Healthy Food Procurement Policies and Their Impact


Abstract
:1. Introduction
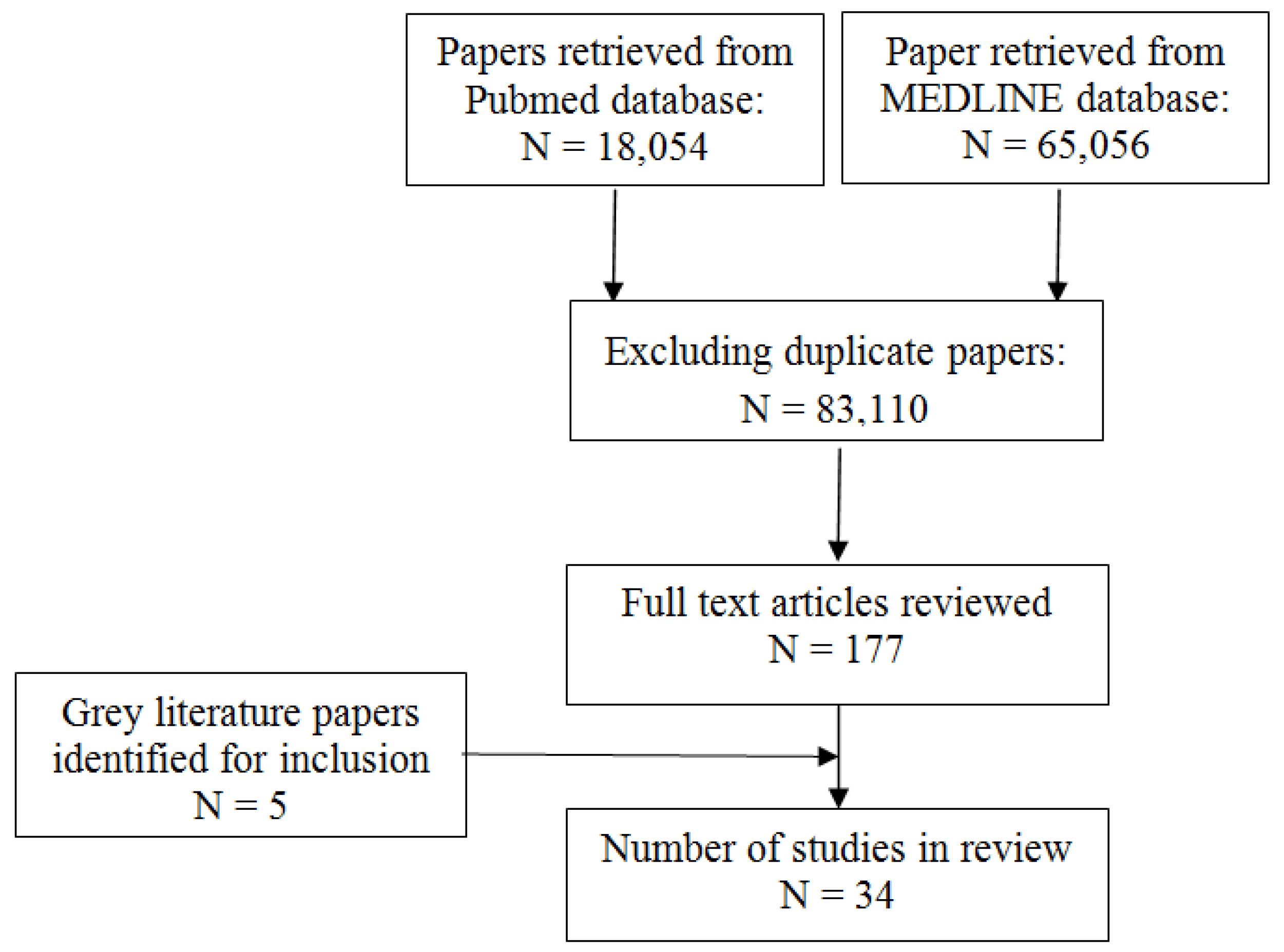
2. Experimental Section
3. Results and Discussion
3.1. Interventions in Schools


{kind=link}
| Study and Year | Study Description | Intervention(s) | Post-intervention Outcome(s)
and Notable Findings |
|---|---|---|---|
| School Food Trust 2009 [28] | At 136 primary schools in England, dietary intake was assessed and compared with 2005 survey results. | Increased provision of healthy foods and decreased the availability of foods high in sodium, fat, and sugar. | Consistent benefits from 2005 to 2009 and included decreased sugar, fat, and saturated fat intake. Further, these lunches in 2009 contained almost one-third less sodium compared with 2005. |
| School Food Trust 2011 [31] | At 80 secondary schools in England, dietary intake was assessed and compared with 2004 results [32]. | Increase provision of healthy foods and decreased the availability of unhealthy foods high in sodium, fat, and sugar. | The average meal contained >30% less saturated fat, total fat, sodium and sugar and 50% more vitamin A than in 2004 and there was a 6% increase in F&V intake since then. |
| School Food Trust 2004 [32] | At 79 secondary schools in England, dietary intake was assessed. | Improved the nutritional quality of foods served in the schools and performed surveys. | On average, the intervention reduced dietary total fat, saturated fat, sugar, sodium, and energy intake by 27%, 23%, 37%, 18%, and 16%, respectively, in the schools. Survey results were with 2011 results [31]. |
| Joshi et al. 2005 [33] | This report showcases innovative farm to school programs from around the USA to include eight case studies. | Predominantly provision of fresh foods from local farms along with education though innovative strategies are detailed. | Results varied with each state’s intervention(s). In California, 65% of students chose healthier menu items over meals high in fat, sugar and sodium and increased intake of F&V by 58%. There were an estimated 950 “Fresh” programs in the USA by 2006. |
| Simons-Morton et al. 1991 [38] | Four elementary schools for K-4th grade students in Texas (USA) with two being controls evaluated the impact of a school-based program on improving diet and physical activity. | The three intervention components were classroom education (Go For Health Curriculum), physical activity (Children’s Active Physical Education), and low fat/low sodium school lunches (New School Lunch). | The two intervention schools had decreased total fat (15.5%; 10.4%), saturated fat (31.7%; 18.8%), and sodium (40.3%; 53.6%). Physical activity increased from less than 10% class time to 40% of class time. Adoption of such programs in other schools may be a challenge. |
| Ellison et al. 1989 [39] | Food service workers ate two high schools in Massachusetts and New Hampshire modified preparation of foods served at dining halls. | Increased availability of healthier food through the food service providers and assessed in all students taking a science course. | Reduced sodium intake by 15%–20% and saturated fat intake by 20%. The lower sodium intake over a school year resulted in lower blood pressure among students receiving the intervention. Intervention was well received by workers and students. |
| Jeffrey et al. 1994 [40] | Cafeteria at a university office building housing 700 employees in Minnesota (USA). | Increased availability and reduced price of fruit and salads in a school cafeteria and assessed by daily sales. | Three-fold increase in the sale of fruit and salad after reducing the price by 50% over a 3-wk period. Women were more prone to make more nutritious purchases. |
| French et al. 2001 [41] (Also in Table 2) | Examined the impact of pricing and promotion of low-fat snacks in vending machines at 12 worksites and 12 schools in Minnesota (USA) over a 12-month period. | Low-fat snacks added to 55 vending machines were subject to four pricing conditions and three promotional conditions and sales were tracked. | Price reductions of 10%, 25%, and 50% were associated with significant increases in sales of low-fat snacks in adults and adolescents. Profits per vending machine were not impacted and promotional signage may have had slight effect. |
| Saksvig et al. 2005 [42] | Ojibway-Cree First Nations 3rd, 4th and 5th grades students with school-based program delivered at the Sandy Lake School in northern Canada assessed at baseline and one year later at follow-up. | Culturally appropriate diabetes prevention program that banned high-fat and high-sugar snack foods and provided a healthier lunch. Included education on diet and physical activity with community support. | This program was associated with improved dietary knowledge, dietary self-efficacy, and understanding of the psychosocial factors related to healthy eating and dietary fiber intake of students in a remote First Nations community. The intake of energy from total fat decreased significantly by 2% after one year. |
