The Joint Influence of Gender and Amount of Smoking on Weight Gain One Year after Smoking Cessation

Abstract
:1. Introduction
2. Methods
2.1. Data
2.2. Outcomes and Inclusion/Exclusion Criteria
2.3. Covariates and Assumptions

2.4. Statistical Analysis
3. Results


{kind=link}
{kind=link}
{kind=link}
| Characteristics | PHASMO (n = 417) | CAROSS (n = 333) | p-value for Difference | Overall (n = 750) |
|---|---|---|---|---|
| Age, mean (SD) | 42.7 (9.8) | 51.4 (9.8) | <0.001 * | 46.6 (9.8) |
| Women, No. (%) | 181 (43.4) | 146 (43.8) | 0.90 † | 327 (43.6) |
| Education level, No. (%) ‡ | 0.09 § | |||
| 9 years | 49 (12.3) | 33 (10.6) | 82 (11.5) | |
| 12 years | 223 (55.9) | 209 (67.2) | 432 (60.9) | |
| 14 years | 72 (18.0) | 32 (10.3) | 104 (14.6) | |
| 16 years | 55 (13.8) | 37 (11.9) | 92 (13.0) | |
| No. cigarettes per day at baseline, median (IQ range) | 25 (20–30) | 20 (17–30) | <0.001 § | 22 (20–30) |
| Follow-up, No. (%) || | <0.001 | |||
| <20 weeks | 110 (26.4) | 0 (0.0) | 110 (14.7) | |
