Comparison of UTCI with Other Thermal Indices in the Assessment of Heat and Cold Effects on Cardiovascular Mortality in the Czech Republic

Abstract
:1. Introduction
2. Data and Methods

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ICD-10 code | Abbreviation | Diagnosis |
|---|---|---|
| I00–I99 | CVD | cardiovascular disease |
| I20–I25 | IHD | ischemic heart disease |
| I60–I69 | CD | cerebrovascular disease |
| I21–I22 | MI | myocardial infarction (acute and subsequent) |
| I25 | CIHD | chronic ischemic heart disease |
| I70 | ASVD | atherosclerosis – atherosclerotic vascular disease |


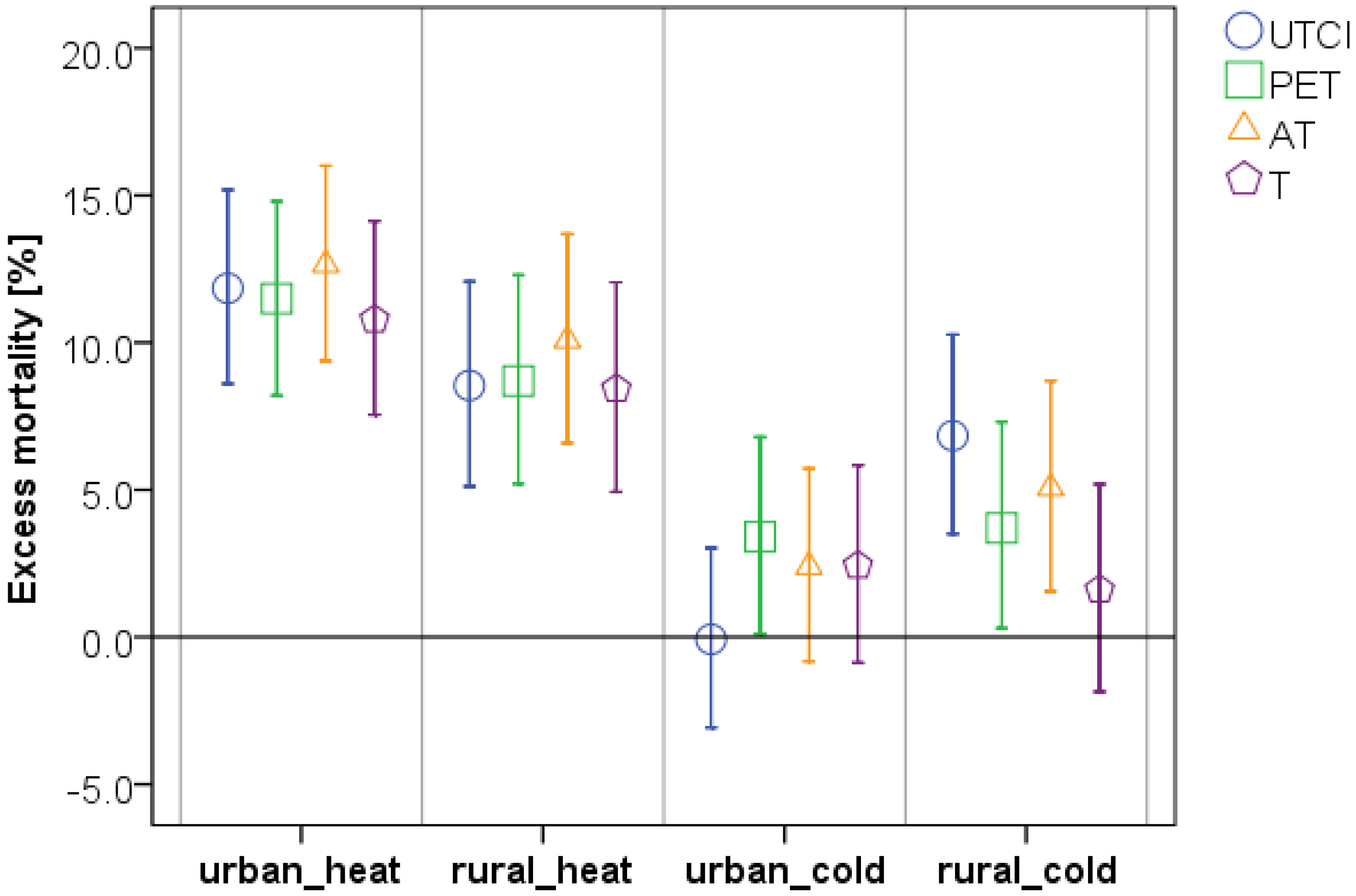
3. Results

| Urban Region (Prague) | ||||
| Thermal index/Diagnosis | UTCI (≥22.0 °C) | PET (≥19.2 °C) | AT (≥22.0 °C) | T (≥22.5 °C) |
| CVD | 11.8 (8.6; 15.2) | 11.5 (8.2; 14.8) | 12.6 (9.4; 16.0) | 10.8 (7.5; 14.1) |
| IHD | 7.8 (2.9; 13.0) | 8.0 (3.0; 13.2) | 8.7 (3.7; 13.9) | 7.0 (2.1; 12.2) |
| CD | 11.6 (5.4; 18.2) | 9.5 (3.3; 16.1) | 13.0 (6.7; 19.7) | 10.0 (3.8; 16.6) |
| MI | −0.8 (−8.8; 7.9) | 1.5 (−6.6; 10.4) | −0.2 (−8.2; 8.5) | −1.6 (−9.6; 7.1) |
| CIHD | 12.0 (5.8; 18.6) | 10.9 (4.7; 17.5) | 13.0 (6.8; 19.7) | 10.9 (4.7; 17.4) |
| ASVD | 17.6 (10.0; 25.7) | 18.5 (10.9; 26.6) | 18.5 (10.9; 26.5) | 19.4 (11.6; 27.7) |
| Rural Region (Southern Bohemia) | ||||
| Themal index/Diagnosis | UTCI (≥21.9 °C) | PET (≥18.0 °C) | AT (≥21.7 °C) | T (≥22.0 °C) |
