
The Effects of Lead Exposure on Serum Uric Acid and Hyperuricemia in Chinese Adults: A Cross-Sectional Study

Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Baseline Data Collection
2.3. Anthropometric Measurements
2.4. Blood Lead Measurements
2.5. Serum Uric Acid and Hyperuricemia
2.6. Other Biochemical Measurements
2.7. Statistical Analyses
3. Results
3.1. General Characteristics of Participants

{kind=link}
| Variables | Males (n = 1180) | Females (n = 940) | p |
|---|---|---|---|
| Age (years) | 43.0 (35.0–48.0) | 47.0 (38.0–58.0) | <0.001 |
| BMI (kg/m2) | 23.3 ± 3.1 | 22.6 ± 3.1 | <0.001 |
| Current smoking, n (%) | 571 (48.4%) | 44 (4.7%) | <0.001 |
| Current drinking, n (%) | 775 (65.7%) | 183 (19.5%) | <0.001 |
| Education, n (%) | 0.412 | ||
| >High school | 103 (8.7%) | 91 (9.7%) | |
| =High school | 435 (36.9%) | 364 (38.7%) | |
| <High school | 642 (54.4%) | 485 (51.6%) | |
| SBP (mmHg) | 121.0 (112.0–130.0) | 120.0 (108.0–130.0) | <0.001 |
| DBP (mmHg) | 81.3 ± 9.9 | 77.7 ± 9.7 | <0.001 |
| Fasting glucose (mmol/L) | 4.6 (4.0–4.8) | 4.5 (4.1–4.9) | 0.074 |
| TC (mmol/L) | 4.1 (3.8–4.5) | 4.2 (3.8–4.5) | 0.003 |
| TG (mmol/L) | 1.4 (1.0–1.6) | 1.3 (1.0–1.6) | 0.034 |
| HDL-C (mmol/L) | 1.6 ± 0.2 | 1.6 ± 0.2 | 0.468 |
| Serum creatinine (μmol/L) | 89.3 ± 11.5 | 88.0 ± 7.4 | 0.004 |
| BUN (mmol/L) | 4.3 ± 0.9 | 4.4 ± 1.0 | 0.067 |
| Uric acid (μmol/L) | 311.6 ± 72.3 | 261.6 ± 63.1 | <0.001 |
| Hyperuricemia, n (%) | 74 (6.3%) | 76 (8.1%) | 0.106 |
| Blood lead (µg/L) | 91.0 (58.0–149.0) | 66.0 (44.0–103.0) | <0.001 |
3.2. Correlations between Serum Uric Acid and other Variables
| Variables | Males
r | p | Females
r | p |
|---|---|---|---|---|
| Blood lead (µg/L) * | 0.095 | 0.001 | 0.134 | <0.001 |
| Age (years) * | 0.127 | <0.001 | 0.111 | 0.001 |
| BMI (kg/m2) | 0.089 | 0.002 | 0.129 | <0.001 |
| Current smoking | 0.096 | 0.028 | 0.066 | 0.043 |
| Current drinking | 0.056 | 0.054 | 0.000 | 0.994 |
| Education | 0.121 | 0.001 | −0.036 | 0.272 |
| SBP (mmHg) * | 0.075 | 0.010 | 0.083 | 0.011 |
| DBP (mmHg) | 0.048 | 0.097 | 0.082 | 0.012 |
| Fasting glucose (mmol/L) * | 0.054 | 0.063 | 0.056 | 0.088 |
| TC (mmol/L) * | 0.041 | 0.156 | 0.071 | 0.029 |
| TG (mmol/L) * | 0.165 | <0.001 | 0.159 | <0.001 |
| HDL-C (mmol/L) | −0.056 | 0.054 | −0.017 | 0.612 |
| Serum creatinine (μmol/L) | 0.281 | <0.001 | 0.044 | 0.175 |
| BUN (mmol/L) | 0.179 | <0.001 | 0.041 | 0.206 |
3.3 Multiple Linear Regression Analysis for Serum Uric Acid Level
| Variables | Males
β | p | Females
β | p |
|---|---|---|---|---|
| Blood lead * | 18.575 | 0.006 | 27.374 | <0.001 |
| Age * | 65.165 | 0.001 | 27.300 | 0.191 |
| BMI | 0.783 | 0.254 | 1.831 | 0.009 |
| Current smoking | 10.350 | 0.012 | 17.232 | 0.075 |
| Current drinking | 0.731 | 0.866 | −3.294 | 0.531 |
| Education | 11.099 | 0.001 | 3.257 | 0.311 |