| 20–40 weeks | 25 (6.0) | 2 (0.6) | 27 (3.6) | |
| >40 weeks | 282 (67.6) | 331 (99.4) | 613 (81.7) | |
| Cumulative duration of abstinence, No. (%) | 0.50 ¶ | |||
| <20 weeks | 212 (50.8) | 174 (52.3) | 386 (51.5) | |
| 20–40 weeks | 50 (12.0) | 31 (9.3) | 81 (10.8) | |
| >40 weeks | 155 (37.2) | 128 (38.4) | 284 (37.7) | |
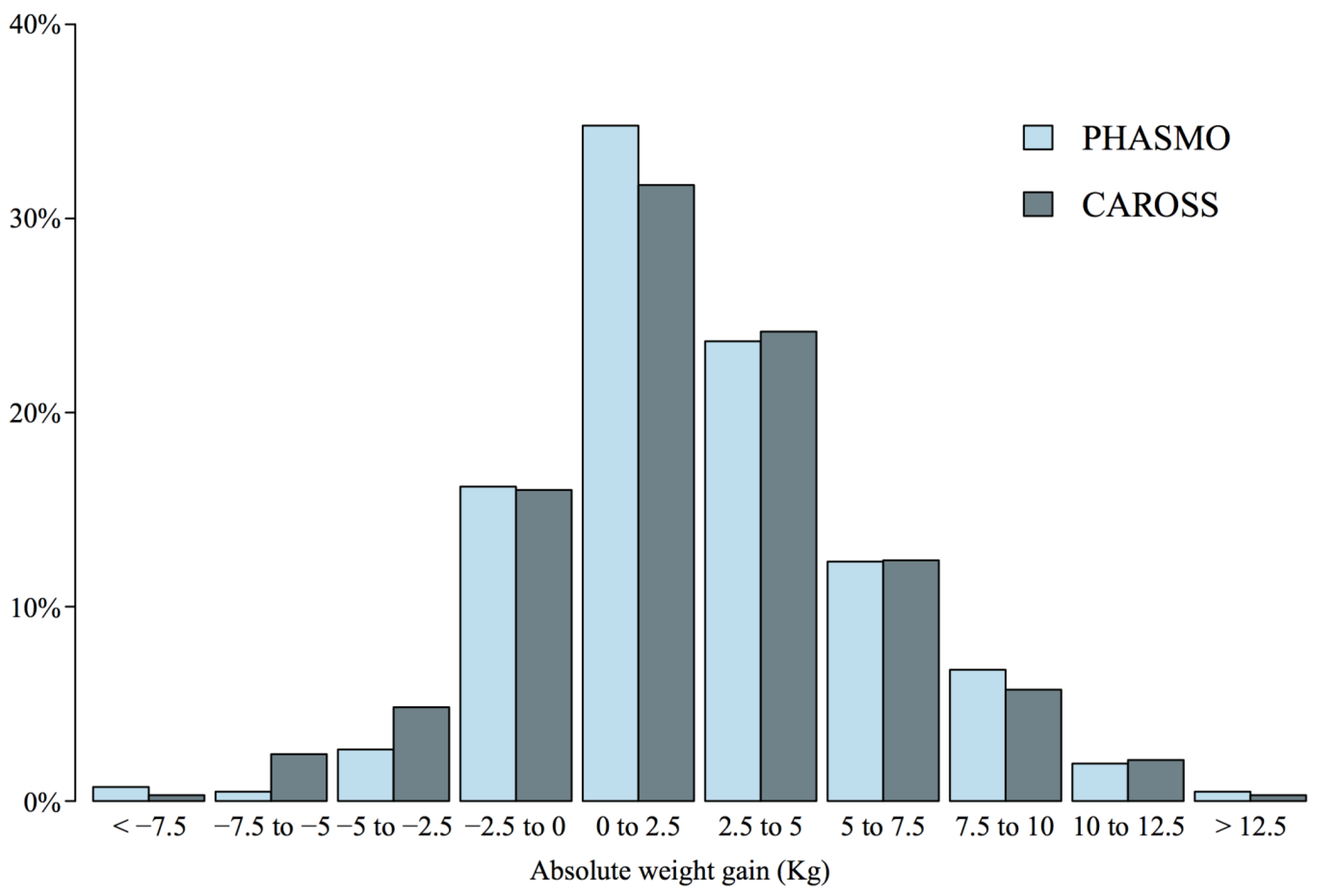
| Absolute weight gain, kg #, mean (SD) | 2.7 (3.6) | 2.4 (3.8) | 0.31 * | 2.6 (3.7) |
| Relative weight gain, %, mean (SD) | 3.8 (5.1) | 3.2 (5.0) | 0.11 * | 3.6 (5.0) |
| Cumulative Duration of Abstinence, No. (%) | Absolute Weight Gain, kg, Mean (SD) | Relative Weight Gain, %, Mean (SD) |
|---|---|---|
| <20 weeks | 1.2 (2.6) | 1.7 (3.7) |
| 20–40 weeks | 2.0 (4.4) | 3.1 (5.9) |
| >40 weeks | 4.6 (3.8) | 6.2 (5.2) |
| Characteristics | Outcome = Absolute Weight Gain (kg) | Outcome = Relative Weight Gain (%) | ||
|---|---|---|---|---|
| Estimate (95% CI) | p-value | Estimate (95% CI) | p-value | |
| Intercept | 1.1 * (0.3; 1.9) | 0.005 | 1.4 (0.3; 2.5) | 0.02 |
