alba, J.L.; Tuya, J.M. Time reproduction disturbances in ADHD children: An ERP study. Int. J. Neurosci. 2008, 118, 119–135. [Google Scholar] [CrossRef]
- Meaux, J.B.; Chelonis, J.J. Time perception differences in children with and without ADHD. J. Pediatr. Health Care 2003, 17, 64–71. [Google Scholar]
- Meaux, J.B.; Chelonis, J.J. The relationship between behavioral inhibition and time perception in children. J. Child Adolesc. Psychiatr. Nurs. 2005, 18, 148–160. [Google Scholar] [CrossRef]
- Smith, A.; Taylor, E.; Rogers, J.W.; Newman, S.; Rubia, K. Evidence for a pure time perception deficit in children with ADHD. J. Child Psychol. Psychiat. 2002, 43, 529–542. [Google Scholar] [CrossRef]
- Radonovich, K.J.; Mostofsky, S.H. Duration judgments in children with ADHD suggest deficient utilization of temporal information rather than general impairment in timing. Child Neuropsychol. 2004, 10, 162–172. [Google Scholar]
- Langberg, J.M.; Epstein, J.N.; Graham, A.J. Organizational-skills interventions in the treatment of ADHD. Expert Rev. Neurother. 2008, 8, 1549–1561. [Google Scholar] [CrossRef]
- Turgay, A.; Goodman, D.W.; Asherson, P.; Lasser, R.A.; Babcock, T.F.; Pucci, M.L.; Barkley, R. Lifespan persistence of ADHD: The life transition model and its application. J. Clin. Psychiat. 2012, 73, 192–201. [Google Scholar] [CrossRef]
- Dovis, S.; van der Oord, S.; Wiers, R.W.; Prins, P.J. Can motivation normalize working memory and task persistence in children with attention-deficit/hyperactivity disorder? The effects of money and computer-gaming. J. Abnorm. Child Psychol. 2011, 40, 669–681. [Google Scholar]
- Prins, P.J.; Dovis, S.; Ponsioen, A.; ten Brink, E.; van der Oord, S. Does computerized working memory training with game elements enhance motivation and training efficacy in children with ADHD? Cyberpsychol. Behav. Soc. Netw. 2011, 14, 115–122. [Google Scholar] [CrossRef]
- Nelson, E.L.; Duncan, A.B.; Peacock, G.; Bui, T. Telemedicine and adherence to national guidelines for ADHD evaluation: A case study. Psychol. Serv. 2012, 9, 293–297. [Google Scholar]
- Palmer, N.B.; Myers, K.M.; van der Stoep, A.; McCarty, C.A.; Geyer, J.R.; Desalvo, A. Attention-deficit/hyperactivity disorder and telemental health. Curr. Psychiatry Rep. 2010, 12, 409–417. [Google Scholar]
- Wilkinson, N.; Ang, R.P.; Goh, D.H. Online video game therapy for mental health concerns: A review. Int. J. Soc. Psychiatr. 2008, 54, 370–382. [Google Scholar] [CrossRef]
- Geurts, H.M.; Luman, M.; van Meel, C.S. What’s in a game: The effect of social motivation on interference control in boys with ADHD and autism spectrum disorders. J. Child Psychol. Psychiat. 2008, 49, 848–857. [Google Scholar] [CrossRef]
- Bioulac, S.; Arfi, L.; Bouvard, M.P. Attention deficit/hyperactivity disorder and video games: A comparative study of hyperactive and control children. Eur. Psychiat. 2008, 23, 134–141. [Google Scholar] [CrossRef]
- Frölich, J.; Lehmkuhl, G.; Döpfner, M. Computer games in childhood and adolescence: Relations to addictive behavior, ADHD, and aggression. Z. Kinder Jugendpsychiatr. Psychother 2009, 37. [Google Scholar] [CrossRef]
- Ferguson, C.J. The influence of television and video game use on attention and school problems: A multivariate analysis with other risk factors controlled. J. Psychiatr. Res. 2011, 45, 808–813. [Google Scholar] [CrossRef]
- Santos, F.E.G.; Bastos, A.P.Z.; Andrade, L.C.V.; Revoredo, K.; Mattos, P. Assessment of ADHD through a Computer Game: An Experiment with a Sample of Students. In Proceedings of Third International Conference on Games and Virtual Worlds for Serious Applications (IEEE), Athens, Greece, 4–6 May 2011; pp. 104–111.