| Auld et al. 1998 [43] | Comprehensive, 4-yr program in three Denver, CO (USA) elementary schools aimed at increasing consumption of whole grains, F&V with nutrition education. | Integrated Nutrition Project included 24 weekly hands-on, teacher led activities; six parent-taught lunchroom mini-lesson. | Students in treatment classrooms achieved significantly greater gains in knowledge and self-efficacy on food preparation and F&V consumption. Integrated approach with education and healthy food procurement may increase desire for healthier foods. |
| French et al. 2004 [44] | 20 secondary schools in Minnesota participated over two years with a portion serving as controls. | Environmental intervention in school cafeterias where they increased availability of lower fat foods and implemented student-based promotions. | There was a significant increase (35%) in the sales of lower-fat foods in the intervention group and a significant increase in lower-fat foods in the al a carte product mix. |
| Perry et al. 1998 [45] | 20 primary schools in Minnesota used a multi-component approach to increase F&V consumption in 4th/5th grade students over a 2 year period. | The 5-a-Day Power Plus Program included behavioral curricula in the classroom, parental involvement, school food changes, and industry involvement. | The program significantly increased lunchtime F&V consumption; fruit consumption; vegetable consumption among girls. |
| Perry et al. 2004 [46] | The project was performed at 26 elementary schools (grades 1–4) in Minnesota (USA) over two consecutive school years. | The Cafeteria Power Plus project sought to increase the daily availability, attractiveness, and encouragement for F&V with kick-offs, samplings, and challenge weeks. Training of food-service staff and cook managers was ongoing. | Students in the intervention schools significantly increased their total fruit intake. Process measures indicated that verbal encouragement by food-service staff was associated with outcomes. The outcomes suggest that multicomponent interventions are more powerful than cafeteria programs alone with this age group. |
| Lytle et al. 2006 [47] | As part of the TEENS study, 16 middle schools in Minnesota (USA) with approximately 3,600 students in the eight intervention schools were exposed to a multi-component intervention from 1997–2000. | The TEENS intervention included classroom-based curricula, family newsletters, and changes in the school food environment including increasing more healthful options on a la carte and on the school lunch line top increase the availability of F&V and lower fat foods in homes and schools. | Parents of students in intervention schools reported making significantly more healthy food choices when shopping than parents of students in control schools. Compared to control schools, intervention schools offered (p = 0.04) and sold (p = 0.07) a significantly higher proportion of healthier foods on a la carte. |
| Reynolds et al. 2000 [48] | 28 elementary schools in Alabama (USA) assessed the effects of a dietary intervention program in 4th graders over two years based on diet and psychosocial variables. | The High 5 project included classroom, parent, and cafeteria intervention components that increased availability of F&V in alliance with education. | F&V consumption was significantly higher in the intervention group children at follow-up one and two when compared to children in the control group. F&V consumption by parents in the intervention group was significantly higher at follow-up one when compared to control parents. |
| Osganian et al. 1996 [49] | The CATCH Eat Smart Program was implemented at 56 schools in four states over 2.5 years and assessed school menu, recipe, and vendor product information on five consecutive days on three occasions. | Targeted school food service staff through education on making positive changes in the nutrient quality of school meals and base them on national dietary goals to lower the total fat, saturated fat, and sodium content of school meals. | There was a significantly greater mean reduction in the calories from total fat and saturated fat in intervention compared with control school from baseline to follow-up.
Though total caloric consumption decreased by 683kcal n the intervention group it was still one-third above the Recommended Dietary Allowances for this age group. |
| Bartholomew & Jowers. 2006 [50] | Two elementary schools of similar size and demographic data in Texas (USA) were used for a two-phase study evaluating an intervention to increase selection of low- and moderate- fat entrees over two semesters. | In Phase 1, the rotation of existing entrees was modified such that one of three entree choices was low or moderate in fat. In Phase 2, the number of competing high-fat entrees was reduced from two choices to one. | In Phase 1 in the intervention school, the number of days that a low-fat entree was offered increased by
