Climatic Factors and Community — Associated Methicillin-Resistant Staphylococcus aureus Skin and Soft-Tissue Infections — A Time-Series Analysis Study


 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Study Participants and Sample Collection
2.3. Isolation of S. aureus and Antibiotic Susceptibility Testing
2.4. Climate Data
2.5. Statistical Analysis
3. Results

{kind=link}
| Seasons | Climatic Factors (Weekly Averages (Range)) | ||
|---|---|---|---|
| Maximum Temperature in °C | Minimum Temperature in °C | Relative Humidity in % | |
| Early summer (mid-February to mid-April) | 34–41 | 18–28 | 55–76 |
| Late summer (mid-April to mid-June) | 33–40 | 25–29 | 64–81 |
| Early monsoon (mid-June to mid-August) | 29–36 | 25–27 | 80–97 |
| Late monsoon (mid-August to mid-October) | 30–33 | 22–27 | 73–95 |
| Early winter (mid-October to mid-December) | 26–33 | 14–24 | 63–87 |
| Late winter (mid-December to mid-February) | 28–32 | 13–18 | 57–74 |
| Weekly Average Maximum Temperature °C | Weekly Average Minimum Temperature °C | Weekly Average Relative Humidity in % | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cut-off ** | Below 33 | Above 33 | Below 24 | Above 24 | Below 78 | Above 78 | ||||||||||||
| Outcomes | Coef. | 95% CI | p | Coef. | 95% CI | p | Coef. | 95% CI | p | Coef. | 95% CI | p | Coef. | 95% CI | p | Coef. | 95% CI | p |
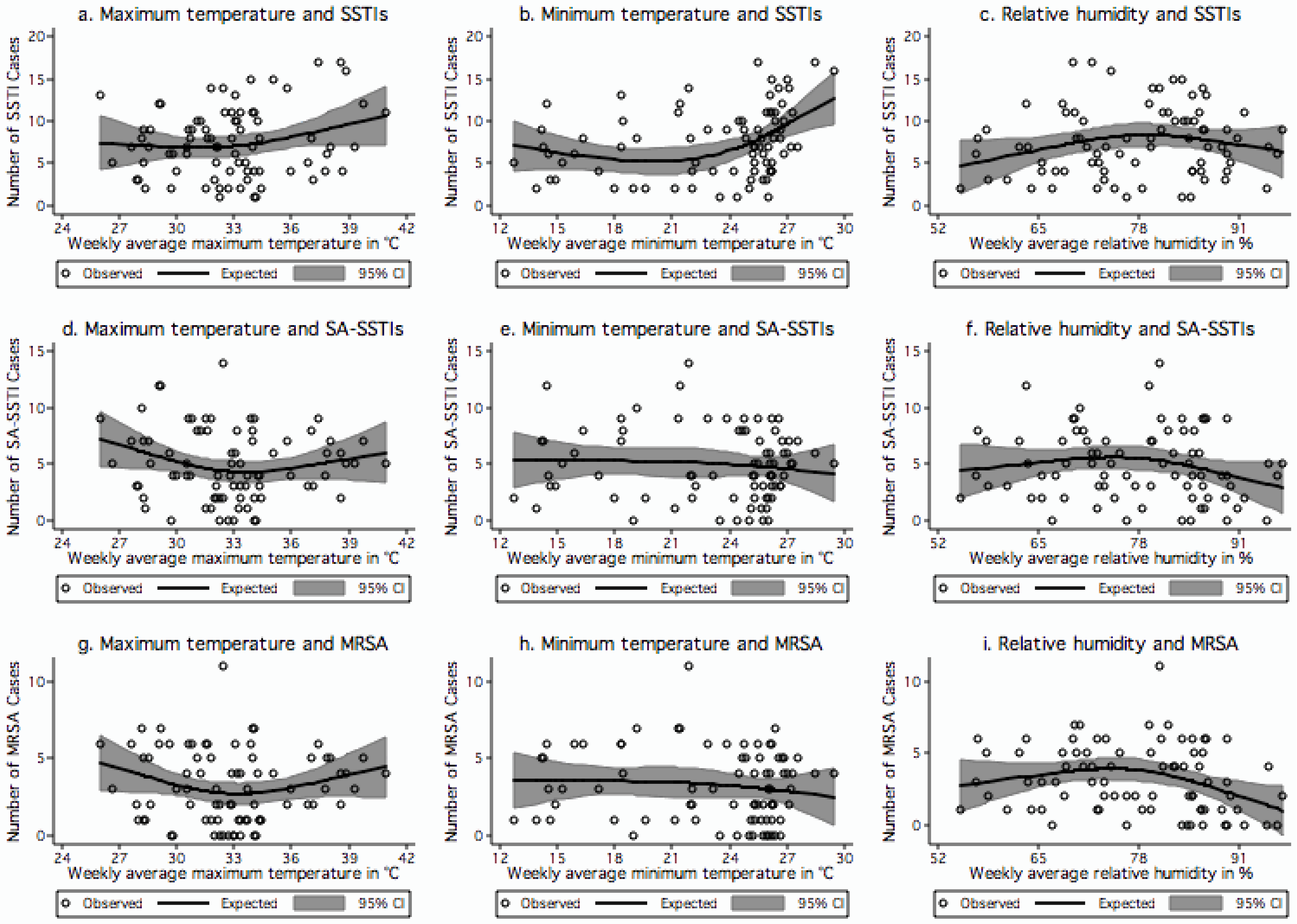
| SSTIs | −0.20 | −0.97 to 0.56 | 0.600 | 0.60 | −0.43 to 1.62 | 0.253 | −0.48 | −1.19 to 0.22 | 0.180 | 0.90 | 0.04 to 1.76 | 0.040 | 0.24 | 0.03 to 0.45 | 0.025 | −0.25 | −0.50 to 0.016 | 0.065 |
| SA-SSTIs | −0.56 | −1.14 to 0.01 | 0.056 | 0.69 | −0.02 to 1.41 | 0.058 | 0.03 | −0.69 to 0.77 | 0.919 | −0.12 | −0.95 to 0.71 | 0.781 | 0.10 | −0.06 to 0.27 | 0.228 | −0.17 | −0.37 to 0.02 | 0.078 |
| MRSA | −0.42 | −0.86 to 0.03 | 0.066 | 0.57 | 0.01 to 1.12 | 0.044 | 0.03 | −0.47 to 0.54 | 0.895 | −0.11 | −0.68 to 0.48 | 0.718 | 0.10 | −0.02 to 0.22 | 0.097 | −0.18 | −0.32 to −0.04 | 0.012 |

| Antibiotics | S. aureus | MSSA | MRSA |
|---|---|---|---|
| N = 387 (100%) | N = 136 (35%) | N = 251 (65%) | |
| Oxacillin | 251 (65) | ||
| Ampicillin/sulbactam | 143 (37) | 14 (10) | 129 (51) |
| Ceftriaxone | 276 (71) | 33 (24) | 243 (97) |
| Erythromycin | 306 (79) | 60 (44) | 246 (98) |
| Amikacin | 183 (47) | 26 (19) | 157 (63) |
| Ciprofloxacin | 236 (61) | 62 (46) | 174 (69) |
| Vancomycin | 0 (0) | 0 (0) | 0 (0) |
| Linezolid | 0 (0) | 0 (0) | 0 (0) |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Altizer, S.; Ostfeld, R.S.; Johnson, P.T.; Kutz, S.; Harvell, C.D. Climate change and infectious diseases: From evidence to a predictive framework. Science 2013, 341, 514–519. [Google Scholar]
- Braks, M.; van Ginkel, R.; Wint, W.; Sedda, L.; Sprong, H. Climate change and public health policy: Translating the science. Int. J. Environ. Res. Public Health 2014, 11, 13–29. [Google Scholar]