| CVD | 8.5 (5.1; 12.1) | 8.7 (5.2; 12.3) | 10.1 (6.6; 13.7) | 8.4 (4.9; 12.0) |
| IHD | 6.9 (2.0; 12.0) | 7.3 (2.3; 12.5) | 7.9 (2.9; 13.2) | 7.2 (2.2; 12.5) |
| CD | 11.4 (5.0; 18.3) | 10.3 (3.8; 17.2) | 13.5 (6.9; 20.6) | 7.9 (1.3; 14.8) |
| MI | 1.6 (−5.6; 9.4) | 1.2 (−6.1; 9.1) | 2.0 (−5.4; 9.9) | 3.6 (−3.9; 11.8) |
| CIHD | 11.4 (4.8; 18.4) | 11.9 (5.2; 19.0) | 12.4 (5.6; 19.5) | 10.2 (3.5; 17.4) |
| ASVD | 9.8 (0.4; 20.2) | 10.9 (1.4; 21.3) | 11.2 (1.5; 21.8) | 14.9 (5.0; 25.6) |
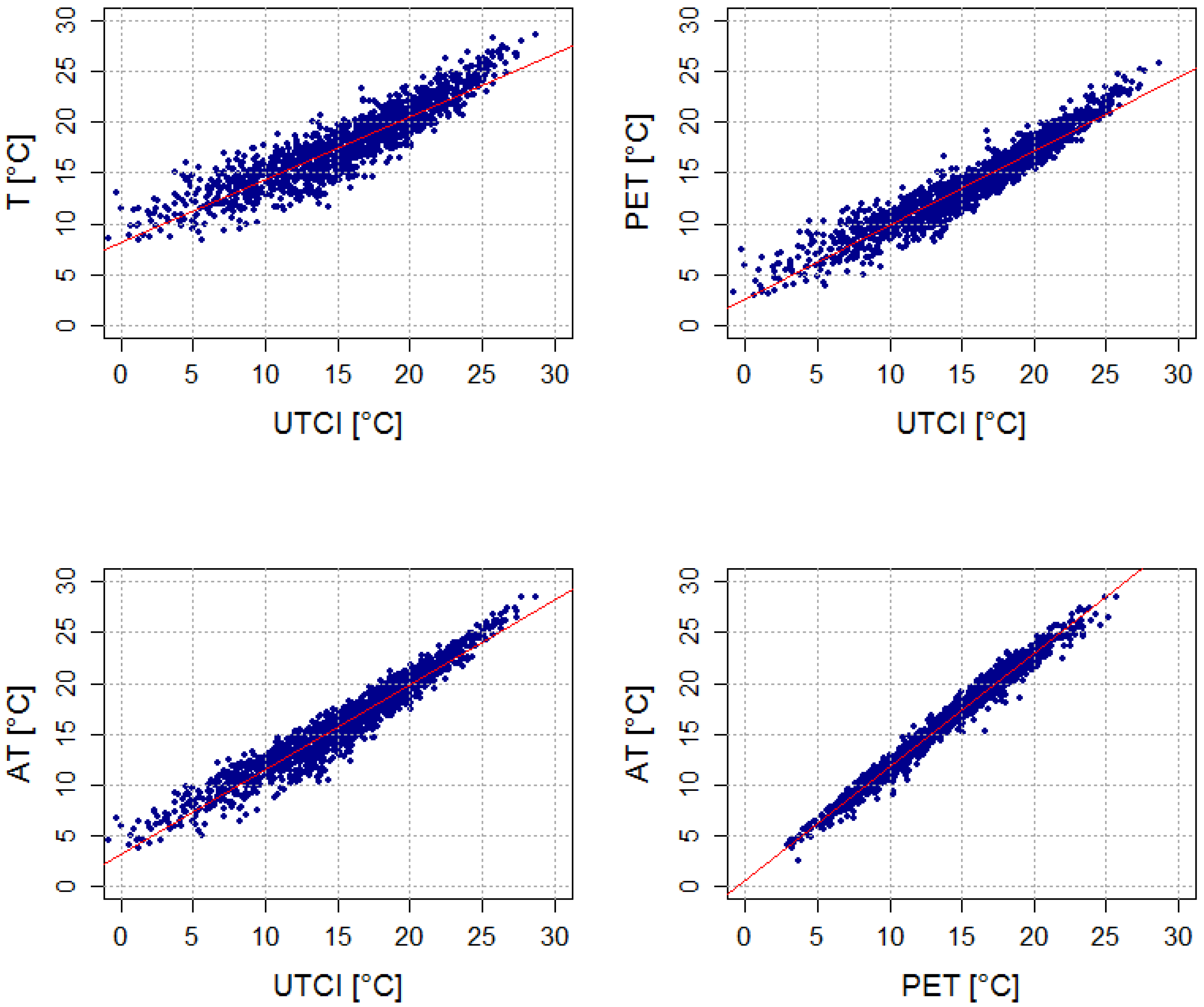
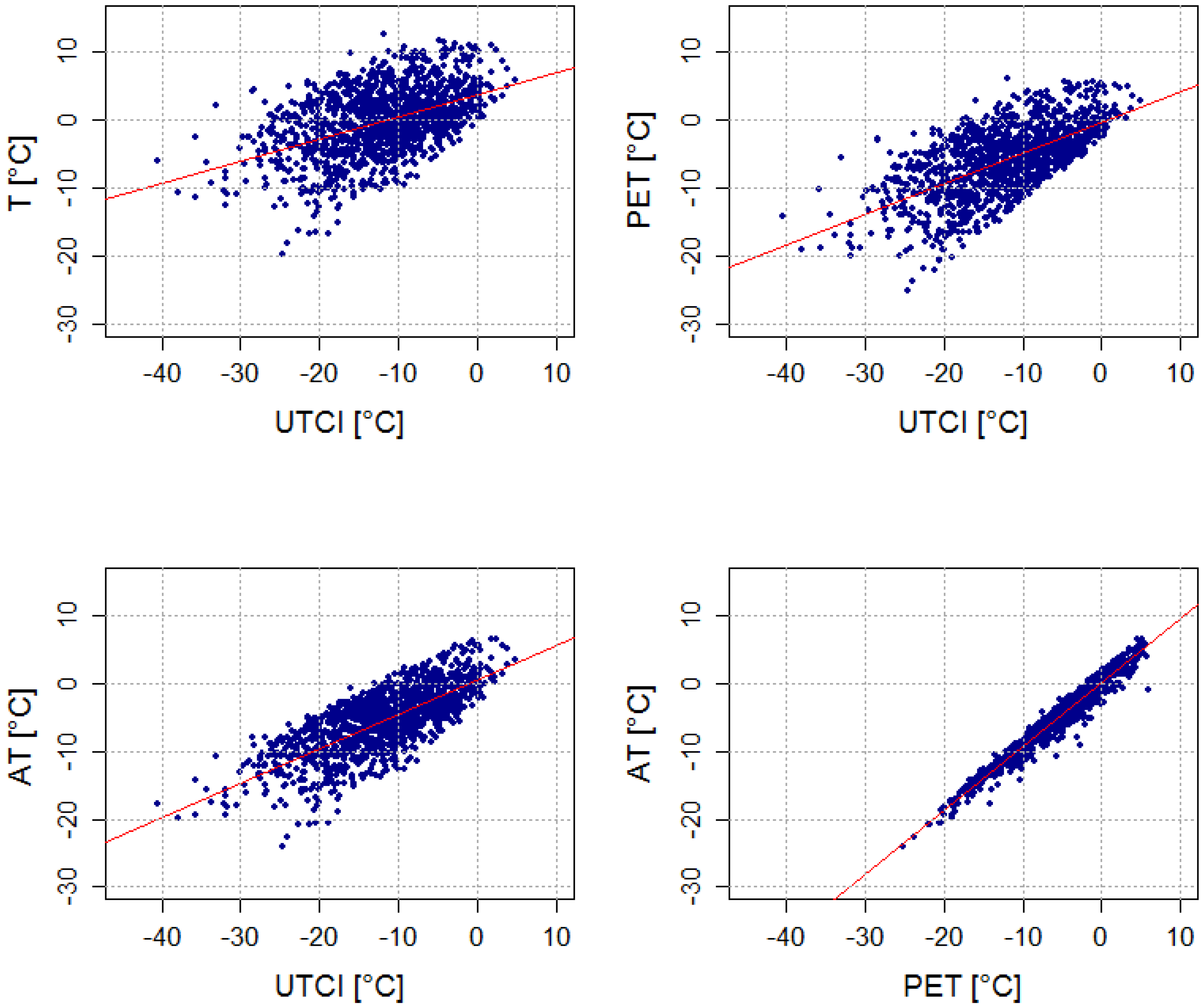
| Thermal Indices Compared | Urban JJA R2 (%) | Urban DJF R2 (%) | Rural JJA R2 (%) | Rural DJF R2 (%) | ||||
|---|---|---|---|---|---|---|---|---|
| T~UTCI | 0.83 | 73 | 0.23 | 31 | 0.86 | 77 | 0.52 | 45 |
| PET~UTCI | 0.91 | 82 | 0.41 | 39 | 0.92 | 82 | 0.68 | 59 |
| AT~UTCI | 0.93 | 83 | 0.56 | 45 | 0.94 | 84 | 0.75 | 62 |
| T~AT | 0.94 | 79 | 0.88 | 86 | 0.95 | 84 | 0.94 | 81 |
| AT~PET | 0.98 | 82 | 0.95 | 91 | 0.98 | 87 | 0.98 | 91 |
| T~PET | 0.96 | 84 | 0.95 | 88 | 0.95 | 87 | 0.96 | 80 |

| Urban Region | UTCI (°C) | PET (°C) | AT (°C) | T (°C) | Tmrt (°C) | v10 (m∙s−1) | RH (%) | C (octas) |
| UTCI | 23.9 | 20.8 | 23.7 | 23.8 | 29.7 | 2.3 | 59 | 3.7 |
| PET | 23.7 | 21.0 | 23.7 | 24.0 | 29.8 | 2.6 | 58 | 3.9 |
| AT | 23.8 | 20.8 | 23.8 | 24.0 | 29.6 | 2.5 | 60 | 3.5 |
