International and National Expert Group Evaluations: Biological/Health Effects of Radiofrequency Fields


Abstract
:1. Introduction
2. Evaluations
2.1. International Organizations
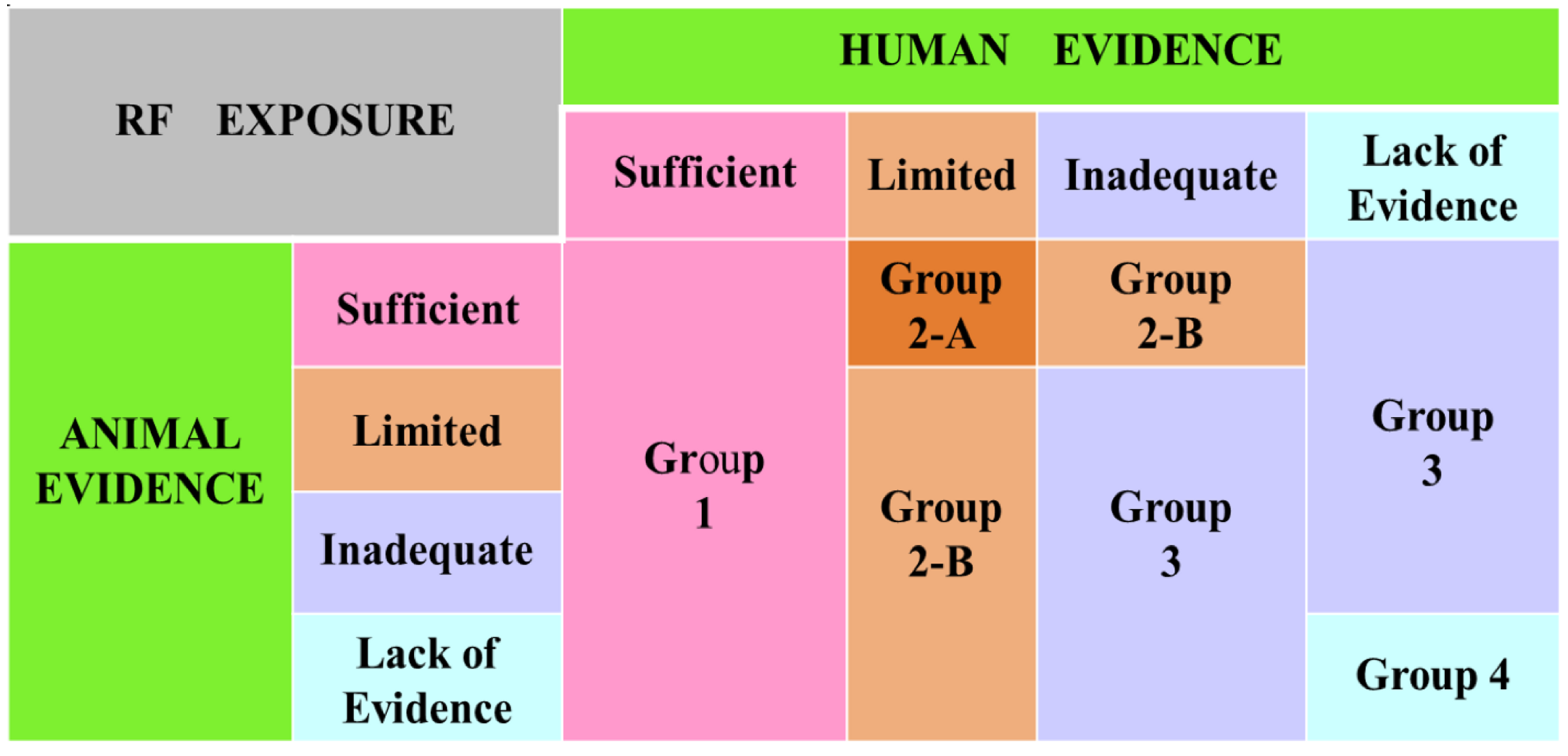
2.1.1. International Agency for Research on Cancer (IARC)

{kind=link}
| International Organization | Expert Group. Literature Evaluated. Year. | Conclusions | Recommendation | Citations (see the text for details) |
|---|---|---|---|---|
| IARC | All topics. 2011. | No increased risk for meningioma and glioma with mobile phone use. Increased risk of glioma at the highest cumulative hours of mobile phone use. Limited evidence from animal studies. Weak evidence from other relevant studies. | RF is a possible carcinogen, class 2-B. | [29] |
| IEEE | COMAR. All topics. 2009. | Public health officials should continue to use RF safety limits of international organizations. | See the text for exposure guidelines. | [40] |
| ICNIRP | All topics. 2009. | Impossible to disprove non-thermal effects. Poor evidence for chronic/low-level effects. Studies with adequate RF exposure assessment did not reveal any health-related effects. | See the text for exposure guidelines. | [42] |
| EU | SCENIHR. All topics. 2013. | No consistent evidence on cognitive function. No clear effect on neurological diseases. Unequivocal evidence on head/neck and childhood cancers. In vivo studies in animals were negative. No in vitro effects below the exposure guidelines. Uncertainties remain. | A total of 37 recommendations made for future research with high, medium and low priorities. | [45,46,47] |
| EU | EFHRAN. All topics. 2012. | No evidence for electromagnetic hypersensitivity. Limited evidence for stress response genes in vitro. Inadequate evidence for cancer and neurological diseases. | - | [49] |
| WHO | All topics. 2011. | IARC recommendation of RF as class 2-B carcinogen, a category used when a causal association is considered credible but, chance, bias or confounding factors cannot be ruled out with reasonable confidence. | Studies on long-term mobile phone use, especially among young people. | [51,52] |
| Base Stations and Accidents. 2013. | Increased traffic accidents due to mobile phone use during driving. | Further research is warranted |

2.1.2. Institute of Electrical and Electronic Engineers (IEEE)
2.1.3. International Commission on Non-Ionizing Radiation Protection (ICNIRP)
2.1.4. European Commission (SCENIHR, Scientific Committee for the Emerging and Newly Identified Health Risks)
2.1.5. European Health Risk Assessment Network (EFHRAN)
2.1.6. The World Health Organization (WHO)
2.2. National Organizations
| Country | Expert Group. Literature Evaluated. Year. | Conclusions | Recommendation | Citations (see the text for details) |
|---|---|---|---|---|
| Australia | ARPANSA. All topics. 2012–2014 | No substantiated evidence for health risk for people living near base stations. Insufficient evidence for higher risk for children. No need to reconsider exposure limits. | Precautionary approach. Reduce exposures. Use hands-free devices. | [55,56,57,58,59] |
| Belgium | Superior Health Council. All topics. 2011–2014 | No proven health risks. Long-term health risks cannot be ruled out. | Limit call numbers/time. As of March 2014, mobile phones designed for young children may not be sold in the market. | [61,62,63] |
| Canada | Health Canada. All topics. 2012–1014 | Cell phone towers are not dangerous. No evidence of adverse effects from WiFi. Since the last revision of safety code 6, no new adverse health effects have been established. | Practical measures to reduce exposures. | [65,66,67] |
| Finland | STUK. Some topics. 2008–2014 | Mobile phone use is not detrimental to health. | Precautionary measures. Not to totally prohibit children to use mobile phones. | [70,71,72,73] |
| France | ANSES. All topics. 2013 | No new proven health effects. | Limit call numbers/time for children and heavy users. | [75,76,77] |
