
A Meta-Analysis of Maternal Smoking during Pregnancy and Autism Spectrum Disorder Risk in Offspring

Abstract
:1. Introduction
2. Methods
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Analysis
3. Results
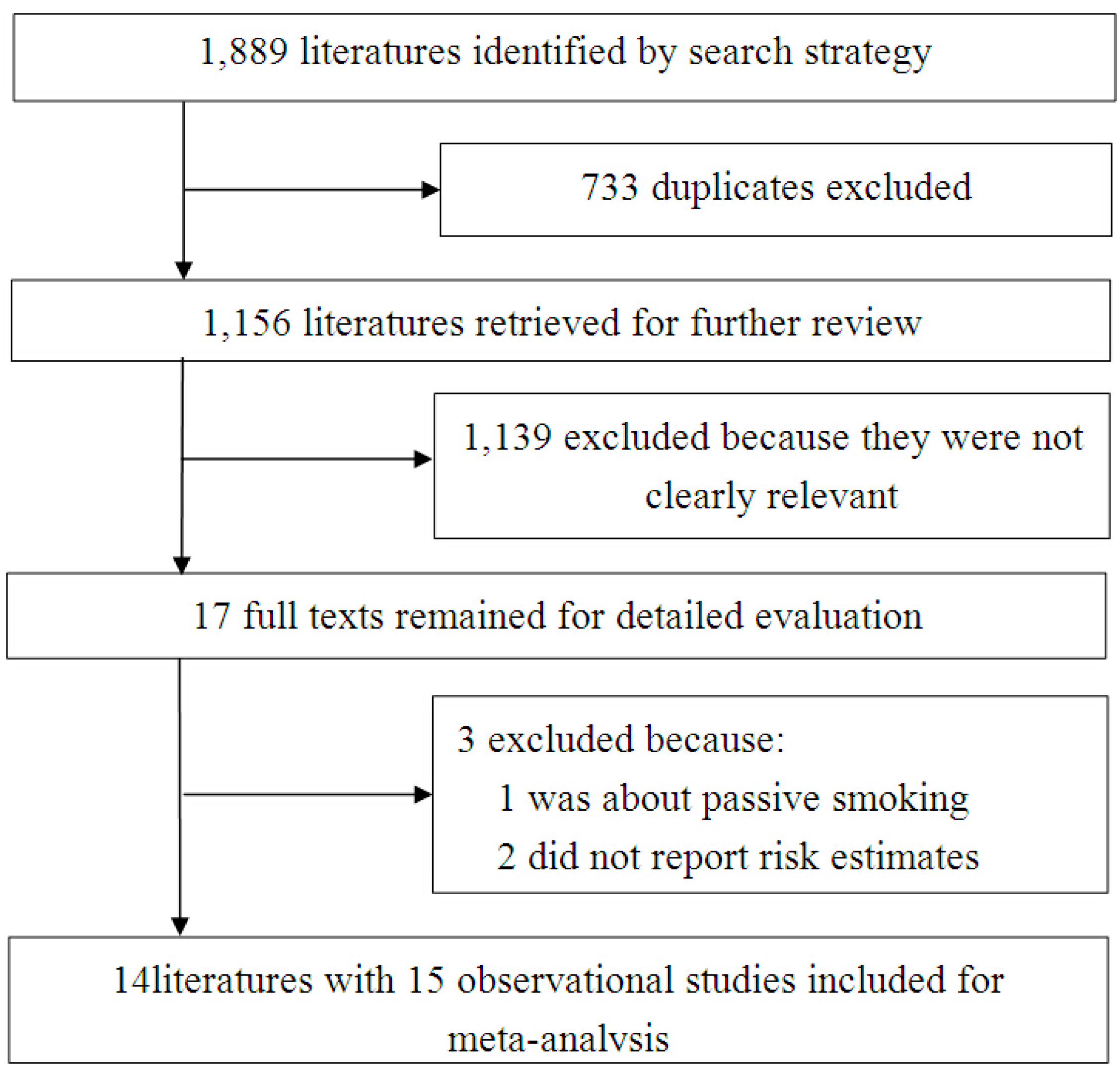
3.1. Literature Search and Selection