| T | 23.4 | 20.8 | 23.5 | 24.2 | 29.8 | 2.9 | 56 | 3.3 |
| Rural Region | UTCI (°C) | PET(°C) | AT (°C) | T (°C) | Tmrt (°C) | v10 (m∙s−1) | RH (%) | C (octas) |
| UTCI | 23.4 | 19.3 | 23.2 | 23.2 | 28.8 | 2.2 | 62 | 2.6 |
| PET | 23.2 | 19.4 | 23.2 | 23.3 | 28.7 | 2.4 | 61 | 2.6 |
| AT | 23.3 | 19.4 | 23.3 | 23.3 | 28.6 | 2.4 | 63 | 2.5 |
| T | 23.1 | 19.3 | 23.2 | 23.5 | 28.9 | 2.6 | 60 | 2.4 |
| Urban Region (Prague) | ||||
| Thermal index/Diagnosis | UTCI (≤−21.5 °C) | PET (≤−12.9 °C) | AT (≤−12.1 °C) | T (≤−6.5 °C) |
| CVD | −0.1 (−3.1; 3.0) | 3.4 (0.1; 6.8) | 2.4 (−0.8; 5.7) | 2.4 (−0.9; 5.8) |
| IHD | −0.6 (−5.4; 4.3) | 3.9 (−1.4; 9.4) | 3.8 (−1.3; 9.3) | 2.1 (−3.1; 7.6) |
| CD | 0.9 (−5.0; 7.2) | 4.6 (−2.0; 11.5) | 4.1 (−2.3; 11.0) | 4.6 (−2.0; 11.6) |
| MI | 4.5 (−3.6; 13.3) | 10.6 (1.3; 20.7) | 10.5 (1.4; 20.4) | 7.1 (−2.1; 17.1) |
| CIHD | −3.1 (−8.9; 3.0) | 0.6 (−5.7; 7.3) | 0.5 (−5.8; 7.1) | −0.3 (−6.7; 6.5) |
| ASVD | 1.7 (−4.7; 8.5) | 3.6 (−3.4; 11.1) | 1.4 (−5.2; 8.5) | 2.8 (−4.0; 10.1) |
| Rural Region (Southern Bohemia) | ||||
| Thermal index/Diagnosis | UTCI (≤−19.9 °C) | PET (≤−13.5 °C) | AT (≤−12.4 °C) | T (≤−7.3 °C) |
| CVD | 6.8 (3.5; 10.3) | 3.7 (0.3; 7.3) | 5.1 (1.6; 8.7) | 1.6 (−1.9; 5.2) |
| IHD | 8.3 (3.4; 13.5) | 3.3 (−1.8; 8.5) | 5.7 (0.6; 11.1) | 2.0 (−3.1; 7.4) |
| CD | 10.7 (4.4; 17.3) | 7.0 (0.5; 14.0) | 8.0 (1.4; 15.1) | 2.7 (−3.8; 9.5) |
