1. Introduction
Artisanal and small-scale mining (ASM) is proliferating worldwide owing to increasing demand and rising prices for minerals and precious metals in growing economies [
1]. At least 20 million people work directly in ASM, and 80–100 million are dependent on it for their livelihood [
1]. In Ghana, an important gold-producing country, artisanal and small-scale gold mining (ASGM) accounted for 10.5% of Ghana’s national gold production and employed 0.5–1 million people as of 2010 [
2,
3]. Gold production from ASGM in Ghana rose 43% from 2011–12 [
4]. Approximately 70% of mining operations in Ghana are illegal; that is, they are not registered and licensed under the provisions of the Small-Scale Gold Mining Act of 1999 [
5].
The ASGM process begins with the excavation of gold-containing ore, which can be accomplished by panning in streams, surface and shallow digging, or by tunneling using shovels, picks, heavy excavation equipment, or dynamite. Ore is then crushed using a large hand-held mortar and pestle or generator-powered grinding machines, or both. Once a fine powder is produced, it is sifted through cloth over a basin. Large pieces trapped in the cloth are re-ground and re-sifted. This fine ore is mixed with water and carefully poured down a carpeted ramp. The carpet traps dense gold-containing particles, and less dense particles are washed down the ramp. The trapped particles are added to a pan with water, and gently centrifuged by hand to further separate the gold from the less dense ore. The gold particles are then mixed in small volumes with several drops of mercury, which forms an amalgam with the gold. Miners heat the amalgam with a blowtorch or small fire, which volatilizes the mercury and leaves behind a piece of concentrated gold. At this stage, the gold is usually sold to dealers, who repeat the mercury amalgamation and volatilization process to further refine the gold.
ASGM processes pose many occupational and community health hazards. The most well-documented of these is mercury exposure [
6,
7], though ASG miners and communities are also potentially exposed to other heavy metals present in the gold ore, airborne silica dust from pulverized ore, and noise from mining equipment [
8,
9,
10,
11]. In addition to these exposures, hazardous physical conditions and activities throughout the process raise concerns about occupational injuries. Even in high-income countries with strong and well-enforced occupational health and safety regulations, mining is a hazardous activity. Rock falls, fires, explosions, mobile equipment accidents, falls, entrapment, and electrocution are all common causes of injury in mining [
12]. The lack of safety regulations and enforcement, education and training, and functional infrastructure and equipment may lead to elevated injury rates in low- and middle-income countries, particularly in ASM. ASM operations may have 6–7 times more non-fatal accidents than large-scale operations [
13], but only a few studies have documented occupational safety issues at ASGM sites in Ghana [
14,
15]. In a study in Ghana's Kumasi Basin, illegal ASG miners identified life-threatening risks at the mine site, including dynamite blasts, collapsing pits and shafts, falls near excavation sites. The respondents reported these risks more often than risks posed by mercury use [
16].
While engineering controls are the preferred approach to mitigate safety hazards, in resource-limited settings such approaches are not often adopted. Unfortunately, the less-preferred alternative to reduce occupational risks, use of personal protective equipment (PPE, e.g., hardhats, safety glasses, gloves, work boots,
etc.), is also uncommon [
13,
17]. In a survey of ASG miners in Ghana’s Upper East Region, 70% responded that they never use PPE [
7]. In Wassa West District, Ghana, <13% of ASG miners wore safety boots, gloves, or a helmet while working [
18].
While there are numerous injury risk factors associated with ASGM work, the frequency and nature of injuries have not been well documented in sub-Saharan Africa, where there are no systematic injury surveillance programs. Because of the informal and often illegal status of many ASG operations, injuries are underreported. In 1999, the ILO estimated that 5–20 fatalities occurred in Ghanaian small-scale mines, but the true number may be much higher, especially given the increase in mining activities in Ghana in recent years [
13]. What data do exist from sub-Saharan Africa are from site-specific studies, and few calculate injury rates. In Ghana’s Wassa West District, 46.6% of small-scale gold miners surveyed reported at least one occupational injury in the last 10 years [
18]. In the Democratic Republic of the Congo, 72% of small-scale miners surveyed had experienced at least one accident in the prior year, with most of these accidents being caused by tools and the handling of heavy loads [
19]. In a study in Geita District in Tanzania, mining accidents caused about 11 fatalities annually, mostly resulting from tunnel collapse or exposure to toxic gases [
20].
