Horizon 2020 Priorities in Clinical Mental Health Research: Results of a Consensus-Based ROAMER Expert Survey


Abstract
:1. Introduction
2. Methods
2.1. The Delphi Approach
2.2. Second Stage Participants and Procedure
2.3. Second Stage Questionnaire
Part I: Demographic Variables
Part II and III: Challenges Built on Pre-Defined Gaps and Open-Ended Questions from the First Stage

{kind=link}
{kind=link}
| Statements | N | Answered “I Don’t Know” N | Median | IQD |
|---|---|---|---|---|
| PART II | ||||
| Challenge 1: To develop new, safe and effective treatment interventions (pharmacological, brain related, psychotherapeutic, systemic, psychosocial, eHealth/mHealth approaches and virtual reality/gamification … or a combination of these) is a challenge in the field of clinical research on mental health | 86 | 0 | 7 | 1 |
| PART II | ||||
| An action to target Challenge 1 is: To increase research on new intervention approaches in order to gain more insight into their working mechanisms and to successfully develop effective new interventions. This research can/should specifically focus on:
| 86 | 2 | 6 | 1 |
| Challenge 2: To understand the mechanisms of diseases is a challenge in the field of clinical research on mental health | 86 | 0 | 7 | 1 |
| An action to target Challenge 2 is: To conduct research in order to reach a clinically relevant understanding of different mechanisms (e.g., psychological mechanisms, biological mechanisms, brain mechanisms, molecular mechanisms and environmental interactions) that may underlie diseases | 86 | 0 | 7 | 2 |
| An action to target Challenge 2 is: To conduct longitudinal clinical cohort studies with nested randomized controlled trials | 86 | 0 | 6 | 2 |
| Challenge 3: To evaluate treatment effects is a challenge in the field of clinical research on mental health | 86 | 0 | 6 | 2 |
| An action to target Challenge 3 is: To conduct research on different approaches to evaluate treatment effects, specifically more research is needed on:
| 86 | 0 | 6 | 2 |
| An action to target Challenge 3 is: To increase the involvement of health-care staff, among others in order to stop non-effective treatments | 86 | 0 | 6 | 2 |
| Challenge 4: To perform proof of concept clinical trials for innovative treatments is a challenge in the field of clinical research on mental health | 86 | 4 | 6 | 2 |
| An action to target Challenge 4 is: To identify or develop standard definitions and guidelines to increase the understanding of the term ‘proof of concept’ | 86 | 3 | 5 | 1 |
| Challenge 5: To gain insight into the role of comorbidity between mental disorders and somatic conditions for diagnosis, treatment decisions, and treatment and patient-related outcomes is a challenge in the field of clinical research on mental health | 86 | 0 | 6 | 2 |
| An action to target Challenge 5 is: To develop research in order to better understand mechanisms of comorbidity and how to investigate and treat comorbidity (including diagnostic strategies) | 86 | 0 | 6 | 2 |
| An action to target Challenge 5 is: To increase research on intervention studies that target comorbidity | 86 | 0 | 6 | 2 |
| Challenge 6: To improve diagnostic strategies and the stratification of diseases is a challenge in the field of clinical research on mental health | 86 | 0 | 6 | 2 |
| An action to target Challenge 6 is: To define and validate stages for different diseases | 86 | 0 | 6 | 3 |
| An action to target Challenge 6 is: To develop and validate new diagnostic approaches and to foster standardization of diagnostic tools | 86 | 0 | 6 | 2 |
| Challenge 7: To improve interventions in terms of return/to/work, presenteeism-absenteeism is a challenge in the field of clinical research on mental health | 86 | 2 | 6 | 2 |
| An action to target Challenge 7 is: To target work disability and return-to-work as the main outcomes | 86 | 2 | 5.5 | 3 |
| An action to target Challenge 7 is: To identify or develop standard measures for return-to-work and related outcomes | 86 | 2 | 6 | 3 |
| Challenge 8: To determine the cost/effectiveness of interventions to increase rates of return to work, presenteeism, decreased rates of absenteeism is a challenge in the field of clinical research on mental health | 86 | 3 | 6 | 2 |
| An action to target Challenge 8 is: To foster the standard inclusion of cost-effectiveness assessments in intervention studies | 86 | 2 | 5 | 1 |