| Germany | SSK. All topics. 2011 | Discrepancy between scientific evidence and risk perception. No overall risks. | - | [79] |
| DMF/BFS. All topics. 2011 | Risk perception is linked to media coverage. | - | [82] | |
| Julich Res Institute. Children. 2009 | No indications of adverse health effects in children. | - | [84] | |
| Latin America | All topics. 2010 | Thermal and non-thermal mechanisms were considered. Insufficient evidence for adverse health effects from in vitro and in vivo studies. | Precaution principle. Advantages of mobile Phones highlighted. | [85] |
| Netherlands | Health Council. All topics. 2009–2013 | No evidence for medically unexplained symptoms. Limited data do not indicate adverse effect on brain and health of children. Insufficient and inconsistent association of tumors in brain and other regions of head. | No reason to recommend different exposure limits for children than for adults. | [87,88,89] |
| New Zealand | NRL. All topics. 2008 | No health problems when complied with international guidelines. A matter of informed choice for children’s use. | Methods to reduce exposures. | [91,93] |
| Nordic Countries | Denmark, Finland, Iceland, Norway and Sweden. All topics. 2009–2013 | No scientific evidence for adverse health effects. If the number of fixed antennas is reduced, mobile phone will need to use higher power to maintain the connection, thereby the exposure of the general public may increase (2009). To date, do not show adverse health effects below the guidelines or limits adopted in the Nordic countries. (2013). | No need to further limit exposure from WLAN and base stations. | [95] |
| Norway | NIPH. All topics. 2012 | No evidence that weak RF fields cause adverse health effects. Uncertainty in risk assessment is small. | Precaution approach. | [97] |
| Spain | CCARS. WiFi. 2011 | To date, no scientific evidence that exposure to the low emissions levels of these systems produces adverse health effects in school children. | No reason that WiFi systems should not be used. | [99,100] |
| Sweden | SSM/SSI. All topics. 2008–2014 | Potential heating is the source for artifacts. The observed cancer risk estimates below the unity may indicate a “protective effect”. Some repetition studies were conducted. No adverse effects were reported. Most do not support earlier adverse effects. | More research is needed in children. | [102,103,105,106,107,109] |
| FAS. All topics. 2012 | Overall data do not support increased cancer risk in mobile phone users. No new interaction mechanisms. | Methods to reduce exposure levels. | ||
| Switzerland | FOEN. All topics. 2012 | No new confirmed health effects. “Absence of proof of health risks” does not automatically mean proof of their absence. | Precautionary measures. Further research. | [111] |
| Tanzania | TCRA. All topics. 2010 | No substantial evidence for harmful health effects. Many benefits of modern technology. | - | [113] |
| UK | HPA/PHE. All topics. 2012–2013 | No convincing evidence in adults or children for adverse effects below the recommended/guideline levels. Modulation has no significant role. | Further research. Methods to reduce exposures. | [115,116] |
| MTHR. All topics. 2012 | No increased cancer risk from wireless technologies. No robust evidence of harmful effects. No definite demonstrable effects in children. | No evidence for modulation effects on biological systems. | [118] | |
| IET. All topics. 2013–2014 | No new robust evidence for adverse effects. Policy makers should consider all evidence including cost and benefits of mobile phone use. | Precaution “just in case”. | [120,121] | |
| ISLE of MAN. Phone Masts/ Children. 2009 | No definite demonstrable effects on children. | Precautionary principle for mobile phone masts. | [123] | |
| USA | ACS. Cancer. 2012 | So far, no link between mobile phone use and cancer. | Further research especially in children and long term use. | [125] |
