3.1. Health Survey Results
The descriptive demographic statistics are summarized in
Table 1. Interviews were conducted in 120 households (
n = 785 individuals). Average household size was 6.7 members, with several homes having more than 20 members. As in many developing countries, the age-structure of the population was young; 14% of individuals were under five years and 52% were under age 18 years. The median age was 17 years and average age was 21 years.
The top three gastrointestinal illness (GI) symptoms reported during the survey were stomach cramps, diarrhoea and fever (
Table 2). On average, stomach cramps were reported to last 6 days (range 1–60 days); diarrhoea, 6 days (1–28); and fever, 8 days (1–60). 11% of the total survey population reported receiving care at a hospital (average duration 2.1 days) and 16% reported being under a doctor’s care (average 6.6 days).
Table 1.
Descriptive statistics of demographic information obtained from heath surveys.
Table 1.
Descriptive statistics of demographic information obtained from heath surveys.
| Demographic Category | Category of Measure | Number | % of Total Study Population (Individuals) |
|---|
| Number of Households Surveyed | Total | 120 | - |
| Number of Individuals Included on Surveys | Total | 785 | - |
| Age | Mean | 21.0 years | - |
| | Median | 17 years | - |
| | Range | 3 days-100 years | - |
| Number less than 5 years | Total | 97 | 13.8% |
| Number between 5-18 years | Total | 286 | 40.6% |
| Number less than 18 years | Total | 367 | 52.1% |
| Number between 19-60 years | Total | 301 | 42.8% |
| Number over 60 years | Total | 101 | 14.3% |
| Gender | Total Males | 385 | 49.0% |
| | Total Females | 400 | 51.0% |
| Household Size | Mean | 6.7 people | - |
| | Median | 6.5 people | - |
| | Range | 2–25 people | - |
| Religion | Total Muslim | 640 | 81.5% |
| | Total Christian | 143 | 18.2% |
| | Total Animist/Other | 2 | 0.3% |
| Number of different ethnic groups reported | Total | 44 | - |
Table 2.
Number and percentage of individuals who reported gastrointestinal illness symptom(s) during the health survey; overall, and by age class and gender.
Table 2.
Number and percentage of individuals who reported gastrointestinal illness symptom(s) during the health survey; overall, and by age class and gender.
| | Overall | (%) | <2 Years | (%) | <5 Years | (%) | 5–18 | (%) | 19–60 | (%) | 61+ | (%) |
|---|
| Diarrhoea 1 | 98 | 12.5 | 16 | 44.4 | 23 | 23.71 | 34 | 11.88 | 31 | 10.29 | 1 | 5.2 |
| Males | 41 | 41.8 | 7 | 43.7 | 11 | 47.8 | 12 | 35.3 | 11 | 35.5 | 1 | 100 |
| Females | 57 | 58.2 | 9 | 56.3 | 12 | 52.2 | 22 | 64.7 | 20 | 64.5 | 0 | 0 |
| Bloody diarrhoea | 9 | 1.14 | 1 | 2.78 | 2 | 2.06 | 5 | 1.74 | 1 | 0.33 | 0 | 0 |
| Males | 4 | 44.4 | 1 | 100 | 2 | 100 | 2 | 40.0 | 0 | 0 | - | - |
| Females | 5 | 55.6 | 0 | 0 | 0 | 0 | 3 | 60.0 | 1 | 100 | - | - |
| Stomach 2 cramps | 131 | 16.7 | 4 | 11.11 | 11 | 11.34 | 55 | 19.23 | 50 | 16.61 | 3 | 1.57 |
| Males | 44 | 33.6 | 1 | 25 | 5 | 45.5 | 16 | 29.1 | 14 | 28.0 | 1 | 33.3 |
| Females | 87 | 66.4 | 3 | 75 | 6 | 54.5 | 39 | 70.9 | 36 | 72.0 | 2 | 66.7 |
| Vomiting | 25 | 3.1 | 2 | 5.56 | 2 | 2.06 | 8 | 2.79 | 9 | 2.99 | 0 | 0 |
| Males | 14 | 56.0 | 1 | 50 | 1 | 50 | 5 | 62.5 | 4 | 44.4 | - | - |
| Females | 11 | 44.0 | 1 | 50 | 1 | 50 | 3 | 37.5 | 5 | 55.6 | - | - |
| Nausea | 34 | 4.3 | 0 | 0 | 0 | 0 | 13 | 4.54 | 17 | 5.64 | 0 | 0 |
| Males | 12 | 35.3 | - | - | - | - | 4 | 30.8 | 6 | 35.3 | - | - |
| Females | 22 | 64.7 | - | - | - | - | 9 | 69.2 | 11 | 64.7 | - | - |
| Fever 3 | 109 | 13.9 | 3 | 8.33 | 6 | 6.1 | 43 | 15.03 | 43 | 14.28 | 3 | 15.78 |
| Males | 58 | 53.2 | 3 | 100 | 6 | 100 | 22 | 51.2 | 19 | 44.2 | 2 | 66.7 |
| Females | 51 | 46.8 | 0 | 0 | 0 | 0 | 21 | 48.8 | 24 | 55.8 | 1 | 33.3 |
Reported gastrointestinal symptoms were higher for the younger age ranges: 55% of individuals 5–18 years (158/286) and 45% of individuals under the age of 5 years (44/97) reported to have had at least one GI symptom in the prior month. Over 16% percent (16/98) of individuals who had experienced diarrhoea were under the age of 2, despite this age group only making up only 5% of the overall population (36/705).