| Study | ||||
| CAROSS | Reference | Reference | ||
| PHASMO | −0.1 (−0.7; 0.4) | 0.66 | 0.1 (−0.7; 0.8) | 0.89 |
| Group | ||||
| Control | Reference | Reference | ||
| Intervention | −0.1 (−0.5; 0.4) | 0.81 | −0.2 (−0.8; 0.5) | 0.65 |
| Abstinence | ||||
| <20 weeks | Reference | Reference | ||
| 20–40 weeks | 0.9 † (0.1; 1.7) | 0.02 | 1.5 (0.4; 2.6) | 0.009 |
| >40 weeks | 3.4 ‡ (2.9; 3.9) | <0.001 | 4.6 (3.9; 5.3) | <0.001 |
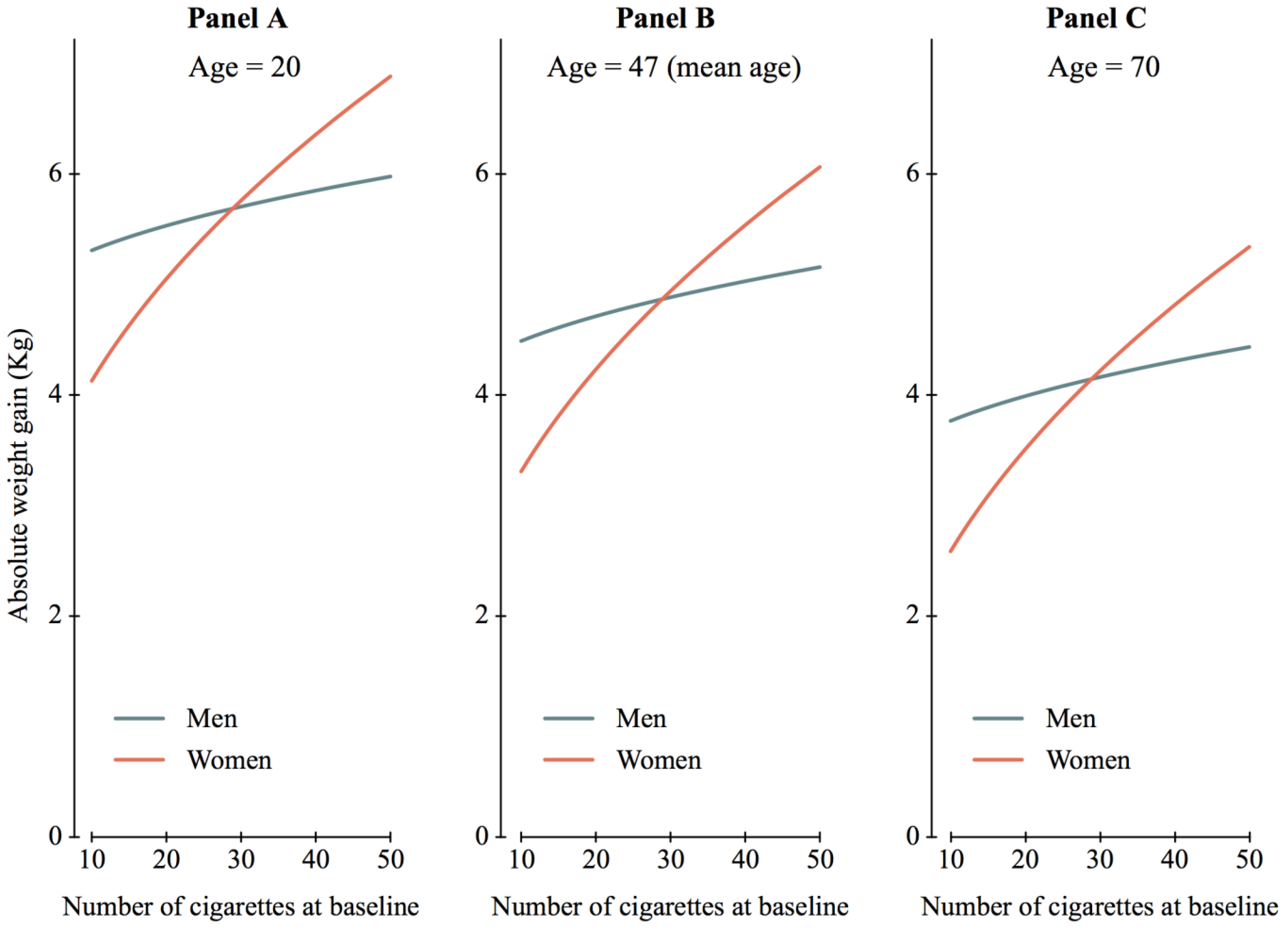
| Age (10 years) | −0.3 (−0.6; 0.0) | 0.02 | −0.4 (−0.8; −0.1) | 0.02 |
| Sex | ||||
| Men | Reference | |||
| Women | −1.2 § (−2.2; −0.2) | 0.02 | −1.0 (−2.4; 0.4) | 0.16 |
| √NCB || | 0.2 # (−0.2; 0.5) | 0.32 | 0.2 (−0.3; 0.6) | 0.52 |
| Sex √NCB | 0.5 ** (0.0; 1.1) | 0.05 | 0.8 (0.0; 1.5) | 0.04 |
4. Discussion

5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization Report on the Global Tobacco Epidemic: Warning about the Dangers of Tobacco; World Health Organization: Geneva, Switzerland, 2011.
