3.1. Primary Data Source
We used data from the 2003–2004 Community Tracking Study (CTS) Household Survey. The data collection started in February 2003 and was completed in February 2004. The Household Survey contains information from approximately 46,587 individuals in 25,419 families. The individuals ages 16 and older, and represents the national civilian, non-institutionalized population who live in the United States. Non-institutionalized population are individuals who are not in a institution (criminal, mental, or other types of facilities) or an active duty military personnel. The sample is clustered in 60 CTS sites: 51 metropolitan areas and nine nonmetropolitan areas, which were randomly selected to form the core CTS and to be representative of the nation as a whole. The survey was administered by telephone, using computer-assisted telephone interviewing technology. Majority of respondents were selected through list-assisted random-digit-dialing. The CTS Household Survey is the last data with a large sample population and was replaced by the Health Tracking Household Survey (HTHS) with the sample size of 17,797 (16,671) individuals in 9407 (9165) families in 2007 (2010). Both 2007 and 2011 HTHSs focuses on only 12 metropolitan areas unlike, the CTS Household Survey 2003–2004: 51 metropolitan areas and 9 nonmetropolitan areas. The CTS Household Survey 2006 was created before the Medicare prescription program started in 2006. This study reveals the relationship between unmet prescription drugs, perceived delay in healthcare, and unmet needed healthcare. In addition, it evaluates the effect of unmet prescription drug on health before the Medicare prescription program.
The Household Survey instruments covered a large variety of topics including: health insurance, use of health services, and satisfaction with care, health status, and certain demographic information. A family informant provided information on insurance coverage, health resource use, usual source of care, and the general health status of all family members. The informant also provided information on family income, employment, earnings, employer-offered insurance plan, and race/ethnicity of all adult family members. Each adult in the family answered questions from a self-response module that covered the issues of unmet needs, patient trust, satisfaction with physician choice, risky behaviors such as smoking, and the last visit to a doctor.
3.2. Dependent Variables: Measures of Delayed Healthcare and Unmet Needs
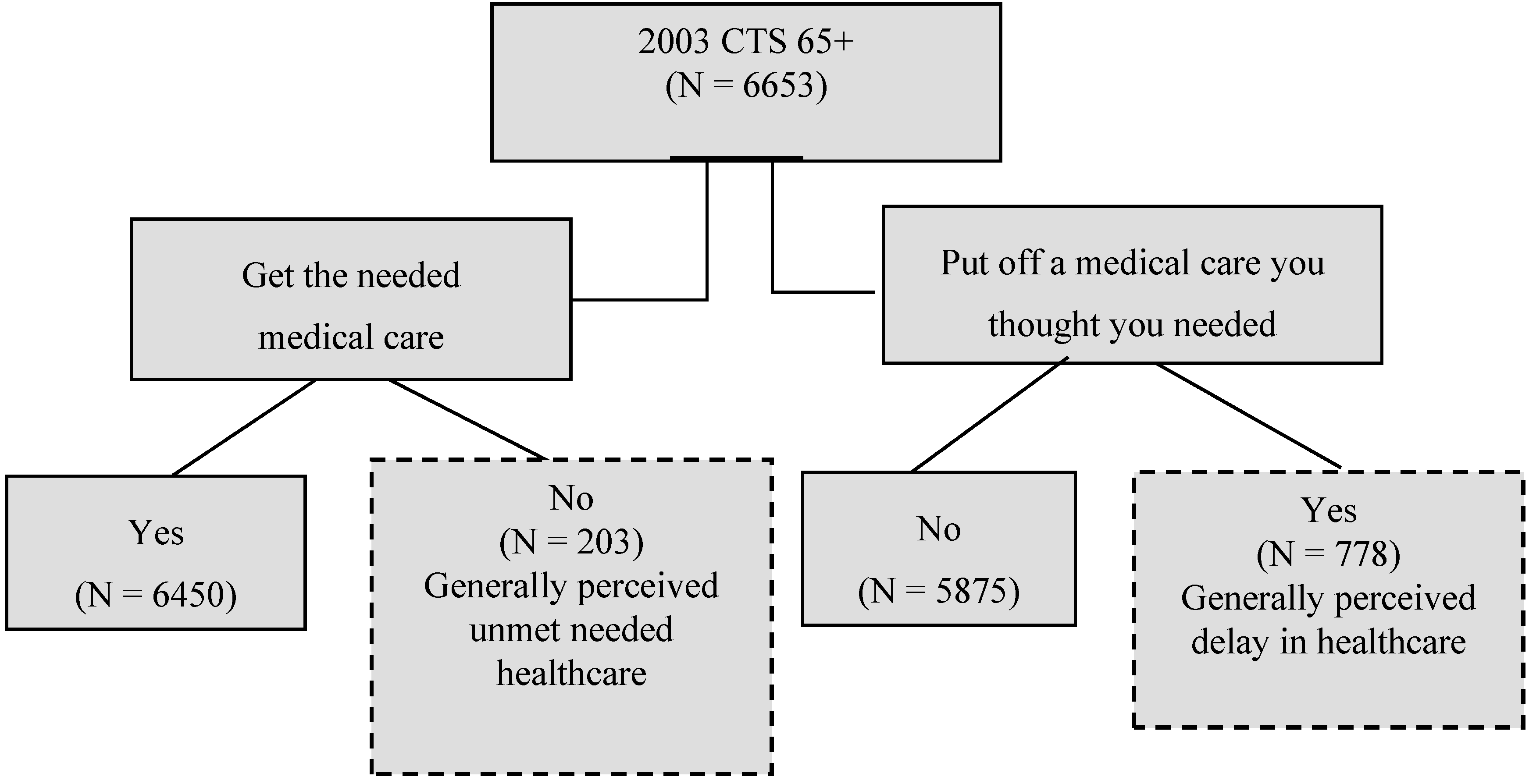
