2.1. What is a Hypothesis-Generating Study?
We defined hypothesis-generating study as a “large” investigation in the sense that it is powered to detect elusive effects with multiple exposures or outcomes assessed (e.g., a case-control study with 1500 case-control sets and several exposures or cases and controls from multiple outcomes evaluated against a single exposure). The investigators believe that only a few of the examined associations are true because for most exposure-outcome associations that are to be investigated they have a weak hypothesis (e.g., not supported by either previous empirical work or biologic considerations) or no particular reason to believe that studied exposures and outcomes are associated (e.g., Genome-Wide or Exposure-Wide Association Studies, such as those that correlate all exposures measured in NHANES with a single health outcome [
5]). We focus on true associations that can be viewed as “weak”, e.g., with odds ratios of ≤2 for a typical categorization of exposure [
6]. Throughout our presentation, we denote probability density function of random variable
z as
f(
z).
The essential part of the calculation of the (posterior) distribution of the
False Positive Rate (FPR) is Bayesian and involves stating the probability that H
0 is true,
i.e., π, a
priori. This allows us to quantify how unlikely a given exposure is to be truly associated with the outcome. Since pre-existing knowledge about the association is nearly always imperfect, we will consider a distribution of
f(π) that is intended to capture a typical representation of hypothesis-generating studies, such that
f(π)~Uniform(0.7, 1): “nearly all of them wrong” [
1]. We also perform sensitivity analyses that either widen this distribution, which may be applicable to accidental releases of a known toxic chemical in which (a) hazards are largely unknown but biologically plausible or (b) narrow the distribution at the upper end of implausible as may be with a highly speculative association with no known mechanism. From the perspective of planning a study, instead of estimating FPR after data was observed, we can fix expected or desired effect size as a constant (denoted here as γ), since the calculation is conditioned on its specific value; however, in a specific application, investigators may wish to estimate FPR under uncertainty about γ by specifying
prior distribution
f(γ|π = 0). Of course, the
False Negative Rate (FNR) may also be of inherent interest at the study planning stage; we revisit this issue later.
For illustrative purposes, we consider a simple study with one binary exposure X imperfectly classified as W and binary outcome Y that measured perfectly, so that the data can be analyzed by estimating odds ratios from a 2 × 2 table. The value α will be fixed at the traditional 0.05 and power is estimated for each desired effect size. We will also consider, without loss of generality, exposure that has prevalence of 0.3 (= p(X = 1)) (alternative exposure prevalence values generated similar conclusions in the main simulations).
2.3. When Exposure is Perfectly Classified
First, let us review what happens to FPR when exposure classification is perfect, so that
W =
X given that SN = SP = 1. In this case, barring any systematic biases,
E(γ
*) =
E(γ), and we can proceed with calculation of FPR, fixing α = 0.05:
We conducted these calculations using expressions in
Supplementary File 1 to derive β (
i.e., to estimate power for a fixed minimal detectable effect and sample size and for type I error) over a specified distribution of π in 20,000 Monte-Carlo simulations (implemented in R [
8], see
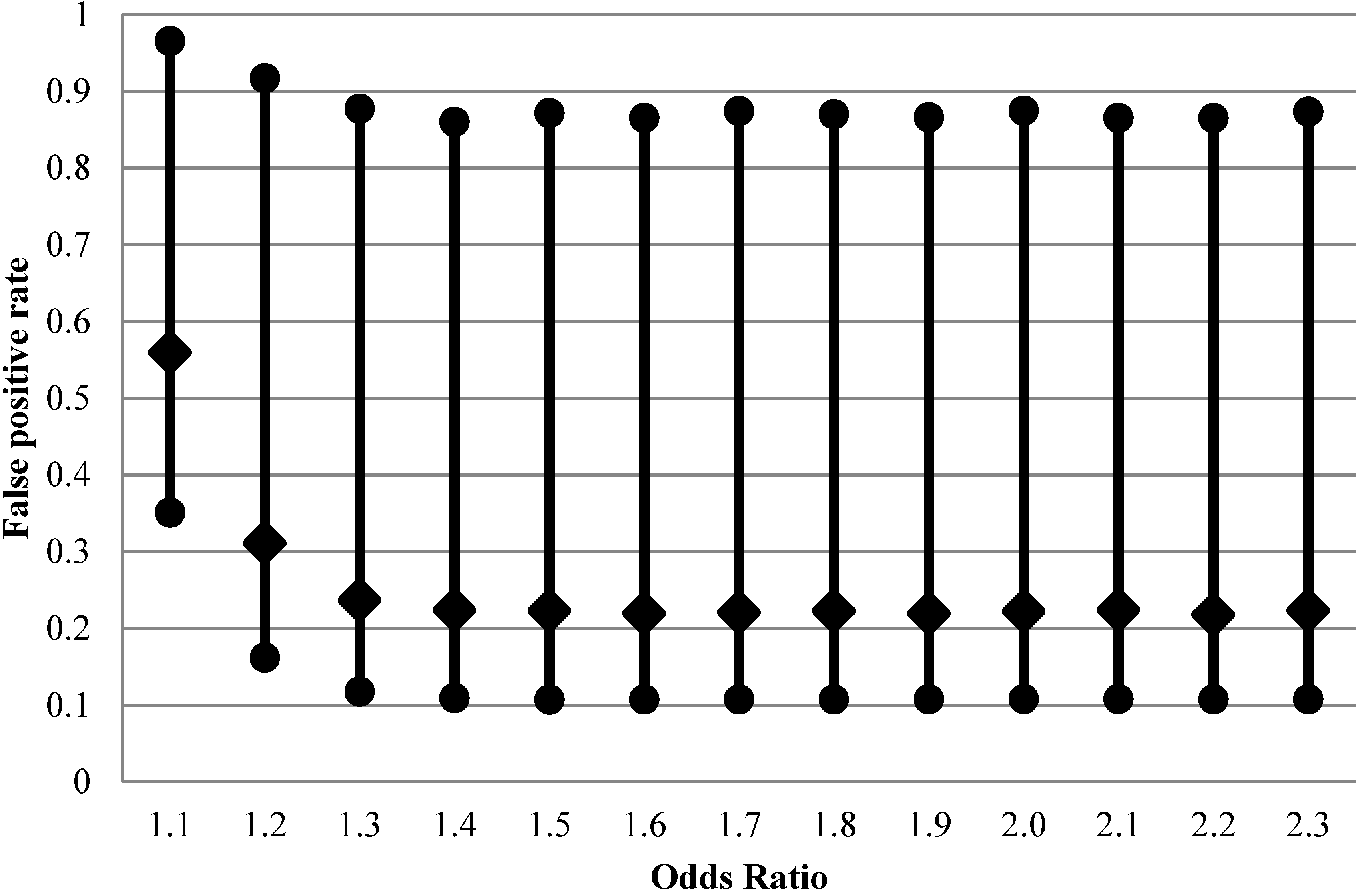
Supplementary File 2). The results of these calculations are presented in
Figure 1 for a range of odds ratios exemplifying true weak associations starting from odds ratio of 1.1. There is a wide variation of FPR that can be occurring in each individual analysis, with 95% range between 10 and 90%. While we structure the main narrative of this article around simulation results, analytical expressions for distributions of FPR and FNR exist (
Supplementary File 3) and are consistent with our results. Particularly, from the distributions of FPR and FNR and assuming
f(π)~Uniform
, we derive the analytical expressions of the expectation of FPR and FNR (
E(FPR),
E(FNR)), and the
-th conditional quantile of FPR (
:
These analytical expressions can be useful to study the trend of FPR and FNR when a certain parameter changes while the other parameters are fixed. We will look at it further in
Section 2.4. The R code in
Supplementary 3 can be used to perform theoretical percentile calculations of FPR and FNR.