In 2012, an online search of Ghanaian newspaper articles resulted in 19 articles reporting 23 separate incidents of accidents and injuries among ASG miners occurring between 2007–12 [
21]. Eight main incident types were described, with the most common being collapses trapping miners (30%), followed by drowning (17%) and violent incidents and falls into mine pits (13% each). Crushing, burns, suffocation, and firearms injuries were among the other types of incidents reported. Most of the incidents (70%) took place in illegal AS mines, and the vast majority (87%) of the reported injuries resulted in fatalities. Seventy-six fatalities were recorded in total, with a range of 1–18 fatalities per incident. While these data have potentially substantial reporting biases, this study does provide some insight into the nature of injuries in Ghanaian ASGM sites.
To better characterize injuries in ASGM sites in Ghana, our team collected cross-sectional and longitudinal data on accidents, injuries, and potentially related risk factors in Kejetia, a legally registered ASGM community in the Talensi District in Ghana's Upper East Region, where our research team has conducted research since 2009.
2. Methods
2.1. Data Collection
Data for this study were collected in Kejetia May–July 2011 and again in May 2013. Institutional Review Board (IRB) approval was obtained through the University of Michigan (HUM00028444 and HUM00073615). The community’s traditional chief and local concession owners gave us permission to work within the community.
Kejetia’s economy is centered around small-scale gold mining, and other enterprises such as beer parlors, food stands, seamstress’ shops, and bicycle repair services have emerged to meet demand for goods and services. Kejetia lacks maps, population estimates, or clear administrative boundaries. In order to achieve random sampling, in 2011, a handheld global positioning system unit (Oregon 450, Garmin International, Inc., Olathe, KS, USA) was used to take a set of geographic coordinates at every household structure in Kejetia. Households were defined as a group of people who eat from the same “pot,” in congruence with local cultural definitions. The community was then geographically divided into 20 clusters of approximately 20 households each, and each household in a cluster was assigned a unique number. Households were selected for interviewing by randomly pulling numbers from a bag, and up to three households were interviewed per day, each from different clusters. By the end of the sampling period, two to three households from each cluster had participated. When a household declined participation, another number from within that cluster was drawn from the bag. Less than 15% of households refused participation, and most cited lack of time as the main reason. Sampling in this manner occurred for six weeks due to funding limitations.
US university students administered surveys written in English with the assistance of local Ghanaian translators, who verbally translated the questions into the participants' preferred language (Talen, Nabt, Gurune, Twi, Dagbani, English, or Hausa). Before conducting interviews, the translators were trained in the necessary medical vocabulary. In 2011, interviews were preferentially administered to the head of household (HOH), followed by their spouse or any adult (age 18 or older) who could knowledgeably answer questions about the other individuals in the household. This primary interviewee completed a survey on demographics (including age, sex, educational history, health, smoking status, and marital status) and familial relationships among household members. Four adults per household at a maximum (including the primary interviewee) were administered a separate occupational history survey, which included questions regarding individuals’ experience in a range of mining activities (excavation, crushing, sifting, washing, amalgamation, burning, and owning or managing a mine site). The HOH or other primary interviewee advised the researchers whom to interview in households with more than four interested adults.
In 2013, participants from 2011 were recruited via convenience sampling. Household GPS coordinates taken in 2011 were used to relocate households of all former participants who reported involvement in mining in the 2011 survey. Any willing former participant who could be identified in this manner was invited to be surveyed. Participants administered a questionnaire examining demographics (including age, sex, educational history, health, smoking status, and marital status) and occupational health and safety. The survey included questions on psychological job demands and co-worker support from the Job Content Questionnaire [
22], stress-related questions from Cohen’s Perceived Stress Scale (PSS) [
23], and injury history (total number of injuries and, for the worst injury, task at time of injury, cause of injury, type of injury, body part injured, medical attention received, and missed work). No threshold of severity was defined for injuries, thus even minor injuries were counted. To facilitate translation, we used dichotic questions (0 = No, 1 = Yes) for the five psychological job demands questions and the four coworker support questions instead of the conventional four-point Likert scales for these scales. For analysis, we then converted the dichotic responses to the four-point Likert scale by replacing “No” with 1 and “Yes” with 4. We used five of the fourteen PSS questions and reported the summary score on a 0–20 scale, with higher scores indicating greater perceived work demands. We also summed the psychological demands and coworker support scales (scale of 4–16), with higher scores indicating greater demands and greater coworker support, respectively. Additional survey items on nutrition, as well as measurements of noise exposure, heart rate, and salivary cortisol, were collected in 2013 and are described in another paper [
24].