- Balato, N.; Megna, M.; Ayala, F.; Balato, A.; Napolitano, M.; Patruno, C. Effects of climate changes on skin diseases. Expert Rev. Anti Infect. 2014, 12, 171–181. [Google Scholar]
- Bush, K.F.; Luber, G.; Kotha, S.R.; Dhaliwal, R.S.; Kapil, V.; Pascual, M.; Brown, D.G.; Frumkin, H.; Dhiman, R.C.; Hess, J.; et al. Impacts of climate change on public health in India: Future research directions. Environ. Health Perspect. 2011, 119, 765–770. [Google Scholar]
- Muller, S.A. Climate change, dermatology and ecosystem services; trends and trade-offs. Int. J. Dermatol. 2011, 50, 504–507. [Google Scholar]
- Thong, H.Y.; Maibach, H.I. Global warming and its dermatologic implications. Int. J. Dermatol. 2008, 47, 522–524. [Google Scholar]
- Deurenberg, R.H.; Stobberingh, E.E. The evolution of Staphylococcus aureus. Infection, genetics and evolution. Infect. Genet. Evol. 2008, 8, 747–763. [Google Scholar] [CrossRef]
- Taylor, A.R. Methicillin-resistant Staphylococcus aureus infections. Prim. Care 2013, 40, 637–654. [Google Scholar]
- Mermel, L.A.; Machan, J.T.; Parenteau, S. Seasonality of MRSA infections. PLoS One 2011, 6. [Google Scholar] [CrossRef]
- Leekha, S.; Diekema, D.J.; Perencevich, E.N. Seasonality of staphylococcal infections. Clin. Microbiol. Infect. 2012, 18, 927–933. [Google Scholar]
- Grundmann, H.; Aires-de-Sousa, M.; Boyce, J.; Tiemersma, E. Emergence and resurgence of meticillin-resistant Staphylococcus aureus as a public-health threat. Lancet 2006, 368, 874–885. [Google Scholar]
- Macal, C.M.; North, M.J.; Collier, N.; Dukic, V.M.; Wegener, D.T.; David, M.Z.; Daum, R.S.; Schumm, P.; Evans, J.A.; Wilder, J.R.; et al. Modeling the transmission of community-associated methicillin-resistant Staphylococcus aureus: A dynamic agent-based simulation. J. Transl. Med. 2014, 12. [Google Scholar] [CrossRef]
- Nickerson, E.K.; Hongsuwan, M.; Limmathurotsakul, D.; Wuthiekanun, V.; Shah, K.R.; Srisomang, P.; Mahavanakul, W.; Wacharaprechasgul, T.; Fowler, V.G.; West, T.E.; et al. Staphylococcus aureus bacteraemia in a tropical setting: Patient outcome and impact of antibiotic resistance. PLoS One 2009, 4. [Google Scholar] [CrossRef]
- Tong, S.Y.; Steer, A.C.; Jenney, A.W.; Carapetis, J.R. Community-associated methicillin-resistant Staphylococcus aureus skin infections in the tropics. Dermatol. Clin. 2011, 29, 21–32. [Google Scholar] [CrossRef]
- Sahoo, K.C.; Tamhankar, A.J.; Johansson, E.; Lundborg, C.S. Antibiotic use, resistance development and environmental factors: A qualitative study among healthcare professionals in Orissa, India. BMC Public Health 2010, 10. [Google Scholar] [CrossRef]
- Sahoo, K.C.; Tamhankar, A.J.; Johansson, E.; Stalsby Lundborg, C. Community perceptions of infectious diseases, antibiotic use and antibiotic resistance in context of environmental changes: A study in Odisha, India. Health Expect. 2012, 5. [Google Scholar] [CrossRef]