Figure 1.
Impact of effect size on false positive rate (2.5th, 50th and 97.5th percentiles of 20,000 Monte-Carlo simulations) for fixed distribution of belief about probability of the effect being null (1500 case-control sets, type I error 5%, prevalence of exposure 30%, perfect exposure classification).
Figure 1.
Impact of effect size on false positive rate (2.5th, 50th and 97.5th percentiles of 20,000 Monte-Carlo simulations) for fixed distribution of belief about probability of the effect being null (1500 case-control sets, type I error 5%, prevalence of exposure 30%, perfect exposure classification).
2.4. Under the Misclassification of Binary Exposure
It is known that non-differential exposure misclassification can, on average, adversely affect power but is not expected to alter type I error rate (at least not in simple case we are considering). It is not realistic to expect perfect exposure classification in most observational studies, and this is a particularly germane expectation for hypothesis-generating studies. Perfect exposure measurement is can be exceedingly costly and, is usually unattainable anyway. To investigate the impact of non-differential misclassification of exposure on FPR, using fixed values of SN = 0.5 and SP = 0.9, which are realistic in many areas of epidemiology and certainly resemble the performance of exposure classifiers typically employed in occupational epidemiology [
9,
10,
11]. We will explore a range of other values of SN and SP through theoretical calculations in sensitivity analyses.
In this context, estimation of FPR proceeds in two steps. First, we determine the expected value of effect size γ
* given its presumed true value γ and the extent of exposure misclassification (defined by SN and SP). Second, we use the derived γ
* value to calculate actual rate of type II error (β
*) that is expected to be diminished due to exposure misclassification compared to the situation where exposure is perfectly classified. With these values in hand, we proceed to estimate FPR, fixing α = 0.05:
The rest of the calculation is the same as in the situation with no exposure misclassification; mathematical details and implementation in the R environment are in
Supplementary File 2. As can be seen from
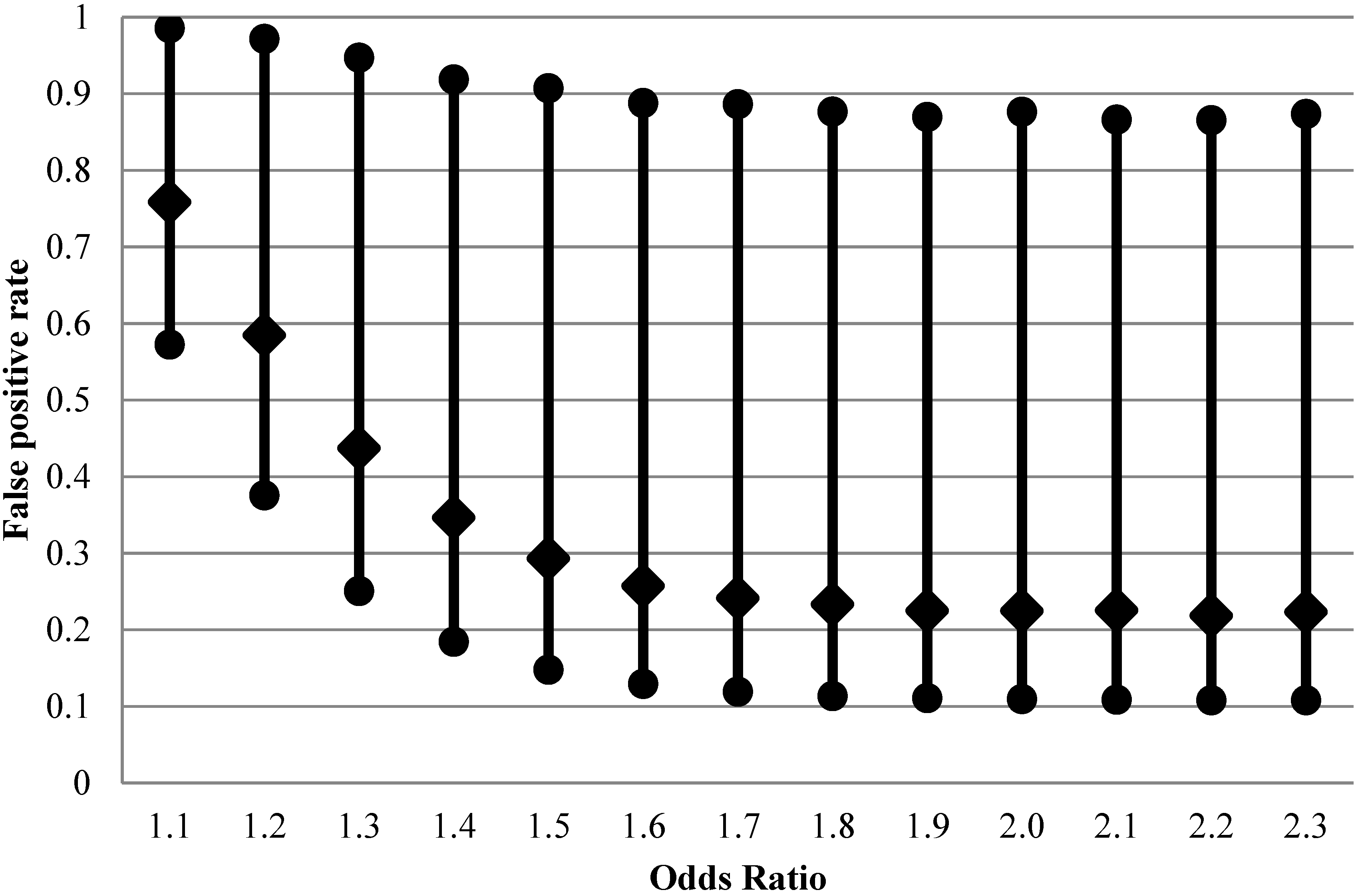
Figure 2, FPR is considerably higher than with perfect exposure assessment at design OR < 1.5, with expected values on the order of 30%–80% for the weaker effects.
Figure 2.
False positive rate (2.5th, 50th and 97.5th percentiles of 20,000 Monte-Carlo simulations) when exposure is imperfectly classified (sensitivity 0.5 and specificity 0.9) for fixed distribution of belief about probability of the effect being null (1500 case-control sets, type I error 5%, prevalence of exposure 30%, true rather than apparent odds ratios are shown).
Figure 2.
False positive rate (2.5th, 50th and 97.5th percentiles of 20,000 Monte-Carlo simulations) when exposure is imperfectly classified (sensitivity 0.5 and specificity 0.9) for fixed distribution of belief about probability of the effect being null (1500 case-control sets, type I error 5%, prevalence of exposure 30%, true rather than apparent odds ratios are shown).