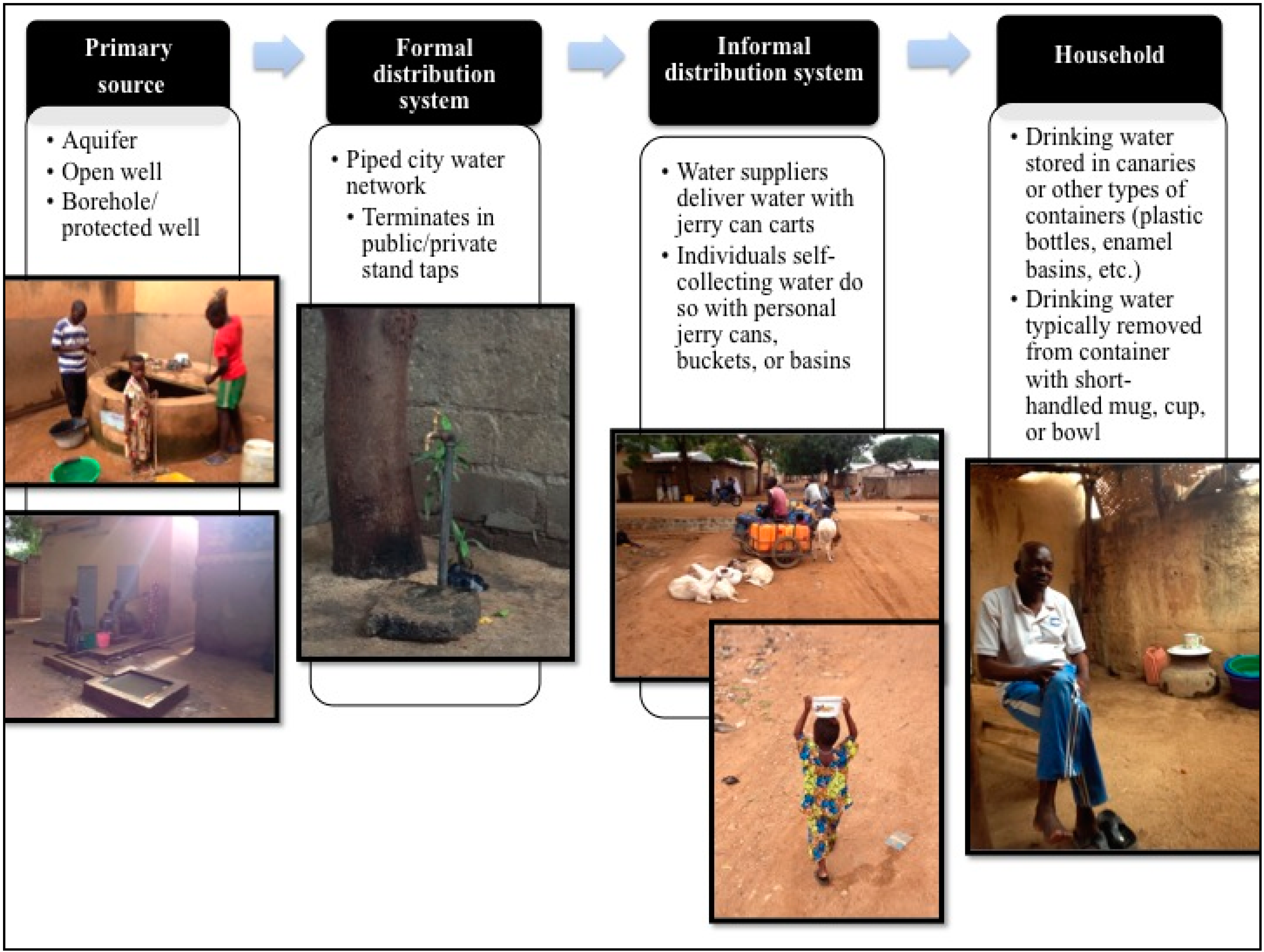
3.2. Sources and Storage of Drinking Water
Overall, 61% of surveyed households reported receiving their drinking water through a water supplier who transports water from a public tap or private water seller using plastic jerry cans loaded on a pull cart and delivers the water to their home; 20% had a private tap in their homes or compound; 13% bought their water from a neighbour using their own jerry cans; 3% regularly got their drinking water from a well; and 2% got their drinking water from a community borehole. Although a majority of households received their drinking water from a supplier, the supplier was not always available in order to obtain a sample from his jerry can. In these cases, the family directed us to the public tap source where their water supplier regularly obtained their water and a sample was taken from that tap. This resulted in the collection of 18 source samples directly from public/private taps, three from water suppliers’ jerry cans, three from open wells, and one from a borehole.
89% of households surveyed reported storing their drinking water at home in canaries. This included households with private taps within their compounds. Households who did not store their water in canaries generally used plastic bottles, buckets, and/or basins. 93% of households reported that they always or usually kept their drinking water storage containers (all types) covered. 73% said that they refilled the container every day, 22% at least every other day, and 1% every 3 or more days.
3.4. Reported Gastrointestinal Illness & Drinking Water Quality
