
Elevated Serum Bisphenol A Level in Patients with Dilated Cardiomyopathy

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Sample Collection
2.3. Sex Hormone Measurement
2.4. BPA Elisa Measurement
2.5. Statistical Analyses
3. Results

{kind=link}
| Variable | DCM (n = 88) | Control (n = 88) | p Value |
|---|---|---|---|
| Age, years | 59.6 ± 13.2 | 59.0 ± 12.7 | 0.767 |
| Male, n (%) | 59 (67%) | 55 (63%) | 0.318 |
| Variables | Total (Mean ± SD) | Male (Mean ± SD) | Female (Mean ± SD) | |||
|---|---|---|---|---|---|---|
| DCM (n = 88) | Controls(n = 88) | DCM (n = 59) | Controls(n = 55) | DCM (n = 29) | Controls (n = 33) | |
| Age (years) | 59.6 ± 13.2 | 59.0 ± 12.7 | 58.0 ± 14.3 | 56.7 ± 14.0 | 62.7 ± 10.4 | 62.8 ± 9.2 |
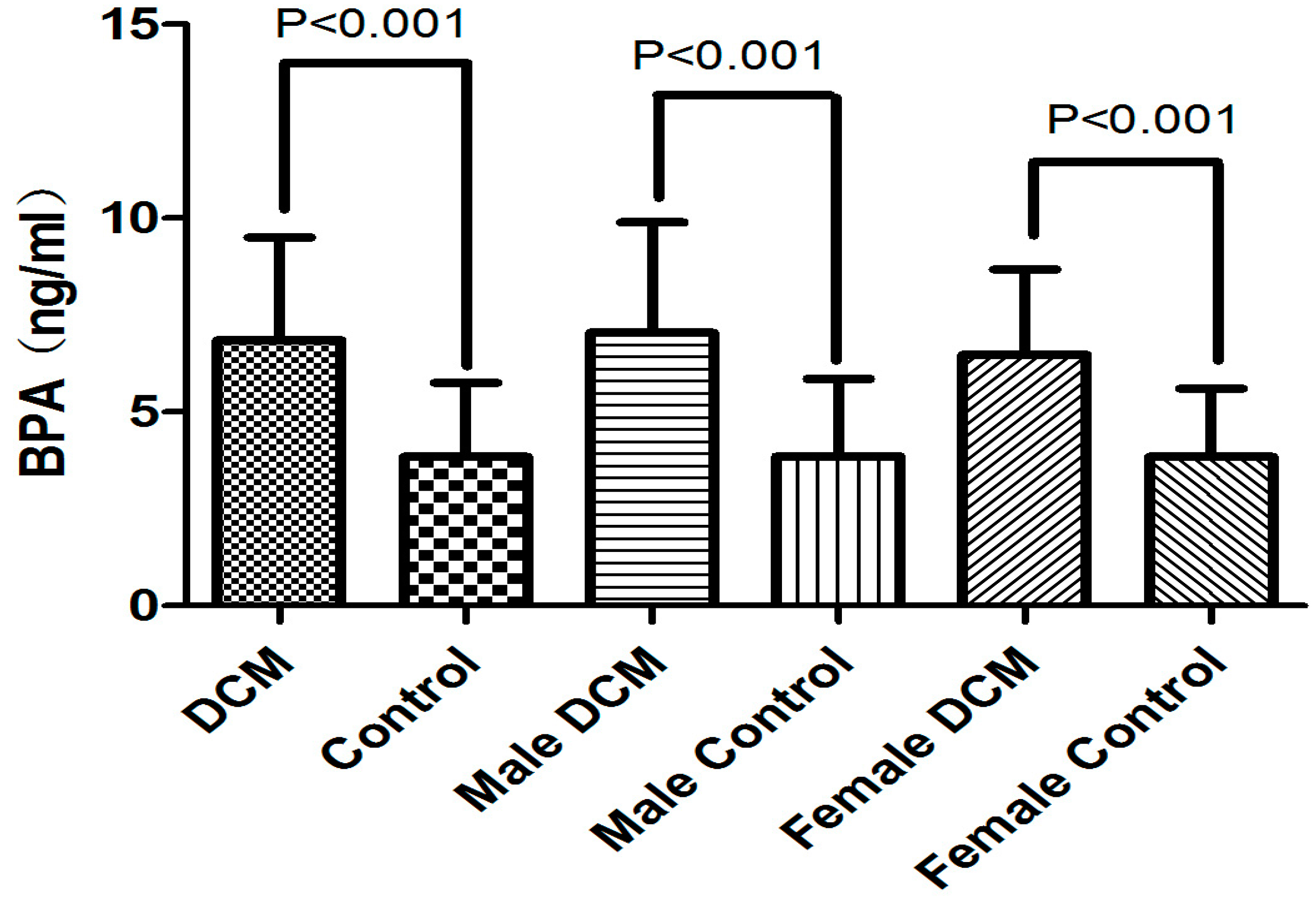
| BPA (ng/mL) | 6.9 ± 2.7 ** | 3.8 ± 1.9 ** | 7.0 ± 2.9 ** | 3.9 ± 2.0 ** | 6.5 ± 2.2 ** | 3.8 ± 1.8 ** |
| E2 (pg/mL) | 17.7 ± 10.5 | 18.1 ± 9.7 | 17.8 ± 12.0 | 18.0 ± 11.7 | 17.6 ± 7.0 | 18.3 ± 5.2 |
| T (pg/mL) | 488.3 ± 188.2 * | 555.8 ± 165.8 * | 540.8 ± 186.0 ** | 656.3 ± 112.9 ** | 381.7 ± 144.1 | 388.4 ± 83.1 |
| SHBG (nM/L) | 76.9 ± 30.9 ** | 41.0 ± 15.6 ** | 75.4 ± 30.8 ** | 42.2 ± 17.8 ** | 80.0 ± 31.2 ** | 39.1 ± 11.1 ** |
| FAI | 2.9 ± 3.5 ** | 5.3 ± 2.6 ** | 3.5 ± 4.2 ** | 6.2 ± 2.6 ** | 1.9 ± 0.8 ** | 3.8 ± 1.8 ** |

| Independent Valuables | β (95% CI) | p Value |
|---|---|---|
| Age (years) | 0.110(−0.21–0.043) | 0.514 |
| E2 (pg/mL) | −0.007(−0.048–0.034) | 0.743 |
| T (pg/mL) | −0.002(−0.004–0.001) | 0.230 |
| SHBG (nmol/L) | 0.041(0.024–0.058) | 0.000 ** |
| FAI | 0.126(−0.054–0.306) | 0.168 |
4. Discussion
5. Conclusion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Vandenberg, L.N.; Maffini, M.V.; Sonnenschein, C.; Rubin, B.S.; Soto, A.M. Bisphenol A and the great divide: A review of controversies in the field of endocrine disruption. Endocrine Rev. 2009, 30, 75–95. [Google Scholar] [CrossRef]
- Michalowicz, J. Bisphenol a—Sources, toxicity and biotransformation. Environ. Toxicol. Pharm. 2014, 37, 738–758. [Google Scholar] [CrossRef]
- Genuis, S.J.; Beesoon, S.; Birkholz, D.; Lobo, R.A. Human excretion of bisphenol A: Blood, urine, and sweat (bus) study. J. Environ. Public Health 2012. [Google Scholar] [CrossRef]