| Challenge 9: To overcome methodological gaps regarding the inclusion of patient preferences by study designs is a challenge in the field of clinical research on mental health | 86 | 3 | 5 | 2 |
| An action to target Challenge 9 is: To develop or identify standard measures of preferences (thus: to reach more consistency in the measures of preference used) | 86 | 6 | 5 | 2 |
| An action to target Challenge 9 is: To develop designs for preference studies | 86 | 6 | 5 | 2 |
| Challenge 10: To overcome methodological gaps regarding psychotherapeutic interventions studies (a specific gap is for instance that placebo studies are missing) is a challenge in the field of clinical research on mental health | 86 | 1 | 6 | 2 |
| An action to target Challenge 10 is: To explore what is the most likely accepted placebo in psychotherapeutic studies | 86 | 2 | 5.5 | 2.75 |
| An action to target Challenge 10 is: To increase research on the process and outcomes of different psychotherapies, especially by conducting more RCT’s in this field | 86 | 2 | 6 | 2.75 |
| Challenge 11: To overcome methodological gaps regarding psychopharmacological intervention studies (one of the specific gaps is that most pharmacological studies are funded by the pharmaceutical industry and that the pharmaceutical industry is withdrawing from psycho-pharmacological research altogether: leaving a gap in research) is a challenge in the field of clinical research on mental health | 86 | 0 | 6 | 2 |
| An action to target Challenge 11 is: To work more closely with industry in a precompetitive environment to ensure high quality trial design, on an independent basis | 86 | 3 | 6 | 2 |
| A general action for targeting all gaps: Increasing funding/financial investment in order to conduct more research is a general action that is relevant for most challenges mentioned | 86 | 3 | 7 | 1 |
| A general action for targeting all gaps: To establish (European) research networks to coordinate and facilitate clinical research is a general action that is needed in order to reach most of the challenges mentioned | 86 | 0 | 6.5 | 1.25 |
| PART III | ||||
| Challenge 12: To conduct research on prevention approaches is a challenge in the field of clinical research on mental health | 86 | 0 | 6 | 2 |
| Challenge 13: To gain more insight into the best outcomes to use (including the use of alternative outcomes) is a challenge in the field of clinical research on mental health | 86 | 1 | 6 | 1 |
| Challenge 14: To understand intervention processes and mechanisms is a challenge in the field of clinical research on mental health | 86 | 0 | 6 | 2 |
| Challenge 15: To conduct research on how to overcome stigma and social exclusion is a challenge in the field of clinical research on mental health | 86 | 0 | 6 | 2.25 |
| Challenge 16: To foster the delivery of and access to mental healthcare is a challenge in the field of clinical research on mental health | 86 | 1 | 6 | 2 |
| Challenge 17: The translation, integration and dissemination of research findings and treatments is a challenge in the field of clinical research on mental health | 86 | 0 | 6 | 2 |
| Challenge 18: Conducting research is a challenge in the field of clinical research on mental health | 86 | 2 | 6 | 2 |
| Challenge 19: Facilitating research is a challenge in the field of clinical research on mental health | 86 | 3 | 6 | 2 |
Part IV: Selection of Top 2 Priorities
Part V: Efficacy, Impact, Feasibility and European Strength
- Efficacy, i.e., the likelihood that addressing the challenge(s) would result in an effective intervention to diminish the appearance of a disease or its consequences or solve a concrete problem.
- Impact on Europe, i.e., the probability that targeting the challenge(s) would result in an impact for Europeans and/or for society (e.g., a decrease in disease burden, improvement of wellbeing, economic benefits, etc.).
- Feasibility in Europe, i.e., can the challenge(s) and actions be addressed in Europe?
- European research strength, i.e., relative competitiveness of Europe to other regions to meet the challenge and to achieve the advances.
2.4. Second Stage Analyses
3. Results
3.1. Sample Characteristics
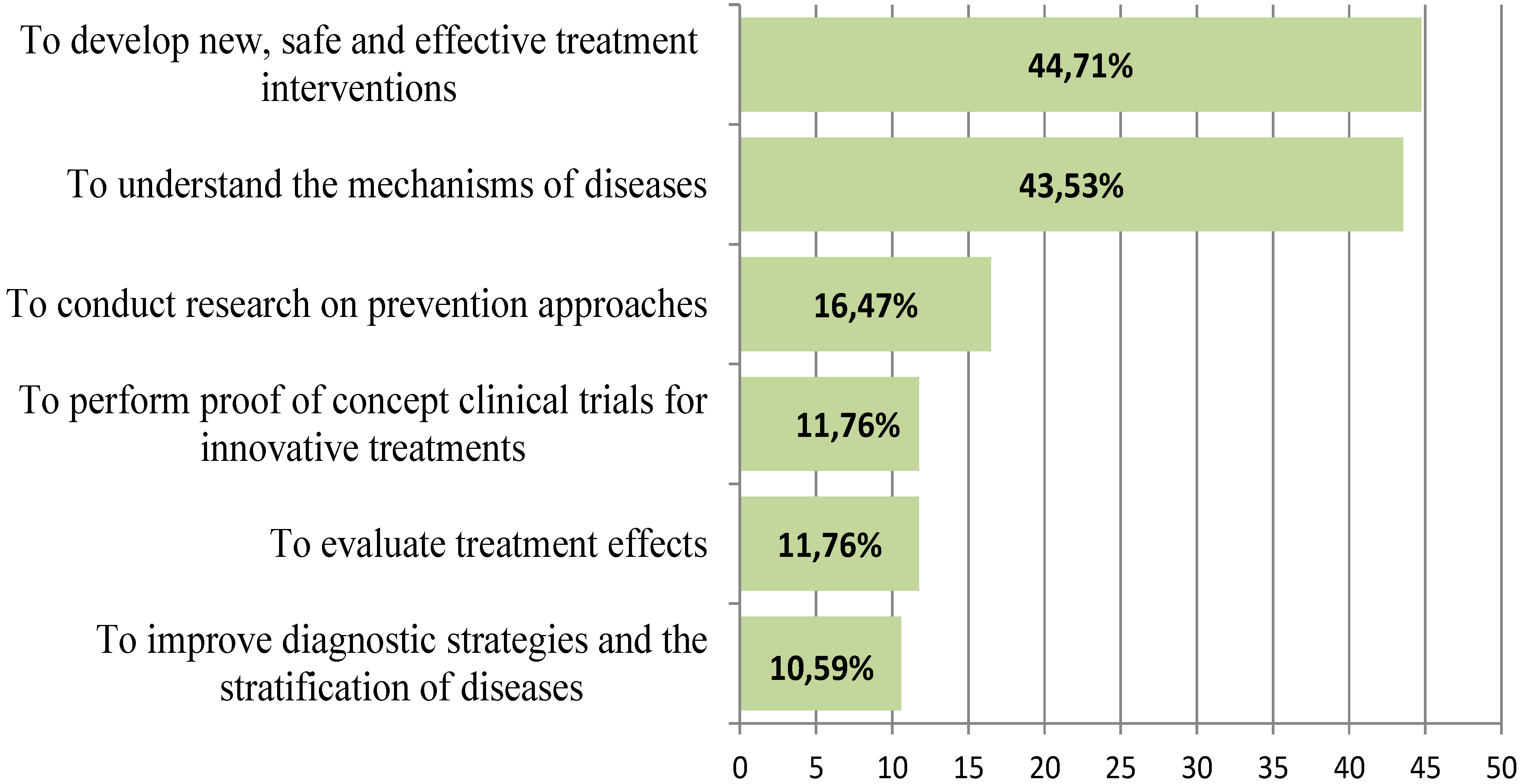
3.2. Top Priorities
- The development of new, safe and effective treatment interventions;
- Understanding the mechanisms of diseases; and
- Gaining more insight into the best outcomes to use for clinical mental health research.