| MI | 15.2 (7.4; 23.6) | 12.6 (4.4; 21.4) | 17.2 (8.8; 26.2) | 10.6 (2.4; 19.5) |
| CIHD | 2.9 (−3.4; 9.6) | −3.5 (−9.8; 3.2) | −2.7 (−9.1; 4.2) | −4.3 (−10.7; 2.6) |
| ASVD | −1.5 (−10.3; 8.2) | −1.4 (−10.7; 8.8) | −1.7 (−11.1; 8.7) | 1.5 (−7.9; 11.9) |

4. Discussion
| Urban Region | UTCI (°C) | PET (°C) | AT (°C) | T (°C) | Tmrt (°C) | v10 (m∙s−1) | RH (%) | C (octas) |
| UTCI | −25.5 | −11.5 | −12.2 | −4.4 | −9.0 | 7.2 | 81 | 5.7 |
| PET | −20.9 | −15.7 | −14.7 | −9.3 | −16.3 | 3.2 | 83 | 4.0 |
| AT | −21.4 | −15.6 | −14.8 | −9.3 | −16.0 | 3.4 | 83 | 4.3 |
| T | −19.3 | −15.5 | −14.6 | −9.6 | −16.3 | 2.6 | 84 | 4.3 |
| Rural Region | UTCI (°C) | PET (°C) | AT (°C) | T (°C) | Tmrt (°C) | v10 (m∙s−1) | RH (%) | C (octas) |
| UTCI | −24.4 | −14.1 | −13.6 | −6.8 | −12.1 | 5.5 | 82 | 5.5 |
| PET | −21.8 | −16.1 | −15.0 | −9.4 | −15.9 | 3.5 | 82 | 4.2 |
| AT | −22.2 | −16.0 | −15.1 | −9.4 | −15.7 | 3.7 | 82 | 4.4 |
| T | −19.6 | −15.8 | −14.7 | −9.6 | −16.3 | 2.8 | 82 | 3.9 |
5. Conclusions
Acknowledgements
Author Contributions
Conflicts of Interest
References
- Cheng, X.; Su, H. Effects of climatic temperature stress on cardiovascular diseases. Eur. J. Intern. Med. 2010, 21, 164–167. [Google Scholar] [CrossRef]
- Basu, R. High ambient temperature and mortality: A review of epidemiologic studies from 2001 to 2008. Environ. Health 2009, 8. [Google Scholar] [CrossRef]