2.2. Analysis
Data were entered into Microsoft Excel (Microsoft, 2010) and then transferred to SPSS 22 (IBM, Armonk, NY, USA) for analysis. Descriptive statistics were calculated by demographic and occupational factors. BMI was computed from height and weight information, and scores for the psychological job demands, co-worker support [
22], and PSS [
23] scales were computed. One-way ANOVA and independent sample t-tests were used to evaluate potential differences in continuous variables between the 2011 sample and 2013 sub-sample, and Chi-square and Fisher’s exact tests were used for categorical variables. We estimated injury rate per person-year by dividing the number of surveyed miners injured in a given year by the number of all surveyed ever-miners and multiplied that by 100, resulting in a rate expressed in people injured/100 person-years. We also adjusted this rate for the number of hours worked in mining per week during the week of the survey by dividing the number of hours worked per week by 40 hours, and multiplying the resulting fraction by the injury rate. In both 2011 and 2013, we excluded those who had not actively mined in the preceding three months. Finally, a binary logistic regression model was used to identify factors predictive of increased injury risk. Demographic factors (e.g., age, BMI, education, religion, ethnicity, marital status and education), mining activities (excavation, crushing/grinding, sifting/shanking, washing/sluicing, amalgamation, burning, and owning/managing a mine) and mining experience, hours worked per week, and frequency of PPE use (defined as apron, coverall, gloves, hat, helmet/hard hat, rubber soled shoes, safety boots/steel toed boots, or safety goggles) were tested individually and in combination for potential association with injury risk. Mining experience was estimated using the greatest number of years an individual had spent on any single mining activity. Independent variables were retained in the model where
p < 0.05, and mining experience was forced into the model due to its potentially confounding role.
4. Discussion
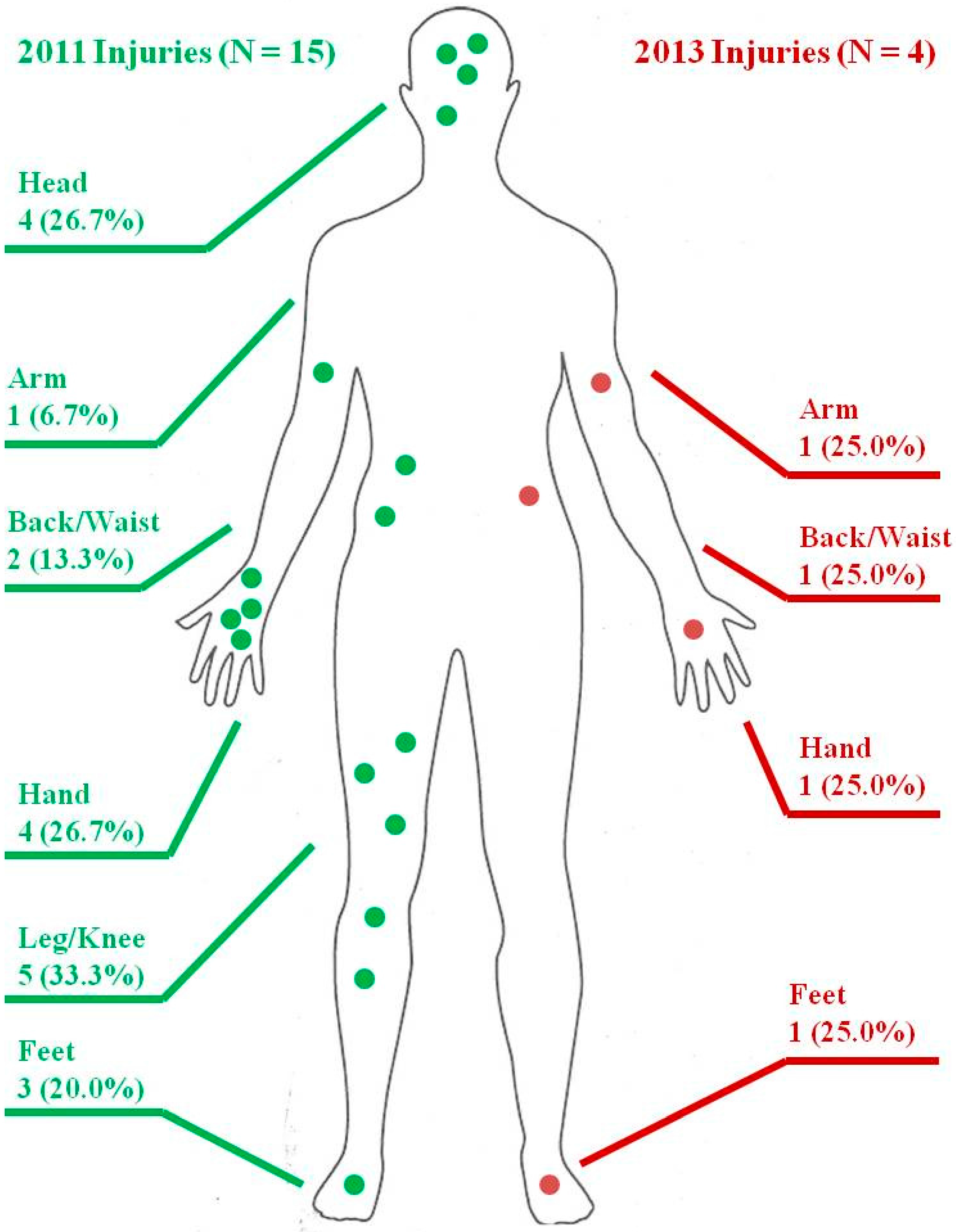
We have documented evidence of a range of occupational hazards and injuries among ASG miners in Ghana's Upper East Region. Participants reported participating in a diverse assortment of mining activities and demonstrated a wide range of mining experience, from days to decades. Demographic factors generally were not predictive of injury risk, though males showed a significantly increased risk of injury, and BMI and smoking status showed a potential (but non-significant) relationship with injury risk. Psychological demands