Priority 1: The Development of New, Safe and Effective Treatment Interventions
- increasing the utilization of tailored approaches (personalized medicine);
- developing (eHealth/mHealth) decision aids/guidance tools that help the clinician to choose between various treatment modalities based on the type of mental disorder, stage/progression, previous outcomes, comorbidity and other factors;
- the development, assessment and use of eHealth/mHealth tools for the patient;
- developing specific treatments in order to better target comorbidity;
- developing more specific pharmacological, psychological and somatic treatments;
- increased attention for combined psychological and psychopharmacological approaches;
- developing deep brain stimulation, transcranial magnetic stimulation and other neuro-stimulation approaches for (treatment refractory) mental disorders.
- □
- To stimulate research on new intervention approaches yielding insight into the working mechanisms and to successfully develop effective new interventions. This research can/should specifically focus on:
- ▪
- exploring strategies in order to foster adherence to treatments/interventions;
- ▪
- exploring mediating factors;
- ▪
- exploring the role of these new treatments as an add-on intervention to existing interventions;
- ▪
- conducting research in order to identify the best diagnostic measures for complexity of interventions and treatment outcomes;
- ▪
- assessing differential treatment effects: are specific approaches more effective for specific subgroups?
- ▪
- conducting research on eHealth/mHealth approaches and assessing the level of human contact that is needed to motivate individuals towards sustained use of eHealth-/mHealth-based treatments in blended eHealth models;
- ▪
- conducting research that incorporates patient perspectives in treatment and in trial designs.
Priority 2: The Challenge to Understand the Mechanisms of Diseases
- gaining more insight into the neurobiological base of brain disorders;
- understanding staging and sub-typing of clinical trajectories based on underlying mechanisms of disease;
- exploring underlying mechanism in co-morbidity in severe mental disorders;
- taking into account protective factors for the development or course of disease;
- acknowledging the developmental perspective, in order to be able to intervene early;
- identifying environmental risk factors and their role in the mechanism of disease;
- integrating biological research with epidemiological, psychological and genetic research; and
- studying specific populations, such as children, adolescents and older people.
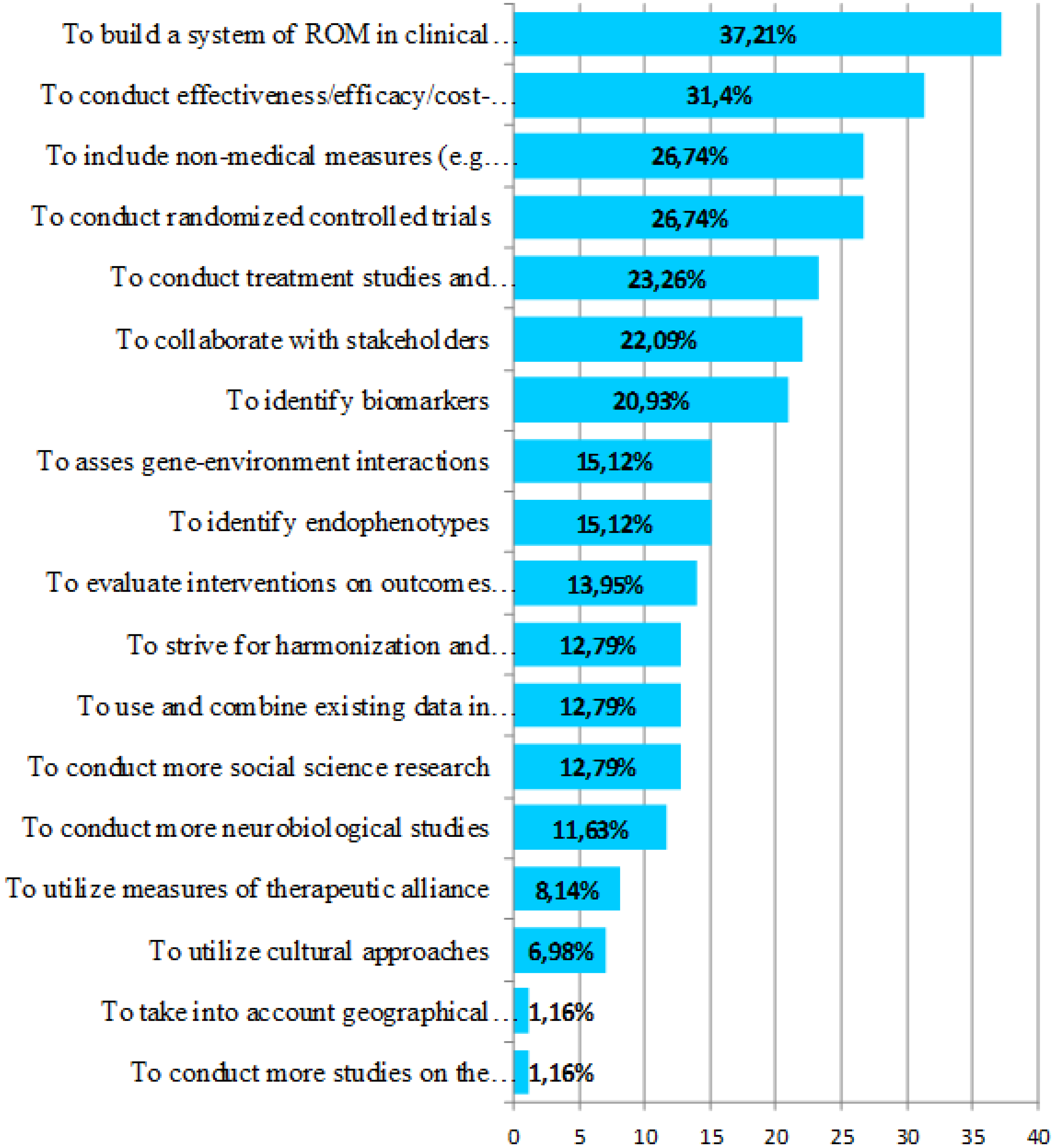
Priority 3: The Challenge to Gain More Insight into the Best Outcomes to Use for Clinical Mental Health Research