In this study, healthcare accessibility is divided into two dimensions: the general perceived delayed healthcare and unmet healthcare needs. Capturing generally perceived delayed healthcare, the survey included the question, “Was there any time during the past 12 months when you put off or postponed getting medical care you though you needed?” This study then evaluated the different influences of enabling, predisposing, and reinforcing factors on this perceived delay in care. The question about generally perceived unmet needs was “During the past 12 months, was there any time when you didn’t receive the medical care you needed?” However, the information does not provide any information on specific illnesses or conditions. The respondent either recognizes the existence of a health problem or perceives needed care sometime in the near future. The same survey item is used to measure unmet needs [
10]. If the response is “yes,” this implies that the person did not get the medical care that he or she needed (see
Table 1 and
Figure 1). It is measured by patient perceptions of disability, symptom, and diagnoses [
28].
Table 1.
Definitions and Characteristics of Delayed Healthcare, and Unmet Needed Healthcare (aged 65 and over).
Table 1.
Definitions and Characteristics of Delayed Healthcare, and Unmet Needed Healthcare (aged 65 and over).
| Dependent Variables and Definitions | Objectives |
|---|
| Generally perceived delay in healthcare a | |
| Was there ever a time during the past 12 months when you put off or postponed getting medical care you thought you needed? | Evaluate the different influences of enabling, predisposing, and reinforcing on generally perceived delayed care. |
| Generally perceived unmet needed healthcare a | |
| During the past 12 months, was there ever a time when you did not receive the medical care you needed? | Evaluate the different influences of enabling, predisposing, and reinforcing on generally perceived unmet medical needs. |
| Actual unmet needed healthcare a | |
| During the past 12 months, did you see a doctor to treat this problem (most recent health problem for which you did not receive or delayed receiving medical care)? | Compare different behavioral differences between generally perceived unmet needs and actual unmet needs. |
| Evaluated delayed healthcare (adherence) a | |
| Did you see a specialist, get tests, or have a procedure or surgery (If care was delayed, did you put off seeing a specialist or getting tested or getting the procedure or having the surgery)? | Examine the effects of delayed care. Focus more on physician assessments of symptoms and diagnoses. |
Figure 1.
Self-reported generally perceived delay in healthcare and generally perceived unmet needed healthcare: Individuals aged 65 or older in the Community Tracking Survey.
Figure 1.
Self-reported generally perceived delay in healthcare and generally perceived unmet needed healthcare: Individuals aged 65 or older in the Community Tracking Survey.