| SBP * | 13.244 | 0.834 | −37.617 | 0.505 |
| DBP | −0.022 | 0.944 | 0.296 | 0.370 |
| Fasting glucose * | 5.234 | 0.854 | −2.509 | 0.924 |
| TC * | −34.085 | 0.296 | 34.864 | 0.314 |
| TG * | 53.158 | <0.001 | 43.553 | <0.001 |
| HDL-C | 1.844 | 0.869 | 9.713 | 0.362 |
| Serum creatinine | 1.513 | <0.001 | 0.108 | 0.700 |
| BUN | 3.125 | 0.198 | 1.274 | 0.544 |
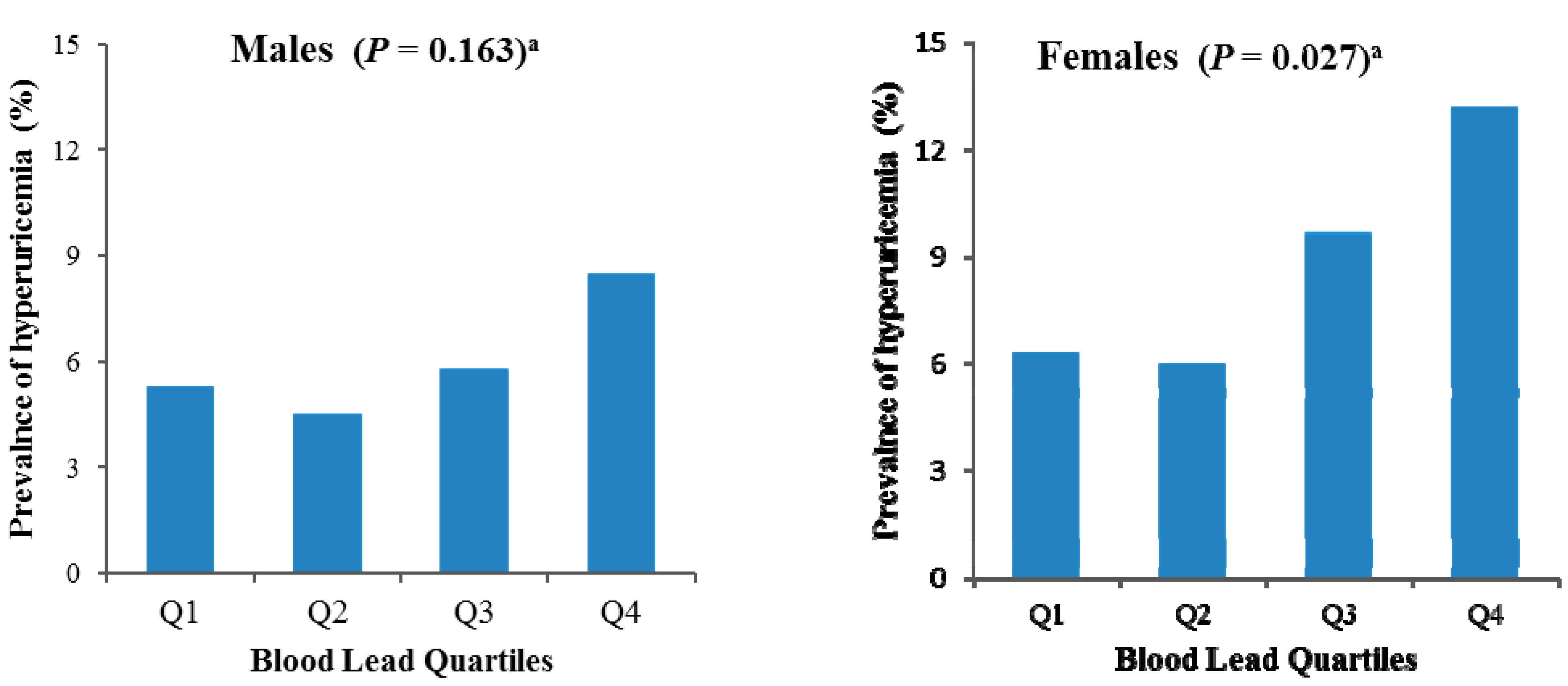
3.4. Association between Blood Lead Levels and the Prevalence of Hyperuricemia

| Blood Lead (µg/L) | C/NC | Model 1 | Model 2 | Model 3 |
|---|---|---|---|---|
| Males | ||||
| Quartile 1 (≤50.2) | 12/214 | 1.00 (Ref) | 1.00 (Ref) | 1.00 (Ref) |
| Quartile 2(>50.2 and ≤79.0) | 12/255 | 0.859 (0.364, 2.024) | 0.953 (0.399, 2.275) | 1.255 (0.480, 3.280) |
| Quartile 3(>79.0 and ≤126.0) | 18/293 | 0.919 (0.416, 2.029) | 0.917 (0.410, 2.053) | 1.181 (0.485, 2.874) |
| Quartile 4 (>126.0) | 32/344 | 1.508 (0.732, 3.106) | 1.551 (0.746, 3.226) | 1.708 (0.742, 3.933) |
| Females | ||||
| Quartile 1 (≤50.2) | 19/285 | 1.00 (Ref) | 1.00 (Ref) | 1.00 (Ref) |
| Quartile 2(>50.2 and ≤79.0) | 16/252 | 0.940 (0.472, 1.869) | 0.950(0.475, 1.898) | 0.928 (0.462, 1.863) |
| Quartile 3(>79.0 and ≤126.0) | 21/196 | 1.516 (0.791, 2.905) | 1.458(0.755, 2.815) | 1.398 (0.716, 2.732) |
| Quartile 4 (>126.0) | 20/131 | 2.294 (1.181, 4.456) | 2.249(1.151, 4.394) | 2.190 (1.106, 4.338) |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- De Oliveira, E.P.; Burini, R.C. High plasma uric acid concentration: causes and consequences. Diabetol. Metab. Syndr. 2012, 4. [Google Scholar] [CrossRef]
- Choi, H.K.; Liu, S.; Curhan, G. Intake of purine-rich foods, protein, and dairy products and relationship to serum levels of uric acid: The Third National Health and Nutrition Examination Survey. Arthritis Rheum. 2005, 52, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Atkinson, K.; Karlson, E.W.; Curhan, G. Obesity, weight change, hypertension, diuretic use, and risk of gout in men: The health professionals follow-up study. Arch. Intern. Med. 2005, 165, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Lipkowitz, M.S. Regulation of uric acid excretion by the kidney. Curr. Rheumatol. Rep. 2012, 14, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.L.; Zhu, T.; Xu, L.; Zhang, W.S.; Liu, B.; Jiang, C.Q.; Yu, H.; Huang, L.M.; Cheng, K.K.; Thomas, G.N.; et al. Uric acid levels, even in the normal range, are associated with increased cardiovascular risk: The Guangzhou Biobank Cohort Study. Int. J. Cardiol. 2013, 168, 2238–2241. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.F.; Chuang, S.Y.; Cheng, H.M.; Sung, S.H.; Ting, C.T.; Lakatta, E.G.; Yin, F.C.; Chou, P.; Chen, C.H. Associations of serum uric acid levels with arterial wave reflections and central systolic blood pressure. Int. J. Cardiol. 2013, 168, 2057–2063. [Google Scholar] [CrossRef] [PubMed]
