Effects of Air Pollution on the Risk of Congenital Anomalies: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods
2.1. Search Methods
2.2. Data Extraction
2.3. Meta-Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Location | Period | Study Design | Congenital Categories | Exposure Assessment | Exposure Variable | Air Pollutants | Results | Confounders |
|---|---|---|---|---|---|---|---|---|---|
| Gianicolo et al. 2014 [23] | Brindisi, Italy | 2000–2010 | Case-control, individual matching | Congenital heart defects, atrial septal defects | Daily average concentration of pollutants measured by 3 monitoring stations and performed for week 3–8 of gestation | Continuous and categorical | SO2 and TSP | Exposure to 90th percentile of SO2 increased risk of CHD (p = 0.01) and VSD (p < 0.05) | No adjusted confounders; cases and controls were matching for gender, socio-economic deprivation and the year of pregnancy |
| Schembari et al. 2013 [22] | Barcelona, Spain | 1994–2006 | Case-control, no matching | Congenital heart defects, neural tube defects, respiratory system defects, orofacial clefts, digestive system defects, abdominal wall | Daily spatio-temperal exposure estimates over week 3–8 of pregnancy | Continuous | NO2, NOx, PM10, PM2.5, PMcoarse | Statistically significant associations (p = 0.05) between NO2 and coarctation of the aorta and digestive system defects, and between PMcoarse and abdominal wall defects | Maternal age, socio-economic status, year of birth, conception season |
| Padula et al., 2013 [20] | California, USA | 1997–2006 | Case-control, no matching | Anotia/microtia, anorectal atresia/stenosis, craniosynostosis, hypospadias degree, diaphragmatic hernia, transverse limb deficiency, intestinal atresia/stenosis, amniotic band syndrome, limb body wall complex, hydrocephaly, longitudinal limb deficiency, esophageal atresia | Residence-based assignments around stations, with daily average values during first two months of were collected; a maximum interpolation radius of 50 km was used | Categorical | NO2, NO, CO, O3, PM10, PM2.5 | No significant association had been revealed | Maternal ethnicity, education, and early prenatal vitamin use |
| Padula et al. 2013 [19] | California, USA | 1997–2006 | Case-control, no matching | Congenital heart diseases groups (27 subtypes) | Residence-based assignments around stations, with daily average values during first two months of were collected; a maximum interpolation radius of 50 km was used | Categorical | NO, NO2, PM10, PM2.5, CO, O3 | No significant association had been revealed | Maternal ethnicity, education, and vitamin use |
| Agay-Shay K et al. 2013 [21] | Tel-Aviv, Israel | 2000–2006 | Case-control, no matching | Multiple congenital heart, atrial and atrial septal defects, isolated ventricular septal defects | Weekly means of exposures during pregnancy week 3–8 according to the distance from stations to each maternal address | Continuous | NO2, SO2, PM10, PM2.5, CO, O3 | No significant association had been revealed | Infant’s sex, plurality, religion, maternal age, maternal and paternal marital status, maternal and paternal origin, paternal age, and the season of conception |