It is crucial to understand that unmet healthcare and delayed care needs are different concepts [
9]. In our analysis, four dimensions of healthcare components were evaluated: generally perceived unmet needs, generally perceived delayed healthcare, actual unmet needs, and evaluated delayed healthcare. For generally perceived delayed care, the logical expectation is that self-perceived delayed care at least once in the past twelve months is experienced by putting off the care as displayed in
Table 1 and
Figure 1. For actual delayed care, a respondent did not receive care after the new occurrence of a specific symptom. Evaluated delayed care is closely related to the kind and amount of treatment that will be provided after a respondent has presented to a medical provider [
22,
28] as shown in
Table 1. The respondent has postponed receiving treatment from a specialist after obtaining a referral from a regular doctor, put off taking a test in spite of the doctor’s recommendation, or deferred having a procedure/surgery in spite of a doctor’s orders. Thus, the evaluated delayed care possibly captures some aspect of adherence. The dimension represents the evaluated side of needs, focusing more on professional assessment of symptoms and diagnoses [
28].
3.3. Empirical Framework: PP Model
The line of research on health behavior and its policy implications originated from the PRECEDE-PROCEED model (PP model) [
29,
30,
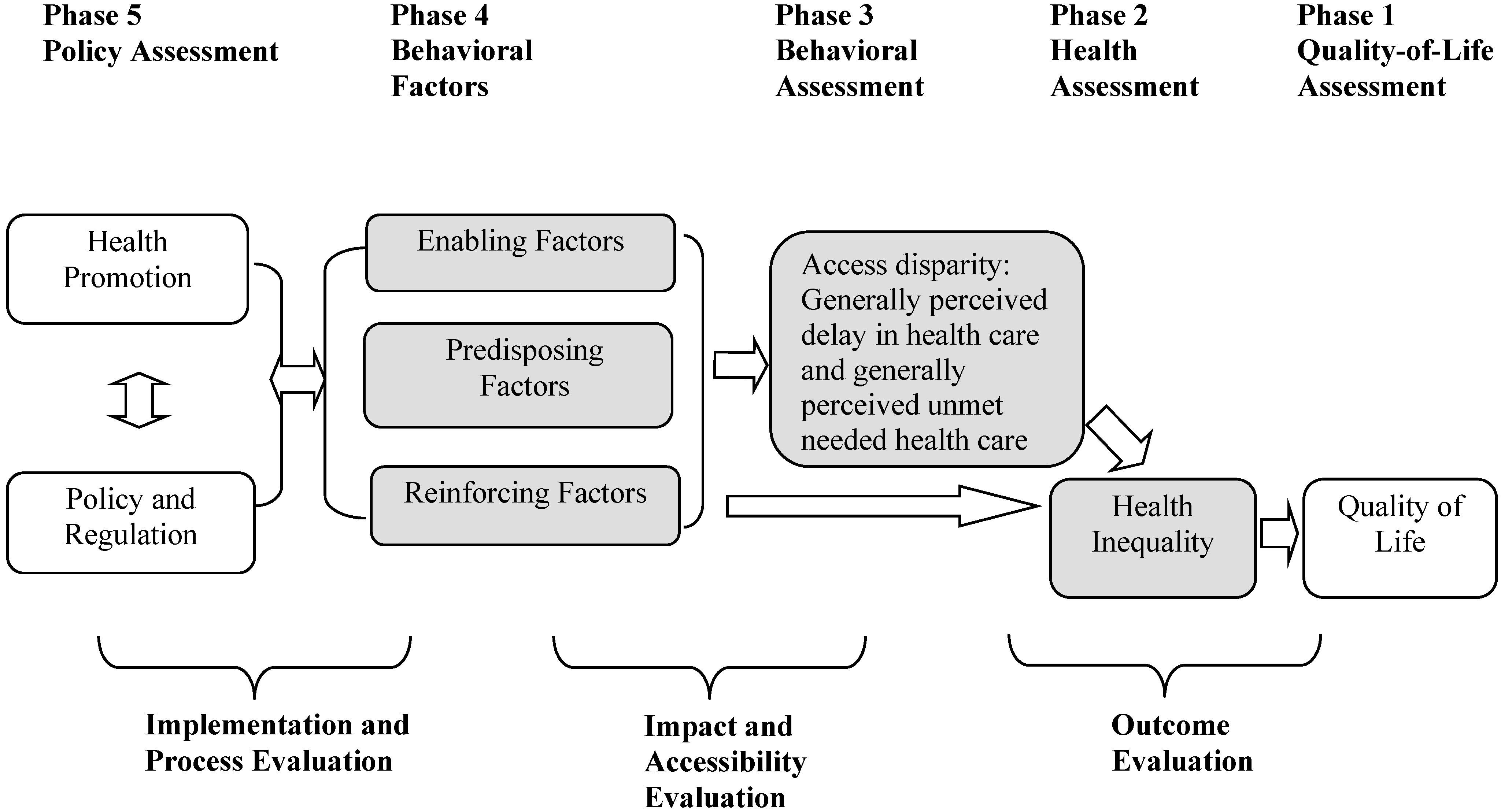
31]. This offers some concepts and analytical tools to help analyze access disparity and health inequality by using the U.S. Household Survey of the Community Tracking Study. The study applies the PP model to evaluate behavioral characteristics for delayed care, unmet needs, and health inequality between Phases 2 and 4 (
Figure 2). Phases 1–5 show the assessment of the PP model in
Figure 2. The focus of this study is to assess three categories of influential behavioral factors (enabling, predisposing, and reinforcing factors) by controlling socio-demographic factors in Phase 4 and by evaluating their behavioral influences on delayed care and unmet needs in Phase 3. Phase 5, the policy assessment section, represents the assessment of health promotion, and government policy and regulation on healthcare financing and delivery.
Individual delayed healthcare and unmet needs healthcare can be attributed to the quantity and quality of physical and environmental domains, which can affect health inequality, as well as quality of life. Enabling factors include: access to healthcare services, availability of recourses, and referrals to appropriate healthcare providers, for example income, healthcare financing (out-of-pocket healthcare costs, Medicare HMO, Medicare Supplementary Medical Insurance, and Medicaid), and available methods of healthcare services [