When the nominal power of 80% is achieved at true OR = 1.6, the median of FPR is still at 25%, higher than the median when there is no exposure misclassification (21%,
Figure 1). The apparent OR at this point is expected to be 1.3.
Thus, we can see that although non-differential exposure misclassification is expected to attenuate OR, the net effect is not only the well-known loss of ability to detect true effects (the false negative conclusion) but also a concurrent increase in false positives, due to inflation in the variability of the estimated effects.One important caveat to these arguments is that we consider exposures, corresponding to multiple exposure-outcome hypotheses, which are independent. This is rarely true in practice and affects FPR (e.g., [
12]). The complex pattern of impact of measurement error on correlated covariates, with direction and magnitude of biases, are difficult to anticipate based on intuition alone (e.g., [
13]).
With the analytic expressions related to the distributions of FPR and FNR in
section 2.3, we can also study how parameters other than the values of target odds ratio may affect FPR and FNR. The R code required to generate these results is given as
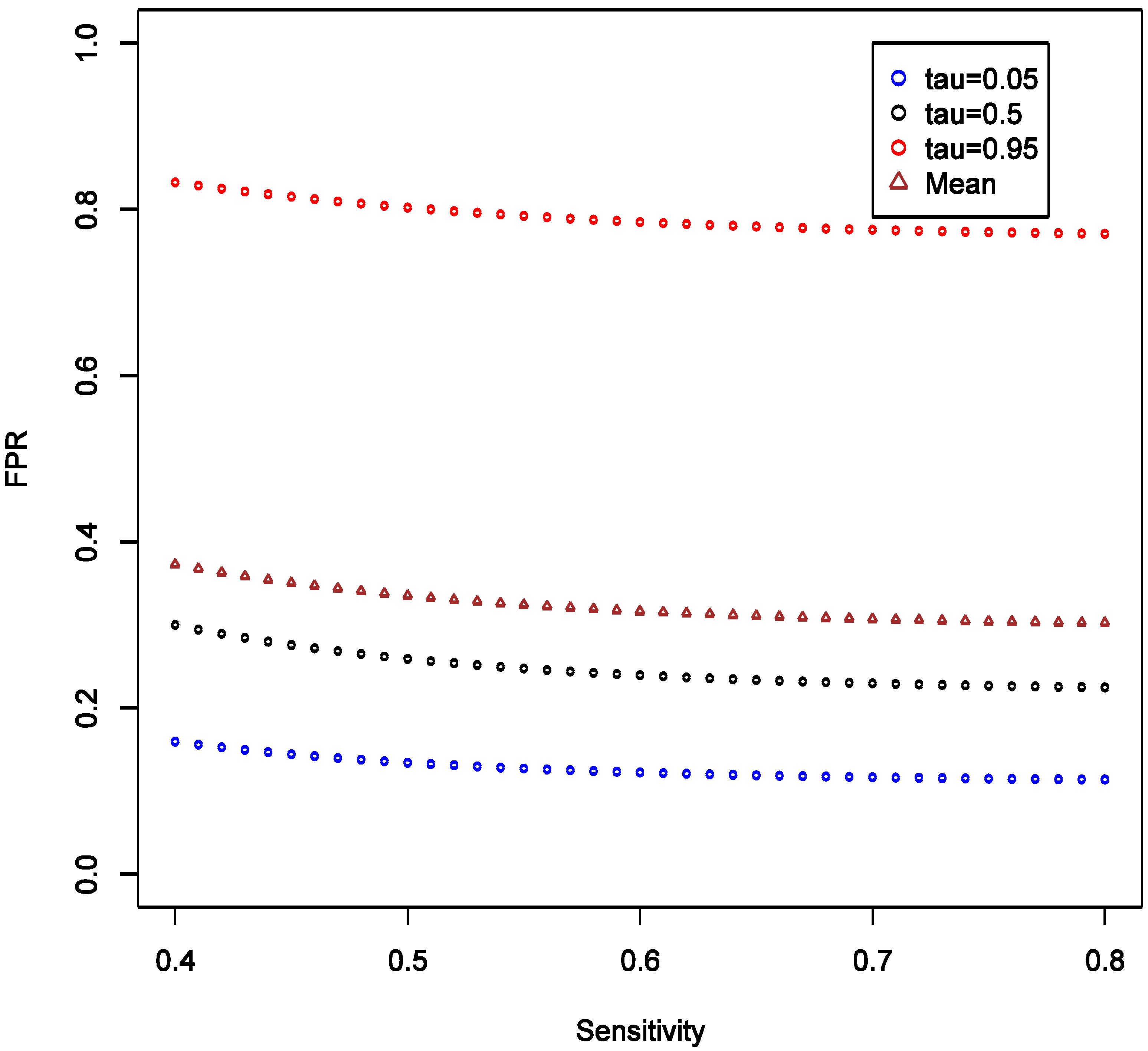
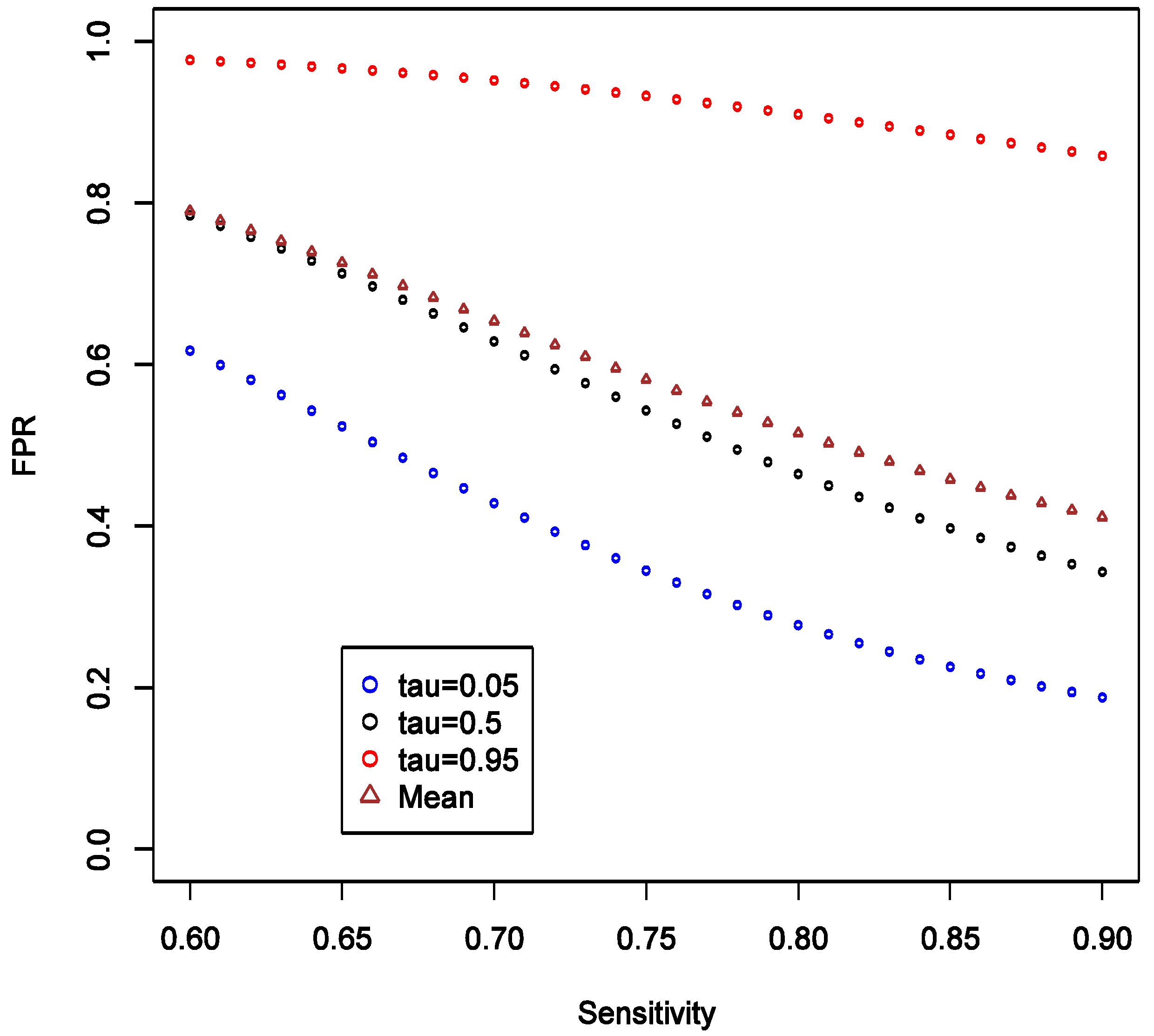
Supplementary File 4. To investigate the effect of SN, we consider the scenario with fixed OR at 1.6, and varying SN from 0.4 to 0.8, while keeping SP fixed at 0.9 and all other parameters as in the main example. We observed that the expectation, 5% and 95% quantiles of FPR are all quite robust to the changes in SN, and the variation of the distribution seems stable (
Figure 3).