and perceived stress were high among the miners assessed, and training on occupational health and safety issues and use of PPE were rare. The most common injury location was lower limbs (legs and feet), the most common injury causes was falling, and the most common type of injury was a cut or laceration. Logistic regression results suggested that mining experience and hours per week worked were slightly but non-significantly associated with increased injury risk, while male sex showed a significantly increased risk of injury. Age, a possible confounder with mining experience, was not significantly associated with injury risk and thus not included in our regression model.
We estimated a past-year injury rate of 45.5 injuries per 100 person-years in 2011 and 38.5 injuries per 100 person-years in 2013 among our participants. After adjusting for the number of hours worked in the miner’s primary mining activity in the week preceding the survey, these rates were 42.0 injuries per 100 person-years and 29.9 injuries per 100 person-years, respectively. The differences between these two sets of estimates are relatively small, and it seems likely that the true injury rate lies somewhere in the range between them. These results are consistent with other studies of small-scale mining operations in Africa that have demonstrated elevated injury rates. Approximately 71% of 180 artisanal miners in the D.R.C reported at least one occupational injury in 2009, and an average of two injuries per person per year (total 392 injuries) [
19]. This equates to an astoundingly high annual rate of 217.8 injuries per 100 person-years. Rates of non-fatal incidents and illnesses in large-scale mining operations in Africa appear much lower. A multi-year study of 13,924 copper mining workers in Zambia reported 165 total injuries. The estimated injury rate was 0.55 per 100 person-years, respectively, though non-fatal cases in that study were restricted to severe injuries, or injuries requiring medical attention with missing work day(s) [
25]. A rate of 0.84 injuries per 100 FTE (approximately 0.84 injuries per 100 person-years) was reported in October 2009 among gold miners in South Africa [
26]. Collectively, this evidence supports statements by the International Labor Organization that ASM operations may have several times more non-fatal accidents than large-scale operations [
13]. For comparison purposes, non-fatal injury rates in the US in 2011 were 3.5 injuries per 100 FTE (approximately 3.5 injuries per 100 person-years) for all private industries and 2.2 injuries per 100 FTE (approximately 2.2 injuries per 100 person-years) for the mining industry [
27].