- McGregor, G.R. Human biometeorology. Prog. Phys. Geogr. 2011, 36, 93–109. [Google Scholar] [CrossRef]
- Jendritzky, G.; de Dear, R.; Havenith, G. UTCI—Why another thermal index? Int. J. Biometeorol. 2012, 56, 421–428. [Google Scholar] [CrossRef] [Green Version]
- Kántor, N.; Unger, J. The most problematic variable in the course of human-biometeorological comfort assessment—The mean radiant temperature. Cent. Eur. J. Geosci. 2011, 3, 90–100. [Google Scholar] [CrossRef] [Green Version]
- Mayer, H.; Höppe, P. Thermal comfort of man in different urban environments. Theor. Appl. Climatol. 1987, 38, 43–49. [Google Scholar] [CrossRef]
- Höppe, P. The physiological equivalent temperature—A universal index for the biometeorological assessment of the thermal environment. Int. J. Biometeorol. 1999, 43, 71–75. [Google Scholar] [CrossRef]
- Matzarakis, A; Mayer, H.; Iziomon, M.G. Applications of a universal thermal index: Physiological equivalent temperature. Int. J. Biometeorol. 1999, 43, 76–84. [Google Scholar] [CrossRef]
- Jendritzky, G.; Staiger, H.; Bucher, K.; Graetz, A.; Laschewski, G. The Perceived Temperature: The Method of the Deutscher Wetterdienst for the Assessment of Cold Stress and Heat Load for the Human Body. In Proceedings of Internet Workshop on Windchill, Environment Canada, Fredericton, New Brunswick, Canada, 3–7 April 2000.