Based on the results of the health survey, individuals were divided into four categories using GI symptoms in the prior 30 days: (1) non-case; (2) diarrhoea case (i.e., any individual who reported experiencing diarrhoea); (3) highly confirmed case of gastrointestinal illness with bloody diarrhoea (HCGI-BD; any individual who reported experiencing bloody diarrhoea, stomach cramps, and fever); or (4) highly confirmed case of gastrointestinal illness without bloody diarrhoea (HCGI-NBD; any individual who reported experiencing non-bloody diarrhoea, stomach cramps, and fever).
Table 4.
Microbial contamination found in water samples from stand tap water sources and all home storage containers.
Table 4.
Microbial contamination found in water samples from stand tap water sources and all home storage containers.
| Genetic Marker or Bacteria | Positive Source º | Positive Home ª | Total Positives |
|---|
| n (% Positive source samples) | n (% Positive home samples) | n (% Of total samples) |
|---|
| E. coli *,Υ | 9 (50) | 52 (87) | 61 (87) |
| tetQ ŧ | 5 (28) | 8 (13) | 13 (19) |
| S. aureus ŧ | 1 (6) | 12 (20) | 13 (19) |
| Campylocbacter ŧ | 1 (6) | 7 (12) | 8 (12) |
| HF183 ŧ | 1 (6) | 4 (7) | 5 (7) |
Spearman Rank-Order analyses were used to measure the relationship between the following home drinking water quality parameters: number of HF183 gene copies/100 mL; number of
tet Qgene copies/100 mL; and concentration of
E. coli CFU/100 mL.
tetQ had a statistically significant inverse relationship both with
E. coli levels (Rho = −0.31,
p = 0.001) and with HF183 (Rho = −0.11,
p = 0.003). Initial statistical analyses did not demonstrate a statistically significant relationship between
Campylobacter,
S. aureus and gastrointestinal illness, thus these parameters were not included in further analyses. Mann-Whitney U tests comparing
tetQ and
E. coli levels present in the HSC of cases and non-cases demonstrated a significant difference only in the average level of
tetQ for all three GI-illness categories (
Table 5).