- standardizing research outcomes of psychological interventions;
- identifying outcome related biomarkers;
- increasing the focus on reducing long-term chronicity; and
- personalized prescribing of antipsychotic medication, discriminating between patients who do and patients who do not require sustained use of medication.
- □
- Building a system of routine outcome measures (ROM) in clinical practice;
- □
- Conducting effectiveness/efficacy/cost-efficacy studies;
- □
- Including non-medical measures that are relevant for patients as outcomes of intervention research, reflecting personal and social recovery (e.g., empowerment, income, housing, work life status, sense of meaningful life);
- □
- Conducting (alternatives for) randomized controlled trials (RCTs).

3.3. Efficacy, Impact, Feasibility and European Strength Concerning the Top Two Priorities

3.3.1. Importance of the Top Two Priorities in Terms of Efficacy
3.3.2. Importance of the Top Two Priorities in Terms of Impact
3.3.3. Feasibility and European Strength Regarding Targeting the Top Two Challenges
4. Discussion
4.1. Development of New Interventions
4.2. Understanding the Mechanisms of Diseases
4.3. Insight into the Best Outcomes to Use in Clinical Mental Health Research
4.4. Strengths and Limitations of This Study
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
- ▪
- Iman Elfeddali declares no conflict of interest.
- ▪
- Christina M. van der Feltz-Cornelis has received grant support for independent research from Eli Lilly.
- ▪
- Jim van Os has received unrestricted investigator-led research grants or recompense for presenting his research from Eli Lilly, Bristol-Myers Squibb, Lundbeck, Organon, Janssen-Cilag, GlaxoSmithKline, AstraZeneca, Pfizer, and Servier, companies that have an interest in the treatment of psychosis.
- ▪
- Susanne Knappe declares no conflict of interest.
- ▪
- Eduard Vieta has received grant support from Astra Zeneca, Ferrer, GSK, Lundbeck, Otsuka, Sunovion and Takeda
- ▪
- Hans-Ulrich Wittchen has received grant support for research from Lundbeck, Pfizer and Roche.
- ▪
- Carla Obradors-Tarragó declares no conflict of interest.
- ▪
- Josep Maria Haro has participated in advisory boards or has given educational presentations for Eli Lilly and Co, Lundbeck, Otsuka and Roche.
References
- Alonso, J. Burden of mental disorders based on the World Mental Health surveys. Revista Brasileira de Psiquiatria 2012, 34, 7–8. [Google Scholar] [CrossRef]
- Mheen Group. Employment and Mental Health: Assessing the Economic Impact and the Case for Intervention. Available online: http://eprints.lse.ac.uk/4236/1/MHEEN_policy_briefs_5_Employment%28LSERO%29.pdf (accessed on 10 January 2008).