| ACS. Cell Towers. 2013 | No evidence that cell phone towers cause any health problems. | [126] | ||
| FCC. All topics. 2013 | No evidence for cancer or a variety of other problems, including headaches dizziness or memory loss | - | [128] | |
| FDA. All topics. 2012 | Studies on biological changes were not replicated. No evidence for health problems in adults, children and teenagers. | Reduce exposures. | [130,131] | |
| NCI. Cancer. 2013 | Studies have not shown a consistent link with cancers of the brain, nerves, or other tissues of the head and neck cancers. | Reduce exposures. More research, technology is changing rapidly. | [133] |
2.2.1. Australia
2.2.2. Belgium
2.2.3. Canada
2.2.4. Finland
2.2.5. France
2.2.6. Germany
2.2.6.1. Commission on Radiological Protection (SSK)
2.2.6.2. The German Mobile Telecommunication Research Program (DMF)
2.2.6.3. Jülich
2.2.7. Latin America
2.2.8. Netherlands (Health Council)
2.2.9. New Zealand
2.2.9.1. National Radiation Laboratory (NRL)
2.2.9.2. Cancer Society of New Zealand
2.2.10. Nordic Countries
2.2.11. Norway
2.2.12. Spain
2.2.13. Sweden
2.2.13.1. Swedish Radiation Safety Authority (SSM/SSI)
2.2.13.2. Swedish Research Council for Working Life (FAS)
2.2.14. Switzerland
2.2.15. Tanzania
2.2.16. United Kingdom
2.2.16.1. Health Protection Agency (Public Health England, PHE)
2.2.16.2. The Mobile Telecommunications and Health Research (MTHR)
2.2.16.3. Institute of Engineering and Technology (IET)
2.2.16.4. Isle of Man
2.2.17. United States of America
2.2.17.1. American Cancer Society (ACS)
2.2.17.2. Federal Communication Commission (FCC)
2.2.17.3. Food and Drug Administration (FDA)
2.2.17.4. National Cancer Institute (NCI)
3. Comments
4. Conclusions
Acknowledgment
Author Contributions
Conflicts of Interest
References
- Vijayalaxmi; Prihoda, T.J. Genetic damage in mammalian somatic cells exposed to radiofrequency radiation: A meta-analysis of data from 63 publications (1990–2005). Radiat Res. 2008, 169, 561–574. [Google Scholar]
- Phillips, J.L.; Singh, N.P.; Lai, H. Electromagnetic fields and DNA damage. Pathophysiology 2009, 16, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Ruediger, H.W. Genotoxic effects of radiofrequency electromagnetic fields. Pathophysiology 2009, 16, 89–102. [Google Scholar] [CrossRef] [PubMed]
- Verschaeve, L. Genetic damage in subjects exposed to radiofrequency radiation. Mutat. Res. 2009, 681, 259–270. [Google Scholar] [CrossRef]
- Verschaeve, L.; Juutilainen, J.; Lagroye, I.; Miyakoshi, J.; Saunders, R.; de Seze, R.; Tenforde, T.; van Rongen, E.; Veyret, B.; Xu, Z. In vitro and in vivo genotoxicity of radiofrequency fields. Mutat. Res. 2010, 705, 252–268. [Google Scholar] [CrossRef] [PubMed]
- Foster, K.R.; Moulder, J.E. Wi-Fi and health: Review of current status of research. Health Phys. 2013, 105, 561–575. [Google Scholar] [CrossRef] [PubMed]
- Leszczynski, D. Effects of radiofrequency-modulated electromagnetic fields on proteome. Adv. Exp. Med. Biol. 2013, 990, 101–106. [Google Scholar] [PubMed]
- Nazıroğlu, M.; Yüksel, M.; Köse, S.A.; Özkaya, M.O. Recent reports of Wi-Fi and mobile phone-induced radiation on oxidative stress and reproductive signaling pathways in females and males. J. Membr. Biol. 2013, 246, 869–875. [Google Scholar]
- Consales, C.; Merla, C.; Marino, C.; Benassi, B. Electromagnetic fields, oxidative stress, and neurodegeneration. Int. J. Cell Biol. 2012. [Google Scholar] [CrossRef]
- Marino, C.; Lagroye, I.; Scarfì, M.R.; Sienkiewicz, Z. Are the young more sensitive than adults to the effects of radiofrequency fields? An examination of relevant data from cellular and animal studies. Progr. Biophys. Mol. Biol. 2011, 107, 374–385. [Google Scholar] [CrossRef]
- Verschaeve, L. Evaluations of international expert group reports on the biological effects of radiofrequency fields. In Wireless Communication Networks—Recent Advances; Eksim, A., Ed.; In Tech: Rijeka, Croatia, 2012; pp. 523–546. [Google Scholar]