30]. Predisposing factors encourage active traits and include: educational level, knowledge, attitude, beliefs, perception, values, culture,
etc. Attributable to knowledge by higher education, health illiteracy and skills in health information seeking, individuals know how to evaluate quality of health and healthcare [
30]. Reinforcing factors are comprised of the different types of feedback, such as the rewards of a particular behavior change made by those in the target population, for example family, marital status, friend, teachers, etc [
30].
The PP model offers some concepts and analytical tools that help analyze policy influences on behavioral decisions (see bottom of
Figure 2) by using influential factors in Phase 4 within the framework of the PP model. This study assumes that delayed care and unmet needs are measurable as a flow per unit of time because delayed care and unmet needs encompass heterogeneous needs, such as routine, preventative physician care, specialty physician services, acute care, dental care, mental care, and health educational services.
Figure 2.
Application of PRECEDE-PROCEED Model to examine generally perceived delay in health care and generally perceived unmet needed health care.
Figure 2.
Application of PRECEDE-PROCEED Model to examine generally perceived delay in health care and generally perceived unmet needed health care.
Note: See the adaptation of a model by Green and Kreuter [
30].
The study assumes that the health inequality in Phase 2 (
Figure 2) is attributed to healthcare service use behavior based on his or her delayed care (DELAY) and unmet needs (UNMET) in Phase 3. This is influenced by socio-demographic factors, as well as predisposing, reinforcing, and enabling factors in Phase 4. Individuals with delayed care and unmet needs are evaluated. A functional behavioral model in Phases 3 and 4 could be expressed as follows:
Equations (1) and (2) represent the relationship between the health behavioral choice of individual “
i” and a person with delayed care and unmet needs in Phases 3 in
Figure 2. Factors will influence an individual’s delayed care, and ω
DELAY is an unobserved error, generally assumed to satisfy E(ω
DELAY|
EN,
PR,
RE,
SD) = 0. ω
UNMET is an unobserved error, generally assumed to satisfy E(ω
UNMET|
EN,
PR,
RE,
SD) = 0.