Two rounds of odds ratios were then performed in order to further measure the association between drinking water quality at the point of use (
i.e., within
canaries) and reported gastrointestinal illness. The first round was performed on each of the following three classes (diarrhoea, HCGI-BD, and HCGI-NBD) and with the following drinking water quality parameters:
E. coli quartiles, presence of HF183, and presence of
tetQ. Simple presence/absence of
tetQ and HF183 genes copies were used in order to include all individuals who had any detectable amount of HF183 or
tetQ in their drinking water (
Table 6). Due to their non-normal distribution and in order to better view the risk associated with varying levels of potential faecal contamination, the
E. coli concentration measures were divided and reported as quartile values. Because diarrhoeal disease symptoms were more heavily reported among younger individuals, the odds ratios were adjusted for age.
Table 5.
Results of Mann-Whitney U tests of E. coli and tetQ concentrations between different types of gastrointestinal illness (diarrhoea, HCGI-BD, HCGI-NBD).
Table 5.
Results of Mann-Whitney U tests of E. coli and tetQ concentrations between different types of gastrointestinal illness (diarrhoea, HCGI-BD, HCGI-NBD).
| Gastrointestinal Illness Class (n = Cases/n = Non-Cases) 1 | Water Quality Parameter Medians & (
Means) | Cases | Non-Cases Y | p-Value |
|---|
| Diarrhoea 2 | tetQ (gene copies/100 mL) | 7.5 (547.9) | 7.5 (278.5) | 0.0032 * |
| (52/347) | E. coli (log CFU/100 mL) | 1.9 (2.0) | 2.2 (2.1) | 0.9405 |
| HCGI-BD 3 | tetQ (gene copies/100 mL | 2310.6 (2310.6) | 7.5 (307.2) | 0.0194 * |
| (1/398) | E. coli (log CFU/100 mL) | 1.11 (1.1) | 2.3 (2.1) | 0.2792 |
| HCGI-NBD 4 | tetQ (gene copies/100 mL | 7.5 (773.2) | 7.5 (290.5) | 0.0021 * |
| (18/381) | E. coli (log CFU/100 mL) | 1.6 (1.8) | 2.3 (2.1) | 0.2377 |
Table 6.
Adjusted odds ratios for diarrhoea, HCGI-BD & HCGI-NBD associated with various exposures levels to E. coli, HF183, or tetQ.
Table 6.
Adjusted odds ratios for diarrhoea, HCGI-BD & HCGI-NBD associated with various exposures levels to E. coli, HF183, or tetQ.
| Genetic Marker or E. coli Quartile (Range log CFU/100 mL) | Diarrhoea | HCGI with Bloody Diarrhoea | HCGI with Non-Bloody Diarrhoea |
|---|
| aOR 1 (95% CI) | (p) | aOR (95% CI) | (p) | aOR (95% CI) | (p) |
|---|
| E. coli Quartile † (0.30–1.23) ‡ | 1.15 (0.57–2.31) | 0.13 | N/A 2 | - | 1.62 (0.61–4.92) | 0.35 |
| E. coli Quartile (1.24–2.26) | 1.92 (0.93–3.42) | 0.05 | N/A | - | 1.72 (0.63–5.08) | 0.30 |
| E. coli Quartile (2.27–2.93) | 0.08 (0.93–3.42) | 0.05 | N/A | - | N/C | - |
| E. coli Quartile (2.92–3.38) | 1.43 (0.78–2.98) | 0.31 | N/A | - | 1.01 (0.32–3.22) | 0.95 |
| HF183 | 0.92 (0.16–3.18) | 0.91 | N/C 3 | - | 2.57 (0.5–12.07) | 0.21 |
| tetQ | 2.48 (1.3–5.16) | 0.01 * | N/A | - | 3.01 (1.02–8.89) | 0.04 * |
Guided by the results of the Spearman Rank-Order analysis (inverse relationship between
tetQ and
E. coli) and the results of the first round of odds ratio calculations (increased odds of reporting gastrointestinal illness with the presence of
tetQ in home drinking water), a second round of odds ratios was conducted using the same three case classes and placed them in four different water quality groups created based on the presence of
tetQ and varying
E. coli levels in HSC drinking water (
Table 7). The highest statistically significant odds ratios occurred between diarrhoea and NCGI-NBD cases that had
E. coli levels below the 1st quartile and
tetQ present in their drinking water. Because few individuals reported having bloody diarrhoea, odds ratios for this case class could not be calculated. Interestingly, even when
tetQ was present in the water, as the level of
E. coli contamination increased above the first quartile, no cases of HCGI-NBD were observed.
Table 7.
Adjusted odds ratios for diarrhoea, HCGI-BD & HCGI-NBD associated with microbial quality groups.
Table 7.