| Padula et al. 2013 [18] | California, USA | 1997–2006 | Case-control, no matching | Neural tubes defects (spina bifida and anencephaly), orofacial clefts, gastroschisis | Residence-based assignments around stations, with daily average values during first two months of were collected; a maximum interpolation radius of 50 km was used | Categorical | NO2, NO, PM10, PM2.5, CO, O3 | No significant association had been revealed | Maternal ethnicity, education, and vitamin use |
| Dadvand et al. 2011 [28] | Northeast of UK | 1993–2003 | Case-control, frequency matching | Cardiac chambers and connection, cardiac septa, pulmonary and tricupid valves, aortic and mitral valves, great arteries and veins, atrial septal defect, coarctation of aorta, pulmonary valve stenosis, tetralogy of Fallot, ventricular septal defect | Weekly average of pollutants at nearest monitors to maternal residential location | Continuous | SO2, NO2, CO, PM10, O3 | An association between NO2 and congenital heart diseases, ventricular septal defect, cardiac septa malformations and tetralogy of Fallot; and CO exposure to ventricular septal defect, cardiac septa malformations and with congenital pulmonary valve stenosis | Socio-economic status, degree of urbanity, and season of conception; cases and controls were matching for the year of birth |
| Dadvand et al. 2011 [29] | Northeast of UK | 1985–1996 | Case-control, frequency matching | Coarctation of aorta, tetralogy of fallot, congenital pulmonary value stenosis, atrial septal defect, ventricular septal defect, congenital cardiac chambers and connections, congenital cardia septa, congenital pulmonary and tricuspid valves, congenital aortic and mitral valves, congenital great arteries and veins | Weekly exposure levels by two stage spaiotemporal modeling at each maternal place of residence | Categorical and continuous | SO2, black smoke | An association between maternal exposure to black smoke and cardiac chambers and connections (only when using exposure as a continuous variable) | Birth year, socio-economic status, infant sex, season of conception, and degree of urbanity; cases and controls were matching for the year of birth |
| Marshall et al. 2010 [30] | New Jersey, US | 1998–2003 | Case-control, frequency matching | Cleft lip with cleft palate, cleft palate | Average concentration of exposures at nearest monitor stations (13–20 km) | Categorical | SO2, NO2, CO, PM10, PM2.5, O3 | No significant association had been revealed | Maternal age, ethnicity, smoking and alcohol, and season of conception; cases and controls were matching with maternal residence at birth |
| Dolk et al. 2010 [31] | Wessex, North West Thamas, Oxford and Northern of UK | 1991–1999 | Cohort | Anomalies of cardiac chambers, transposition of great vessels, malformations of cardiac septa, atrioventricular septal defects, tetralogy of Fallot, malformations of valves, hypoplastice left heart syndrome, great arteries and veins, coarctation of aorta | Annual mean exposure at census level in 1996 | Continuous | SO2, NO2, PM10 | A significant association between SO2 and tetralogy of Fallot, and between PM10 and omphalocele | Maternal age, socio-economic deprivation |