70%, with no increase in the rate of selection of the lower moderate-fat entrees. In Phase 2, both low- and moderate-fat entrees were selected at a significantly higher rate in the intervention school (32.1% and 26.4%, respectively) than the control school (13.8% and 7.5%, respectively). |
| Belansky et al. 2010 [51] | The project surveyed 45 low-income, rural elementary schools in Colorado one year before and after a healthy eating, wellness policy mandated in 2006. | The What’s Working project described the influence of a mandated Local Wellness Policy (LWP) to identify impacts, opportunities, and barriers. | Three improvements were associated with the new policy, namely: increased percentage of schools with policies stipulating healthy items be offered in classroom parties (21.4% in 2005 vs. 48.7% in 2007), daily fresh fruit be offered in lunchrooms (0.80 choices in 2005 vs. 1.15 choices in 2007), and skinless poultry be used (27% in 2005 vs. 59% in 2007). |
| Anderson et al. 2005 [52] | Investigated the impact of a school-wide nutrition education program in primary schools in Scotland at baseline and 9 months. Dietary and attitude assessments of children aged 6–7 and 10–11 were performed. | Increased provision of F&V and provided point-of-purchase marketing materials, education materials, newsletters, and teacher information. | Children in the two intervention schools had a significantly higher average increase in fruit consumption than those in two control schools. No other changes in nutrient uptake were detected. |
3.2. Interventions in Worksites
| Study and Year | Study Description | Intervention(s) | Post-intervention Outcome(s)
and Notable Findings |
|---|---|---|---|
| Lassen et al. 2004 [55] | Five worksites in Denmark with canteens promoted healthier lunches with an end point and follow up data collection. | Implemented a continuous quality improvement of canteen lunches through a spectrum of strategies to include increased availability of healthy foods, staff training, goal setting, and support groups. | On average across the five sites there was 70g /day/customer increase in the intake of F&V intake at endpoint and a 95 g/day/customer increase four months after endpoint. |
| Beresford et al. 2001 [56] | Targeted 28 Seattle, WA (USA) worksites with cafeterias in Seattle to increase F&V intake assessed at baseline and two-year follow-up. | Seattle “5 a Day for Better Health” is a simple message encouraging people to eat more F&V which was launched at 14 intervention worksites and compared with 14 control worksites. | Significantly higher intake of F&V in the intervention group after two years with 0.3 more servings than the control group. |
| Sorensen et al. 1999 [57] | 22 Community Health Centers in Massachusetts (USA) implemented the Treatwell 5-a-day project to get participants to consume >five F&V servings per day. | The program incorporated three interventions, namely minimal intervention, worksite intervention, and worksite plus family intervention which included education components. | Total intake increased by 19% in worksite plus family group, 7% in worksite group, and 0% in minimal intervention group. Only 23% of all participants reported consuming more than five servings per day. Consumption of F&V was directly associated with level of household support for healthy eating. |
| Sorensen et al. 1998 [58] | 24 manufacturing worksites in Massachusetts (USA) assessed the impact of an integrated health promotion effort. | Implemented three intervention components: joint worker-management participation in program planning and implementation, consultation with management on worksite environment, and health education. | The intervention group had a reduced intake of calories consumed as fat (2.3% vs. 1.5% in control) and increased intake of F&V (10% vs. 4% in control. |
| French et al. 2001 [41] (Also in Table 1) | Examined the impact of pricing and promotion of low-fat snacks in vending machines at 12 worksites and 12 in Minnesota (USA). | Low-fat snacks added to 55 vending machines were subject to four pricing conditions and three promotional conditions. Sales and profits were tracked over a 12-month period. | Price reductions of 10%, 25%, and 50% were associated with significant increases in sales of low-fat snacks in adults and adolescents. Profits per vending machine were not impacted and promotional signage may have had slight effect. |