Figure 3.
Theoretical calculations of the impact of varying sensitivity of exposure classifier while keeping specificity fixed at 0.9; tau (τ) = expected quintiles of the distribution for false positive rate (FPR); see text for details of other parameter settings.
Figure 3.
Theoretical calculations of the impact of varying sensitivity of exposure classifier while keeping specificity fixed at 0.9; tau (τ) = expected quintiles of the distribution for false positive rate (FPR); see text for details of other parameter settings.
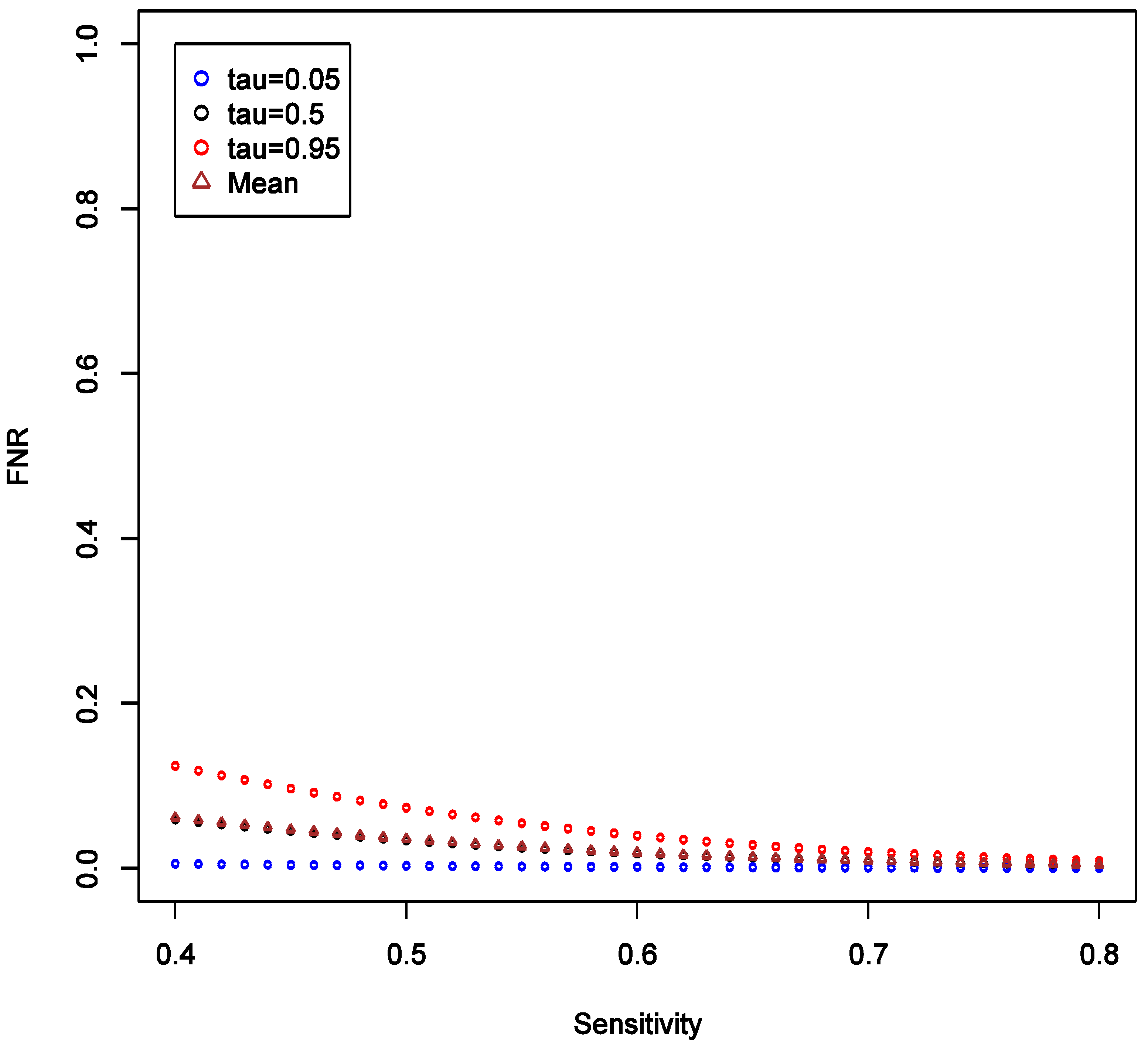
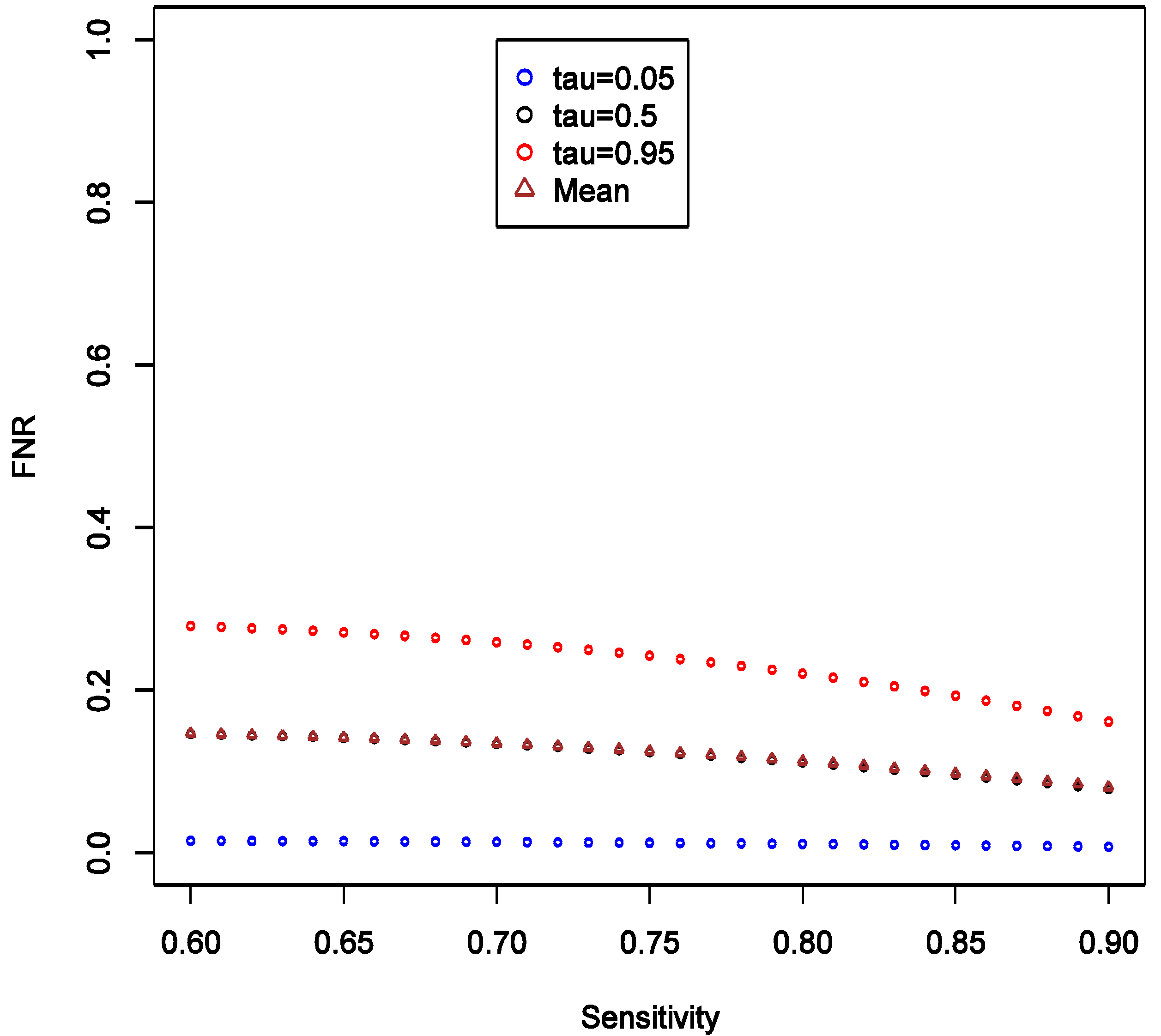
This implies that the chance of false positive is insensitive to increase in SN of exposure classifier. With increasing SN, the FNR tends to decrease, and such decrease is more obvious in the higher quantiles (
Figure 4), implying that our confidence in negative (null) results ought to grow as well. Unlike the effect on FPR, the variation of the distribution of FNR decreases substantially with increasing SN and FNR becomes considerably smaller than FPR (40%
vs. <5%). Overall, we conclude that under such settings the confidence in null result ought to be greater than the confidence in a non-null result. This also confirms intuition that boosting sensitivity, so long