| Hansen et al. 2009 [32] | Brisbane, Australia | 1998–2004 | Case-control, individual matching | Aortic artery and valve defects, atrial septal defects, pulmonary artery and valve defects, ventricular septal defects, conotruncal defects, endocardial cushion and mitral valve defects, cleft lip, cleft palate, cleft lip with cleft palate | Daily average exposures at 18 monitors with the majority located within a 30 km radius of city | Continuous | SO2, NO, CO, PM10 and O3 | No significant association had been revealed | Infant sex, birth order, season of birth, maternal age, education, alcohol, and body mass index; cases and controls were matching with mother’s age, marital status, number of previous pregnancies, month of LMP, area-level SES, and distance to pollution monitor |
| Rankin et al., 2009 [33] | Northern region, UK | 1985–1990 | Case-control, no matching | Nervous system, congenital heart defects, atrio ventricular septal defects, tetralogy of fallot, hypoplastic left heart, coarctation of aorta, patent ductus arteriosus, ventricular septal defect, respiratory tract, cleft lip and palate, eye, ear, face and neck, digestive system, internal urogenital system, musculoskeletal, miscellaneous | Daily average exposures during the first trimester from monitors within 10 km of maternal residence | Continuous and categorical | SO2, black smoke | A significant association between black smoke and nervous system anomalies. | Birth weight, infant sex, and maternal deprivation |
| Strickland et al. 2009 [34] | Atlanta, USA | 1986–2003 | Cohort | Tansposition of the great arteries, tetralogy of fallot, pulmonary stenosis and valvar, patent ductus arteriosus, hypoplastic left heart , coarctation of aorta, atrial septal defect, secundum, ventricular septal defect, muscular, ventricular septal defect, permimemnranous, conotruncal defect, Left ventricular outflow tract defect, right ventricular outflow tract defect | Average of daily concentration from one central monitoring station | Continuous | SO2, NO2, CO, PM10, and O3 | A significant association between PM10 and patent ductus arteriosus | No adjusted variables |
| Hwang et al. 2008 [24] | Taiwan | 2001–2003 | Case-control, no matching | Cleft lip | Monthly average of exposures at 72 stations by using inverse distance weighting method during the first trimester | Continuous | SO2, NO2, CO, PM10 and O3 | A significant association for first and second month O3 exposure | Maternal age, infant sex, plurality §, gestational age, population density, and season of conception |
| Kim et al. 2007 [35] | Seoul, Korea | 2001–2004 | Birth cohort | Not specified | Residence based average exposure levels at each trimester from nearest monitoring stations | Continuous and categorical | PM10 | Congenital anomalies were influenced by exposure to PM10 | Infant sex, birth order, season of birth, maternal age, maternal and paternal education, alcohol, body mass index and maternal weight before delivery |