| Perlmutter et al. 1997 [59] | Assessed acceptance of more healthful entrees in a Kansas (USA) worksite cafeteria that services est. 200 employees per day based on sales data, nutrient analysis, customer acceptability. | Five phase study modified entrees over a 7-month period to include less than 30% energy from fat and less than 1,000 mg sodium per serving. A marketing component identified healthier food offerings. | No significant difference in sales was observed though customers may be more willing to accept changes in flavor attributes when they are identified as healthful and include nutrient information. |
3.3. Interventions in Hospitals, Care Homes, Correctional Facilities, Government Institutions and Miscellaneous Settings
| Study and Year | Study Description | Intervention(s) | Post-intervention Outcome(s) and Notable Findings |
|---|---|---|---|
| L’Abbé et al. 2011 [26] | Comprehensive review on existing healthy food procurement policies and programs. | Details multiple programs and their interventions on healthy food procurement initiatives. | Numerous successful food procurement programs in Canada and Internationally are described to include criteria (such as sodium limits) for healthy foods and recommendations for a healthy food procurement framework in Canada. |
| CDC 2012 [27] | 28 correctional facilities across Indiana (USA). | Implemented new menu with 20% less sodium than the previous diet. | Successfully launched healthier food menu statewide. Menu also increased servings of fruit in place of baked desserts, averaging at least five servings of F&V per day. To help lower cholesterol, the menu also serves no fried foods and fewer high-fat menu items. |
| Geaney et al. 2011 [60] | Two public hospitals in Ireland and monitored food and nutrient intake monitored for participants aged 18–64 in their canteen. | One of the two hospitals implemented a catering initiative designed to provide nutritious foods while reducing sugar, fat, and salt intakes in their canteen. | Mean intakes of total sugars, total fat, saturated fat, and salt were significantly lower in the intervention hospital where 72% of respondents, compared with 42% in the control, complied with the recommended under-3 daily servings of food high in fat and sugar. In the intervention hospital, 43% of respondents exceeded the recommended salt intake of 4–6 g/day, compared with 57% in the control. |
| Johnson et al. 2004 [62] | 480 homebound, low-income seniors receiving Meals on Wheels over 4 months in Seattle, WA (USA) | Increased access to fresh F&V via home delivery. | Seniors receiving baskets consumed 1.04 more servings than those in the control group. The number of seniors consuming >five servings per day increased by 17% from baseline. |
| Vander Wekken & Naylor 2010 [63] | 48 local governments in British Columbia, Canada, including 12 First Nations addressed food environments in 142 community funded facilities. | Evaluated food and beverage framework in local recreational settings during 2008–2010. | The initiative was successful at facilitating changes in policy, practices, food provision, and patron awareness. Key factors for change and challenges to implementation were identified. |
| PSFPI 2009 [64] | Comprehensive initiative for food public institutions such as schools, hospitals, and prisons in the United Kingdom. | Developed and disseminated the PSFPI report to encourage consumption of locally grown foods and availability of healthy foods and build momentum for progress. | Awareness of the program increased by 24% in 2 years; 72% of local authorities and 69% of schools supported initiative; 54% of users find the guidelines very useful or extremely useful; constraints were identified. |
3.4. Interventions in Remote Communities
3.5. Discussion
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Morgan, K.; Sonnino, R. Empowering consumers: The creative procurement of school meals in Italy and the UK. Int. J. Const. Stud. 2006, 1–7. [Google Scholar]
- Webster, J.L.; Dunford, E.K.; Hawkes, C.; Neal, B.C. Salt reduction initiatives around the world. J. Hypertens. 2011, 29, 1043–1050. [Google Scholar] [CrossRef]
- He, F.J.; MacGregor, G. A comprehensive review on salt and health and current experience of worldwide salt reduction programmes. J. Hum. Hypertens. 2009, 23, 363–384. [Google Scholar] [CrossRef]
- Cutler, J.A.; Follmann, D.; Alexander, P.S. Randomized trials of sodium reduction: An overview. Amer. J. Clin. Nutr. 1997, 65, S643–S651. [Google Scholar]
- Cook, N.R.; Cutler, J.A.; Obarzanek, E.; Buring, J.E.; Rexrode, K.M.; Kumanyika, S.K.; Appel, L.J.; Whelton, P.K. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: Observational follow-up of the trials of hypertension prevention (TOHP). Brit. Med. J. 2007, 334, S885–S888. [Google Scholar] [CrossRef]
- CDC Grand Rounds: Dietary Sodium Reduction—Time for Choice, Centers for Disease Control and Prevention. Available online: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6105a2.htm (accessed on 21 February 2014).