- Perkins, K.A. Weight gain following smoking cessation. J. Consult Clin. Psychol. 1993, 61, 768–777. [Google Scholar] [CrossRef]
- Froom, P.; Melamed, S.; Benbassat, J. Smoking cessation and weight gain. J. Fam. Pract. 1998, 46, 460–464. [Google Scholar]
- Filozof, C.; Fernandez Pinilla, M.C.; Fernandez-Cruz, A. Smoking cessation and weight gain. Obes. Rev. 2004, 5, 95–103. [Google Scholar] [CrossRef]
- Pistelli, F.; Aquilini, F.; Carrozzi, L. Weight gain after smoking cessation. Monaldi Arch. Chest Dis. 2009, 71, 81–87. [Google Scholar]
- Klesges, R.C.; Brown, K.; Pascale, R.W.; Murphy, M.; Williams, E.; Cigrang, J. Factors associated with participation, attrition, and outcome in a smoking cessation program at the workplacee. Health Psychol. 1988, 7, 575–589. [Google Scholar] [CrossRef]
- Klesges, R.C.; Shumaker, S.A. Understanding the relations between smoking and body weight and their importance to smoking cessation and relapse. Health Psychol. 1992, 11, 1–3. [Google Scholar] [CrossRef]
- Klesges, R.C.; Meyers, A.W.; Klesges, L.M.; La Vasque, M.E. Smoking, body weight, and their effects on smoking behavior: A comprehensive review of the literature. Psychol. Bull. 1989, 106, 204–230. [Google Scholar] [CrossRef]
- United States Department of Health and Human Services. The Health Benefits of Smoking Cessation; U.S. Government Printing Office: Washington, DC, USA, 1990. [Google Scholar]
- Aubin, H.-J.; Farley, A.; Lycett, D.; Lahmek, P.; Aveyard, P. Weight gain in smokers after quitting cigarettes: Meta-analysis. BMJ 2012. [Google Scholar] [CrossRef]
- Bize, R.; Willi, C.; Chiolero, A.; Stoianov, R.; Payot, S.; Locatelli, I.; Cornuz, J. Participation in a population-based physical activity programme as an aid for smoking cessation: A randomised trial. Tob. Control 2010, 19, 488–494. [Google Scholar] [CrossRef]
- Prod’hom, S.; Locatelli, I.; Giraudon, K.; Marques-Vidal, P.; Clair, C.; Bize, R.; Cornuz, J. Predictors of weight change in sedentary smokers receiving a standard smoking cessation intervention. Nicotine Tob. Res. 2013, 15, 910–916. [Google Scholar] [CrossRef]
- Rodondi, N.; Collet, T.H.; Nanchen, D.; Locatelli, I.; Depairon, M.; Aujesky, D.; Bovet, P.; Cornuz, J. Impact of carotid plaque screening on smoking cessation and other cardiovascular risk factors: A randomized controlled trial. Arch. Intern. Med. 2012, 172, 344–352. [Google Scholar] [CrossRef]
- West, R.; Hajek, P.; Stead, L.; Stapleton, J. Outcome criteria in smoking cessation trials: Proposal for a common standard. Addiction 2005, 100, 299–303. [Google Scholar] [CrossRef]
- Klesges, R.C.; Winders, S.E.; Meyers, A.W.; Eck, L.H.; Ward, K.D.; Hultquist, C.M.; Ray, J.V.; Shadish, W.R. How much weight gain occurs following smoking cessation? A comparison of weight gain using both continuous and point prevalence abstinence. J. Consult Clin. Psychol. 1997, 65, 286–291. [Google Scholar] [CrossRef]
- Hall, S.M.; Ginsberg, D.; Jones, R.T. Smoking cessation and weight gain. J. Consult Clin. Psychol. 1986, 54, 342–346. [Google Scholar] [CrossRef]
- Williamson, D.F.; Madans, J.; Anda, R.F.; Kleinman, J.C.; Giovino, G.A.; Byers, T. Smoking cessation and severity of weight gain in a national cohort. N. Engl. J. Med. 1991, 324, 739–745. [Google Scholar] [CrossRef]
- Swan, G.; Carmelli, D. Characteristics associated with excessive weight gain after smoking cessation in men. Amer. J. Public Health 1995, 85, 73–77. [Google Scholar] [CrossRef]
- O’Hara, P.; Connett, J.E.; Lee, W.W.; Nides, M.; Murray, R.; Wise, R. Early and late weight gain following smoking cessation in the Lung Health Study. Amer. J. Epidemiol. 1998, 148, 821–830. [Google Scholar] [CrossRef]