| Giloba et al. 2005 [36] | Texas, USA | 1997–2000 | Case-control, frequency matching | Aortic artery and valve defects, atrial septal defects, pulmonary artery and valve defects, ventricular septal defects, conotruncal defects, endo-cardial cushin and mitral valve defects, cleft lip with cleft palate, cleft palate | Average of daily measurements based on the first closest monitor (median distance 8.6–14.2 km) | Categorical | SO2, NO2, CO, PM10 and O3 | A significant association between exposure to SO2 and VSD (p < 0.0001), CO and tetralogy of fallot (p < 0.0017), PM10 and ASD (p < 0.0001), SO2 with ASD (0.0017) | Maternal age, ethnicity, education, marital status, illness, tobacco use, season § of conception, plurality, parity, infant sex, prenatal care, and gravidity; cases and control were matching with vital status, year, maternal county of residence at delivery |
| Ritz et al. 2002 [9] | California, USA | 1987–1993 | Case-control, no matching | Aortic defects, Pulmonary valve, Conotruncal defects, Ventricular septal defects, Multiple cardiac or cleft defect, Syndrome with cardiac or cleft defect, Isolated cleft palate, Isolated cleft lip with/without palate | 24 h average measurements every 6 days over duration of pregnancy | Continuous and categorical | CO, O3 | No significant association had been revealed | Maternal age, ethnicity, education, marital status, illness, tobacco use, season of conception, plurality §, parity, decade of infant’s birth, infant sex, access to prenatal care, time since last pregnancy and birth type |
3. Results
| Studies | Case | Control | Total | ||
|---|---|---|---|---|---|
| Congenital Defects | Air Pollutants | Congenital Defects | Air Pollutants | ||
| Gianicolo et al. 2014 [23] | CHD | SO2, mean 2.9 μg/m3 | CHD | SO2, mean 2.8 μg/m3 | - |
| VSD | SO2, mean 3.2 μg/m3 | VSD | SO2, mean 2.8 μg/m3 | ||
| Schembari et al. 2013 [22] | - | IQR: NO2, 12.7 μg/m3 PM10, 2.8 μg/m3 | - | NO2, IQR 11.8 μg/m3 | - |
| - | - | PM10, IQR 3.0 μg/m3 | |||
| Agay-Shay et al. 2013 [21] | - | - | - | - | Minimum, median, maxmum: SO2 0.33 ppb, 2.1 ppb, 51.4 ppb; CO, 0.15 ppm, 0.9 ppm, 13.5 ppm; NO2 0.2 ppb, 23.1 ppb, 104.5 ppb; O3 0.45 ppb, 26.5 ppb, 128 ppb; PM10, 3.8 μg/m3, 43, 3183.4 μg/m3 |
| Padula et al. 2013 [18] | - | - | - | - | CO, Q1 0.13–0.39 ppm, Q4 0.72–1.37 ppm; NO2, Q1 2.4–13.36 ppb, Q4 20.54–638.94 ppb; O3, Q1 10.49–29.05 ppb, Q4 62.65–91.92 ppb; PM10, Q1 7.9–25.24 μg/m3, Q4 44.09–95.32 μg/m3 |
| Dadvand et al. 2011 [29] | - | - | - | - | Percentile 25- percentile 75: CO, 0.39–0.64 mg/m3; NO2, 29.2–38.4 μg/m3; NO, 13.3–32.5 μg/m3; O3, 33.2–42.4 μg/m3; PM10, 20.5–30.2 μg/m3 |
| Dadvand et al. 2011 [28] | - | - | - | - | Percentile 25–percentile 75: SO2, 17.6–31.2 μg/m3 |
| Marshall et al. 2010 [30] | - | Mean: PM10, 28.7 μg/m3 NO2, 2.4E−2 ppm SO2, 5.3E−3 ppm O3, 2.5E−2 ppm CO, 0.83 ppm | - | Mean: PM10, 28.1 μg/ m3 NO2, 2.4E−2 ppm SO2, 5.1E−3 ppm O3, 2.5E−2 ppm CO, 0.85 ppm | - |
| Dolk et al. 2010 * [31] | - | - | - | - | Percentile 10, median, percentile 90: SO2, 3.87 μg/m3, 7.86 μg/m3, 14.99 μg/m3 NO2, 21.48 μg/m3, 35.11 μg/m3, 47.78 μg/m3 PM10, 18.84 μg/m3, 21.97 μg/m3, 26.4 μg/m3 |
| Hansen et al. 2009 [32] | - | - | - | - | Minmum, mean, maxmum: SO2, 0, 1.5 ppb, 7.1 ppb; CO, 0.02 ppm, 1.1 ppm, 7.0 ppm; NO2, 1.4 ppb, 8.2 ppb, 22.7 ppb; O3, 4.3 ppb, 25.8 ppb, 54.4 ppb; PM10, 4.4 μg/m3, 18.0 μg/m3, 151.7 μg/m3 |
| Rankin et al. 2009 [33] | - | SO2 Q1–Q3, 2.7–4.4 μg/m3 | - | - | - |