- Gustavsson, A.; Svensson, M.; Jacobi, F.; Allgulander, C.; Alonso, J.; Beghi, E.; Dodel, R.; Ekman, M.; Faravelli, C.; Fratiglioni, L.; et al. Cost of disorders of the brain in Europe 2010. Eur. Neuropsychopharmacol. 2012, 21, 718–779. [Google Scholar] [CrossRef]
- Kessler, R.C.; Aguilar-Gaxiola, S.; Alonso, J.; Chatterji, S.; Lee, S.; Ormel, J.; Ustun, T.B.; Wang, P.S. The global burden of mental disorders: An update from the WHO World Mental Health (WMH) surveys. Epidemiol. Psichiatr. Soc. 2009, 18, 23–33. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Vos, T.; Lozano, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shinuya, K.; Salomon, J.A.; et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2197–2223. [Google Scholar] [CrossRef]
- Wittchen, H.U.; Jacobi, F.; Rehm, J.; Gustavsson, A.; Svensson, M.; Jönsson, B.; Olesen, J.; Allgulander, C.; Alonso, J.; Faravelli, C.; et al. The size and burden of mental disorders and other disorders of the brain in Europe 2010. J. Eur. Coll. Neuropsychopharmacol. 2011, 21, 655–679. [Google Scholar] [CrossRef]
- Catala-Lopez, F.; Genova-Maleras, R.; Vieta, E.; Tabares-Seisdedos, R. The increasing burden of mental and neurological disorders. Eur. Neuropsychopharmacol. 2013, 23, 1337–1339. [Google Scholar] [CrossRef] [PubMed]
- Wittchen, H.-U. The Burden of Mood Disorders. Science 2012, 338. [Google Scholar] [CrossRef]
- Haro, J.M.; Ayuso-Mateos, J.L.; Bitter, I.; Demotes-Mainard, J.; Leboyer, M.; Lewis, S.W.; Linszen, D.; Mario, M.A.J.; Mcdaid, D.; Anderas, M.L.; et al. ROAMER: Roadmap for mental health research in Europe. Int. J. Methods Psychiatr. Res. 2014, 23, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Emmelkamp, P.M.G.; David, D.; Beckers, T.; Muris, P.; Cuijpers, P.; Lutz, W.; Andersson, G.; Araya, R.; Banos Rivera, R.M.; Barkham, M.; et al. Advancing psychotherapy and evidence-based psychological interventions. Int. J. Methods Psychiatr. Res. 2014, 23, 58–91. [Google Scholar] [CrossRef] [PubMed]
- Evans-Lacko, S.; Courtin, E.; Fiorillo, A.; Knapp, M.; Luciano, M.; Park, A.L.; Brunn, M.; Byford, S.; Chevreul, K.; Forsman, A.; et al. The state of the art in European research on reducing social exclusion and stigma related to mental health: A systematic mapping of the literature. Eur. Psychiatry 2014, 29, 381–389. [Google Scholar] [CrossRef]
- Schumann, G.; Binder, E.B.; Holte, A.; de Kloet, E.R.; Oedegaard, K.J.; Robbins, T.W.; Walker-Tilley, T.R.; Bitter, I.; Brown, V.J.; Buitelaar, J.; et al. Stratified medicine for mental disorders. Eur. Neuropsychopharmacol. 2014, 24, 5–50. [Google Scholar] [CrossRef] [Green Version]
- Wittchen, H.-U. Mental health and disorders. Ed. Int. J. Methods Psychiatr. Res. 2014, 23, V–VI. [Google Scholar] [CrossRef]
- Wittchen, H.-U.; Knappe, S.; Andersson, G.; Araya, R.; Banos Rivera, R.M.; Barkham, M.; Bech, P.; Beckers, T.; Berger, T.; Berking, M.; et al. The need for a behavioural science focus in research on mental health and mental disorders. Int. J. Methods Psychiatr. Res. 2014, 23, 28–40. [Google Scholar] [CrossRef]
- Wittchen, H.-U.; Knappe, S.; Schumann, G. The psychological perspective on mental health and mental disorder research: Introduction to the ROAMER work package 5 consensus document. Int. J. Methods Psychiatr. Res. 2014, 23, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Van der Feltz-Cornelis, C.M.; van Os, J.; Knappe, S.; Schumann, G.; Vieta, E.; Wittchen, H.U.; Lewis, S.W.; Elfeddali, I.; Wahlbeck, K.; Linszen, D.; et al. Towards, Horizon 2020: Challenges and advances for clinical mental health research-outcome of an expert survey. Neuropsychiatr. Dis. Treat. 2014, 10, 1057–1068. [Google Scholar]
- Collins, P.Y.; Patel, V.; Joestl, S.S.; March, D.; Insel, T.R.; Daar, A.S.; Bordin, I.A.; Costello, E.J.; Durkin, M.; Fairburn, C.; et al. Grand challenges in global mental health. Nature 2011, 475, 27–30. [Google Scholar] [CrossRef]
- Adler, M.; Ziglio, E. Gazing into the Oracle: The Delphi Method and its Application to Social Policy and Public Health; Jessica Kingsley Publishers: London, UK, 1996. [Google Scholar]
- Custer, R.L.; Scarcella, J.A.; Stewart, B.R. The Modified Delphi Technique-A Rotational Modification. J. Vocat. Techn. Educ. 1999, 15, 50–58. [Google Scholar]
- Meyrick, J.D. The Delphi method and health research. Health Educ. 2003, 103, 7–16. [Google Scholar] [CrossRef]
- De Vet, E.; Brug, J.; De Nooijer, J.; Dijkstra, A.; Vries, N.K. Determinants of forward stage transitions: A Delphi study. Health Educ. Res. 2005, 20, 195–205. [Google Scholar]
- Elfeddali, I.; Bolman, C.; Mesters, I.; Wiers, R.; de Vries, H. Factors underlying smoking relapse prevention: Results of an international Delphi study. Health Educ Res. 2010, 25, 1008–1020. [Google Scholar] [CrossRef] [PubMed]
- Pacchiarotti, I.; Bond, D.J.; Baldessarini, R.J.; Nolen, W.A.; Grunze, H.; Licht, R.W.; Post, R.M.; Berk, M.; Goodwin, G.M.; Sachs, G.S.; et al. The International Society for Bipolar Disorders (ISBD) task force report on antidepressant use in bipolar disorders. Am. J. Psychiatry 2013, 170, 1249–1262. [Google Scholar] [CrossRef]
- Webropol 2.0, Online Survey and Analysis Software. Available online: http://www.webropol.com/ (accessed on 7 July 2014).