- Calafat, A.M.; Ye, X.; Wong, L.Y.; Reidy, J.A.; Needham, L.L. Exposure of the u.S. Population to bisphenol a and 4-tertiary-octylphenol: 2003–2004. Environ. Health Persp. 2008, 116, 39–44. [Google Scholar] [CrossRef]
- Lang, I.A.; Galloway, T.S.; Scarlett, A.; Henley, W.E.; Depledge, M.; Wallace, R.B.; Melzer, D. Association of urinary bisphenol a concentration with medical disorders and laboratory abnormalities in adults. JAMA 2008, 300, 1303–1310. [Google Scholar] [CrossRef] [PubMed]
- Shankar, A.; Teppala, S. Urinary bisphenol a and hypertension in a multiethnic sample of us adults. J. Environ. Public Health 2012. [Google Scholar] [CrossRef]
- Melzer, D.; Gates, P.; Osborne, N.J.; Henley, W.E.; Cipelli, R.; Young, A.; Money, C.; McCormack, P.; Schofield, P.; Mosedale, D.; et al. Urinary bisphenol a concentration and angiography-defined coronary artery stenosis. PLoS One 2012. [Google Scholar] [CrossRef] [Green Version]
- Lind, P.M.; Lind, L. Circulating levels of bisphenol a and phthalates are related to carotid atherosclerosis in the elderly. Atherosclerosis 2011, 218, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.; Kim, J.H.; Lim, Y.H.; Park, H.Y.; Hong, Y.C. Associations of bisphenol a exposure with heart rate variability and blood pressure. Hypertension 2012, 60, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Codd, M.B.; Sugrue, D.D.; Gersh, B.J.; Melton, L.J. Epidemiology of idiopathic dilated and hypertrophic cardiomyopathy, a population-based study in olmsted county, Minnesota, 1975–1984. Circulation 1989, 80, 564–572. [Google Scholar] [CrossRef] [PubMed]
- Rezg, R.; El-Fazaa, S.; Gharbi, N.; Mornagui, B. Bisphenol a and human chronic diseases: Current evidences, possible mechanisms, and future perspectives. Environ. Int. 2014, 64, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Deutschmann, A.; Hans, M.; Meyer, R.; Haberlein, H.; Swandulla, D. Bisphenol a inhibits voltage-activated Ca(2+) channels in vitro: Mechanisms and structural requirements. Molecul. Pharm. 2013, 83, 501–511. [Google Scholar] [CrossRef]
- Gao, X.; Wang, H.S. Impact of bisphenol a on the cardiovascular system—Epidemiological and experimental evidence and molecular mechanisms. Int. J. Environ. Res. Public Health 2014, 11, 8399–8413. [Google Scholar] [CrossRef] [PubMed]