as SP is maintained at a high value, has negligible impact on the chance of picking up true signal from noise case-control studies of uncommon exposures. As in the main example explored though simulations, FNR is calculated to be smaller than FPR across the settings.
Figure 4.
Theoretical calculations of the impact of varying sensitivity of exposure classifier while keeping specificity fixed at 0.9; tau (τ) = expected quintiles of the distribution for false positive negative (FNR); see text for details of other parameter settings.
Figure 4.
Theoretical calculations of the impact of varying sensitivity of exposure classifier while keeping specificity fixed at 0.9; tau (τ) = expected quintiles of the distribution for false positive negative (FNR); see text for details of other parameter settings.
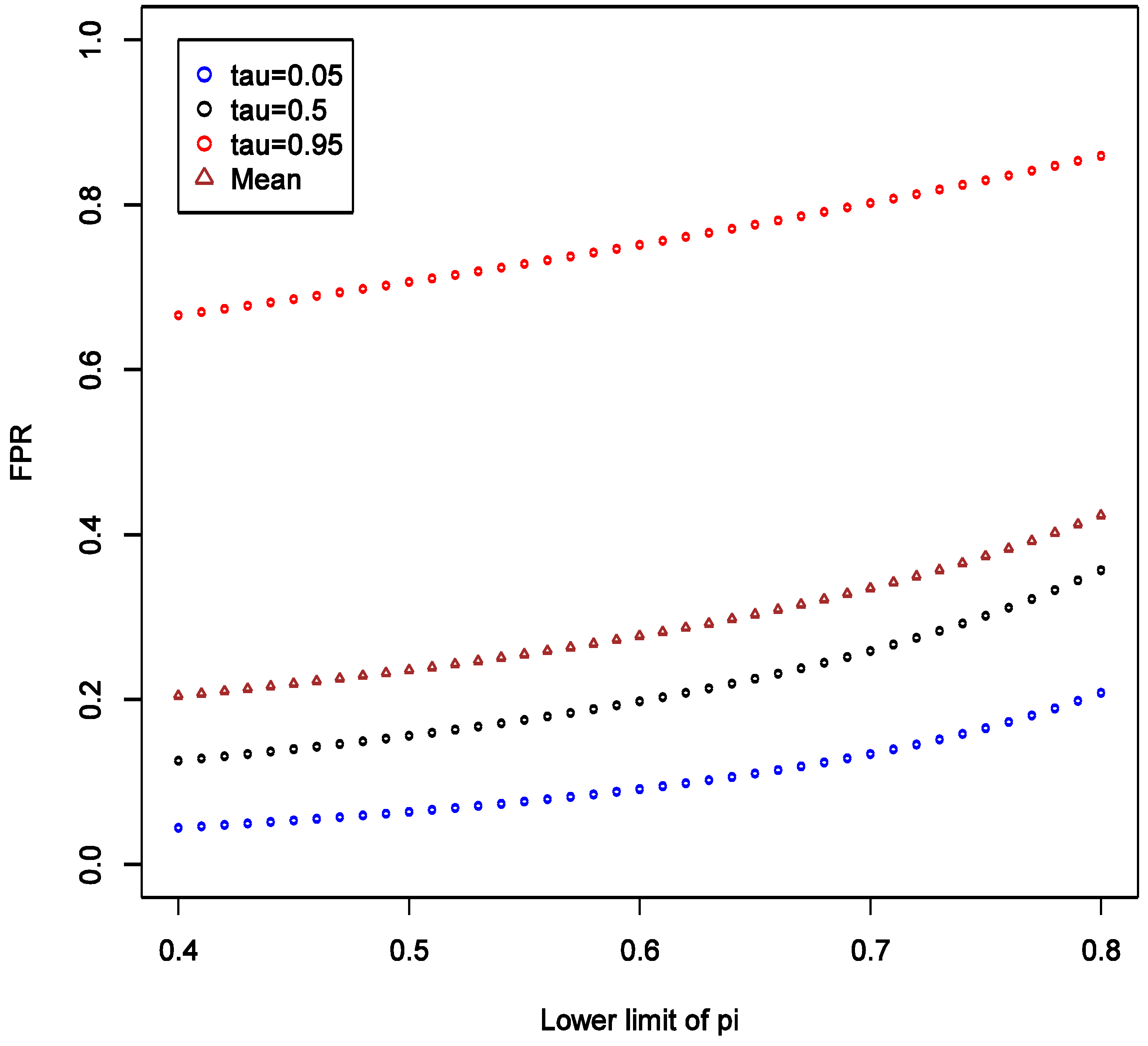
We also consider varying the lower limit of the prior distribution of π from 0.4 to 0.8 with the upper limit fixed at 1, while keeping all other parameters fixed as in the main example. This reflects varying degree of uncertainty about strength of hypothesis. We observed that as the lower limit increases, the mean, the 5% and 95% quantiles of FPR all increase, and the variation of the distribution appears to be stable (
Figure 5).