Both delayed healthcare (DELAY) and unmet healthcare needs (UNMET) consist of enabling (EN), predisposing (PR), reinforcing (RE), and socio-demographic factors (SD) that will influence healthcare disparity of the elderly. The study incorporates the extended PP Model to observe health inequality and the influential determinants.
In our estimation, enabling factors include income, health insurance related aspects, price of healthcare expenditures (out-of-pocket expenditures), usual source of care, and time related accessibility measures. This study analyzes a variety of health insurance aspects to fill the gap in literature. In order to capture coverage and managed care cost saving aspects, this study includes Medicare HMO, private health insurance with HMO, and Medicare Supplementary Medical Insurance [
25,
32,
33]. In addition to the price of healthcare services, an individual’s income level affects the living standard which contributes to unmet needs and delayed care and, in turn, health outcome [
34]. Low income, minority populations received less healthcare than the wealthier population, who has a higher probability of obtaining healthcare when they need it [
35]. Various components, as well as the amount of time invested in health services by using usual source of care and time input for accessibility to healthcare services, also influences an individual’s health status through enabling factors as seen in
Table 1 [
21].
Predisposing factors are education as a substitute for knowledge, patient trust, patient satisfaction, patient-provider communication, and lifestyle risk. The educational level as knowledge is associated with unmet needs and delayed care. Higher education levels affect health capital development and increase efficiency in health status. Years of education represent health capital related to health knowledge, allowing individuals to make better behavioral decisions, which is related to educational attainment [
36]. Another barrier to obtaining needed care without delay may be lack of knowledge of the importance of seeing a referred specialist, of getting the recommended test, or receiving proper procedure [
37].
There has been a dramatic increase in the interest of measuring patients’ trust in their physicians. Trust is a defining element in any interpersonal relationship and it is particularly central to the patient-provider relationship [
38]. Any consideration of the patients’ interpersonal trust in physicians must take into account the general atmosphere in healthcare institutions. Although evidence shows that the majority of patients continue to trust their physicians and health information, concern is growing over the rapid and far-reaching changes in the healthcare system, which have placed great pressure on that trust and may undermine it [
39]. The new concerns about patient trust has triggered a recognition that there needs to be a better understanding of the role of trust in a patient-physician relationship and health information, and the relationship between trust and health outcomes.
An increasingly important role in the provision of clinical process and outcomes are related to patient satisfaction through service improvements in nursing homes, hospitals, and clinics. The scope of patient satisfaction includes physician’s inpatient care, primary care services, patient-perceived nurse care, waiting time for services at clinics,
etc. [
40]. Patient satisfaction not only depends on services from healthcare providers but also varies by anxiety level of patient, mental status of patient, and geographic correlation with physician [
41,
42].
The relationship between patients and their physicians is influenced by lack of cultural competence of physicians to improve communication with patients, lack of knowledge about procedural issues, inconsistencies of recommendation guidelines to patients, lack of physicians’ encouragement of patients’ interest, lack of evidence for benefit from patients’ health insurance coverage, and failure to call back patients for screening. These are all barriers that stem, in part, from the communication between patients and physicians [
43,
44], and inevitably hinder a patient’s incentive to decrease unmet needs and delayed care. Thus efforts to improve unmet/met needs and delayed care should focus at least in part on improving patient-provider communication. The possible role of health communication between patients and physicians with unmet/met needs and delayed care has recently received greater attention. Health communication is the art and technique of informing, influencing, and motivating individual, institutional, and public audiences about important health issues. Quality oriented communication between patients and their physicians is related to patients’ awareness of unmet needs and delayed care. A lack of communication between a patient and a healthcare provider can lead to serious problems (e.g., chance of survival).
In socio-demographic factors, behavioral aspects of choosing unmet/met needs and delayed care in relation to maintaining good health, use healthcare services which vary by the factors that include age, gender, race/ethnicity, and poverty level. In socio-demographic factors, an individual’s health status based on subjective health is included in a base specification without making a health index because of the lack of ADL objective measurements [
45,
46]. Estimation is an alternative specification without a health status variable. An underlying factor in the discussion above implies that the estimated coefficient on unmet needs and delayed care would be an upward biased estimate of the true impact of these variables, assuming that individual health status variables are omitted. The results would be biased.




 and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}