| Strickland et al. 2009 * [34] | - | - | - | - | IQR: SO2, 4.0 ppb; CO, 0.3 ppm; NO2, 5.7 ppb; O3, 29.9 μg/m3; PM10, 14.2 μg/m3 |
| Hwang et al. 2008 [24] | - | - | - | - | Minmum, median, maxmum: O3, 16.7 ppb, 26.8 ppb, 45 ppb; CO, 25 pphm, 62 pphm, 277 pphm; NOx, 1.0 ppb, 20.2 ppb, 44.2 ppb; PM10, 20.8 μg/m3, 57.2 μg/m3, 78.1 μg/m3 |
| Gioboa et al. 2005 [36] | - | - | - | - | CO, Q1 < 0.4 ppm, Q4 ≥ 0.7 ppm; NO2, Q1 <1.3 pphm, Q4 ≥ 2.1 pphm; O3, Q1 < 1.8 pphm, Q4 ≥ 3.1 pphm; SO2, Q1 < 1.3 ppb, Q4 ≥ 2.7 ppb; PM10, Q1 < 19.5 μg/m3, Q4 ≥ 29 μg/m3 |




4. Discussion
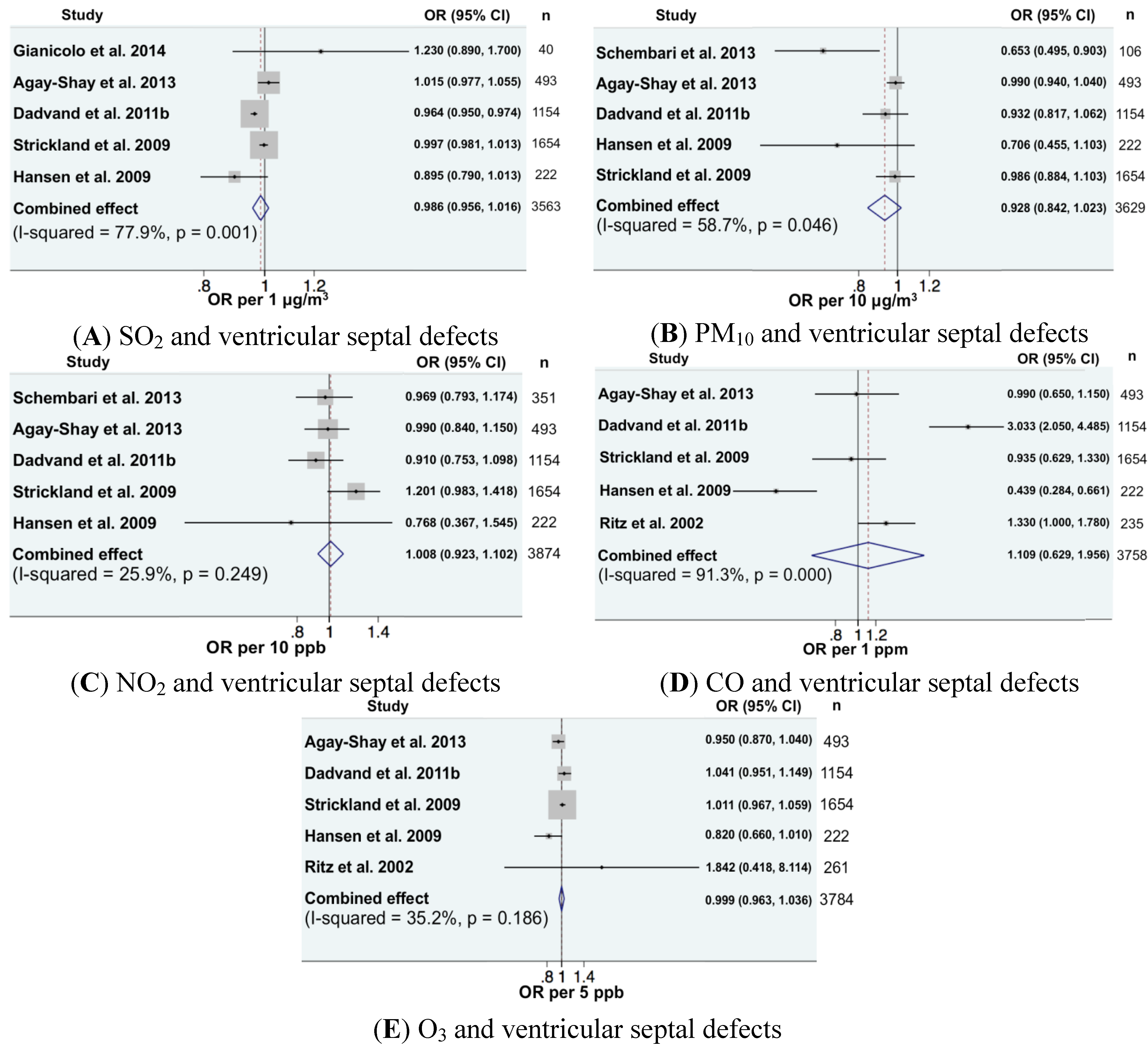
| Numbers of cases and controls exposed under various pollutants among different studies | Gianicolo et al. 2014 [23] | Schembari et al. 2013 [22] | Agay-Shay et al. 2013 [21] | Dadvand et al. 2011 [29] | Strickland et al. 2009 [34] | Hansen et al. 2009 [32] | Ritz et al. 2002 [9] | Total Number | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| case | control | case | control | case | control | case | control | case | control | case | control | case | control | case | control | |
| SO2 | 40 | 150 | - | - | 493 | 130,402 | 1154 | 4616 | 1654 | 713,846 | 222 | 1110 | 235 | 9049 | 3798 | 859,173 |
| PM10 | - | - | 106 | 903 | 493 | 130,402 | 1154 | 4616 | 1654 | 713,846 | 222 | 1110 | 235 | 9049 | 3864 | 859,926 |
| NO2 | - | - | 351 | 2869 | 493 | 130,402 | 1154 | 4616 | 1654 | 713,846 | 222 | 1110 | - | - | 3874 | 852,843 |
| CO | - | - | - | - | 493 | 130,402 | 1154 | 4616 | 1654 | 713,846 | 222 | 1110 | - | - | 3523 | 849,974 |
| O3 | - | - | - | - | 493 | 130,402 | 1154 | 4616 | 1654 | 713,846 | 222 | 1110 | - | - | 3523 | 849,974 |
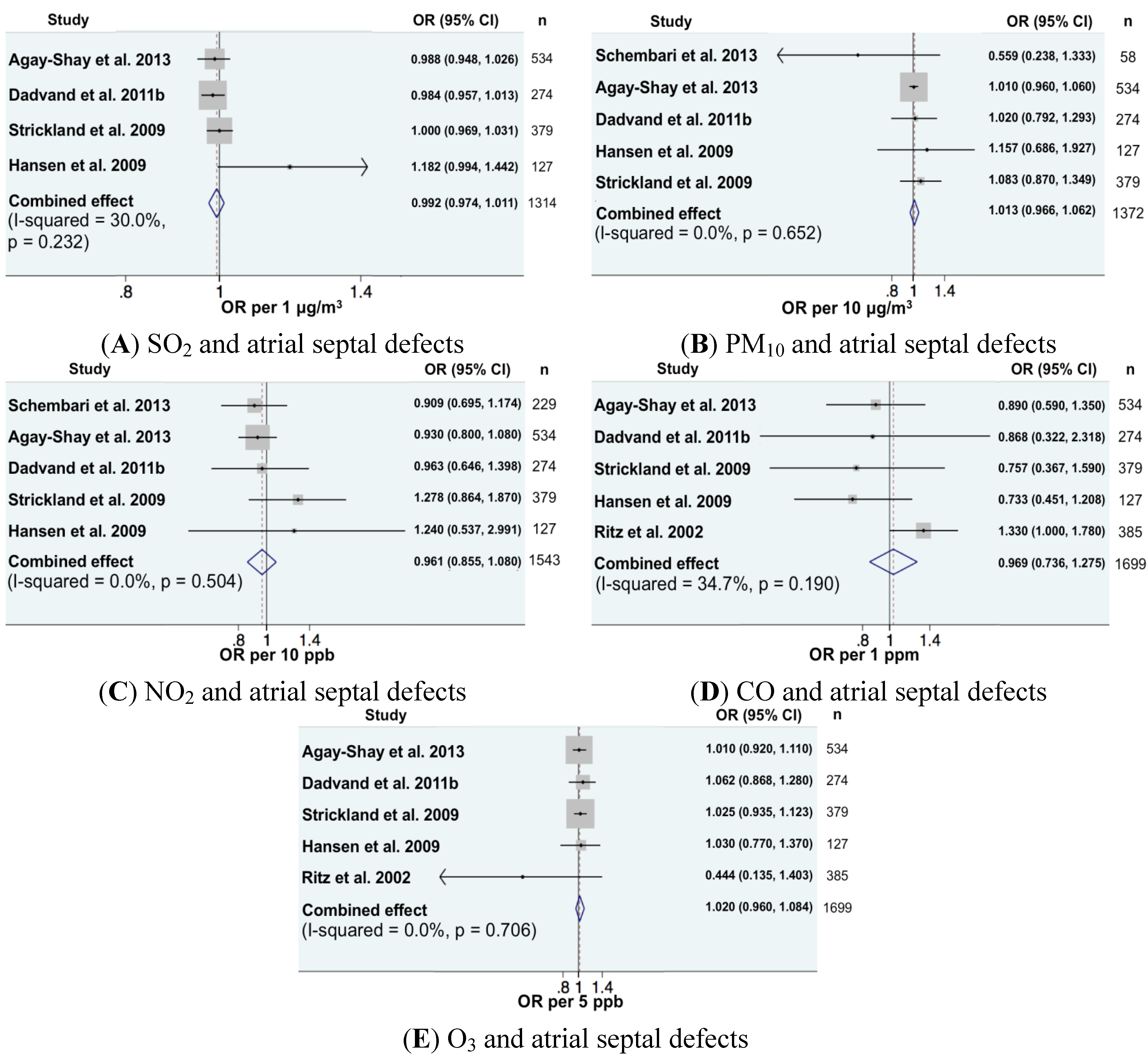
| Numbers of cases and controls exposed under various pollutants among different studies | Schembari et al. 2013 [22] | Agay-Shay et al. 2013 [21] | Dadvand et al. 2011 [29] | Strickland et al. 2009 [34] | Hansen et al. 2009 [32] | Ritz et al. 2002 [9] | Total Number | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| case | control | case | control | case | control | case | control | case | control | case | control | case | control | |
| SO2 | - | - | 534 | 130,402 | 274 | 1096 | 379 | 715,121 | 127 | 635 | - | - | 1314 | 847,254 |
| PM10 | 106 | 903 | 534 | 130,402 | 274 | 1096 | 379 | 715,121 | 127 | 635 | - | - | 1420 | 848,157 |
| NO2 | 229 | 2869 | 534 | 130,402 | 274 | 1096 | 379 | 715,121 | 127 | 635 | - | - | 1543 | 850,123 |
| CO | - | - | 534 | 130,402 | 274 | 1096 | 379 | 715,121 | 127 | 635 | 385 | 3000 | 1699 | 850,254 |
| O3 | - | - | 534 | 130,402 | 274 | 1096 | 379 | 715,121 | 127 | 635 | 385 | 3000 | 1699 | 850,254 |
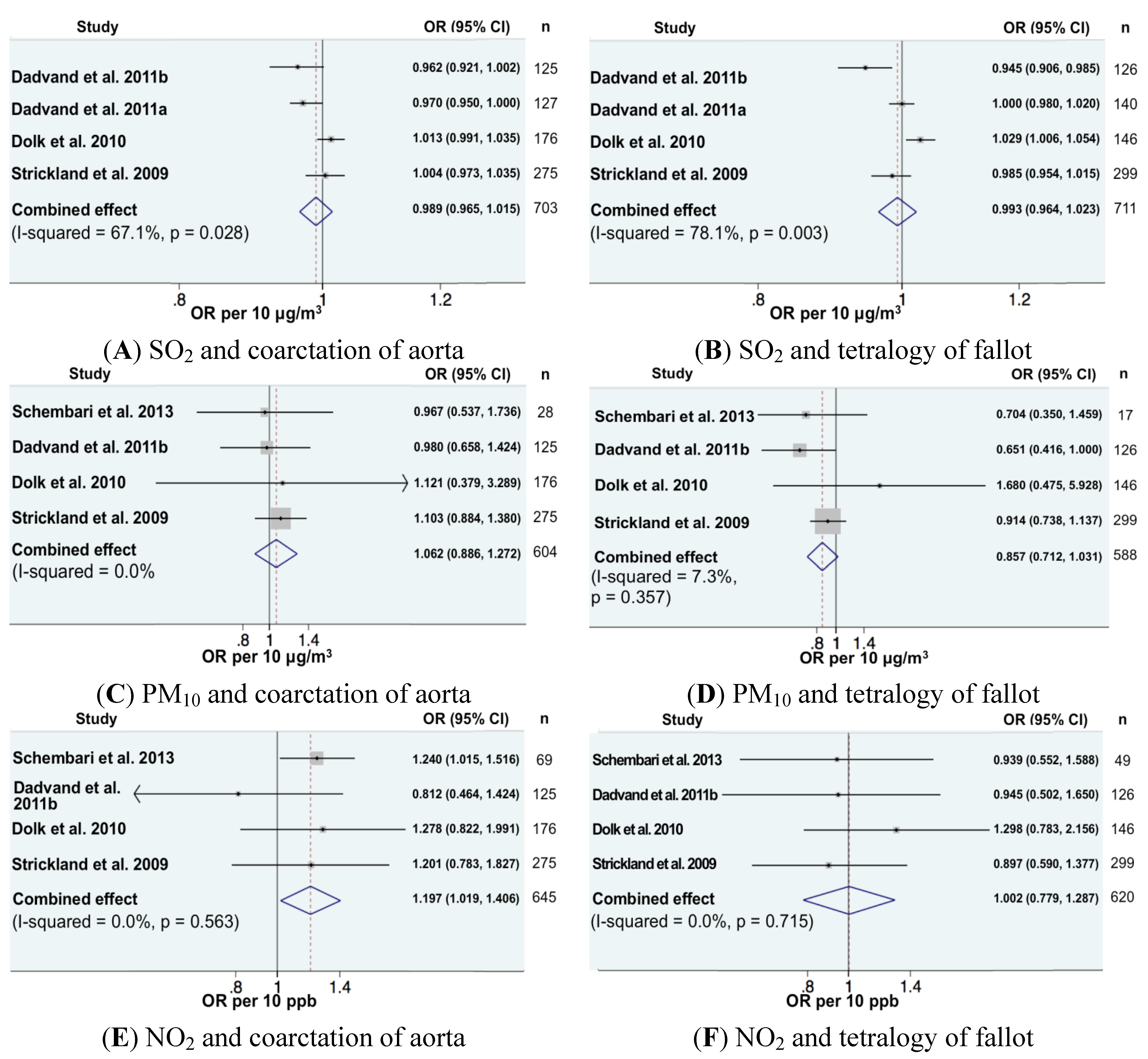
| Numbers of cases and controls exposed under various pollutants among different studies | Schembari et al. 2013 [22] | Dadvand et al. 2011 [29] | Dadvand et al. 2011 [28] | Dolk et al. 2010 [31] | Strickland et al. 2009 [34] | Total Number | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| case | control | case | control | case | control | case | control | case | control | case | control | |
| SO2 | - | - | 125 | 500 | 127 | 508 | 176 | 759,817 | 275 | 715225 | 703 | 1,476,050 |
| PM10 | 28 | 890 | 125 | 500 | - | - | 176 | 759,817 | 275 | 715225 | 604 | 1,476,432 |