- Maron, B.J.; Towbin, J.A.; Thiene, G.; Antzelevitch, C.; Corrado, D.; Arnett, D.; Moss, A.J.; Seidman, C.E.; Young, J.B.; American Heart, A.; et al. Contemporary definitions and classification of the cardiomyopathies: An american heart association scientific statement from the council on clinical cardiology, heart failure and transplantation committee; quality of care and outcomes research and functional genomics and translational biology interdisciplinary working groups; and council on epidemiology and prevention. Circulation 2006, 113, 1807–1816. [Google Scholar] [CrossRef] [PubMed]
- Patel, B.B.; Raad, M.; Sebag, I.A.; Chalifour, L.E. Lifelong exposure to bisphenol a alters cardiac structure/function, protein expression, and DNA methylation in adult mice. Toxicol. Sci. Off. J. Soc. Toxicol. 2013, 133, 174–185. [Google Scholar] [CrossRef]
- Yan, S.; Chen, Y.; Dong, M.; Song, W.; Belcher, S.M.; Wang, H.S. Bisphenol a and 17beta-estradiol promote arrhythmia in the female heart via alteration of calcium handling. PLoS ONE 2011. [Google Scholar] [CrossRef]
- Pant, J.; Ranjan, P.; Deshpande, S.B. Bisphenol a decreases atrial contractility involving no-dependent g-cyclase signaling pathway. J. Appl. Toxicol. 2011, 31, 698–702. [Google Scholar] [CrossRef] [PubMed]
- Liang, Q.; Gao, X.; Chen, Y.; Hong, K.; Wang, H.S. Cellular mechanism of the nonmonotonic dose response of bisphenol a in rat cardiac myocytes. Environ. Health Persp. 2014, 122, 601–608. [Google Scholar]
- Jiang, Y.; Xia, W.; Yang, J.; Zhu, Y.; Chang, H.; Liu, J.; Huo, W.; Xu, B.; Chen, X.; Li, Y.; et al. Bpa-induced DNA hypermethylation of the master mitochondrial gene pgc-1alpha contributes to cardiomyopathy in male rats. Toxicology 2015, 329, 21–31. [Google Scholar] [CrossRef] [PubMed]
- Vandenberg, L.N.; Chahoud, I.; Heindel, J.J.; Padmanabhan, V.; Paumgartten, F.J.; Schoenfelder, G. Urinary, circulating, and tissue biomonitoring studies indicate widespread exposure to bisphenol A. Cienc. Saude Coletiva 2012, 17, 407–434. [Google Scholar] [CrossRef]