- Sahoo, K.C.; Tamhankar, A.J.; Sahoo, S.; Sahu, P.S.; Klintz, S.R.; Lundborg, C.S. Geographical variation in antibiotic-resistant Escherichia coli isolates from stool, cow-dung and drinking water. Int. J. Environ. Res. Public Health 2012, 9, 746–759. [Google Scholar] [CrossRef]
- Chandy, S.J.; Michael, J.S.; Veeraraghavan, B.; Abraham, O.C.; Bachhav, S.S.; Kshirsagar, N.A. ICMR programme on Antibiotic Stewardship, Prevention of Infection & Control (ASPIC). Indian J. Med. Res. 2014, 139, 226–230. [Google Scholar]
- Raghunath, D. Emerging antibiotic resistance in bacteria with special reference to India. J. Biosci. 2008, 33, 593–603. [Google Scholar]
- The Clinical and Laboratory Standards Institute (CLSI). Performance Standard for Antimicrobial Disk Susceptibility Testing; Nineteenth informational supplement (document M100-S19) 2009; CLSI: Wayne, PA, USA, 2009. [Google Scholar]
- Kakar, N.; Kumar, V.; Mehta, G.; Sharma, R.C.; Koranne, R.V. Clinico-bacteriological study of pyodermas in children. J. Dermatol. 1999, 26, 288–293. [Google Scholar]
- Kaimal, S.; D’Souza, M.; Kumari, R.; Parija, S.C.; Sistla, S.; Badhe, B.A. Dermatitis cruris pustulosa et atrophicans revisited: Our experience with 37 patients in south India. Int. J. Dermatol. 2009, 48, 1082–1090. [Google Scholar]
- Loffeld, A.; Davies, P.; Lewis, A.; Moss, C. Seasonal occurrence of impetigo: A retrospective 8-year review (1996–2003). Clin. Exp. Dermatol. 2005, 30, 512–514. [Google Scholar]
- Koning, S.; Mohammedamin, R.S.; van der Wouden, J.C.; van Suijlekom-Smit, L.W.; Schellevis, F.G.; Thomas, S. Impetigo: Incidence and treatment in Dutch general practice in 1987 and 2001—Results from two national surveys. Br. J. Dermatol. 2006, 154, 239–243. [Google Scholar]
- Elegbe, I.A. Influence of seasonal and weather variation on the incidence of coagulase positive Staphylococci isolates among Nigerians with boil infections. J. R. Soc. Health. 1983, 103, 118–119. [Google Scholar]
- Grassly, N.C.; Fraser, C. Seasonal infectious disease epidemiology. Proc. Biol. Sci. 2006, 273, 2541–2550. [Google Scholar]
- Taplin, D.; Zaias, N.; Rebell, G. Environmental influences on the microbiology of the skin. Arch. Environ. Occup. Health 1965, 11, 546–550. [Google Scholar]
- Wang, X.; Towers, S.; Panchanathan, S.; Chowell, G. A population based study of seasonality of skin and soft tissue infections: Implications for the spread of CA-MRSA. PLoS One 2013, 8. [Google Scholar] [CrossRef]
- Hare, R.; Thomas, C.G. The transmission of Staphylococcus aureus. BMJ 1956, 2, 840–844. [Google Scholar]
- Verma, S.; Joshi, S.; Chitnis, V.; Hemwani, N.; Chitnis, D. Growing problem of methicillin resistant Staphylococci—Indian scenario. Indian J. Med. Sci. 2000, 54, 535–540. [Google Scholar]