| NO2 | 69 | 2869 | 125 | 500 | - | - | 176 | 759,817 | 127 | 715225 | 497 | 1,478,411 |
| Numbers of cases and controls exposed under various pollutants among different studies | Schembari et al. 2013 [22] | Dadvand et al. 2011 [29] | Dadvand et al. 2011 [28] | Dolk et al. 2010 [31] | Strickland et al. 2009 [34] | Total Number | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| case | control | case | control | case | control | case | control | case | control | case | control | |
| SO2 | - | - | 126 | 504 | 140 | 560 | 146 | 759,817 | 299 | 715,201 | 711 | 1,476,082 |
| PM10 | 17 | 890 | 126 | 504 | - | - | 146 | 759,817 | 299 | 715,201 | 588 | 1,476,412 |
| NO2 | 49 | 2650 | 126 | 504 | - | - | 146 | 759,817 | 299 | 715,201 | 620 | 1,478,172 |
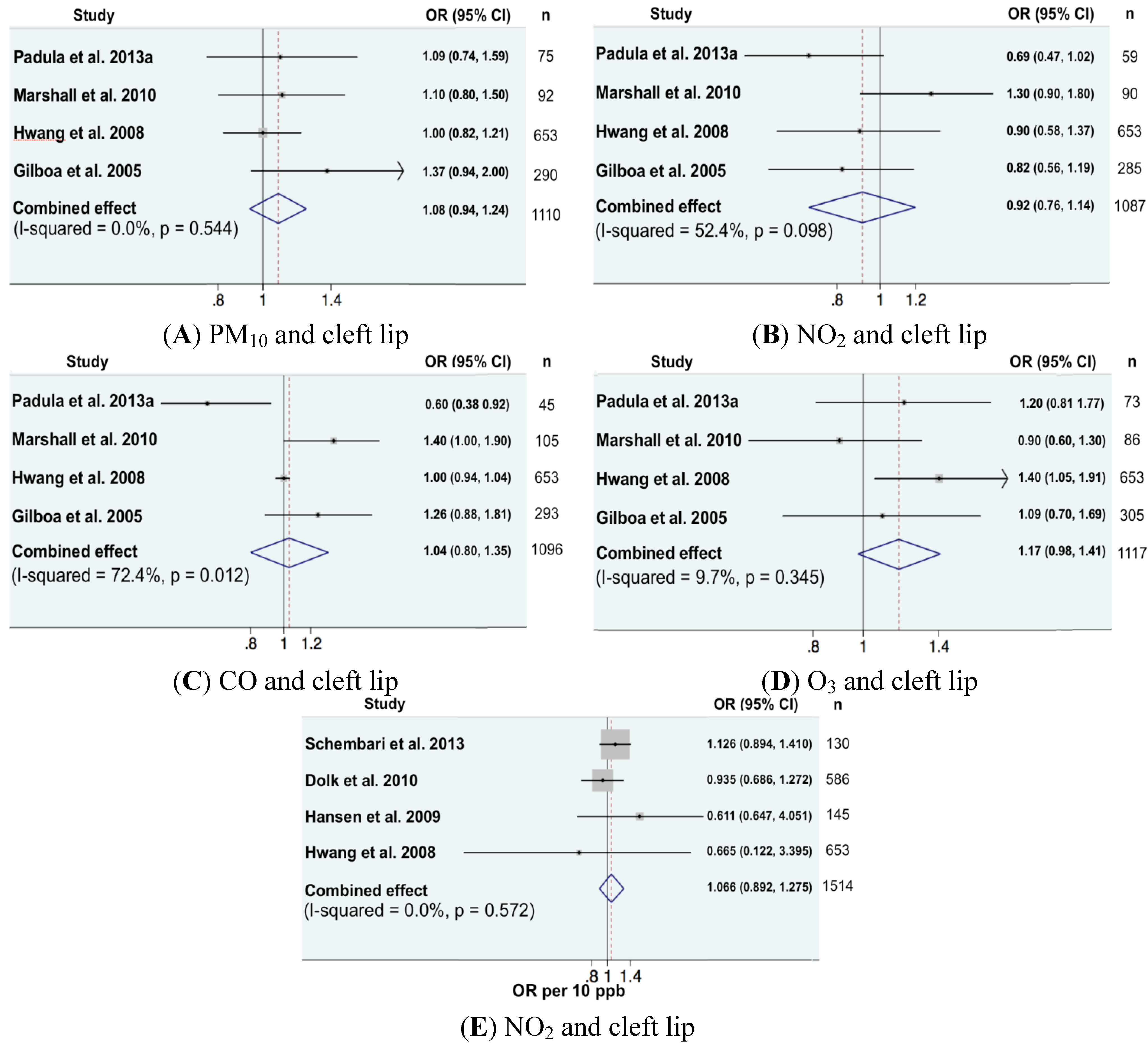
| Numbers of cases and controls exposed under various pollutants among different studies | Padula et al. 2013 [18] | Marshall et al. 2010 [30] | Hwang et al. 2008 [24] | Giloba et al. 2005 [36] | Total Number | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| case | control | case | control | case | control | case | control | case | control | |
| PM10 | 75 | 200 | 92 | 12,925 | 653 | 6530 | 290 | 3450 | 1110 | 23,105 |
| NO2 | 59 | 205 | 92 | 12,925 | 653 | 6530 | 285 | 3237 | 1089 | 22,897 |
| CO | 45 | 157 | 92 | 12,925 | 653 | 6530 | 293 | 3309 | 1083 | 22,921 |
| O3 | 73 | 201 | 92 | 12,925 | 653 | 6530 | 305 | 3594 | 1123 | 23,250 |
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- McConnell, R.; Islam, T.; Shankardass, K.; Jerrett, M.; Lurmann, F.; Gilliland, F.; Gauderman, J.; Avol, E.; Künzli, N.; Yao, L.; et al. Childhood incident asthma and traffic-related air pollution at home and school. Environ. Health Perspect. 2010, 118, 1021–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zmirou, D.; Gauvin, S.; Pin, I.; Momas, I.; Sahraoui, F.; Just, J.; le Moullec, Y.; Brémont, F.; Cassadou, S.; Reungoat, P.; et al. Traffic-related air pollution and incidence of childhood asthma: Results of the VESTA case control study. J. Epidemiol. Community Health 2004, 58, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Ko, F.W.; Hui, D.S. Air pollution and chronic obstructive pulmonary disease. Respirology 2012, 17, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Ito, K.; Thurston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA 2002, 287, 1132–1141. [Google Scholar]
- Nafstad, P.; Haheim, L.L.; Ofterdal, B.; Gram, F.; Holme, I.; Hjermann, I.; Leren, P. Lung cancer and air pollution: A 27 year follow up of 16,209 Norwegian men. Thorax 2003, 58, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Brunekreef, B.; Beelen, R.; Hoek, G.; Schouten, L.; Bausch-Goldbohm, S.; Fischer, P.; et al. Effects of long-term exposure to traffic-related air pollution on respiratory and cardiovascular mortality in the Netherlands: the NLCS-AIR study. Res. Rep. Health Eff. Inst. 2009, 139, 5–71. [Google Scholar]
- Nieuwenhuijsen, M.J.; Basagaña, X.; Dadvand, P.; Martinez, D.; Cirach, M.; Beelen, R.; Jacquemin, B. Air pollution and human fertility rates. Environ. Int. 2014, 27, 9–14. [Google Scholar] [CrossRef]
- Air Quality Guidelines; WHO: Copenhagen, Denmark, 2005.