- Otsuka, R.; Kato, Y.; Imai, T.; Ando, F.; Shimokata, H. Decreased salt intake in Japanese men aged 40 to 70 years and women aged 70 to 79 years: An 8-year longitudinal study. J. Amer. Diet. Assn. 2011, 111, 844–850. [Google Scholar] [CrossRef]
- Millett, C.; Laverty, A.A.; Stylianou, N.; Bibbins-Domingo, K.; Pape, U.J. Impacts of a national strategy to reduce population salt intake in England: Serial cross sectional study. PLoS Clin. Trials 2012, 7, S1–S7. [Google Scholar]
- He, F.J.; Appel, L.J.; Cappuccio, F.P.; de Wardener, H.E.; MacGregor, G.A. Does reducing salt intake increase cardiovascular mortality? Kidney Int. 2011, 80, 696–698. [Google Scholar] [CrossRef]
- He, F.J.; Jenner, K.H.; Farrand, C.E.; MacGregor, G.A. World salt awareness week. J. Clin. Hypertens. 2011, 13, S141–S145. [Google Scholar] [CrossRef]
- He, F.J.; Jenner, K.H.; MacGregor, G.A. WASH—World action on salt and health. Kidney Int. 2010, 78, 745–753. [Google Scholar] [CrossRef]
- Woodward, E.; Eyles, H.; Mhurchu, C.N. Key opportunities for sodium reduction in New Zealand processed foods. Aust. N. Z. J. Public Health 2012, 36, 84–89. [Google Scholar] [CrossRef]
- Dotsch-Klerk, M.; Jansen, L. The Choices programme: A simple, front of pack stamp making healthy choices easy. Asia Pac. J. Clin. Nutr. 2008, 17, S383–S386. [Google Scholar]
- Conseil de la Transformation Agroalimentaire et des Produits des Consummation (CTAC) Reformulation of Products to Reduce Sodium: Salt Reduction Guide for the Food Industry; (in French). CTAC: Quebec, Canada, 2009; pp. 1–76.
- Fischer, P.W.F.; Vigneault, M.; Huang, R.; Arvaniti, K.; Roach, P. Sodium food sources in the Canadian diet. Appl. Physiol. Nutr. Metab. 2009, 34, 884–892. [Google Scholar] [CrossRef]
- Hutchinson, H.; L’Abbé, M.R.; Campbell, N.R.; Tanaka, P. Sodium Working Group: Sodium Reduction Strategy for Canada; Authority of the Minister of Health: Ottawa, ON, Canada, 2010; pp. 1–61. [Google Scholar]
- Penz, E.D.; Joffres, M.R.; Campbell, N.R. Reducing dietary sodium and decreases in cardiovascular disease in Canada. Can. J. Cardiol. 2008, 24, S497–S501. [Google Scholar] [CrossRef]
- World Health Organization Global Strategy on Diet, Physical Activity, and Health, Eighth Plenary Meeting—Committee A, Third Report; World Health Organization: Geneva, Switzerland, 2004; pp. 1–19.
- Tracking Heart Disease and Stroke in Canada; Public Health Agency of Canada, Heart and Stroke Foundation of Canada: Ottawa, ON, Canada, 2009; pp. 1–115.
- Sodium Kills 30 Canadians Every Day; Canadian Stroke Network: Ottawa, ON, Canada, 2007; Volume 7, pp. 1–16.
- Van Vliet, B.; Campbell, N.R.C. Efforts to reduce sodium intake in Canada: Why, what, and when? Can. J. Cardiol. 2011, 27, S437–S445. [Google Scholar] [CrossRef]
- Joffres, M.R.; Campbell, N.R.; Manns, B.; Tu, K. Estimate of the benefits of a population-based reduction in dietary sodium additives on hypertension and its related health care costs in Canada. Can. J. Cardiol. 2007, 23, 437–443. [Google Scholar] [CrossRef]
- Reducing the Sodium Intake of Canadians: A Provincial and Territorial Report on Progress and Recommendations for Future Action; Conference of Health Ministers: Ottawa, ON, Canada; pp. 1–40.