- Richette, P.; Bardin, T. Gout. Lancet 2010, 375, 318–328. [Google Scholar] [CrossRef]
- Kenny, J.E.S.; Goldfarb, D.S. Update on the pathophysiology and management of uric acid renal stones. Curr. Rheumatol. Rep. 2010, 12, 125–129. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, J.P.; Oliveira, A.; Severo, M.; Santos, A.C.; Lopes, C. Cross-sectional and longitudinal associations between serum uric acid and metabolic syndrome. Endocrine. 2012, 41, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.C.; Hung, C.C.; Chen, S.C.; Yeh, S.M.; Lin, M.Y.; Chiu, Y.W.; Kuo, M.C.; Chang, J.M.; Hwang, S.J.; Chen, H.C. Association of hyperuricemia with renal outcomes, cardiovascular disease, and mortality. Clin. J. Am. Soc. Nephrol. 2012, 7, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Wang, Y.; Zeng, Y.; Gao, G.F.; Liang, X.; Zhou, M.; Wan, X.; Yu, S.; Jiang, Y.; Naghavi, M.; et al. Rapid health transition in China, 1990–2010: Findings from the Global Burden of Disease Study 2010. Lancet 2013, 381, 1987–2015. [Google Scholar] [CrossRef]
- Wang, V.S.; Lee, M.T.; Chiou, J.Y.; Guu, C.F.; Wu, C.C.; Wu, T.N.; Lai, J.S. Relationship between blood lead levels and renal function in lead battery workers. Int. Arch. Occup. Environ. Health. 2002, 75, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, R.; Robins, T.; Jordaan, E.; Miller, S.; Mbuli, S.; Selby, P.; Wynchank, S.; Cantrell, A.; de Broe, M.; D’Haese, P.; et al. Lead absorption and renal dysfunction in a South African battery factory. Occup. Environ. Med. 1998, 55, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Serrato, M.I.; Fortoul, T.I.; Rojas-Martinez, R.; Mendoza-Alvarado, L.R.; Canales-Trevino, L.; Bochichio-Riccardelli, T.; Avila-Costa, M.R.; Olaiz-Fernández, G. Lead blood concentrations and renal function evaluation: Study in an exposed Mexican population. Environ. Res. 2006, 100, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Omae, K.; Sakurai, H.; Higashi, T.; Muto, T.; Ichikawa, M.; Sasaki, N. No adverse effects of lead on renal function in lead-exposed workers. Ind. Health. 1990, 28, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Weaver, V.M.; Jaar, B.G.; Schwartz, B.S.; Todd, A.C.; Ahn, K.D.; Lee, S.S.; Wen, J.; Parsons, P.J.; Lee, B.K. Associations among lead dose biomarkers, uric acid, and renal function in Korean lead workers. Environ. Health Perspect. 2005, 113, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Zhang, X.M.; Wang, Y.L.; Liu, B.C. Prevalence of hyperuricemia among Chinese adults: A national cross-sectional survey using multistage, stratified sampling. J. Nephrol. 2014, 27, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Liu, Z.; Zhang, C.; Zhao, Y.; Sun, S.; Wang, S.; Zhao, Y.; Zhang, Y.; Li, J.; Lu, F. The prevalence of hyperuricemia and its correlates in an inland Chinese adult population, urban and rural of Jinan. Rheumatol. Int. 2013, 33, 1511–1517. [Google Scholar] [CrossRef] [PubMed]