- International Committee on Non Ionizing Radiation Protection (ICNIRP). ICNIRP guidelines for limiting exposure to time-varying electric, magnetic and electromagnetic fields (up to 300 GHz). Health Phys. 1998, 74, 494–522. [Google Scholar]
- Institute of Electrical and Electronic Engineers Inc (IEEE). IEEE Standard for Safety Levels with Respect to Human Exposure to Radio Frequency Electromagnetic Fields,3 kHz to 300 GHz; IEEE: Piscataway, NJ, USA, 2006. [Google Scholar]
- International Committee on Non Ionizing Radiation Protection (ICNIRP). Exposure to High Frequency Electromagnetic Fields, Biological Effects and Health Consequences (100 kHz–300 GHz); Vecchia, P., Matthes, R., Ziegelberger, G., Lin, J., Saunders, R., Swerdlow, A., Eds.; ICNIRP: Obserschleisheim, Germany, 2009. [Google Scholar]
- International Agency for Research on Cancer. Available online: http://www.iarc.fr/ (accessed on 3 April 2014).
- International Agency for Research on Cancer. Available online: http://www.iarc.fr/en/Publications/PDFs-online/World-Cancer-Report/ (accessed on 3 April 2014).
- International Agency for Research on Cancer. Available online: http://www.monographs.iarc.fr/ENG/Classification/index.php/ (accessed on 3 April 2014).
- The INTERPHONE Study Group. Brain tumours risk in relation to mobile telephone use: Results of the INTERPHONE international case-control study. Int. J. Epidemiol. 2010, 39, 675–694. [Google Scholar]
- International Agency for Research on Cancer. Available online: http://www.iarc.fr/en/media-centre/pr/2011/pdfs/pr208_E.pdf (accessed on 3 April 2014).
- Baan, R.; Grosse, Y.; Lauby-Secretan, B.; F-El Ghissassi, F.; Bouvard, V.; Benbrahim-Tallaa, L.; Guha, N.; Islami, F.; Galichet, L.; Straif, K.; on behalf of the WHO International Agency for Research on Cancer Monograph Working Group. Carcinogenicity of radiofrequency electromagnetic fields. Lancet Oncol. 2011, 12, 424–426. [Google Scholar]
- Vijayalaxmi; Prihoda, T.J. Genetic damage in human cells exposed to non-ionizing radiofrequency fields: A meta-analysis of the data from 88 publications (1990–2011). Mutat. Res. 2012, 749, 1–16. [Google Scholar]
- Röösli, M.; Michel, G.; Kuehni, C.E.; Spoerri, A. Cellular telephone use and time trends in brain tumour mortality in Switzerland from 1969 to 2002. Eur. J. Cancer Prev. 2007, 16, 77–82. [Google Scholar]
- Inskip, P.D.; Hoover, R.N.; Devesa, S.S. Brain cancer incidence trends in relation to cellular telephone use in the United States. Neuro-Oncol. 2010, 12, 1147–1151. [Google Scholar]
- De Vocht, F.; Burstyn, I.; Cherrie, J.W. Time trends (1998–2007) in brain cancer incidence rates in relation to mobile phone use in England. Bioelectromagnetics 2011, 32, 334–339. [Google Scholar]
- Deltour, I.; Auvinen, A.; Feychting, M.; Johansen, C.; Klaeboe, L.; Sankila, R.; Schuz, J. Mobile phone use and incidence of glioma in the Nordic countries 1979–2008: Consistency check. Epidemiology 2012, 23, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Benson, V.S.; Pirie, K.; Schuz, J.; Reeves, G.K.; Beral, V.; Green, J. Mobile phone use and risk of brain neoplasms and other cancers: Prospective study. Int. J. Epidemiol. 2013, 42, 792–802. [Google Scholar] [CrossRef] [PubMed]
- Vijayalaxmi; Prihoda, T.J. Mobile phones, non-ionizing radiofrequency fields and brain cancer: Is there an adaptive response? Dose-Response 2014, 12, 509–514. [Google Scholar]
- Vijayalaxmi; Cao, Y.; Scarfi, M.R. Adaptive response in mammalian cells exposed to nonionizing radiofrequency fields: A review and gaps in knowledge. Mutat. Res. 2014, 760, 36–45. [Google Scholar]
- International Agency for Research on Cancer (IARC). IARC monographs on the evaluation of carcinogenic risks to humans. Non-ionizing radiation, part II: Radiofrequency electromagnetic fields. Lyon Fr. 2013, 102, 1–429. [Google Scholar]
- The Australian Mobile Telecommunications Association. Available online: http://www.amta.org.au/pages/ARPANSA.Response/ (accessed on 8 April 2014).