- Likert, R. A technique for the measurement of attitudes. Arch. Psychol. 1932, 140, 1–55. [Google Scholar]
- Linstone, H.A.; Turoff, M. The Delphi Method: Techniques and Applications; Addison-Wesley: Reading, MA, USA, 1975. [Google Scholar]
- Dols, A.; Sienaert, P.; van Gerven, H.; Schouws, S.; Stevens, A.; Kupka, R.; Stek, M.L. The prevalence and management of side effects of lithium and anticonvulsants as mood stabilizers in bipolar disorder from a clinical perspective: A review. Int. Clin. Psychopharmacol. 2013, 28, 287–296. [Google Scholar] [CrossRef]
- Fava, G.A.; Tossani, E.; Bech, P.; Berrocal, C.; Chouinard, G.; Csillag, C.; Wittchen, H.-U; Rief, W. Emerging clinical trends and perspectives on comorbid patterns of mental disorders in research. Int. J. Methods Psychiatr. Res. 2014, 1, 92–101. [Google Scholar] [CrossRef]
- Kramer, I.; Simons, C.J.; Hartmann, J.A.; Menne-Lothmann, C.; Viechtbauer, W.; Peeters, F.; Schruers, K.; Bemmel, A.L.; Myin-Germeys, I.; Delespaul, P.; et al. A therapeutic application of the experience sampling method in the treatment of depression: A randomized controlled trial. World Psychiatry 2014, 13, 68–77. [Google Scholar] [CrossRef]
- Van Os, J.; Delespaul, P.; Wigman, J.; Myin-Germeys, I.; Wichers, M. Beyond DSM and ICD: Introducing “precision diagnosis” for psychiatry using momentary assessment technology. World Psychiatry 2013, 12, 113–117. [Google Scholar]
- Hilty, D.M.; Ferrer, D.C.; Parish, M.B.; Johnston, B.; Callahan, E.J.; Yellowlees, P.M. The effectiveness of telemental health: A 2013 review. Telemed. J. E Health 2013, 19, 444–454. [Google Scholar] [CrossRef] [PubMed]
- Spek, V.; Cuijpers, P.; Nyklicek, I.; Riper, H.; Keyzer, J. Internet-based cognitive behaviour therapy for symptoms of depression and anxiety: A meta-analysis. Psychosom. Med. 2007, 37, 319–328. [Google Scholar] [CrossRef]
- Tate, D.; Finkelstein, E.; Khavjou, O.; Gustafson, A. Cost effectiveness of internet interventions: Review and recommendations. Ann. Behav. Med. 2009, 38, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Rains, S.; Young, V. A meta-analysis of research on formal computer-mediated support groups: Examining group characteristics and health outcomes. Hum. Commun. Res. 2009, 35, 309–336. [Google Scholar] [CrossRef]
- Lal, S.; Adair, C.E.A. E-mental health: A rapid review of the literature. Psychiatr. Serv. 2014, 65. [Google Scholar] [CrossRef]
- Wichers, M.; Hartmann, J.A.; Kramer, I.M.; Lothmann, C.; Peeters, F.; van Bemmel, L.; Myin-Germeys, I.; Delespaul, P.; van Os, J.; Simons, C.J.P. Translating assessments of the film of daily life into person-tailored feedback interventions in depression. Acta Psychiatr. Scand. 2011, 123, 402–403. [Google Scholar] [CrossRef] [PubMed]
- Nordqvist, C.; Hanberger, L.; Timpka, T.; Nordfeldt, S. Health professionals’ attitudes towards using a Web 2.0 portal for child and adolescent diabetes care: Qualitative study. J. Med. Internet Res. 2009, 11. [Google Scholar] [CrossRef] [PubMed]
- Richards, H.; King, G.; Reid, M.; Selvaraj, S.; McNicol, I.; Brebner, E.; Godden, D. Remote working: Survey of attitudes to eHealth of doctors and nurses in rural general practices in the United Kingdom. Fam. Pract. 2005, 22, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Wells, M.; Mitchell, K.; Finkelhor, D.; Becker-Blease, K. Online mental health treatment: Concerns and considerations. CyberPsychol. Behav. 2007, 10, 453–459. [Google Scholar] [CrossRef] [PubMed]
- McLaren, P. Telemedicine and telecare: What can it offer mental health services? Adv. Psychiatr. Treat. 2003, 9, 54–61. [Google Scholar] [CrossRef]
- Myers, A.; Nemeroff, C.B. New vistas in the management of treatment-refractory psychiatric disorders: Genomics and personalized medicine. Focus 2010, 8, 525–535. [Google Scholar]
- Mehta, R.; Jain, R.K.; Badve, S. Personalized medicine: The road ahead. Clin. Breast Cancer 2011, 11, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Ozomaro, U.; Wahlestedt, C.; Nemeroff, C.B. Personalized medicine in psychiatry: Problems and promises. BMC Med. 2013, 11. [Google Scholar] [CrossRef]