- Ritz, B.; Yu, F.; Fruin, S.; Chapa, G.; Shaw, G.M.; Harris, J.A. Ambient air pollution and risk of birth defects in southern California. Amer. J. Epidemiol. 2002, 155, 17–25. [Google Scholar] [CrossRef]
- Karr, C.; Lumley, T.; Schreuder, A.; Davis, R.; Larson, T.; Ritz, B. Effects of subchronic and chronic exposure to ambient air pollutants on infant bronchiolitis. Amer. J. Epidemiol. 2007, 165, 553–560. [Google Scholar] [CrossRef]
- Pedersen, M.; Giorgis-Allemand, L.; Bernard, C.; Aguilera, I.; Anderson, A.M.; Ballester, F.; Beelen, R.M.; Chatzi, L.; Cirach, M.; Danileviciute, A.; et al. Ambient air pollution and low birthweight: A European cohort study (ESCAPE). Lancet Respir. Med. 2013, 1, 695–704. [Google Scholar] [CrossRef] [PubMed]
- Effects of Air Pollution on Children’s Health and Development; WHO: Copenhagen, Denmark, 2005.
- World Health Statistics; WHO: Geneva, Switzerland, 2013.
- Perinatal Mortality Associated with Congenital Anomalies in EUROCAT Full Member Registries, 2008–2012; European Surveillance of Congenital Anomalies (EUROCAT). Table 1. Available online: http://www.eurocat-network.eu/accessprevalencedata/keypublichealthindicators (accessed on 21 July 2014).
- Christianson, A.; Howson, C.P.; Modell, B. March of Dimes: Global Report on Birth Defects, the Hidden Toll of Dying and Disabled Children; March of Dimes Birth Defects Foundation: New York, NY, USA, 2006. [Google Scholar]
- Vrijheid, M.; Martinez, D.; Manzanares, S.; Dadvand, P.; Schembari, A.; Rankin, J.; Nieuwenhuijsen, M. Ambient air pollution and risk of congenital anomalies: A systematic review and meta-analysis. Environ. Health Perspect. 2011, 119, 598–606. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuijsen, M.J.; Martinez, D.; Grellier, J.; Bennett, J.; Best, N.; Iszatt, N.; Vrijheid, M.; Toledano, M.B. Chlorination disinfection by-products in drinking water and congenital anomalies: Review and meta-analyses. Environ. Health Perspect. 2009, 117, 1486–1493. [Google Scholar] [CrossRef] [PubMed]
- Padula, A.M.; Tager, I.B.; Carmichael, S.L.; Hammond, S.K.; Lurmann, F.; Shaw, G.M. The association of ambient air pollution and traffic exposures with selected congenital anomalies in the San Joaquin Valley of California. Amer. J Epidemiol. 2013, 177, 1074–1085. [Google Scholar] [CrossRef]
- Padula, A.M.; Tager, I.B.; Carmichael, S.L.; Hammond, S.K.; Yang, W.; Lurmann, F.; Shaw, G.M. Ambient air pollution and traffic exposures and congenital heart defects in the San Joaquin Valley of California. Paediatr. Perinat. Epidemiol. 2013, 27, 329–339. [Google Scholar] [CrossRef]
- Padula, A.M.; Tager, I.B.; Carmichael, S.L.; Hammond, S.K.; Yang, W.; Lurmann, F.W.; Shaw, G.M. Traffic-related air pollution and selected birth defects in the San Joaquin Valley of California. Birth Defects Res. Pt. A 2013, 97, 730–735. [Google Scholar] [CrossRef]
- Agay-Shay, K.; Friger, M.; Linn, S.; Peled, A.; Amitai, Y.; Peretz, C. Air pollution and congenital heart defects. Environ. Res. 2013, 124, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Schembari, A.; Nieuwenhuijsen, M.J.; Salvador, J.; de Nazelle, A.; Cirach, M.; Dadvand, P.; Beelen, R.; Hoek, G.; Basagaña, X.; Vrijheid, M. Traffic-related air pollution and congenital anomalies in Barcelona. Environ. Health Perspect. 2014, 122, 317–323. [Google Scholar] [PubMed]
- Gianicolo, E.A.; Mangia, C.; Cervino, M.; Bruni, A.; Andreassi, M.G.; Latini, G. Congenital anomalies among live births in a high environmental risk area—A case-control study in Brindisi (southern Italy). Environ. Res. 2014, 128, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Hwang, B.F.; Jaakkola, J.J.K. Ozone and other air pollutants and risk of oral clefts. Environ. Health Perspect. 2008, 116, 1411–1415. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6. [Google Scholar] [CrossRef]
- Warren, J.; Fuentes, M.; Herring, A.; Kanglois, P. Bayesian spatial-temporal model for cardiac congenital anomalies and ambient air pollution risk assessment. Environmetrics 2012, 23, 673–684. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 1557–1560. [Google Scholar] [CrossRef] [Green Version]
- Dadvand, P.; Rankin, J.; Rushton, S.; Pless-Mulloli, T. Ambient air pollution and congenital heart disease: A register-based study. Environ. Res. 2011, 111, 435–441. [Google Scholar] [CrossRef]
- Dadvand, P.; Rankin, J.; Rushton, S.; Pless-Mulloli, T. Association between maternal exposure to ambient air pollution and congenital heart disease: A register-based spatiotemperal analysis. Amer. J. Epidemiol. 2011, 173, 171–182. [Google Scholar] [CrossRef]
- Marshall, E.G.; Harris, G.; Wartenberg, D. Oral cleft defects and maternal exposure to ambient air pollutants in New Jersey. Birth Defects Res. Pt. A 2010, 88, 205–215. [Google Scholar] [CrossRef]
- Dolk, H.; Armstrong, B.; Lachowycz, K.; Vrijheid, M.; Rankin, J.; Abramsky, L.; Boyd, P.A.; Wellesley, D. Ambient air pollution and risk of congenital anomalies in England,1991–1999. Occup. Environ. Medicine 2010, 67, 223–227. [Google Scholar] [CrossRef]
- Hansen, C.A.; Barnett, A.G.; Jalaludin, B.B.; Morgan, G.G. Ambient air pollution and birth defects in Brisbane, Australia. PLoS One 2009, 4. [Google Scholar] [CrossRef] [Green Version]