- De Andrade, L.C.V.; Carvalho, L.A.V.; Lima, C.; Cruz, A.; Mattos, P.; Franco, C.; Grieco, B. Supermarket Game: An Adaptive Intelligent Computer Game for Attention Deficit/Hyperactivity Disorder Diagnosis. In Proceedings of Fifth Mexican International Conference on Artificial Intelligence (IEEE), Apizaco, Mexico, November 2006; pp. 359–365.
- Rizzo, A.A.; Bowerly, T.; Shahabi, C.; Buckwalter, J.G.; Klimchuk, D.; Mitura, R. Diagnosing attention disorders in a virtual classroom. Computer 2004, 6, 87–89. [Google Scholar]
- Díaz-Orueta, U.; Garcia-López, C.; Crespo-Eguílaz, N.; Sánchez-Carpintero, R.; Climent, G.; Narbona, J. AULA virtual reality test as an attention measure: Convergent validity with Conners’ Continuous Performance Test. Child Neuropsychoogy 2013, 1–15. [Google Scholar] [CrossRef]
- Kerns, K.A. The CyberCruiser: An investigation of development of prospective memory in children. J. Int. Neuropsychol. Soc. 2000, 6, 62–70. [Google Scholar] [CrossRef]
- Kerns, K.A.; Price, K.J. An investigation of prospective memory in children with ADHD. Child Neuropsychol. 2001, 7, 162–171. [Google Scholar] [CrossRef]
- Bartle, D.W. Development of cognitive video games for children with attention and memory impairment. PhD Thesis, University of Victoria, Victoria, BC, Canada, 2010. [Google Scholar]
- Pei, J.; Kerns, K. Using games to improve functioning in children with fetal alcohol spectrum disorders. Game. Health. J. 2012, 1, 308–311. [Google Scholar] [CrossRef]
- Pope, A.T.; Bogart, E.H. Method of Encouraging Attention by Correlating Video Game Difficulty with Attention Level. U.S. Patent 5377100, 27 December 1994. [Google Scholar]
- Palsson, O.S.; Harris, R.L., Sr.; Pope, A.T. Method and Apparatus for Encouraging Physiological Self-Regulation through Modulation of an Operator’s Control Input to a Video Game or Training Simulator. U.S. Patent 6450820, 17 September 2002. [Google Scholar]
- Bell, C. The Journey to Wild Divine; The Wild Divine Project: Las Vegas, NV, USA, 2003. [Google Scholar]
- Statements, F.; Lives, T.; Bear, P.; McCall, D.; Bruce, F.; Harper, D.; McCabe, K.; Murnaghan, D.; Hadley, T.; Fry, M.; et al. Helping children affected by disability and infections Action Medical Research for children; Action Medical Research: Horsham, UK, 2012. [Google Scholar]
- Van Dijk, D.; Hunneman, R.; Wildlevuur, S. Self City: Training Social Skills in a Game. In Proceedings of Second European Conferences on Game-based Learning, Barcelona, Spain, October 2008; pp. 481–488.
- Conconi, A.; Ganchev, T.; Kocsis, O.; Papadopoulos, G.; Fernández-Aranda, F.; Jiménez-Murcia, S. PlayMancer: A Serious Gaming 3D Environment. In Proceedings of the International Conference on Automated Solutions for Cross Media Content and Multi-Channel Distribution, Florence, Italy, 17–19 November 2008; pp. 111–117.