- Cancer Council Australia. Available online: http://www.CancerCouncilAustralia/au/2011/November/Reports/mobilephones/Cancer/IARC/ (accessed on 3 April 2014).
- Health Canada. Available online: http://www.Health Canada updates advice for mobile phone users/IARC/ (accessed on 4 April 2014).
- International Commission on Non-Ionising Radiation Protection. Available online: http://www.icnirp.org/documents/ICNIRP_IARC classificationRF.pdf/ (accessed on 4 April 2014).
- The Scientific Advisory Committee on Radio Frequencies and Health. Available online: http://www.ccars.es/en/news/The WHO report neither establishes nor quantifies the risk that mobile phones can produce cancer/30Nov2011/ (accessed on 4 April 2014).
- Health Protection Agency. Available online: http://www.hpa.org.uk/NewsCentre/NationalPressReleases/31May2011/PressRelease/electromagnetic fields/ (accessed on 4 April 2014).
- The American Cancer Society Pressroom. Available online: http://www.pressroom.cancer.org/index.php?s=438item=312/cell phones/ (accessed on 4 April 2014).
- National Cancer Institute. Available online: http://www.cancer.gov/newscenter//May2011/IARC/cellphones/ (accessed on 8 April 2014).
- World Health Organization. Available online: http://www.WHO/verdict/IARC/10May2011/ (accessed on 3 April 2014).
- Institute of Electrical and Electronics Engineers. Available online: http://www.ieee.org/ (accessed on 3 April 2014).
- The Committee on Man and Radiation (COMAR). COMAR technical information statement: Expert reviews on potential health effects of radiofrequency electromagnetic fields and comments on the bioinitiative report. Health Phys. 2009, 97, 348–356. [Google Scholar]
- International Commission on Non-Ionising Radiation Protection. Available online: http://www.icnirp.de/ (accessed on 12 April 2014).
- ICNIRP. International committee on non-ionizing radiation protection statement on the “guidelines for limiting exposure to time-varying electric, magnetic and electromagnetic fields (up to 300 GHz)”. Health Phys. 2009, 97, 247–258. [Google Scholar]
- Swerdlow, A.J.; Feychting, M.; Green, A.C.; Kheifets, L.; Savitz, D.A. Mobile phones,brain tumors,and the interphone study: Where are we now? Environ. Health Persp. 2011, 119, 1534–1538. [Google Scholar] [CrossRef]
- Public Health Europe. Available online: http://www.ec.europa.eu/health/scientific committees/emerging/index_en/ (accessed on 2 May 2014).
- Public Health Europe. Available online: http://www.ec.europa.eu/health/ph_risk/committees/04_scenihr/scenihr_opinions_en.html/ (accessed on 2 April 2014).
- Public Health Europe. Available online: http://www.ec.europa.eu/health/scientific_committees/emerging/docs/scenihr_2013/ (accessed on 3 April 2014).
- Public Health Europe. Available online: http://www.Scientific Committee on Emerging and newly Identified Health Risks (SCENIHR): Preliminary opinion of potential health effects of exposure to electromagnetic fields/ (accessed on 4 April 2014).
- Public Health Europe. Available online: http://www.efhran.polimi.it/docs/brochure.pdf/ (accessed on 4 April 2014).
- Public Health Europe. Available online: http://www.efhran.polimi.it/reports/ (accessed on 5 April 2014).
- World Health Organization. Available online: http://www.who.int/ (accessed on 5 April 2014).
- World Health Organization. Available online: http://www.who.int/mediacentre/factsheets/en/fs193/June2011/ (accessed on 5 April 2014).
- World Health Organization. Available online: http://www.who.int/features/qa/30/en/2013/ (accessed on 5 April 2014).
- The Australian Mobile Telecommunications Association. Available online: http://www.arpansa.gov.au/ (accessed on 2 April 2014).
- The Australian Mobile Telecommunications Association. Available online: http://www.arpansa.gov.au/eme-series.pdf/ (accessed on 3 April 2014).
- The Australian Mobile Telecommunications Association. Available online: http://www.arpansa.gov.au/pubs/eme/fact1.pdf: updated in 2012/ (accessed on 8 April 2014).