- Rankin, J.; Chadwick, T.; Natarajan, M.; Howel, D.; Pearce, M.S.; Pless-Mulloli, T. Maternal exposure to ambient air pollutants and risk of congenital anomalies. Environ. Res. 2009, 109, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Strickland, M.J.; Klein, M.; Correa, A.; Reller, M.D.; Mahle, W.T.; Riehle-Colarusso, T.J.; Botto, L.D.; Flanders, W.D.; Mulholland, J.A.; Siffel, C.; et al. Ambient air pollution and cardiovascular malformations in Atlanta, Georgia, 1986–2003. Amer. J. Epidemiol. 2009, 169, 1004–1014. [Google Scholar]
- Kim, O.J.; Ha, E.H.; Kim, B.M.; Seo, J.H.; Park, H.S.; Jung, W.J.; Lee, B.E.; Suh, Y.J.; Kim, Y.J.; Lee, J.T.; et al. PM10 and pregnancy outcomes: A hospital-based cohort study of pregnant women in Seoul. J. Occup. Environ. Med. 2007, 49, 1394–1402. [Google Scholar] [CrossRef] [PubMed]
- Giloba, S.M.; Mendola, P.; Olshan, A.F.; Langlois, P.H.; Savitz, D.A.; Loomis, D.; Herring, A.H.; Fixler, D.E. Relation between ambient air quality and selected birth defects, seven county study, Texas, 1997–2000. Amer. J. Epidemiol. 2005, 162, 238–252. [Google Scholar] [CrossRef]
- Institut de Veille Sanitaire (InVS). Available online: http://www.invs.sante.fr/fr/Espace-presse/Communiques-de-presse/2014/L-Institut-de-veille-sanitaire-publie-pour-la-premiere-fois-des-estimations-nationales-sur-le-nombre-d-anomalies-congenitales-en-France (accessed on 18 July 2014).
- Botto, L.D.; Lin, A.E.; Riehle-Colarusso, T.; Malik, S.; Correa, A.; National Birth Defects Prevention Study. Seeking causes: Classifying and evaluating congenital heart defects in etiologic studies. Birth Defects Res. Pt. A 2007, 79, 714–727. [Google Scholar]
- Hackshw, A.; Rodeck, C.; Boniface, S. Maternal smoking in pregnancy and birth defects: A systematic review based on 173,687 malformed cases and 11.7 million controls. Hum. Reprod. Update. 2011, 17, 589–604. [Google Scholar] [CrossRef]
- Cresci, M.; Foffa, I.; Ait-Ali, L.; Pulignani, S.; Gianicolo, E.A.; Botto, N.; Picano, E.; Andreassi, M.G. Maternal and paternal environmental risk factors, metabolizing GSTM1 and GSTT1 polymorphisms, and congenital heart disease. Amer. J Cardiol. 2011, 108, 1625–1631. [Google Scholar] [CrossRef] [PubMed]
- Loane, M.; Dolk, H.; Morris, J.K.; EUROCAT Working Group. Maternal age-specific risk of non-chromosomal anomalies. BJOG 2009, 116, 1111–1119. [Google Scholar]
- De la Vega, A.; López-Cepero, R. Seasonal variations in the incidence of some congenital anomalies in Puerto Rico based on the timing of conception. P. R. Health Sci. J. 2009, 28, 121–125. [Google Scholar] [PubMed]
- Varela, M.M.; Nohr, E.A.; Llopis-González, A.; Andersen, A.M.; Olsen, J. Socio-occupational status and congenital anomalies. Eur. J. Public Health 2009, 19, 161–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Ottawa Hospital Research Institute. 2014. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 21 July 2014).
- Detsky, A.S.; Naylor, C.D.; O’Rourke, K.; McGeer, A.J.; L’Abbé, K.A. Incorporating variations in the quality of individual randomized trials into meta-analysis. J. Clin. Epidemiol. 1992, 45, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Julian, P.T.H.; Sally, G. Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0. ed. The Cochrane Collaboration. 2011. Available online: www.cochrane-handbook.org (accessed on 21 July 2014).
- Kampa, M.; Castanas, E. Human health effects of air pollution. Environ. Pollut. 2008, 151, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Kannan, S.; Misra, D.P.; Dvonch, J.T.; Krishnakumar, A. Exposures to airborne particulate matter and adverse perinatal outcomes: A biologically plausible mechanistic framework for exploring potential effect modification by nutrition. Environ. Health Perspect. 2006, 114, 1636–1642. [Google Scholar] [PubMed]
- Slama, R.; Darrow, L.; Parker, J.; Woodruff, T.J.; Strickland, M.; Nieuwenhuijsen, M.; et al. Meeting report: Atmospheric pollution and human reproduction. Environ. Health Perspect. 2008, 116, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Baccarelli, A.; Bollati, V. Epigenetics and environmental chemicals. Curr. Opin. Pediatr. 2009, 21, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Hou, L.; Wang, D.; Baccarell, A. Environmental chemicals and microRNAs. Mutat. Res. 2011, 714, 105–112. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Chen, E.K.-C.; Zmirou-Navier, D.; Padilla, C.; Deguen, S. Effects of Air Pollution on the Risk of Congenital Anomalies: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2014, 11, 7642-7668. https://doi.org/10.3390/ijerph110807642
Chen EK-C, Zmirou-Navier D, Padilla C, Deguen S. Effects of Air Pollution on the Risk of Congenital Anomalies: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2014; 11(8):7642-7668. https://doi.org/10.3390/ijerph110807642
Chicago/Turabian StyleChen, Esther Kai-Chieh, Denis Zmirou-Navier, Cindy Padilla, and Séverine Deguen. 2014. "Effects of Air Pollution on the Risk of Congenital Anomalies: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 11, no. 8: 7642-7668. https://doi.org/10.3390/ijerph110807642
APA StyleChen, E. K. -C., Zmirou-Navier, D., Padilla, C., & Deguen, S. (2014). Effects of Air Pollution on the Risk of Congenital Anomalies: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 11(8), 7642-7668. https://doi.org/10.3390/ijerph110807642