- McManus, R.J.; Mant, J.; Haque, M.S.; Bray, E.P.; Bryan, S.; Greenfield, S.M.; Jones, M.I.; Jowett, S.; Little, P.; Penaloza, C.; et al. Effect of self-monitoring and medication self-titration on systolic blood pressure in hypertensive patients at high risk of cardiovascular disease: The TASMIN-SR randomized clinical trial. JAMA 2014, 312, 799–808. [Google Scholar] [CrossRef]
- Huijbregts, K.M.; de Jong, F.J.; van Marwijk, H.W.J.; Beekman, A.T.; Ader, H.J.; Hakkaart-van Rooijen, L.; Unutzer, J.; van der Feltz-Cornelis, C.M. A target-driven collaborative care model for major depressive disorder is effective in primary care in the Netherlands. A randomized clinical trial from the depression initiative. J. Affect. Disord. 2013, 146, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Mulley, A.G.; Trimble, C.; Elwyn, G. Stop the silent misdiagnosis: Patients’ preferences matter. BMJ 2012, 345. [Google Scholar] [CrossRef] [PubMed]
- Joseph-Williams, N.; Elwyn, G.; Edwards, A. Knowledge is not power for patients: A systematic review and thematic synthesis of patient-reported barriers and facilitators to shared decision making. Patient Educ. Couns. 2014, 94, 291–309. [Google Scholar] [CrossRef] [PubMed]
- Legare, F.; Ratte, S.; Stacey, D.; Kryworuchko, J.; Gravel, K.; Graham, I.D.; Turcotte, S. Interventions for improving the adoption of shared decision making by healthcare professionals. Cochrane Database Syst. Rev. 2010, 5. [Google Scholar] [CrossRef]
- Van der Feltz-Cornelis, C.M.; Andrea, H.; Kessels, E.; van Duivenvoorden, H.; Biemans, H.; Metz, M. Wat kan er met Routine Outcome Monitoring? Een klinisch-empirische verkenning inzake Shared Decision Making in combinatie met ROM bij patienten met gecombineerde lichamelijke en psychische klachten [Does routine outcome monitoring have a promising future? An investigation into the use of shared decision-making combined with ROM for patients with a combination of physical and psychiatric symptoms]. Tijdschrift voor Psychiatrie 2014, 56, 375–384. [Google Scholar]
- Harris, E.C.; Barraclough, B. Excess mortality of mental disorder. Br. J. Psychiatry 1998, 173, 11–53. [Google Scholar] [CrossRef] [PubMed]
- Wahlbeck, K.; Westerman, J.; Nordentoft, M.; Gissler, M; Laursen, T.M. Outcomes of Nordic mental health systems: Life expectancy of patients with mental disorders. Br. J. Psychiatry 2011, 199, 453–458. [Google Scholar] [CrossRef] [PubMed]
- Bushe, C.J.; Taylor, M.; Haukka, J. Mortality in schizophrenia: A measurable clinical endpoint. J. Psychopharmacol. 2010, 24, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Osborn, D.P.J.; Levy, G.; Nazareth, I.; Petersen, I.; Islam, A.; King, M.B. Relative risk of cardiovascular and cancer mortality in people with severe mental illness from the United Kingdom’s General Practice Research Database. Arch. Gen. Psychiatry 2007, 64, 242–249. [Google Scholar] [CrossRef]
- Saha, S.; Chant, D.; McGrath, J. A systematic review of mortality in schizophrenia: Is the differential mortality gap worsening over time? Arch. Gen. Psychiatry 2007, 64, 1123–1131. [Google Scholar] [CrossRef] [Green Version]
- Cuthbert, B.N. The RDoC framework: Facilitating transition from ICD/DSM to dimensional approaches that integrate neuroscience and psychopathology. World Psychiatry 2014, 13, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Vieta, E. The bipolar maze: A roadmap through translational psychopathology. Acta Psychiatr. Scand. 2014, 129, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Bouwmans, C.; De Jong, K.; Timman, R.; Zijlstra-Vlasveld, M.; Van der Feltz-Cornelis, C.; Tan, S.; Hakkaart-van Roijen, L. Feasibility, reliability and validity of a questionnaire on healthcare consumption and productivity loss in patients with a psychiatric disorder (TiC-P). BMC Health Serv. Res. 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Goorden, M.; Muntingh, A.; van Marwijk, H.; Spinhoven, P.; Ader, H.; van Balkom, A.; van der Feltz-Cornelis, C.M.; Hakkaart-van Roijen, L. Cost utility analysis of a collaborative stepped care intervention for panic and generalized anxiety disorders in primary care. J. Psychosom. Res. 2014, 77, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Goorden, M.; Vlasveld, M.C.; Anema, J.R.; van Mechelen, W.; Beekman, A.T.; Hoedeman, R.; van der Feltz-Cornelis, C.M.; Hakkaart-van Roijen, L. Cost-utility analysis of a collaborative care intervention for major depressive disorder in an occupational healthcare setting. J. Occup. Rehabil. 2013, 2013, 1–8. [Google Scholar]