- Jiménez-Murcia, S.; Fernández-Aranda, F.; Kalapanidas, E.; Konstantas, D.; Ganchev, T.; Kocsis, O.; Lam, T.; Santamaría, J.J.; Raguin, T.; Breiteneder, C.; et al. PlayMancer project: A serious videogame as an additional therapy tool for eating and impulse control disorders. Stud. Health Technol. Inform. 2009, 144, 163–166. [Google Scholar]
- Coyle, D.; Matthews, M.; Sharry, J.; Nisbet, A.; Doherty, G. Personal investigator: A therapeutic 3D game for adolecscent psychotherapy. Interact. Technol. Smart Educ. 2007, 2, 73–88. [Google Scholar]
- Klingberg, T.; Fernell, E.; Olesen, P.J.; Johnson, M.; Gustafsson, P.; Dahlström, K.; Gillberg, C.G.; Forssberg, H.; Westerberg, H. Computerized training of working memory in children with ADHD—A randomized, controlled trial. J. Am. Acad. Child Adolesc. Psychiatry 2005, 44, 177–186. [Google Scholar]
- Siglin, J.A.; Logic, U. Play Attention-focusing on success. Intervention School Clinic 2000, 36, 122–124. [Google Scholar] [CrossRef]
- Abikoff, H.; Gallagher, R.; Wells, K.C.; Murray, D.W.; Huang, L.; Lu, F.; Petkova, E. Remediating organizational functioning in children with ADHD: Immediate and long-term effects from a randomized controlled trial. J. Consult. Clin. Psychol. 2013, 81, 113–128. [Google Scholar] [CrossRef]
- Langberg, J.M.; Becker, S.P.; Epstein, J.N.; Vaughn, A.J.; Girio-Herrera, E. Predictors of response and mechanisms of change in an organizational skills intervention for students with ADHD. J. Child Fam. Stud. 2013, 22. [Google Scholar] [CrossRef]
- Pfiffner, L.J.; Villodas, M.; Kaiser, N.; Rooney, M.; McBurnett, K. Educational outcomes of a collaborative school-home behavioral intervention for ADHD. Sch. Psychol. Q. 2013, 28, 25–36. [Google Scholar] [CrossRef]
- Rolands, L.; Sawilowsky, S.; Hoffman, S.F.; Parker, D.R. Self-control in postsecondary settings: Students’ perceptions of ADHD college coaching. J. Atten. Disord. 2011, 17, 215–232. [Google Scholar]
- Field, S.; Parker, D.R.; Sawilowsky, S.; Rolands, L. Assessing the impact of ADHD coaching services on university students learning skills, self-regulation, and well-being. J. Postsecond. Educ. Disabil. 2013, 26, 67–81. [Google Scholar]
- Hart, H.; Radua, J.; Mataix-Cols, D.; Rubia, K. Meta-analysis of fMRI studies of timing in attention-deficit hyperactivity disorder (ADHD). Neurosci. Biobehav. Rev. 2012, 36, 2248–2256. [Google Scholar] [CrossRef]
- Bioulac, S.; Philip, P.; Lallemand, S.; Fabrigoule, C.; Rizzo, A.; Bouvard, M.P. Impact of time on task on ADHD patient’s performances in a virtual classroom. Eur. J. Paediatr. Neurol. 2012, 16, 514–521. [Google Scholar] [CrossRef]
- Langberg, J.M.; Epstein, J.N.; Becker, S.P.; Girio-Herrera, E.; Vaughn, A.J. Evaluation of the homework, organization, and planning skills (HOPS) intervention for middle school students with attention deficit hyperactivity disorder as implemented by school mental health providers. Sch. Psych. Rev. 2012, 41, 342–364. [Google Scholar]
- Gureasko-Moore, S.; Dupaul, G.J.; White, G.P. The effects of self-management in general education classrooms on the organizational skills of adolescents with ADHD. Behav. Modif. 2006, 30, 159–183. [Google Scholar] [CrossRef]
- Prior, H.; Walg, M.; Oepen, J. Adjustment of time perception in the range of seconds and milliseconds: The nature of time-processing alterations in children with ADHD. J. Atten. Disord. 2012. [Google Scholar] [CrossRef]
- Carelli, M.G.; Wiberg, B. Time out of mind: Temporal perspective in adults with ADHD. J. Atten. Disord. 2012, 16, 460–466. [Google Scholar] [CrossRef]
- Abikoff, H.; Gallagher, R.; Ma, J. Measuring and treating organizational, time management, and planning deficits in children with ADHD. J. Child Adolesc. Psychopharmacol. 2003, 13, 422–423. [Google Scholar]
- Django. Available online: https://www.djangoproject.com/ (accessed on 19 July 2013).