- Staiger, H.; Laschewski, G.; Grätz, A. The perceived temperature—A versatile index for the assessment of the human thermal environment. Part A: Scientific basics. Int. J. Biometeorol. 2012, 56, 165–76. [Google Scholar] [CrossRef]
- Laschewski, G.; Jendritzky, G. Effects of the thermal environment on human health: An investigation of 30 years of daily mortality data from SW Germany. Clim. Res. 2002, 21, 91–103. [Google Scholar] [CrossRef]
- Matzarakis, A.; Muthers, S.; Koch, E. Human biometeorological evaluation of heat-related mortality in Vienna. Theor. Appl. Climatol. 2010, 105, 1–10. [Google Scholar] [CrossRef]
- Burkart, K.; Schneider, A.; Breitner, S.; Khan, M.H.; Krämer, A.; Endlicher, W. The effect of atmospheric thermal conditions and urban thermal pollution on all-cause and cardiovascular mortality in Bangladesh. Environ. Pollut. 2011, 159, 2035–2043. [Google Scholar] [CrossRef]
- Gabriel, K.M.A.; Endlicher, W.R. Urban and rural mortality rates during heat waves in Berlin and Brandenburg, Germany. Environ. Pollut. 2011, 159, 2044–2050. [Google Scholar] [CrossRef]
- Kim, Y.-M.; Kim, S.; Cheong, H.-K.; Kim, E.-H. Comparison of temperature indexes for the impact assessment of heat stress on heat-related mortality. Environ. Health Toxicol. 2011, 26. [Google Scholar] [CrossRef]
- Nastos, P.T.; Matzarakis, A. The effect of air temperature and human thermal indices on mortality in Athens, Greece. Theor. Appl. Climatol. 2011, 108, 591–599. [Google Scholar] [CrossRef]
- Fiala, D.; Havenith, G.; Bröde, P.; Kampmann, B.; Jendritzky, G. UTCI-Fiala multi-node model of human heat transfer and temperature regulation. Int. J. Biometeorol. 2012, 56, 429–441. [Google Scholar] [CrossRef] [Green Version]
- UTCI—Universal Thermal Climate Index. Available online: http://www.utci.org/ (accessed on 10 June 2013).
- Havenith, G.; Fiala, D.; Błazejczyk, K.; Richards, M.; Bröde, P.; Holmér, I.; Rintamaki, H.; Benshabat, Y.; Jendritzky, G. The UTCI-clothing model. Int. J. Biometeorol 2012, 56, 461–470. [Google Scholar] [CrossRef] [Green Version]
- Błażejczyk, K.; Epstein, Y.; Jendritzky, G.; Staiger, H.; Tinz, B. Comparison of UTCI to selected thermal indices. Int. J. Biometeorol. 2012, 56, 515–535. [Google Scholar] [CrossRef]
- Urban, A.; Davídkovová, H.; Kyselý, J. Heat- and cold-stress effects on cardiovascular mortality and morbidity among urban and rural populations in the Czech Republic. Int. J. Biometeorol. 2013. [Google Scholar] [CrossRef]
- Spiezia, V. Measuring Regional Economies. Statistics Brief OECD, No. 6, 2003. Available online: http://www.oecd.org/dataoecd/2/15/15918996.pdf (accessed on 14 August 2013).
- Blatecká, K. The Basic Characteristics of Czech Rural Areas. (in Czech). Available online: http://is.muni.cz/th/137827/esf_m/Diplomova_prace.pdf (accessed on 14 August 2013).
- CZSO—Czech Statistical Office. Statistical Yearbook 2011. Available online: http://www.czso.cz/csu/2011edicniplan.nsf/publ/0001-11-2010 (accessed on 20 August 2012).