- Improving the Food Environment through Nutrition Standards: A Guide for Government Procurement; National Center for Chronic Disease Prevention and Health Promotion, Centre for Disease Control: Atlanta, GA, USA, 2011; pp. 1–24.
- Story, M.; Kaphingst, K.M.; Robinson-O’Brien, R.; Glanz, K. Creating healthy food and eating environments: Policy and environmental approaches. Annu. Rev. Public Health 2008, 29, 253–272. [Google Scholar] [CrossRef]
- L’Abbé, M.; Sunohara, D.; Wan, J. Environmental Scan of Public Food proCurement Policies Related to Sodium; Public Health Agency of Canada: Ottawa, ON, Canada, 2011; pp. 1–93. [Google Scholar]
- Under Pressure: Strategies for Sodium Reduction in Institutionalized Environments. Available online: http://www.cdc.gov/salt/pdfs/Institutional_Sodium_Reduction_Guide.pdf (accessed on 27 May 2012).
- School Food Trust: Eat Better Do Better. Research Report: Primary School Food Survey; England Department of Education: London, UK, 2009; pp. 1–11.
- UK Target Nutrient Specifications (TNS) For Manufactured Products Used In School Meals. 2005. Available online: http://www.food.gov.uk/multimedia/pdfs/tnssummary.pdf (accessed on 4 June 2012).
- Food and Catering Services Specifications. Available online: http://sd.defra.gov.uk/advice/public/buying/products/food/ (accessed on 7 June 2012).
- School Food Trust: Eat Better Do Better. Research Report: Secondary School Food Survey; England Department of Education: London, UK, 2011; pp. 1–27.
- Modeling Compositional Changes in School Meals—Further Analysis of the 2004 Survey: School Meals in Secondary Schools in England. Available online: http://www.food.gov.uk/multimedia/pdfs/modellingchanges.pdf (accessed on 21 February 2014).
- Joshi, A.; Kalb, M.; Beery, M. Going Local: Paths to Success for Farm to School Programs. Available online: http://departments.oxy.edu/uepi/cfj/publications/goinglocal.pdf (accessed on 17 May 2012).
- Schools Food Sales and Policies Provincial Report II. Available online: http://www.bced.gov.bc.ca/health/sales_policy_feb08.pdf (accessed on 15 July 2012).
- Understanding Healthy Procurement: Using Government’s Purchasing Power to Increase Access to Healthy Food; National Policy and Legal Analysis Network to Prevent Childhood Obesity: Oakland, CA, USA, 2011; pp. 1–18.
- Gase, L.N.; Kuo, T.; Dunet, D.; Schmidt, S.M.; Simon, P.A.; Fielding, J.E. Estimating the potential health impact and costs of implementing a local policy for food procurement to reduce the consumption of sodium in the county of Los Angeles. Amer. J. Pub. Health 2011, 101, S1501–S1507. [Google Scholar] [CrossRef]
- Samuels, S.E.; Bullock, S.L.; Woodward-Lopez, G.; Clark, S.E.; Kao, J.; Craypo, L.; Barry, J.; Crawford, P.B. To what extent have high schools in California been able to implement state-mandated nutrition standards? J. Adolescent Health 2009, 45, S38–S44. [Google Scholar]
- Simons-Morton, B.G.; Parcel, G.S.; Baranowski, T.; Forthofer, R.; O’Hara, N.M. Promoting physical activity and a healthful diet among children: Results of a school-based intervention study. Amer. J. Public Health 1991, 81, S986–S991. [Google Scholar] [CrossRef]
- Ellison, R.C.; Capper, A.L.; Goldberg, R.J.; Witschi, J.C.; Stare, F.J. The environmental component: Changing school food service to promote cardiovascular health. Health Educ. Quart. 1989, 16, S285–S297. [Google Scholar] [CrossRef]
- Jeffery, R.W.; French, S.A.; Raether, C.; Baxter, J.E. An environmental intervention to increase fruit and salad purchases in a cafeteria. Prev. Med. 1994, 23, S788–S792. [Google Scholar] [CrossRef]
- French, S.A.; Jeffrey, R.W.; Story, M.; Breitlow, K.K.; Baxter, J.S.; Hannan, P.; Snyder, M.P. Pricing and promotion effects on low fat vending snack purchases: The CHIPS Study. Amer. J. Public Health 2001, 91, 112–117. [Google Scholar] [CrossRef]
- Saksvig, B.I.; Gittelsohn, J.; Harris, S.B.; Hanley, A.J.G.; Valente, T.W.; Zinman, B. A pilot school-based healthy eating and physical activity intervention improves diet, food knowledge, and self-efficacy for native Canadian children. J. Nutr. 2005, 135, S2392–S2398. [Google Scholar]
- Auld, G.W.; Romaniello, C.; Heimendinger, J.; Hambidge, C.; Hambidge, M. Outcomes from a school-based nutrition education program using resource teachers and cross-disciplinary models. J. Nutr. Educ. 1998, 30, S268–S280. [Google Scholar] [CrossRef]