- The Australian Mobile Telecommunications Association. Available online: http://www.arpansa.gov.au/pubs/eme/fact4.pdf: updated in 2012/ (accessed on 8 April 2014).
- The Australian Mobile Telecommunications Association. Available online: http://www.arpansa.gov.au/pubs/eme/fact9.pdf: updated in 2012/ (accessed on 8 April 2014).
- The Australian Mobile Telecommunications Association. Available online: http://www.arpansa.gov.au/pubs/eme/fact11.pdf; updated in 2013/ (accessed on 8 April 2014).
- The Australian Mobile Telecommunications Association. Available online: http://www.arpansa.gov.au/Technical Report164/2014.pdf/ (accessed on 4 April 2014).
- Federal Public Service Health, Food Chain Safety and Environment. Available online: http://www.health.fgov.be/eportal?fodnlang=en/ (accessed on 3 April 2014).
- Federal Public Service Health, Food Chain Safety and Environment. Available online: http://www.health.fgov.be/eportal/Environment/Electromagnetic_fields/...sensible mobile phone use/ (accessed on 4 April 2014).
- Federal Public Service Health, Food Chain Safety and Environment. Available online: http://www.health.fgov.be/eportal/Environment/Electromagnetic_fields/June/2011–2014/ (accessed on 4 April 2014).
- Emfacts Consultancy. Available online: http://www.emfacts.com/2014/03/the-belgian-government-has-announced/2014/ (accessed on 5 April 2014).
- Health Canada. Available online: http://www.hc-sc.gc.ca/ (accessed on 11 April 2014).
- Health Canada. Available online: http://www.hc-sc.gc.ca/radiaiton/environment/workplace/health/2012/2013/Jan2014/ (accessed on 12 April 2014).
- Health Canada. Available online: http://www.hc-sc.gc.ca/ewh-semt/radiation/cons/wifi/index-eng.php/Feb2014/ (accessed on 6 April 2014).
- The Royal Society of Canada. Available online: http://www.rsc-src.ca/sites/default/files/pdf/SC6_Report/2014/pdf/ (accessed on 12 April 2014).
- Radiation and Nuclear Safety Authority. Available online: http://www.stuk.fi/en_GB/ (accessed on 11 April 2014).
- Radiation and Nuclear Safety Authority. Available online: http://www.finland/mobile phones pose no health risk/2007/ (accessed on 12 April 2014).
- Karinen, A.; Heinävaara, S.; Nylund, R.; Leszczynski, D. Mobile phone radiation might alter protein expression in human skin. BMC Genomics 2008. [Google Scholar] [CrossRef]
- Radiation and Nuclear Safety Authority. Available online: http://www.Statement of STUK concerning mobile phones and health/January 7,2009/pdf/ (accessed on 2 May 2014).
- Radiation and Nuclear Safety Authority. Available online: http://www.Statement of STUK concerning mobile phones and health/2013/pdf/ (accessed on 2 May 2014).
- Radiation and Nuclear Safety Authority. Available online: http://www.Statement of STUK concerning mobile phones and health/2014/pdf/ (accessed on 2 May 2014).
- French Agency for Food, Environment and Occupational Health and Safety. Available online: http://www.afsset/anses/fr/ (accessed on 2 May 2014).
- French Agency for Food, Environment and Occupational Health and Safety. Available online: http://www.afsset.fr/upload/bibliotheque/9Rapport_RF_20_151009_l.pdf/ (accessed on 1 May 2014).
- French Agency for Food, Environment and Occupational Health and Safety. Available online: http://www.French agency for Food,Environment and Occupational Health and Safety/ANSES/mobile-telephony/1october2013.pdf/ (accessed on 1 May 2014).
- French Agency for Food, Environment and Occupational Health and Safety. Available online: http://www.ssk.de/EN/Home/home_node.html/ (accessed on 26 April 2014).
- The German Commission on Radiological Protection. Available online: http://www.SSK/ (accessed on 21 April 2014).
- The German Commission on Radiological Protection. Available online: http://www.SSK/ Evidence of Cancer Risks/Electromagnetic Fields/2011/pdf/ (accessed on 21 April 2014).
- German Mobile Telecommunication Research Programme. Available online: http://www.emfforschungsprogramm.de/ (accessed on 22 April 2014).
- German Federal Office for Radiation Protection. Available online: http://www.Bundesambt für Strahlenschutz/BfS/ (accessed on 23 April 2014).
- The German Commission on Radiological Protection. Available online: http://www.ssk/biological effects of mobile phone use-An overview/2011/pdf/ (accessed on 29 April 2014).
- Juelich Research Center. Available online: http://www.fz-juelich.de/ (accessed on 30 April 2014).
- Juelich Research Center. Available online: http://www.juwel.fz-juelich.de:8080/.../bitstream/2128/3683/1/Gesundheit_16.pdf/ (accessed on 30 April 2014).