A recent study (also published in this special edition (
https://www.mdpi.com/journal/ijerph/special_issues/asgm)) in the Tarkwa mining district in Ghana’s Western Region employed methods similar to ours to profile injuries among both legal and illegal small-scale gold miners. In this study, 404 participants reported 121 injuries severe enough to make them miss days of work in the ten years (2245 person-work years) preceding the survey. This yielded an overall severe injury rate of 5.39 per 100 person years [
28]. This severe-injury rate is much lower than the all-injury rate (which could include even injuries requiring only first-aid) in our own study. This is due at least in part to the fact that severe injuries occur much less frequently than minor injuries. However, the injury rate difference may also indicate differences in work conditions between the mines studied by Calys-Tagoe
et al. and those in our own study. For example, only 12.1% of miners in Calys-Tagoe
et al.’s study reported ever refusing to work because of safety concerns, compared to over half of the miners in our study [
28]. Calys-Tagoe
et al. identified the most common cause of injury as being hit or struck by an object. The study also found that the most common type of injury was a cut or laceration, which agrees with our own findings. Patterns in body parts injured were also similar between the two studies.
Another study (also published in this special edition (
https://www.mdpi.com/journal/ijerph/special_issues/asgm)) on severe injuries from ASGM in Ghana, which examined 72 hospital records from Nkawkaw Hospital in the Eastern Region from between 2006 and 2013, found that when causes of injuries were listed, they were most frequently collapsed mine pits [
29]. Fractures (30.5%) and contusions (29.1%), followed by spinal cord injuries (18.0%), were the most common types of injury listed, which is not surprising given the severe type of accident most commonly identified in their study. Collectively, these three studies of ASGM in Ghana—our own and those of Calys-Tagoe
et al. and Kyeremateng-Amoah and Clarke—indicate that ASG miners have elevated all-injury and severe-injury risk.
Our study also demonstrates substantial psychosocial stressors among ASG miners in Ghana. Male ever-miners had significantly higher psychological job demands scores than did females. For comparison purposes, female ever-miners in our study had an average psychological job demands score that was slightly lower (better) than the average for female workers in the US Quality of Employment Survey (QES) [
22], while male ever-miners scored slightly worse than US male workers. The average scores of co-worker support for female and male ever-miners were slightly higher (better) than average scores of female and male workers in the US [
22]. PSS scores were higher among female and male ever-miners in our study (average score was approximately one-half of the possible scale, with scores greater than half indicating “high stress”) than among US workers (average score was approximately one-quarter of the full scale), but comparable to scores among low-income and mostly black or multiracial South African adults (about half of the total scale) [
30]. Male ever-miners in our study perceived higher stress than females, while the opposite was true among US workers and low-income South African workers [
23]. Our results indicate that miners have concerns about their safety; over half of participants in our study had at some point refused work due to safety concerns, and 80% had made complaints about their safety while mining. Our results further suggest that safety training in ASGM communities is inadequate. Only two miners in our study had ever received any form of occupational safety training (and that they were the two miners injured in both 2011 and 2013). Similarly, Calys-Tagoe
et al. 2015 found that less than a third of the 404 miners surveyed had ever received any mining safety training [
28]. Reported PPE use was very low in our study, consistent with findings of other studies of ASG miners in Ghana and sub-Saharan Africa [
17,
18].
Our study has a number of limitations. The primary limitation is its small sample size, especially for the 2013 subsample, which may limit our ability to generalize our results. Limited resources allowed for a sample size of 173 in 2011. Of these, only 22 participants could be identified in 2013, primarily due to the transient nature of miners' lifestyles and lack of mobile phone numbers or other means of contacting former participants in advance to arrange their 2013 interviews. Many miners return to their home villages to farm depending on the season and the weather, and some take multiple-day trips to nearby villages or cities for family or religious events, selling gold, or purchasing or repairing equipment. Future longitudinal studies could mitigate the loss of participants by anticipating a high rate of subject attrition and recruiting a higher-than-necessary number of subjects, collecting detailed contact information (e.g., mobile phone numbers, alternate dwelling locations), and following up more regularly with participants to determine their locations prior to scheduling interviews. It is important to note that even the collection of mobile phone numbers does not guarantee access to subjects, as many mining areas lack mobile phone coverage.