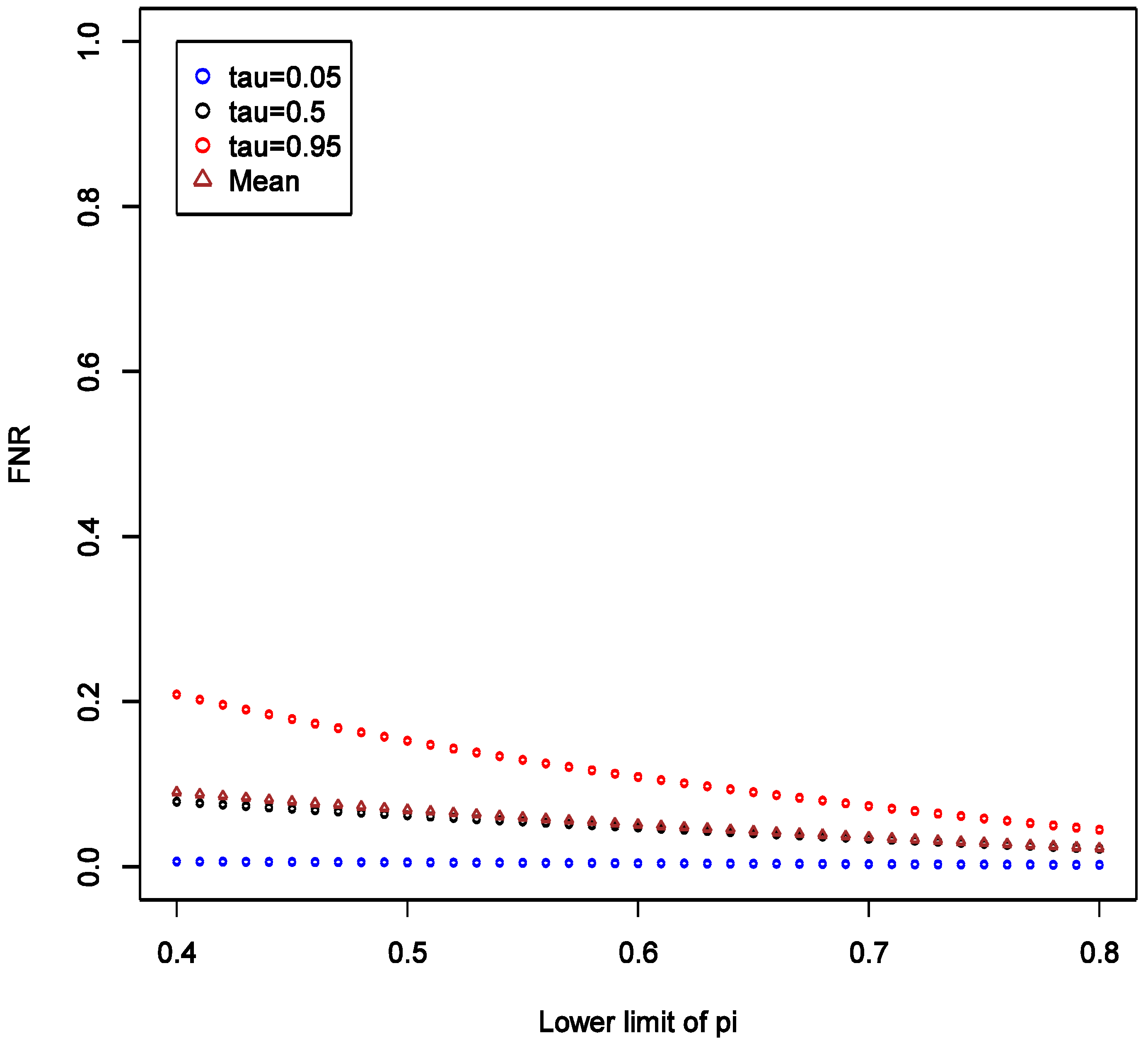
There is also a natural increase in certainty that a “statistically significant” result is a false positive as the prior on it being so becomes narrower with higher lower bound. The increasing lower limit of
distribution instead leads to a decrease in FNR especially at high quantiles, and the variation of distribution decreases (
Figure 6). Again, we see by comparing
Figure 5 and
Figure 6 that FNR is smaller across wide range of settings than FPR—
i.e., more confidence can be placed on findings consistent with the null. The other conclusion that we can draw from these calculations is the confirmation that the stronger the prior (here in a sense that the distribution of
is narrow or has a higher lower limit), the less informative any data becomes in arriving at novel conclusions. Thus, it is very important to articulate such priors at least qualitatively, if not quantitatively in the motivation of research.
Figure 5.
Theoretical calculations of the impact of varying strength belief in null hypothesis being true = pi (π); tau (τ) = expected quintiles of the distribution for false positive rate (FPR); see text for details of other parameter settings.
Figure 5.
Theoretical calculations of the impact of varying strength belief in null hypothesis being true = pi (π); tau (τ) = expected quintiles of the distribution for false positive rate (FPR); see text for details of other parameter settings.
Figure 6.
Theoretical calculations of the impact of varying strength belief in null hypothesis being true = pi (π); tau (τ) = expected quintiles of the distribution for false negative rate (FNR); see text for details of other parameter settings.
Figure 6.
Theoretical calculations of the impact of varying strength belief in null hypothesis being true = pi (π); tau (τ) = expected quintiles of the distribution for false negative rate (FNR); see text for details of other parameter settings.