- Pascual-Figal, D.A.; Tornel, P.L.; Nicolas, F.; Sanchez-Mas, J.; Martinez, M.D.; Gracia, M.R.; Garrido, I.P.; Ruiperez, J.A.; Valdes, M. Sex hormone-binding globulin: A new marker of disease severity and prognosis in men with chronic heart failure. Rev. Espan. Cardiol. 2009, 62, 1381–1387. [Google Scholar] [CrossRef]
- Meeker, J.D.; Calafat, A.M.; Hauser, R. Urinary bisphenol a concentrations in relation to serum thyroid and reproductive hormone levels in men from an infertility clinic. Environ. Sci. Technol. 2010, 44, 1458–1463. [Google Scholar] [CrossRef] [PubMed]
- Mendiola, J.; Jorgensen, N.; Andersson, A.M.; Calafat, A.M.; Ye, X.; Redmon, J.B.; Drobnis, E.Z.; Wang, C.; Sparks, A.; Thurston, S.W.; et al. Are environmental levels of bisphenol a associated with reproductive function in fertile men? Environ. Health Persp. 2010, 118, 1286–1291. [Google Scholar] [CrossRef]
- Zhou, Q.; Miao, M.; Ran, M.; Ding, L.; Bai, L.; Wu, T.; Yuan, W.; Gao, E.; Wang, J.; Li, G.; et al. Serum bisphenol-a concentration and sex hormone levels in men. Fertil. Steril. 2013, 100, 478–482. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiong, Q.; Liu, X.; Shen, Y.; Yu, P.; Chen, S.; Hu, J.; Yu, J.; Li, J.; Wang, H.-S.; Cheng, X.; et al. Elevated Serum Bisphenol A Level in Patients with Dilated Cardiomyopathy. Int. J. Environ. Res. Public Health 2015, 12, 5329-5337. https://doi.org/10.3390/ijerph120505329
Xiong Q, Liu X, Shen Y, Yu P, Chen S, Hu J, Yu J, Li J, Wang H-S, Cheng X, et al. Elevated Serum Bisphenol A Level in Patients with Dilated Cardiomyopathy. International Journal of Environmental Research and Public Health. 2015; 12(5):5329-5337. https://doi.org/10.3390/ijerph120505329
Chicago/Turabian StyleXiong, Qinmei, Xiao Liu, Yang Shen, Peng Yu, Sisi Chen, Jinzhu Hu, Jianhua Yu, Juxiang Li, Hong-Sheng Wang, Xiaoshu Cheng, and et al. 2015. "Elevated Serum Bisphenol A Level in Patients with Dilated Cardiomyopathy" International Journal of Environmental Research and Public Health 12, no. 5: 5329-5337. https://doi.org/10.3390/ijerph120505329
APA StyleXiong, Q., Liu, X., Shen, Y., Yu, P., Chen, S., Hu, J., Yu, J., Li, J., Wang, H. -S., Cheng, X., & Hong, K. (2015). Elevated Serum Bisphenol A Level in Patients with Dilated Cardiomyopathy. International Journal of Environmental Research and Public Health, 12(5), 5329-5337. https://doi.org/10.3390/ijerph120505329