- Python. Available online: http://www.python.org/ (accessed on 19 July 2013).
- MySQL. Available online: http://www.mysql.com/ (accessed on 19 July 2013).
- JQuery. Available online: http://jquery.com/ (accessed on 27 August 2013).
- Touch Punch. Available online: http://touchpunch.furf.com/ (accessed on 27 August 2013).
- Macan, T.H.; Shahani, C.; Dipboye, R.L.; Phillips, A.P. College students’ time management: Correlations with academic performance and stress. J. Educ. Psychol. 1990, 82, 760–768. [Google Scholar] [CrossRef]
- Macan, T.H. Time management: Test of a process model. J. Appl. Psychol. 1994, 79, 381–391. [Google Scholar] [CrossRef]
- Macan, T.H. Time-management training: Effects on time behaviors, attitudes, and job performance. J. Psychol. 1996, 130, 229–236. [Google Scholar] [CrossRef]
- García-Ros, R.; Pérez-González, F. Spanish version of the time management behavior questionnaire for university students. Span. J. Psychol. 2012, 15, 1485–1494. [Google Scholar] [CrossRef]
- Aponte, E.D.; Pujol, L. Manejo del tiempo académico en jóvenes que inician estudios en la Universidad Simón Bolívar. Rev. Latinoamer. De Cienc. Sociales Niñez y Juventud 2013, 11, 93–108. [Google Scholar]
- Google Forms. Available online: http://www.google.com/drive (accessed on 19 July 2013).
- Brooke, J. SUS—A quick and dirty usability scale. Usability Eval. Ind. 1996, 189, 189–194. [Google Scholar]
- IBM SPSS Software. Available online: http://www-01.ibm.com/software/analytics/spss/ (accessed on 19 July 2013).
- Quinlan, J.R. Induction of decision trees. Mach. Learn. 1986, 1, 81–106. [Google Scholar]
- Harrington, P. Machine Learning in Action; Manning Publications Co.: Shelter Island, NY, USA, 2012. [Google Scholar]
- Shannon, C.E. The mathematical theory of communication. 1963. M. D. Comput. 1948, 14, 306–317. [Google Scholar]
- Balance Online Tool. Available online: http://deustotechlife.deusto.es/balanza/activity/ (accessed on 28 August 2013).
- Wu, W.-H.; Wu, Y.-C.J.; Chen, C.-Y.; Kao, H.-Y.; Lin, C.-H.; Huang, S.-H. Review of trends from mobile learning studies: A meta-analysis. Comput. Educ. 2012, 59, 817–827. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Frutos-Pascual, M.; Zapirain, B.G.; Zorrilla, A.M. Adaptive Tele-Therapies Based on Serious Games for Health for People with Time-Management and Organisational Problems: Preliminary Results. Int. J. Environ. Res. Public Health 2014, 11, 749-772. https://doi.org/10.3390/ijerph110100749
Frutos-Pascual M, Zapirain BG, Zorrilla AM. Adaptive Tele-Therapies Based on Serious Games for Health for People with Time-Management and Organisational Problems: Preliminary Results. International Journal of Environmental Research and Public Health. 2014; 11(1):749-772. https://doi.org/10.3390/ijerph110100749
Chicago/Turabian StyleFrutos-Pascual, Maite, Begoña García Zapirain, and Amaia Méndez Zorrilla. 2014. "Adaptive Tele-Therapies Based on Serious Games for Health for People with Time-Management and Organisational Problems: Preliminary Results" International Journal of Environmental Research and Public Health 11, no. 1: 749-772. https://doi.org/10.3390/ijerph110100749
APA StyleFrutos-Pascual, M., Zapirain, B. G., & Zorrilla, A. M. (2014). Adaptive Tele-Therapies Based on Serious Games for Health for People with Time-Management and Organisational Problems: Preliminary Results. International Journal of Environmental Research and Public Health, 11(1), 749-772. https://doi.org/10.3390/ijerph110100749