- Latin American Science. Available online: http://www.wireless-health.org.br/downloads/LatinAmericanScienceReviewReport.pdf/ (accessed on 30 April 2014).
- The Health Council of The Netherland. Available online: http://www.gr.nl/en/about-us/health-council/ (accessed on 29 April 2014).
- The Health Council of The Netherland. Available online: http://www.gezondheidsraad.nl/sites/default/files/2009.pdf/ (accessed on 29 April 2014).
- The Health Council of The Netherland. Available online: http://www.Health Council of the Netherlands. Influence of radiofrequency telecommunication signals on children’s brains. The Hague: Health Council of the Netherlands,2011; publication no. 2011/20E/pdf/ (accessed on 30 April 2014).
- The Health Council of The Netherland. Available online: http://www.Health Council of the Netherlands. Mobile phones and cancer. Part 1: Epidemiology of tumours in the head. The Hague: Health Council of the Netherlands, 2013; publication no. 2013/11.pdf/ (accessed on 30 April 2014).
- National Center for Radiation Science. Available online: http://www.National Centre for Radiation Science/New Zealand/ (accessed on 4 April 2014).
- National Center for Radiation Science. Available online: http://www.nrl.nz.gov/Information Sheet_IS_21_Revised August 2008.pdf/ (accessed on 3 May 2014).
- Cancer Society of New Zealand. Available online: http://www.cancernz.org/nz/ (accessed on 4 May 2014).
- Cancer Society of New Zealand. Available online: http://www.cancernz.org.nz/.../IS_Mobiles&Cancer_June2010.pdf/ (accessed on 2 May 2014).
- Nordic Radiation Safety Authority. Available online: http://www.stralsakerhetsmyndigheten.se/.../2009/091116norden-emf.pdf/ (accessed on 2 May 2014).
- Nordic Radiation Safety Authority. Available online: http://www.Exposure from mobile phones, base stations and wireless networks/statement by the Nordic radiation safety authorities/17Dec2013.pdf/ (accessed on 2 May 2014).
- Norwegian Institute of Public Health. Available online: http://www. Norwegian_Institute_of_Public_Health.org/ (accessed on 30 April 2014).
- Norwegian Institute of Public Health. Available online: http://www. Low-level radiofrequency electromagnetic fields-an assessment of health risks and evaluation of regulatory practice.pdf/ (accessed on 30 April 2014).
- The Scientific Advisory Committee on Radio Frequencies and Health. Available online: http://www.comité cientifico asesor en radio-frecuencias y salud/ccars/ (accessed on 29 April 2014).
- The Scientific Advisoty Committee on Radio Frequencies and Health. Available online: http:// www.ccars.es/docs/informes/INFORME%20CCARS%202007-2008.pdf/ (accessed on 29 April 2014).
- The Scientific Advisory Committee on Radio Frequencies and Health. Available online: http://www.ccars.es/en/news/there-no-scientific-evidence-wifi-systems-produce-adverse-health-effects-schoolchildren/30Nov2011/ (accessed on 29 April 2014).
- Swedish Radiation Safety Authority. Available online: http://www.stralsakerhetsmyndigheten.se/In-English/ (accessed on 3 April 2014).
- Swedish Radiation Safety Authority. Available online: http://www.stralsakerhetsmyndigheten.se/Global/Publikationer/Rapport/Stralskydd/2008/ssi-rapp-2008–12.pdf/ (accessed on 3 April 2014).
- Swedish Radiation Safety Authority. Available online: http://www.Recent Research on EMF and Health Risks. Sixth annual report/Swedish radiation safety authority/independent Expert Group on Electromagnetic Fields/2009:36/pdf/ (accessed on 3 April 2014).
- Kundi, M. The controversy about a possible relationship between mobile phone use and cancer. Environ. Health Persp. 2009, 117, 316–324. [Google Scholar] [CrossRef]
- Swedish Radiation Safety Authority. Available online: http://www.Recent Research on EMF and Health Risks. Seventh annual report/Swedish radiation safety authority/independent Expert Group on Electromagnetic Fields/2010:44/pdf/ (accessed on 2 April 2014).
- Swedish Radiation Safety Authority. Available online: http://www.stralsakerhetsmyndigheten.se/Global/Publikationer/Rapport/Stralskydd/2013/SSM-Rapport-2013–19.pdf/ (accessed on 2 April 2014).
- Swedish Radiation Safety Authority. Available online: http://www.stralsakerhetsmyndigheten.se/Global/Publikationer/Rapport/Stralskydd/2014/SSM-Rapport-2014–16.pdf/ (accessed on 2 April 2014).
- Swedish Research Council for Health, Working Life and Welfare. Available online: http://www. Swedish Research Council for Working Life.org/ (accessed on 3 April 2014).
- Swedish Research Council for Health, Working Life and Welfare. Available online: http://www.Swedish Research Council for Working Life and Social Research/orderNo.2012-003/pdf/ (accessed on 3 April 2014).