- Abdel, M.A.; Dkhil, M.A.; Al-Quraishy, S. The protective effect of flaxseed oil on lead acetate-induced renal toxicity in rats. J. Hazard. Mater. 2011, 194, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Shrivastava, S.; Shukla, S. Reversal of lead-induced toxicity due to the effect of antioxidants. J. Environ. Pathol. Toxicol. Oncol. 2013, 32, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.M.; Sun, Y.Z.; Sun, J.M.; Ma, J.Q.; Cheng, C. Protective role of quercetin against lead-induced inflammatory response in rat kidney through the ROS-mediated MAPKs and NF-κB pathway. Biochim. Biophys. Acta. 2012, 1820, 1693–1703. [Google Scholar] [CrossRef] [PubMed]
- Kilikdar, D.; Mukherjee, D.; Mitra, E.; Ghosh, A.K.; Basu, A.; Chandra, A.M.; Bandyoapdhyay, D. Protective effect of aqueous garlic extract against lead-induced hepatic injury in rats. Indian J. Exp. Biol. 2011, 49, 498–510. [Google Scholar] [PubMed]
- Khan, D.A.; Qayyum, S.; Saleem, S.; Khan, F.A. Lead-induced oxidative stress adversely affects health of the occupational workers. Toxicol. Ind. Health. 2008, 24, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Alasia, D.D.; Emem-Chioma, P.C.; Wokoma, F.S. Association of lead exposure, serum uric acid and parameters of renal function in Nigerian lead-exposed workers. Int. J. Occup. Environ. Med. 2010, 1, 182–190. [Google Scholar] [PubMed]
- Vishwanath, P.; Devegowda, D.; Prashant, A.; Nayak, N.; D'Souza, V.; Venkatesh, T.; Scott, C. Environmental lead levels in a coastal city of India: The lead burden continues. Indian J. Med. Sci. 2012, 66, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C.; Mallamaci, F. Uric acid, hypertension, and cardiovascular and renal complications. Curr. Hypertens. Rep. 2013, 15, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Mazzali, M.; Hughes, J.; Kim, Y.G.; Jefferson, J.A.; Kang, D.H.; Gordon, K.L.; Lan, H.Y.; Kivlighn, S.; Johnson, R.J. Elevated uric acid increases blood pressure in the rat by a novel crystal-independent mechanism. Hypertension 2001, 38, 1101–1106. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, R.; Robins, T.; Jordaan, E.; Miller, S.; Mbuli, S.; Selby, P.; Wynchank, S.; Cantrell, A.; de Broe, M.; D’Haese, P.; et al. Lead absorption and renal dysfunction in a South African battery factory. Occup. Environ. Med. 1998, 55, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Muntner, P.; He, J.; Vupputuri, S.; Coresh, J.; Batuman, V. Blood lead and chronic kidney disease in the general United States population: Results from NHANES III. Kidney Int. 2003, 63, 1044–1050. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.; Tai-Yi, J. Benchmark dose approach for renal dysfunction in workers exposed to lead. Environ. Toxicol. 2007, 22, 229–233. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Aro, A.; Payton, M.; Korrick, S.; Sparrow, D.; Weiss, S.T.; Rotnitzky, A. The relationship of bone and blood lead to hypertension. The Normative Aging Study. JAMA 1996, 275, 1171–1176. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Schwartz, J.; Sparrow, D.; Aro, A.; Weiss, S.T.; Hu, H. Bone lead and blood lead levels in relation to baseline blood pressure and the prospective development of hypertension: The Normative Aging Study. Am. J. Epidemiol. 2001, 153, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Nash, D.; Magder, L.; Lustberg, M.; Sherwin, R.W.; Rubin, R.J.; Kaufmann, R.B.; Silbergeld, E.K. Blood lead, blood pressure, and hypertension in perimenopausal and postmenopausal women. JAMA 2003, 289, 1523–1532. [Google Scholar] [CrossRef] [PubMed]
- Qiu, L.; Cheng, X.Q.; Wu, J.; Liu, J.T.; Xu, T.; Ding, H.T.; Liu, Y.H.; Ge, Z.M.; Wang, Y.J.; Han, H.J.; et al. Prevalence of hyperuricemia and its related risk factors in healthy adults from Northern and Northeastern Chinese provinces. BMC Public Health 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Lou, S.; Xu, K.; Meng, Z.; Zhang, Q.; Song, K. Relationship between lifestyle choices and hyperuricemia in Chinese men and women. Clin. Rheumatol. 2013, 32, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Vahter, M.; Akesson, A.; Liden, C.; Ceccatelli, S.; Berglund, M. Gender differences in the disposition and toxicity of metals. Environ. Res. 2007, 104, 85–95. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dai, H.; Huang, Z.; Deng, Q.; Li, Y.; Xiao, T.; Ning, X.; Lu, Y.; Yuan, H. The Effects of Lead Exposure on Serum Uric Acid and Hyperuricemia in Chinese Adults: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2015, 12, 9672-9682. https://doi.org/10.3390/ijerph120809672
Dai H, Huang Z, Deng Q, Li Y, Xiao T, Ning X, Lu Y, Yuan H. The Effects of Lead Exposure on Serum Uric Acid and Hyperuricemia in Chinese Adults: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2015; 12(8):9672-9682. https://doi.org/10.3390/ijerph120809672
Chicago/Turabian StyleDai, Haijiang, Zhijun Huang, Qihong Deng, Ying Li, Ting Xiao, Xingping Ning, Yao Lu, and Hong Yuan. 2015. "The Effects of Lead Exposure on Serum Uric Acid and Hyperuricemia in Chinese Adults: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 12, no. 8: 9672-9682. https://doi.org/10.3390/ijerph120809672
APA StyleDai, H., Huang, Z., Deng, Q., Li, Y., Xiao, T., Ning, X., Lu, Y., & Yuan, H. (2015). The Effects of Lead Exposure on Serum Uric Acid and Hyperuricemia in Chinese Adults: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 12(8), 9672-9682. https://doi.org/10.3390/ijerph120809672