A second limitation relates to the nature of tasks involved in ASGM work, and likely influenced our observed injury outcomes. Mining tasks appear segregated by sex, with women predominantly working in sifting and less frequently in other tasks, and men rarely working in sifting but performing all other tasks. Sifting appears to be one of the least dangerous parts of the mining process, which may help explain why the injury rate for females was so much lower than that for males. While we had data on the duration of each miner’s experience, no data were collected regarding the timing of this experience. Thus, though a miner may have had several years of experience in excavation, for example, it is possible that this experience could have occurred before the period that the questions on injury addressed (the one year prior to the survey). This may partially explain the lack of a significant relationship between mining activity type and injury rates. Further research examining injury differences by gender may benefit from oversampling female miners working in activities other than sifting.
We also assumed a full-time work schedule (40 hours per week) for our participants for one set of injury risk estimates. Though on average participants reported working nearly full-time (36.9 and 31.0 hours per week in 2011 and 2013, respectively), our measure of hours worked per week was imperfect. The survey asked about the number of hours worked in the week preceding the survey and only in the participant’s primary mining activity, which may not be representative of the entire year preceding the survey, and may underestimate the amount of time spent working if the participant does other mining activities. It is thus unclear that adjusting for number of hours worked per week resulted in a more accurate injury rate.
An additional limitation is the possibility that our study results are biased. We attempted to limit recall bias by restricting our injury recall period to the previous year, but it is possible that some injuries were not reported due to insufficient recall, or that injuries were reported inaccurately. This is likely a larger issue for minor injuries than for major injuries. The healthy worker effect may have caused some injured or ill miners to leave ASGM work and move away from the mining community sampled, but given the relative lack of employment alternatives for individuals involved in ASGM mining, this does not seem likely. Selection bias is likewise a possibility. However, within the community, no households refused to participate in the study for reasons obviously related to health status or other issues related to occupational health or injury, so we feel this is also unlikely. Finally, we excluded from our injury analysis those who had not mined within the last 3 months; due to a survey design flaw, mining injuries in the past year were not accurately recorded for these individuals. This exclusion may have biased our results negatively (i.e., by excluding individuals who worked injury-free as miners) or positively (i.e., by excluding injured miners who had not done mining within the past 3 months).
5. Conclusions
As one of the first studies to qualitatively and quantitatively assess injuries at ASGM sites in Ghana, the research described here helps address the paucity of occupational health and safety information on artisanal mining in the existing literature. Future studies should consider recording injuries among all community members to determine the proportion related to surrounding mining activities. Adequately funded, larger-scale and longitudinal studies using systematic survey methods—including improved methods of contacting transient miners combined with regular schedule of contact with subjects—or data already available in medical records from hospitals and clinics are needed to further elucidate the causes, nature, severity, and frequency of injuries at ASM sites in Ghana. However, such studies—and, in particular, studies based on medical records—must be designed carefully, as records are likely to contain substantial bias due to geographical and income-related disparities in medical access.
It is also worth noting that injuries may be a significant source of morbidity and mortality not just for miners, but also for non-miners. Anecdotal evidence from participants in our study suggests that non-miners and children have fallen into uncovered and abandoned mine pits, resulting in severe injury and even death. No studies that we are aware of to date have examined the prevalence of non-miner injuries due to ASGM.
Finally, our study suggests that, despite the relative uncertainty in our injury estimates due to the sample size limitations, the burden of injuries in ASGM communities is quite large. Further research to better characterize injury rates and determinants of injury risk is needed, but there is a clear need for occupational health interventions even in the absence of additional research. Additional resources should be dedicated to reducing the burden of injury and death in ASGM communities; such efforts will likely improve both occupational and public health in these communities.




{kind=link}