- Whitman, S.; Good, G.; Donoghue, E.R.; Benbow, N. Public health biefs mortality in Chicago attributed to the July 1995 heat wave. Public Health 1997, 87, 1515–1518. [Google Scholar]
- Smoyer, K.E.; Rainham, D.G.; Hewko, J.N. Heat-stress-related mortality in five cities in Southern Ontario: 1980–1996. Int. J. Biometeorol. 2000, 44, 190–197. [Google Scholar] [CrossRef]
- Kynčl, J.; Procházka, B.; Goddard, N.L.; Havlíčková, M.; Částková, J.; Otavová, M.; Kříž, B. A study of excess mortality during influenza epidemics in the Czech Republic, 1982–2000. Eur. J. Epidemiol. 2005, 20, 365–371. [Google Scholar] [CrossRef]
- Kyselý, J.; Pokorná, L.; Kynčl, J.; Kříž, B. Excess cardiovascular mortality associated with cold spells in the Czech Republic. BMC Public Health 2009, 9. [Google Scholar] [CrossRef]
- Matzarakis, A.; Rutz, F.; Mayer, H. Modelling radiation fluxes in simple and complex environments—Application of the RayMan model. Int. J. Biometeorol. 2007, 51, 323–334. [Google Scholar] [CrossRef]
- Matzarakis, A.; Rutz, F.; Mayer, H. Modelling radiation fluxes in simple and complex environments—Basics of the RayMan model. Int. J. Biometeorol. 2010, 54, 131–139. [Google Scholar] [CrossRef]
- Bañuelos-Ruedas, F.; Camacho, C.Á. Methodologies Used in the Extrapolation of Wind Speed Data at Different Heights and Its Impact in the Wind Energy Resource Assessment in a Region. In Wind Farm—Technical Regulations, Potential Estimation and Siting Assessment; Suvire, G.O., Ed.; InTech: Rijeka, Croatia, 2011. [Google Scholar]
- Bröde, P.; Fiala, D.; Błażejczyk, K.; Holmér, I.; Jendritzky, G.; Kampmann, B.; Tinz, B.; Havenith, G. Deriving the operational procedure for the Universal Thermal Climate Index (UTCI). Int. J. Biometeorol. 2012, 56, 481–94. [Google Scholar] [CrossRef] [Green Version]
- Steadman, R.G. A universal scale of apparent temperature. J. Appl. Meteorol. Climatol. 1984, 23, 1674–1687. [Google Scholar]
- Steadman, R.G. Norms of apparent temperature in Australia. Aust. Meteorol. Mag. 1994, 43, 1–16. [Google Scholar]
- Australian Government, Bureau of Meterology. Thermal Comfort observations. Available online: http://www.bom.gov.au/info/thermal_stress (accessed on 5 November 2013).
- Hajat, S.; Kovats, R.S.; Lachowycz, K. Heat-related and cold-related deaths in England and Wales: Who is at risk? Occup Environ. Med. 2007, 64, 93–100. [Google Scholar]
- Medina-Ramón, M.; Schwartz, J. Temperature, temperature extremes, and mortality: A study of acclimatization and effect modification in 50 United States cities. Occup. Environ. Med. 2007, 827–834. [Google Scholar]
- Gómez-Acebo, I.; Dierssen-Sotos, T.; Llorca, J. Effect of cold temperatures on mortality in Cantabria (Northern Spain): A case-crossover study. Public Health 2010, 124, 398–403. [Google Scholar] [CrossRef]
- Schoenberg, B.S. Calculating confidence intervals for rates and ratios. Neuroepidemiology 1983, 2, 257–265. [Google Scholar] [CrossRef]
- Novák, M. Use of the UTCI in the Czech Republic. Geogr. Pol. 2013, 86, 21–28. [Google Scholar] [CrossRef]
- Spreitzhofer, G. Synoptic classification of severe snowstorms over Austria. Met. Z. 1999, 8, 3–15. [Google Scholar]
- Kalkstein, S.; Davis, R. Weather and human mortality: An evaluation of demographic and interregional responses in the united states. Ann. Assn. Amer Geogr 1989, 79, 44–64. [Google Scholar] [CrossRef]
- Baker-Blocker, A. Winter weather and cardiovascular mortality in Minneapolis-St. Paul. Amer. J. Public Health 1982, 72, 261–265. [Google Scholar] [CrossRef]
- Southern, D.A.; Knudtson, M.L.; Ghali, W.A. Myocardial infarction on snow days: Incidence, procedure use and outcomes. Can. J. Cardiol. 2006, 22, 59–61. [Google Scholar] [CrossRef]
- Vaneckova, P.; Neville, G.; Tippett, V.; Aitken, P.; FitzGerald, G.; Tong, S. Do biometeorological indices improve modeling outcomes of heat-related mortality? J. Appl. Meteorol. Climatol. 2011, 50, 1165–1176. [Google Scholar] [CrossRef]
- Ye, X.; Wolff, R.; Yu, W.; Vaneckova, P.; Pan, X.; Tong, S. Ambient temperature and morbidity: a review of epidemiological evidence. Environ. Health Perspect. 2012, 120, 19–28. [Google Scholar] [CrossRef]