Adjusted odds ratios for diarrhoea, HCGI-BD & HCGI-NBD associated with microbial quality groups.
| Microbial Quality Group | Diarrhoea | HCGI-BD | HCGI-NBD |
|---|
| aOR 1 (95% CI) | (p) | aOR (95% CI) | (p) | aOR (95% CI) | (p) |
|---|
| Group 1 (tetQ & 1st Quartile E. coli) † | 2.95 (1.35–6.45) | 0.005 * | N/A 2 | - | 5.31 (1.72–16.35) | 0.001 * |
| Group 2 (tetQ & 2nd Quartile E. coli) | 2.06 (0.43–9.76) | 0.248 | N/C | - | N/C | - |
| Group 3 (tetQ & 3rd Quartile E. coli) | 0.48 (0.03–7.27) | 0.588 | N/C | - | N/C | - |
| Group 4 (tetQ & 4th Quartile E. coli) | N/C 3 | - | N/C | - | N/C | - |
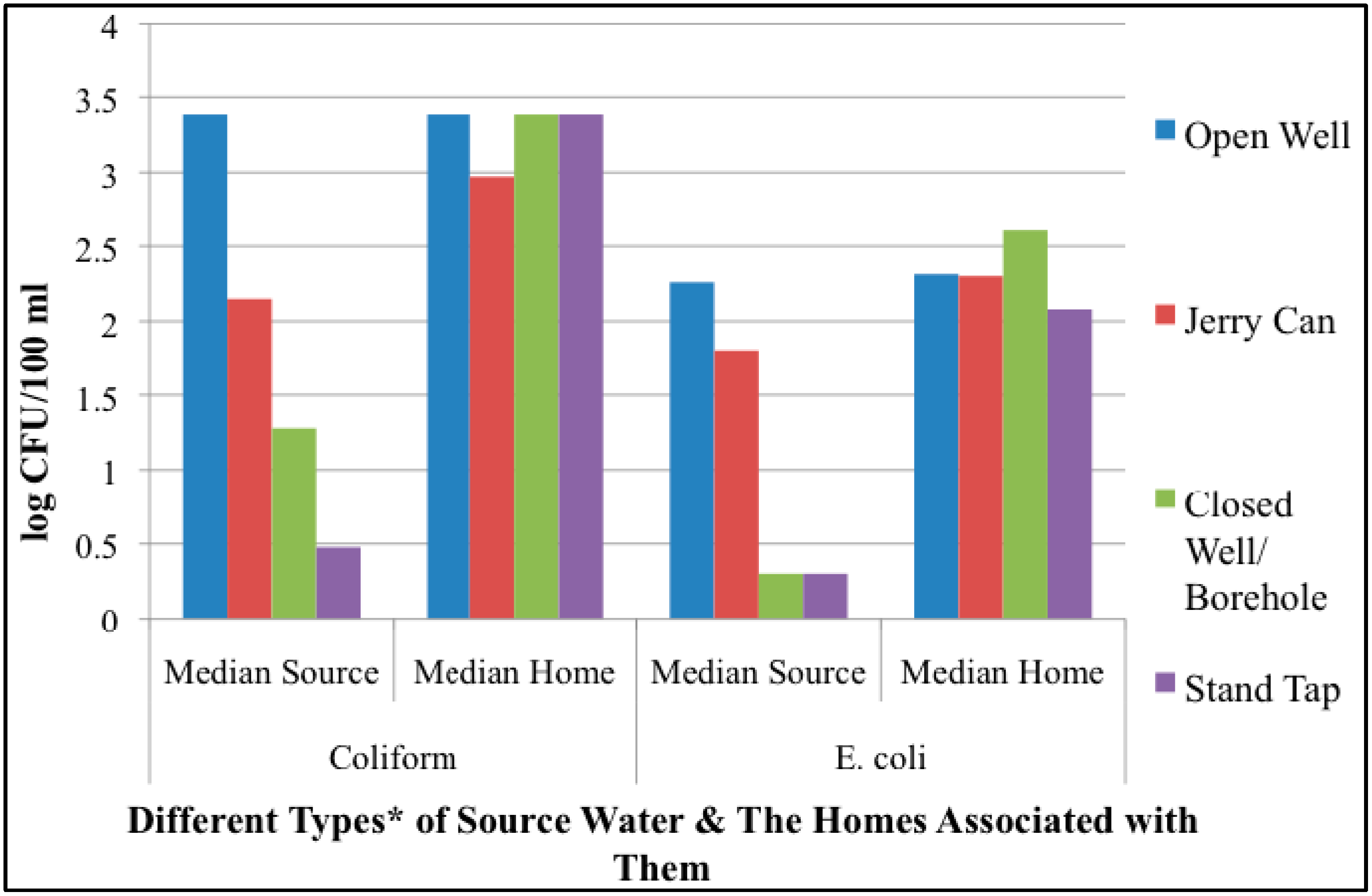
3.5. Discussion
The results from this study suggest that the greatest bacterial contamination of drinking water in the city of Maroua occurs within the household and that improvements of the originating source water quality deteriorate once the drinking water moves through the distribution system and is stored in the household. Despite the fact that a majority of the study population received their water from improved sources, 87% of drinking water samples taken from HSC surpassed the WHO’s “no action required” threshold for
E. coli in drinking water. The
tetQ positive samples also confirm that tetracycline-resistant bacteria are present within the study area, a steadily increasing trend in the developed and developing world [
22,
23].