Lastly, we investigated expected effect on FPR and FNR when SN is greater than SP, as might be expected when not all sources of a ubiquitous compound (e.g., polycyclic aromatic hydrocarbons, benzene, bisphenol-A, perfluorinated acids,
etc.) are accounted for in exposure assessment. To accomplish this, we fixed SP = 0.5 and varied SN from 0.6 to 0.9, keeping all other parameters fixed as in the main example; see
Supplementary File 5 for implementation details. Comparing
Figure 3 and
Figure 7, we note that having SP exceed sensitivity (at least in this setting) stabilizes FPR on average at around 0.4, while when SP is lower than SN, the average FPR tends to be large and only approaches 0.4 when SN is at the upper end of 0.9. As SN increases relative to SP the rates of both false positives (
Figure 7) and false negatives (
Figure 8) decline: the higher the quality of data the more reliable the conclusions. Yet again, FPR is higher than FNR, reflecting, most likely, influence of prior belief consistent with the exploratory nature of the study design we are considering. The distribution of FNR appears to be relatively insensitive to increase in SN relative to SP (
Figure 8). Comparing
Figure 4 and
Figure 8, we also observe that FNR is more favorable when SP exceeds SN. This reinforces previous work that in case-control studies, SP should be kept higher than SN [
14], though that conclusion was reached without consideration of FPR.
While our findings appear to be robust, we cannot be certain that exceptions to patterns we have reported do not occur. It is for this reason that we share with the reader all the tools necessary to evaluate their specific circumstances though the supplemental materials.
Figure 7.
Theoretical calculations of the impact of varying sensitivity of exposure classifier while keeping specificity fixed at 0.5; tau (τ) = expected quintiles of the distribution for false positive rate (FPR); see text for details of other parameter settings.
Figure 7.
Theoretical calculations of the impact of varying sensitivity of exposure classifier while keeping specificity fixed at 0.5; tau (τ) = expected quintiles of the distribution for false positive rate (FPR); see text for details of other parameter settings.
Figure 8.
Theoretical calculations of the impact of varying sensitivity of exposure classifier while keeping specificity fixed at 0.5; tau (τ) = expected quintiles of the distribution for false negative rate (FNR); see text for details of other parameter settings.
Figure 8.
Theoretical calculations of the impact of varying sensitivity of exposure classifier while keeping specificity fixed at 0.5; tau (τ) = expected quintiles of the distribution for false negative rate (FNR); see text for details of other parameter settings.
2.5. How do These Calculations Help Make Decisions & Plan Studies?
Consider a case-control study with 1500 cases and 1500 controls, aiming to detect OR of at least 1.3, while allowing for 5% type I error rate and assuming prevalence of exposure of 30%. The conventional power calculation indicates that power is ~90% so we may feel encouraged, on statistical grounds, to pursue the study as one that can yield valuable insights into the hypothesis. However, after considering typical values of exposure misclassification assuming SN = 0.5 and SP = 0.9, the re-calculated power is only 36%! This is a more realistic assessment of whether to pursue such a weak effect as OR = 1.3.
Next, consider that among exposures that the study can evaluate with respect to the outcome, there is one that also has prevalence of 30% and with expected effect, based on prior literature, of at least OR of 1.6. Re-estimation of power under exposure misclassification is rather encouraging: 80%. But is this enough to proceed with the study? Let us further consider that prior evidence for this particular exposure causing the disease is “weak” as we posit in this paper (i.e., f(π)~Uniform(0.7, 1)). Then our calculations reveal that we can expect the chance of false positive results for this association to be between 26 and 89%, with 95% probability. This is a far cry from the reassuring 5% figure implied (incorrectly!) by type I error rate. On the other hand, if we could be certain that f(π)~Uniform(0, 0.3), i.e., there is at most 30% chance that null is true, then the 97.5th percentile of FPR can be estimated to be 2.5%. Clearly one should weigh carefully whether study is worth pursuing when one cannot be reasonably certain that “positive” findings are sufficiently trustworthy.
The terminology “reasonably certain” and “sufficiently trustworthy” was left intentionally vague at the end of previous paragraph. These quantities can only be appraised if we consider the consequences of drawing false conclusions (i.e., acting on wrong assumption about how the world actually works). In the context of environmental and occupational epidemiology, this means assessing societal costs of making wrong decision. One can argue that decisions are never made based on a results of a single study but rather involve synthesis of a vast body of knowledge that may involve meta-analyses or pooled re-analyses of multiple investigations. We do not disagree with this general statement. However, it is always worth considering whether one more study will change how we view the world (e.g., accept or reject conjecture) or act on it (e.g., conduct more research, take a product off the market, impose regulations on exposure or a product). Even if a study does not lead to any material change, the lack of change is in fact consequence of a study. Thus, every investigation that is informative (i.e., not of such poor quality that it contains no information) has consequences. Once we accept this, we shall be closer to conducting useful and responsible research: every well-conducted study counts and the question only is just how much it counts or matters. We shall not develop this argument further in the current manuscript but challenge ourselves and the reader to reflect on these matters and attempt to address them in specific applied problems that we face in epidemiology and public health.
Furthermore, if there is a cause of a specific outcome among studied exposures, then it is also important to consider the
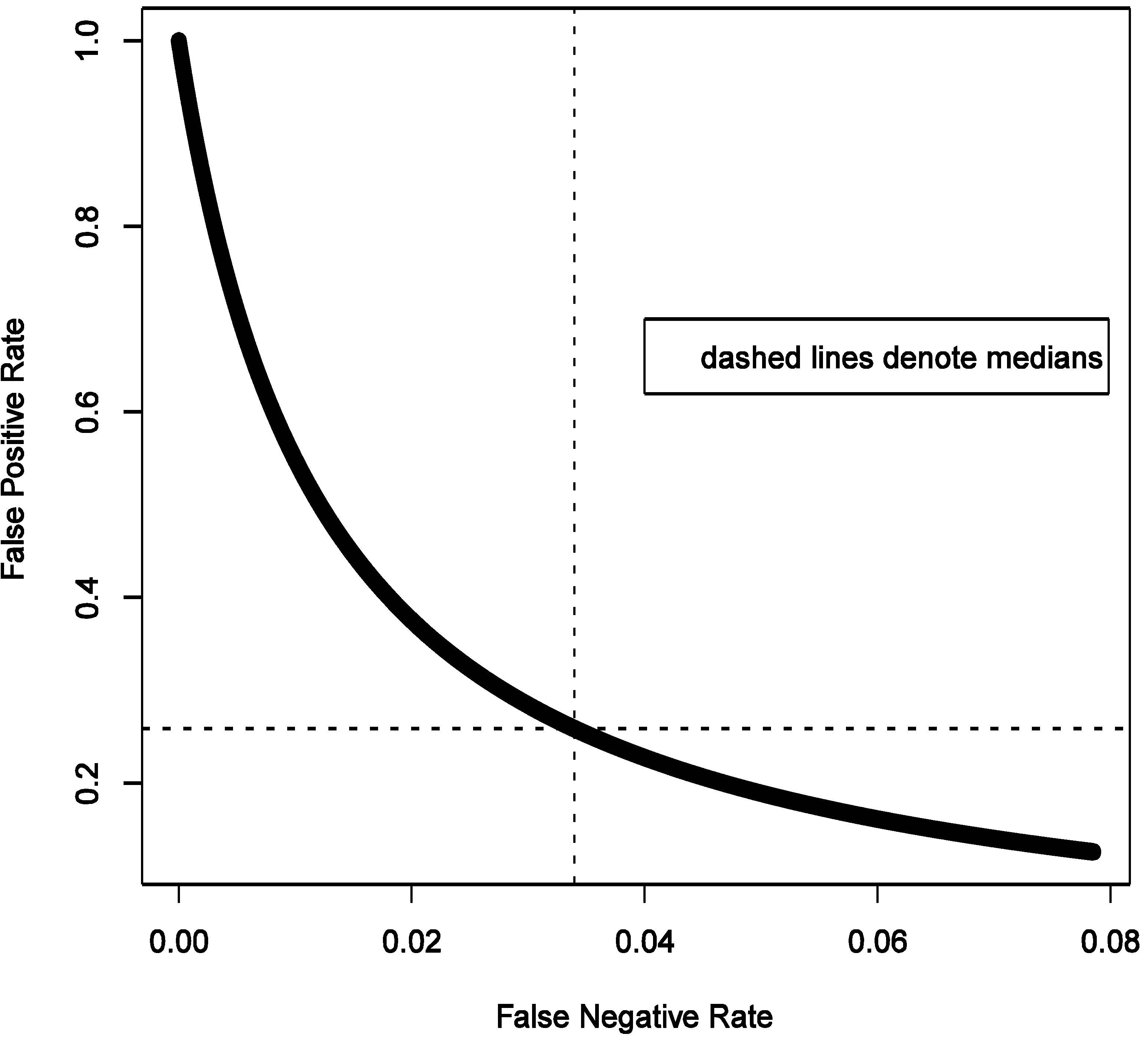
consequences of a false negative finding. We start with belief that at least some of the exposures we study do cause the outcome. To formally consider this, we need to calculate false negative rate estimated as FNR = β × (1 − π)/(β × (1 − π) + (1 − α) × π) under the same conditions as calculation of FPR. For a hypothesis generating study that we describe above in the simulations that anchor the main narrative, with OR = 1.6 and imperfect exposure assessment, FNR can be estimated to have median of 3.4% with 95% of the values falling between 0.2 and 7.6% (procedure for estimation is analogous to FPR and is summarized in code in
Supplementary File 2).