- Gosling, S.N.; Lowe, J.A.; McGregor, G.R.; Pelling, M.; Malamud, B.D. Associations between elevated atmospheric temperature and human mortality: A critical review of the literature. Climate Change 2008, 92, 299–341. [Google Scholar]
- Markandya, A.; Chiabai, A. Valuing climate change impacts on human health: Empirical evidence from the literature. Int. J. Environ. Res. Public Health 2009, 6, 759–786. [Google Scholar] [CrossRef]
- Christidis, N.; Donaldson, G.C.; Stott, P.A. Causes for the recent changes in cold- and heat-related mortality in England and Wales. Climate Change 2010, 102, 539–553. [Google Scholar] [CrossRef]
- Mercer, J.B. Cold, an underrated risk factor for health. Environ. Res. 2002, 92, 8–13. [Google Scholar] [CrossRef]
- Kenney, W.L.; Munce, T.A. Invited review: Aging and human temperature regulation. J. Appl. Physiol. 2003, 95, 2598–2603. [Google Scholar]
- Weihs, P.; Staiger, H.; Tinz, B.; Batchvarova, E.; Rieder, H.; Vuilleumier, L.; Maturilli, M.; Jendritzky, G. The uncertainty of UTCI due to uncertainties in the determination of radiation fluxes derived from measured and observed meteorological data. Int. J. Biometeorol. 2012, 56, 537–555. [Google Scholar] [CrossRef]
- Iñiguez, C.; Ballester, F.; Ferrandiz, J.; Pérez-Hoyos, S.; Sáez, M.; López, A. Relation between temperature and mortality in thirteen Spanish cities. Int. J. Environ. Res. Public Health 2010, 7, 3196–3210. [Google Scholar] [CrossRef]
- Hattis, D.; Ogneva-Himmelberger, Y.; Ratick, S. The spatial variability of heat-related mortality in Massachusetts. Appl. Geogr. 2012, 33, 45–52. [Google Scholar] [CrossRef]
- Burkart, K.; Khan, M.H.; Krämer, A.; Breitner, S.; Schneider, A.; Endlicher, W.R. Seasonal variations of all-cause and cause-specific mortality by age, gender, and socioeconomic condition in urban and rural areas of Bangladesh. Int. J. Equity Health 2011, 10. [Google Scholar] [CrossRef]
- Carder, M.; McNamee, R.; Beverland, I.; Elton, R.; Cohen, G.R.; Boyd, J.; Agius, R.M. The lagged effect of cold temperature and wind chill on cardiorespiratory mortality in Scotland. Occup. Environ. Med. 2005, 62, 702–710. [Google Scholar] [CrossRef]
- Wichmann, J.; Andersen, Z.J.; Ketzel, M.; Ellermann, T.; Loft, S. Apparent temperature and cause-specific mortality in Copenhagen, Denmark: A case-crossover analysis. Int. J. Environ. Res. Public Health 2011, 8, 3712–3727. [Google Scholar] [CrossRef]
- Yu, W.; Mengersen, K.; Wang, X.; Ye, X.; Guo, Y.; Pan, X.; Tong, S. Daily average temperature and mortality among the elderly: A meta-analysis and systematic review of epidemiological evidence. Int. J. Biometeorol. 2012, 56, 569–581. [Google Scholar] [CrossRef] [Green Version]
- Shitzer, A.; Tikuisis, P. Advances, shortcomings, and recommendations for wind chill estimation. Int. J. Biometeorol. 2012, 56, 495–503. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Urban, A.; Kyselý, J. Comparison of UTCI with Other Thermal Indices in the Assessment of Heat and Cold Effects on Cardiovascular Mortality in the Czech Republic. Int. J. Environ. Res. Public Health 2014, 11, 952-967. https://doi.org/10.3390/ijerph110100952
Urban A, Kyselý J. Comparison of UTCI with Other Thermal Indices in the Assessment of Heat and Cold Effects on Cardiovascular Mortality in the Czech Republic. International Journal of Environmental Research and Public Health. 2014; 11(1):952-967. https://doi.org/10.3390/ijerph110100952
Chicago/Turabian StyleUrban, Aleš, and Jan Kyselý. 2014. "Comparison of UTCI with Other Thermal Indices in the Assessment of Heat and Cold Effects on Cardiovascular Mortality in the Czech Republic" International Journal of Environmental Research and Public Health 11, no. 1: 952-967. https://doi.org/10.3390/ijerph110100952
APA StyleUrban, A., & Kyselý, J. (2014). Comparison of UTCI with Other Thermal Indices in the Assessment of Heat and Cold Effects on Cardiovascular Mortality in the Czech Republic. International Journal of Environmental Research and Public Health, 11(1), 952-967. https://doi.org/10.3390/ijerph110100952