- Doherty, K.; Militello, F.S.; Kinnunen, T.; Garvey, A.J. Nicotine gum dose and weight gain after smoking cessation. J. Consult Clin. Psychol. 1996, 64, 799–807. [Google Scholar] [CrossRef]
- Chinn, S.; Jarvis, D.; Melotti, R.; Luczynska, C.; Ackermann-Liebrich, U.; Antó, J.M.; Cerveri, I.; de Marco, R.; Gislason, T.; Heinrich, J.; et al. Smoking cessation, lung function, and weight gain: A follow-up study. Lancet 2005, 365, 1629–1935. [Google Scholar] [CrossRef]
- Nides, M.; Rand, C.; Dolce, J.; Murray, R.; O’Hara, P.; Voelker, H.; Connett, J. Weight gain as a function of smoking cessation and 2-mg nicotine gum use among middle-aged smokers with mild lung impairment in the first 2 years of the Lung Health Study. Health Psychol. 1994, 13, 354–361. [Google Scholar] [CrossRef]
- Aubin, H.-J.; Berlin, I.; Smadja, E.; West, R. Factors associated with higher body mass index, weight concern, and weight gain in a multinational cohort study of smokers intending to quit. Int. J. Environ. Res. Public Health 2009, 6, 943–957. [Google Scholar] [CrossRef]
- Riley, R.D.; Lambert, P.C.; Abo-Zaid, G. Meta-analysis of individual participant data: Rationale, conduct, and reporting. BMJ 2010. [Google Scholar] [CrossRef]
- Lycett, D.; Munafo, M.; Johnstone, E.; Murphy, M.; Aveyard, P. Associations between weight change over 8 years and baseline body mass index in a cohort of continuing and quitting smokers. Addiction 2011, 106, 188–196. [Google Scholar] [CrossRef]
- Garvey, W.T.; Ryan, D.H.; Look, M.; Gadde, K.M.; Allison, D.B.; Peterson, C.A.; Schwiers, M.; Day, W.W.; Bowden, C.H. Two-year sustained weight loss and metabolic benefits with controlled-release phentermine/topiramate in obese and overweight adults (SEQUEL): A randomized, placebo-controlled, phase 3 extension study. Amer. J. Clin. Nutr. 2012, 95, 297–308. [Google Scholar] [CrossRef]
- Batterham, M.J.; Tapsell, L.C.; Charlton, K.E. Analyzing weight loss intervention studies with missing data: Which methods should be used? Nutrition 2013, 29, 1024–1029. [Google Scholar] [CrossRef]
- Killen, J.D.; Fortmann, S.P.; Telch, M.J.; Newman, B. Are heavy smokers different from light smokers? Comparison after 48 h without cigarettes. JAMA 1988, 260, 1581–1585. [Google Scholar] [CrossRef]
- Burns, D.M.; Major, J.M.; Vaughn, J.W.; Anderson, C.M.; Shanks, T.G. Cigarette Smoking among Adolescents in California, 1990–1996; NIH Publication: Bethesda, MD, USA, 2001. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Locatelli, I.; Collet, T.-H.; Clair, C.; Rodondi, N.; Cornuz, J. The Joint Influence of Gender and Amount of Smoking on Weight Gain One Year after Smoking Cessation. Int. J. Environ. Res. Public Health 2014, 11, 8443-8455. https://doi.org/10.3390/ijerph110808443
Locatelli I, Collet T-H, Clair C, Rodondi N, Cornuz J. The Joint Influence of Gender and Amount of Smoking on Weight Gain One Year after Smoking Cessation. International Journal of Environmental Research and Public Health. 2014; 11(8):8443-8455. https://doi.org/10.3390/ijerph110808443
Chicago/Turabian StyleLocatelli, Isabella, Tinh-Hai Collet, Carole Clair, Nicolas Rodondi, and Jacques Cornuz. 2014. "The Joint Influence of Gender and Amount of Smoking on Weight Gain One Year after Smoking Cessation" International Journal of Environmental Research and Public Health 11, no. 8: 8443-8455. https://doi.org/10.3390/ijerph110808443
APA StyleLocatelli, I., Collet, T. -H., Clair, C., Rodondi, N., & Cornuz, J. (2014). The Joint Influence of Gender and Amount of Smoking on Weight Gain One Year after Smoking Cessation. International Journal of Environmental Research and Public Health, 11(8), 8443-8455. https://doi.org/10.3390/ijerph110808443