- Federal Office for the Environment. Available online: http://www.Federal Office for the Environment/FOEN/Switzerland.org/ (accessed on 2 April 2014).
- Federal Office for the Environment. Available online: http://www.bafu.admin.ch/publikationen/publikation/01739/index.html?lang=en; Abstract/ (accessed on 2 April 2014).
- Tanzania Communications Regulatory Authority. Available online: http://www.Tanzania Communications Regulatory Authority.org/ (accessed on 2 April 2014).
- Tanzania Communications Regulatory Authority. Available online: http://www.tcra.go.tz/images/headlines/radiationPressReleaseEng.pdf/ (accessed on 2 April 2014).
- Health Protection Agency. Available online: http:// www.hpa.org.uk/ (accessed on 2 April 2014).
- Health Protection Agency. Available online: http://www.hpa.org.uk/webw/HPAweb&HPAwebStandard/HPA/1317133826368/2012/ (accessed on 2 April 2014).
- Health Protection Agency. Available online: http://www.hpa.org.uk/webw/HPAweb&HPAwebStandard/HPAweb/2013 (accessed on 2 May 2014).
- Mobile Telecommunication and Health Research. Available online: http://www.mthr.org.uk/ (accessed on 3 April 2014).
- Mobile Telecommunication and Health Research. Available online: http://www.mthr.org.uk/documents/MTHRreport2012.pdf/ (accessed on 8 April 2014).
- Institute of Engineering and Technology. Available online: http://www.theiet.org/ (accessed on 3 April 2014).
- Institute of Engineering and Technology. Available online: http://www.theiet.org/factfiles/bioeffects/emf-position-page/2013.cfm?type=pdf/ (accessed on 3 April 2014).
- Institute of Engineering and Technology. Available online: http://www.theiet.org/factfiles/bioeffects/emf-position-page/2014.cfm?type=pdf/ (accessed on 8 April 2014).
- Isle of Man. Available online: http://www.isle_of_man.org/ (accessed on 8 April 2014)).
- Isle of Man. Available online: http:www.gov.im/lib/docs/cso/mobilephonemastscominreport.pdf/ (accessed on 7 April 2014).
- American Cancer Society. Available online: http:www.cancer.org/ (accessed on 10 April 2014).
- American Cancer Society. Available online: http:www.cancer.org/cancer/cancercauses/othercarcinogens/athome/cell-phones/2012/ (accessed on 10 April 2014).
- American Cancer Society. Available online: http:www.cancer.org/cancer/cancercauses/othercarcinogens/athome/cellular-phone-towers/2013/ (accessed on 11 April 2014).
- Federal Communications Commission. Available online: http:www.fcc.org/ (accessed on 12 April 2014).
- Federal Communications Commission. Available online: http:www.fcc.gov/encyclopedia/faqs-wireless-phones/ (accessed on 12 April 2014).
- Food and Drug Administration. Available online: http:www.fda.org/ (accessed on 13 April 2014).
- Food and Drug Administration. Available online: http:www.fda.gov/Radiation-EmittingProducts/Health Issues/Cell Phones/2012/ (accessed on 13 April 2014).
- Food and Drug Administration. Available online: http:www.fda.gov/Radiation-EmittingProducts/Children and Cell phones/2012/ (accessed on 14 April 2014).
- American Cancer Society. Available online: http:www.cancer.gov/ (accessed on 15 April 2014).
- American Cancer Society. Available online: http:www.cancer.gov/cancertopics/factsheet/Risk/cellphones/2013/ (accessed on 15 April 2014).
- Wiedemann, P.M.; Boerner, F.U.; Repacholi, M.H. Do people understand IARC’s 2B categorization of RF fields from cell phones? Bioelectromagnetics 2014, 35, 373–378. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Available online: http:www.who.int/mediacentre/factsheets/en/fs193/June2011/ (accessed on 4 April 2014).
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Vijayalaxmi; Scarfi, M.R. International and National Expert Group Evaluations: Biological/Health Effects of Radiofrequency Fields. Int. J. Environ. Res. Public Health 2014, 11, 9376-9408. https://doi.org/10.3390/ijerph110909376
Vijayalaxmi, Scarfi MR. International and National Expert Group Evaluations: Biological/Health Effects of Radiofrequency Fields. International Journal of Environmental Research and Public Health. 2014; 11(9):9376-9408. https://doi.org/10.3390/ijerph110909376
Chicago/Turabian StyleVijayalaxmi, and Maria R. Scarfi. 2014. "International and National Expert Group Evaluations: Biological/Health Effects of Radiofrequency Fields" International Journal of Environmental Research and Public Health 11, no. 9: 9376-9408. https://doi.org/10.3390/ijerph110909376
APA StyleVijayalaxmi, & Scarfi, M. R. (2014). International and National Expert Group Evaluations: Biological/Health Effects of Radiofrequency Fields. International Journal of Environmental Research and Public Health, 11(9), 9376-9408. https://doi.org/10.3390/ijerph110909376