Figure 9 shows that FNR is relatively invariant and small compared to FPR in this situation. This confirms intuition that false negative findings are unlikely in a hypothesis-generating study and such work can be more reassuring than not when it fails to uncover associations. This observation is consistent with theoretical expectations derived in section 2.4 and presented in
Figure 3,
Figure 4,
Figure 5 and
Figure 6.
Let us explore some implications numerically in hypothetical study that has been the focus of this article. For this purpose, we fix OR = 1.6, α = 0.05, assumed exposure misclassification as defined above. The expected probabilities of the four study outcomes are summarized in the
Table 1 (from 20,000 MC simulations).
It is curious to note that as FPR exceeds FNR (
Figure 9), we can also expect on average more false positive results (4%) than false negative ones (3%); the certainty of false positive result is greater as seen from much narrower variability of the estimate (±1%
vs. ±3%). True negative findings are expected to dominate results of study we are considering. This is consistent with the notion that the likelihood of there being a true association is small in a hypothesis-generating study.
Figure 9.
Illustrated relationship between false positive and false negative rates in a hypothesis generating study: 20,000 Monte-Carlo simulations when exposure is imperfectly classified (sensitivity 0.5 and specificity 0.9) for fixed distribution of belief about probability of the effect being null (1500 case-control sets, type I error 5%, prevalence of exposure 30%, true odds ratio 1.6).
Figure 9.
Illustrated relationship between false positive and false negative rates in a hypothesis generating study: 20,000 Monte-Carlo simulations when exposure is imperfectly classified (sensitivity 0.5 and specificity 0.9) for fixed distribution of belief about probability of the effect being null (1500 case-control sets, type I error 5%, prevalence of exposure 30%, true odds ratio 1.6).
Table 1.
Expected rates of different outcomes of study considered in
Figure 9 (percent: median, (2.5 to 97.5%)).
Table 1.
Expected rates of different outcomes of study considered in Figure 9 (percent: median, (2.5 to 97.5%)).
| The truth | Acceptance of H0 |
|---|
| Reject | Do not Reject |
|---|
| H0 is true | FP | TN |
| 4 | 80 |
| (3–5) | (67–94) |
| H0 is false | TP | FN |
| 12 | 3 |
| (1–24) | (0.1–6) |
We argue that these issues must be addressed while applying for funding.
i.e., motivating research on a given topic. Power calculations can be corrected for expected or suspected misclassification in a given setting. The question of just how good the exposure estimates are is usually debated and presented in any grant proposal, with the applicants maintaining a fine balance between claiming that exposure assessment methods are useful without overstating their utility. At the very least, the applicants must defend a position that exposure assessment is adequate and in doing so they can refer to previous research with similar exposure assessment tools—there is plenty of relevant literature most common applications such as assessment of exposure to in case-control studies (e.g., see [
15]). It is typically possible to derive sensible guesses on SN and SP from the existing research, even if one has to ask for experts to guess such values, e.g., see Liu
et al [
10]. If the information on quality of exposure assessment is completely lacking or yields calculations that are too uncertain to be useful, this argues for a grant to be submitted to develop and test exposure assessment tool. Such projects, sadly, are difficult to find support for but it has been argued by many that they are absolutely essential to progress in the field. Perhaps our work will add to substantial body of evidence that argues for better understating of exposure assessment methods and their improvement (impossible without assessments of reliability and validity).
It is also important to reflect what our calculations mean for interpretation of studies. It is possible to conduct Bayesian analysis of “hypothesis-generating” studies that accounts for the likelihood of any specific association being true (
i.e., the distribution of π) although developing such a method is outside of scope of current work. Outside of application of formal methods for determining false discovery rate,
etc., it is also possible to appraise such results qualitatively in light of the expected false positives and negatives (as in
Table 1), as one does with the simplest corrections for multiple comparisons in hypothesis testing (
i.e., expecting 1/20 associations be by due to chance with statistical significance is set at 5%). It is reasonable to argue that our analytical framework more naturally applies to “confirmatory” rather than “exploratory” studies if one accepts that all possible hypotheses already exist [
1]. From this perspective, we would be interested in evaluating both the strength of exposure-outcome association (θ, typically a coefficients of regression used to estimate the disease model) supported by the data and consistent with hypothesized effect, and the probability that the null effect is true given some observed association in the data (
i.e., π). Formally, we would be interested in the
posterior distributions
f(θ|data) and
f(π|data). Given that, intuitively, the knowledge about value of θ is related to knowledge of how likely it is equal exactly to the null value, the
posterior distribution of interest,
f(θ,π|data), is anticipated to be a mixture distribution with point mass density at null governed by
f(π|data), such that, say δ~
Bernoulli(π) is an indicator variable of whether θ is null and a constant when δ = 1, or θ is non-null and follows a continuous distribution, such as normal for log-OR, when δ = 0. In this case we need to view π as a hyper-parameter in a Bayesian hierarchical model. By Bayes theorem, the model that we need to then consider is
f(θ,π|data) =
f(data| θ,π)
f(θ)
f(π)/
f(data), where
f(data|θ,π) is the likelihood, and
f(θ) is the
prior on the disease model parameter(s). The analytic approach should be able incorporate correction for measurement error and risk factor misclassification [
13], as well as latent confounding, making it a perhaps a very useful general framework for a wide range of data analysis problems common in epidemiology. We will not develop this argument further at present.













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}