- French, S.A.; Story, M.; Fulkerson, J.A.; Hannan, P. An environmental intervention to promote lower-fat food choices in secondary schools: outcomes of the TACOS Study. Amer. J. Public Health 2004, 94, S1507–S1512. [Google Scholar] [CrossRef]
- Perry, C.L.; Bishop, D.B.; Taylor, G.; Murray, D.M.; Mays, R.W.; Dudovitz, B.S.; Smyth, M.; Story, M. Changing fruit and vegetable consumption among children: The 5-a-day power plus program in St. Paul, Minnesota. Amer. J. Public Health 1998, 88, S603–S609. [Google Scholar] [CrossRef]
- Perry, C.L.; Bishop, D.B.; Taylor, G.L.; Davis, M.; Story, M.; Gray, C.; Bishop, S.C.; May, R.A.W.; Lytle, L.A.; Harnack, L. A randomized school trial of environmental strategies to encourage fruit and vegetable consumption among children. Health Educ. Behav. 2004, 31, S65–S76. [Google Scholar] [CrossRef]
- Lytle, L.A.; Kubik, M.Y.; Perry, C.; Story, M.; Birnbaum, A.S.; Murray, D.M. Influencing healthful food choices in school and home environments: Results from the TEENS study. Prev. Med. 2006, 43, 8–13. [Google Scholar] [CrossRef]
- Reynolds, K.D.; Franklin, F.A.; Binkley, D.; Raczynski, J.M.; Harrington, K.F.; Kirk, K.A.; Person, S. Increasing the fruit and vegetable consumption of fourth-graders: Results from the high 5 project. Prev. Med. 2000, 30, S309–S319. [Google Scholar] [CrossRef]
- Osganian, S.K.; Ebzery, M.K.; Montgomery, D.H.; Nicklas, T.A.; Evans, M.A.; Mitchell, P.D.; Lytle, L.A.; Snyder, M.P.; Stone, E.J.; Zive, M.M.; et al. Changes in the nutrient content of school lunches: Results from the CATCH eat smart food service intervention. Prev. Med. 1996, 25, S400–S412. [Google Scholar] [CrossRef]
- Bartholomew, J.B.; Jowers, E.M. Increasing frequency of lower-fat entrees offered at school lunch: An environmental change strategy to increase healthful selections. J. Amer. Diet. Assn. 2006, 106, S248–S252. [Google Scholar] [CrossRef]
- Belansky, E.S.; Cutforth, N.; Delong, E.; Litt, J.; Gilbert, L.; Scarbro, S.; Beatty, B.; Romaniello, C.; Brink, L.; Marshall, J.A. Early effects of the federally mandated local wellness policy on school nutrition environments appear modest in colorado’s rural, low-income elementary schools. J. Amer. Diet. Assn. 2010, 110, 1712–1717. [Google Scholar] [CrossRef]
- Anderson, A.S.; Porteous, L.E.G.; Foster, E.; Higgins, C.; Stead, M.; Hetherington, M.; Ha, M-A.; Adamson, A.J. The impact of a school-based nutrition education intervention on dietary intake and cognitive and attitudinal variables relating to fruits and vegetables. Public Health Nutr. 2005, 8, S650–S656. [Google Scholar]
- Recommended Nutrition Standards for Procurement of Foods and Beverages Offered in the Workplace; American Heart Association: Dallas, TX, USA, 2010; pp. 1–4.
- Pomerleau, J.; Lock, K.; Knai, C.; McKee, M. Interventions designed to increase adult fruit and vegetable intake can be effective: A systematic review of the literature. J. Nutr. 2005, 135, 2486–2495. [Google Scholar]
- Lassen, A.; Thorsen, A.V.; Trolle, E.; Elsig, M.; Oveson, L. Successful strategies to increase the consumption of fruits and vegetables: Results from the Danish “6 a day” Work-site Canteen Model Study. Public Health Nutr. 2004, 7, S263–S270. [Google Scholar]
- Beresford, S.A.; Thompson, B.; Feng, Z.; Christianson, A.; McLerran, D.; Patrick, D.L. Seattle 5-a-day worksite program to increase fruit and vegetable consumption. Prev. Med. 2001, 32, S230–S238. [Google Scholar] [CrossRef]
- Sorensen, G.; Stoddard, A.; Peterson, K.; Stoddard, A.; Stein, E.; Phillips, J.; Baker, F.; Combe, C.; Hebert, J.; Palombo, R. Increasing fruit and vegetable consumption through worksites and families in the Treatwell 5-a-day study. Amer. J. Public Health 1999, 89, S54–S60. [Google Scholar] [CrossRef]
- Sorensen, G.; Stoddard, A.; Hunt, M.K.; Hebert, J.R.; Ockene, J.K.; Avrunin, J.S.; Himmelstein, J.; Hammond, S.K. The effects of a health promotion-health protection intervention on behavior change: The wellworks study. Amer. J. Public Health 1998, 88, S1685–S1690. [Google Scholar] [CrossRef]
- Perlmutter, C.A.; Canter, D.D.; Gregoire, M.B. Profitability and acceptability of fat- and sodium-modified hot entrees in a worksite cafeteria. J. Amer. Diet. Assn. 1997, 97, S391–S395. [Google Scholar] [CrossRef]
- Geaney, F.; Harrington, J.; Perry, I. The impact of a workplace catering initiative on dietary intakes of salt and other nutrients: A pilot study. Pub. Health Nutr. 2011, 14, S1345–S1349. [Google Scholar] [CrossRef]
- Guidance on Food Served to Older People in Residential Care; Food Standards Agency (FSA): London, UK, 2008; pp. 1–27.