tetQ had an interesting relationship between
E. coli levels in HSC and this relationship provided a more demonstrable association with reported diarrhoeal disease than
E. coli levels alone. This finding implies that adding additional screening factors, such as detection of antibacterial resistance genes, may provide improved assessment of the diarrhoeal risk associated with a drinking water source especially in tropical and semi-tropical regions of the world, like Maroua, where the traditional faecal indicators may not be as effective signalers of potential faecal contamination due to increased persistence of environmental presence [
35,
36,
37].
This
tetQ-
E. coli relationship suggests that the growing problem of antibiotic resistant bacteria adds a new dimension to the kind of drinking water contamination that can occur. Antibiotic use is often uncontrolled in developing countries [
38,
39,
40,
41] leading to great concern as the number of organisms resistant to multiple types of antibiotics grows and is present in the greater environment. A study in Nepal demonstrated that even communal exposure to antibiotics increased the number of antibiotic resistant pathogens within an individual’s faeces [
42]. In addition, animal studies have demonstrated that antibiotic use can lower the infectious dose of certain pathogens [
43].
The presence of
tetQ and of HF183 in drinking water is an interesting finding for two reasons. First, both genetic markers confirm that there is human faecal contamination (and/or possibly livestock in the case of
tetQ) occurring within areas where drinking water is accessed and utilized in our study area. In addition, the near equal HF183 positive detection (
Table 4) percentage among home and source samples and the higher
tetQ positive detection in sources samples suggest that this specific type of contamination is coming from the greater environment and/or in addition to within the home.
tetQ and HF183 were not found together in any of the samples, suggesting that
tetQ genes could be potentially coming from non-human sources (
i.e., livestock) within the environment. The detection of
Campylobacter spp. also supports the possibility that contamination is coming from livestock or wildlife within the home and within the areas where drinking water is collected. In the urban environment of Maroua, livestock density is relatively high (specifically goats, sheep, and poultry) and animals mingle freely within homes, on the streets and frequently congregate near public stand taps (
Figure 1). Lizards and birds are also common within household compounds.
Second, tetQ was detected in source samples at more than twice the positive percentage found in HSC samples, suggesting that tetracycline-resistant bacteria are present within the city distribution system (from either human or livestock sources) despite chlorinated water treatment. It is possible that the bacteria with this resistance are less susceptible to disinfection or that they are being introduced at the point of collection and there is not sufficient residual chlorination remaining to kill them.
The inverse relationship between
tetQ and
E. coli within
canaries, in addition to the results of the second round of odds ratios, suggests that there may be an interaction between antibiotic-resistant bacteria and
E. coli within drinking water that has a relationship to gastrointestinal illness. While the study design did not allow for identification of which bacteria were in the water when individuals became ill, the cause of the diarrheal illness, or if individuals were currently taking antibiotics (
i.e., tetracycline), it seems that in our study area that tetracycline usage has caused an additional environmental risk factor to drinking water quality. And while there are some inherent limitations to using qPCR, namely lack of discrimination between viable and non-viable organisms and the potential for false detection within a mixed microbial community, the results of this study strengthen the suggestion that there may be a link between genetic determinants of antibiotic resistance and virulence such that fewer bacteria are necessary to create disease when resistance genes are present [
44].





{kind=link}
{kind=link}
{kind=link}