- Mallick, S.K.; Basak, S. MRSA—Too many hurdles to overcome: A study from Central India. Trop. Dr. 2010, 40, 108–110. [Google Scholar]
- Pathak, A.; Mahadik, K.; Dhaneria, S.P.; Sharma, A.; Eriksson, B.; Lundborg, C.S. Antibiotic prescribing in outpatients: Hospital and seasonal variations in Ujjain, India. Scand. J. Infect. Dis. 2011, 43, 479–488. [Google Scholar]
- Pathak, A.; Marothi, Y.; Iyer, R.V.; Singh, B.; Sharma, M.; Eriksson, B.; Ragini, M.; Stålsby, L.C. Nasal carriage and antimicrobial susceptibility of Staphylococcus aureus in healthy preschool children in Ujjain, India. BMC Pediatr. 2010, 10. [Google Scholar] [CrossRef]
- Chen, C.J.; Huang, Y.C. New epidemiology of Staphylococcus aureus infection in Asia. Clin. Microbiol. Infect. 2014, 20, 605–623. [Google Scholar] [CrossRef]
- Pottinger, P.S. Methicillin-resistant Staphylococcus aureus infections. Med. Clin. N. Am. 2013, 97, 601–619. [Google Scholar] [CrossRef]
- McKinnell, J.A.; Miller, L.G.; Eells, S.J.; Cui, E.; Huang, S.S. A systematic literature review and meta-analysis of factors associated with methicillin-resistant Staphylococcus aureus colonization at time of hospital or intensive care unit admission. Infect. Control Hosp. Epidemiol. 2013, 34, 1077–1086. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Sahoo, K.C.; Sahoo, S.; Marrone, G.; Pathak, A.; Lundborg, C.S.; Tamhankar, A.J. Climatic Factors and Community — Associated Methicillin-Resistant Staphylococcus aureus Skin and Soft-Tissue Infections — A Time-Series Analysis Study. Int. J. Environ. Res. Public Health 2014, 11, 8996-9007. https://doi.org/10.3390/ijerph110908996
Sahoo KC, Sahoo S, Marrone G, Pathak A, Lundborg CS, Tamhankar AJ. Climatic Factors and Community — Associated Methicillin-Resistant Staphylococcus aureus Skin and Soft-Tissue Infections — A Time-Series Analysis Study. International Journal of Environmental Research and Public Health. 2014; 11(9):8996-9007. https://doi.org/10.3390/ijerph110908996
Chicago/Turabian StyleSahoo, Krushna Chandra, Soumyakanta Sahoo, Gaetano Marrone, Ashish Pathak, Cecilia Stålsby Lundborg, and Ashok J. Tamhankar. 2014. "Climatic Factors and Community — Associated Methicillin-Resistant Staphylococcus aureus Skin and Soft-Tissue Infections — A Time-Series Analysis Study" International Journal of Environmental Research and Public Health 11, no. 9: 8996-9007. https://doi.org/10.3390/ijerph110908996
APA StyleSahoo, K. C., Sahoo, S., Marrone, G., Pathak, A., Lundborg, C. S., & Tamhankar, A. J. (2014). Climatic Factors and Community — Associated Methicillin-Resistant Staphylococcus aureus Skin and Soft-Tissue Infections — A Time-Series Analysis Study. International Journal of Environmental Research and Public Health, 11(9), 8996-9007. https://doi.org/10.3390/ijerph110908996