- Johnson, D.B.; Beaudoin, S.; Smith, L.T.; Beresford, S.A.A.; LoGerfo, J.P. Increasing fruit and vegetable intake in homebound elders: The Seattle seniors farmers’ market nutrition pilot program. Prev. Chronic Dis. 2004, 1, S1–S9. [Google Scholar]
- Wekken, S.V.; Naylor, P.-J. Healthy Food and Beverage Sales in Recreation Facilities and Local Government Buildings. Available online: http://www.stayactiveeathealthy.ca/files/Initiative%20Summary%20and%20Evaluation%20Synopsis.pdf (accessed on 15 July 2012).
- Twiss, J.; Dickinson, J.; Duma, S.; Kleinman, T.; Paulsen, H.; Rilveria, L. Community Gardens: Lessons learned from California healthy cities and communities. Amer. J. Public Health 2003, 93, S1435–S1438. [Google Scholar] [CrossRef]
- Public Sector Food Procurement Initiative (PSFPI): An Evaluation; Department for Environment, Food, and Rural Affairs: London, UK, 2009; pp. 1–78.
- Norum, K.R. Some Aspects of Norwegian Nutrition and Food Policy. In Diet, Nutrition and chronic disease: Lessons from Contrasting Worlds; Shelty, P., McPherson, K., Eds.; Wiley and Sons, Ltd.: Chichester, UK, 1997; pp. 195–206. [Google Scholar]
- Sharma, S.; Gittelsohn, J.; Rosol, R.; Beck, L. Addressing the public health burden caused by the nutrition transition through the Healthy Foods North nutrition and lifestyle intervention programme. J. Hum. Nutr. Diet. 2010, 23, S120–S127. [Google Scholar]
- Glacken, J.B.; Hill, F. The Food Mail Pilot Projects: Achievements and Challenges; Minister of Indian Affairs and Northern Development and Federal Interlocutor for Métis and Non-status Indians: Ottawa, ON, Canada, 2009; pp. 1–52. [Google Scholar]
- Retail Based Nutrition Program; Food Security and Nutrition Unit, Health Canada: Ottawa, ON, Canada, 2009.
- Health and Sustainability Guidelines for Federal Concessions and Vending Operations. Available online: http://www.gsa.gov/portal/content/104429 (accessed on 15 July 2012).
- Ligaya, A. Food Fight: High School Students Lobby to Bring Back Pizza, Coffee andChocolate. Available online: http://news.nationalpost.com/2012/05/07/food-fight-high-school-students-lobby-to-bring-back-pizza-coffee-and-chocolate/ (accessed on 14 July 2012).
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Niebylski, M.L.; Lu, T.; Campbell, N.R.C.; Arcand, J.; Schermel, A.; Hua, D.; Yeates, K.E.; Tobe, S.W.; Twohig, P.A.; L'Abbé, M.R.; et al. Healthy Food Procurement Policies and Their Impact. Int. J. Environ. Res. Public Health 2014, 11, 2608-2627. https://doi.org/10.3390/ijerph110302608
Niebylski ML, Lu T, Campbell NRC, Arcand J, Schermel A, Hua D, Yeates KE, Tobe SW, Twohig PA, L'Abbé MR, et al. Healthy Food Procurement Policies and Their Impact. International Journal of Environmental Research and Public Health. 2014; 11(3):2608-2627. https://doi.org/10.3390/ijerph110302608
Chicago/Turabian StyleNiebylski, Mark L., Tammy Lu, Norm R. C. Campbell, Joanne Arcand, Alyssa Schermel, Diane Hua, Karen E. Yeates, Sheldon W. Tobe, Patrick A. Twohig, Mary R. L'Abbé, and et al. 2014. "Healthy Food Procurement Policies and Their Impact" International Journal of Environmental Research and Public Health 11, no. 3: 2608-2627. https://doi.org/10.3390/ijerph110302608
APA StyleNiebylski, M. L., Lu, T., Campbell, N. R. C., Arcand, J., Schermel, A., Hua, D., Yeates, K. E., Tobe, S. W., Twohig, P. A., L'Abbé, M. R., & Liu, P. P. (2014). Healthy Food Procurement Policies and Their Impact. International Journal of Environmental Research and Public Health, 11(3), 2608-2627. https://doi.org/10.3390/ijerph110302608