- Jochems, E.C.; Mulder, C.L.; Duivenvoorden, H.J.; van der Feltz-Cornelis, C.M.; van Dam, A. Measures of motivation for psychiatric treatment based on self-determination theory: Psychometric properties in Dutch psychiatric outpatients. Assessment 2014, 21, 494–510. [Google Scholar] [CrossRef] [PubMed]
- Muntingh, A.; van der Feltz-Cornelis, C.; van Marwijk, H.; Spinhoven, P.; Assendelft, W.; de Waal, M.; Adèr, H.; van Balkom, A. Effectiveness of collaborative stepped care for anxiety disorders in primary care: A pragmatic cluster randomised controlled trial. Psychother. Psychosom. 2014, 83, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Vemer, P.; Bouwmans, C.A.; Zijlstra-Vlasveld, M.C.; van der Feltz-Cornelis, C.M.; Hakkaart-van Roijen, L. Let’s get back to work: Survival analysis on the return-to-work after depression. Neuropsychiatr. Dis. Treat. 2013, 9, 1637–1645. [Google Scholar]
- Van der Krieke, L.; Emerencia, A.C.; Aiello, M.; Sytema, S. Usability evaluation of a web-based support system for people with a schizophrenia diagnosis. J. Med. Internet Res. 2012, 14. [Google Scholar] [CrossRef]
- Lambert, M.J.; Harmon, C.; Slade, K.; Whipple, J.L.; Hawkins, E.J. Providing feedback to psychotherapists on their patients’ progress: Clinical results and practice suggestions. J. Clin. Psychol. 2005, 61, 165–174. [Google Scholar] [CrossRef]
- De Beurs, E.; den Hollander-Gijsman, M.E.; van Rood, Y.R.; van der Wee, N.J.; Giltay, E.J.; van Noorden, M.S.; van der Lem, R.; van Fenema, E.; Zitman, F.G. Routine outcome monitoring in the Netherlands: Practical experiences with a web-based strategy for the assessment of treatment outcome in clinical practice. Clin. Psychol. Psychother. 2011, 18, 1–12. [Google Scholar]
- Madan, A.; Borckardt, J.J.; Connell, A.; Book, S.B.; Campbell, S.; Gwynette, M.F.; Wimberly, L.A.; Weinstein, B.; McLeod-Bryant, S.; Cooney, H.; et al. Routine assessment of patient-reported outcomes in behavioral health: Room for improvement. Qual. Manag. Health Care 2010, 19, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, M.A.; Oude Voshaar, R.C.; Pot, A.M. Clinicians’ perspectives on a web-based system for routine outcome monitoring in old-age psychiatry in the Netherlands. J. Med. Internet Res. 2012, 14. [Google Scholar] [CrossRef]
- Hsu, C.C.; Sandford, B.A. The Delphi technique: Making sense of consensus. Pract. Assess. Res. Eval. 2007, 12, 1–8. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elfeddali, I.; Van der Feltz-Cornelis, C.M.; Van Os, J.; Knappe, S.; Vieta, E.; Wittchen, H.-U.; Obradors-Tarragó, C.; Haro, J.M. Horizon 2020 Priorities in Clinical Mental Health Research: Results of a Consensus-Based ROAMER Expert Survey. Int. J. Environ. Res. Public Health 2014, 11, 10915-10939. https://doi.org/10.3390/ijerph111010915
Elfeddali I, Van der Feltz-Cornelis CM, Van Os J, Knappe S, Vieta E, Wittchen H-U, Obradors-Tarragó C, Haro JM. Horizon 2020 Priorities in Clinical Mental Health Research: Results of a Consensus-Based ROAMER Expert Survey. International Journal of Environmental Research and Public Health. 2014; 11(10):10915-10939. https://doi.org/10.3390/ijerph111010915
Chicago/Turabian StyleElfeddali, Iman, Christina M. Van der Feltz-Cornelis, Jim Van Os, Susanne Knappe, Eduard Vieta, Hans-Ulrich Wittchen, Carla Obradors-Tarragó, and Josep Maria Haro. 2014. "Horizon 2020 Priorities in Clinical Mental Health Research: Results of a Consensus-Based ROAMER Expert Survey" International Journal of Environmental Research and Public Health 11, no. 10: 10915-10939. https://doi.org/10.3390/ijerph111010915
APA StyleElfeddali, I., Van der Feltz-Cornelis, C. M., Van Os, J., Knappe, S., Vieta, E., Wittchen, H. -U., Obradors-Tarragó, C., & Haro, J. M. (2014). Horizon 2020 Priorities in Clinical Mental Health Research: Results of a Consensus-Based ROAMER Expert Survey. International Journal of Environmental Research and Public Health, 11(10), 10915-10939. https://doi.org/10.3390/ijerph111010915