3.2. Study Characteristics

{kind=link}
{kind=link}
| Study | Location | Design a | ASD Cases/Total Participants | Age(y), Sex | Ascertainment of Smoking | Ascertainment of ASDs | OR(95%CI) | Confounding |
|---|---|---|---|---|---|---|---|---|
| Hultman 2002 [23] | Sweden | CC | 408/2448 | <10, M&F b | Collected by midwives at registration for antenatal care | Medical record | 1.4(1.1,1.8) | Maternal age, parity, mothers’ country of birth, hypertensive diseases, diabetes, mode of delivery, pregnancy bleeding, season of birth, gestational age, birth weight for gestational age, Apgar at 5 min, congenital malformations |
| Larsson 2005 [25] | Denmark | CC | 249/6474 | ≤24, M&F | Reported at the first antenatal visit | Medical record | 1.06(0.80,1.39) | NA |
| Maimburg 2006 [28] | Denmark | CC | 473/5203 | <10, M&F | Collected by midwives at the first antenatal visit | Medical record | 0.9(0.7,1.4) | Mother and fathers age, mothers citizenship, birth weight and gestational age, Apgar, birth defect and irregular foetal position |
| Bilder 2009 [19] | US | CC | 132/13,332 | 8, M&F | NAc | Clinician review of medical and school record | 0.506(0.222,1.152) | NA |
| Larsson 2009 [26] | Sweden | C | 72/4779 | 6–8, M&F | Parent-report collected for pregnancy when child was age 1–3 years | Parent-report collected by follow-up questionnaire | 2.09(1.08,4.03) | Unadjusted |
| Burstyn 2010 [20] | Canada | C | 1138/218,890 | ≤9, M&F | Collected on admission to hospital for delivery | Medical registry record | 0.86(0.72,1.02) | Maternal age, maternal weight, maternal height, pre-pregnancy diabetes, gestational diabetes, bleeding, weight gain, parity, socio-economic status, pre-eclampsia, presentation, type of labour, delivery by caesarian section, gestational age, birth weight, apgar at 1 min, Apgar at 5 min, birth year |
| Dodds 2010 [21] | Canada | C | 924/129,733 | 1–17, M&F | Investigated by a standardized questionnaire | Administrative databases with relevant diagnostic information | 0.93(0.81,1.08) | Unadjusted |
| Haglund 2011 [22] | Sweden | CC | 157/68,964 | 8–15, M&F | Swedish Medical Birth Registry | Medical registry | 0.7(0.5,1.0) | Year of birth, maternal age at delivery, parity , sex, gestational age at birth, standard deviations scores, obstetrical risk factor |
| Kalkbrenner 2012 [24] | US | CC | 3315/633,989 | 8, M&F | Birth certificate data | Surveillance-ascertained | 0.9(0.8,1.01) | Maternal education, race and ethnicity, marital status, maternal age, county population size, birth year and surveillance site. |
| Lee 2012 [27] | Sweden | CC | 3958/42,941 | 4–17, M&F | Recorded by midwives at the first prenatal visit | Medical registry | 1.10(1.01,1.20) | Unadjusted |
| Tran 2013 [6] | Finland | CC | 4019/20,601 | ≤7, M&F | Collected by maternity clinic nurses during routine obstetric visits | Medical registry | 1.0(0.9,1.2) | Maternal age, maternal mental diagnosis, socioeconomic status and weight for gestational age |
| Nilsen 2013 [18] | Norway | C | 2072/507,856 | 3–11, M&F | Recorded by check boxes at the beginning and the end of pregnancy | Medical registry | 1.20(0.84,1.71) | Year of birth, maternal age, marital status, hospital size. |
| Norway | C | 234/89,836 | 3–11, M&F | The same as above | Medical registry | 1.17(1.04,1.31) | The same as above | |
| Mrozek-Budzyn 2013 [29] | Poland | CC | 96/288 | 2–15, M&F | Investigated by a standardized questionnaire | Medical record | 3.32(1.23,9.82) | Unadjusted |
| Xiang 2015 [30] | US | C | 643/64,924 | 1.5–2 M&F | Extracted from medical records and birth certificate records | Screened by a modified version of CHAT d and diagnosed by pediatric developmental specialist evaluation | 0.83(0.33,2.09) | Birth year |
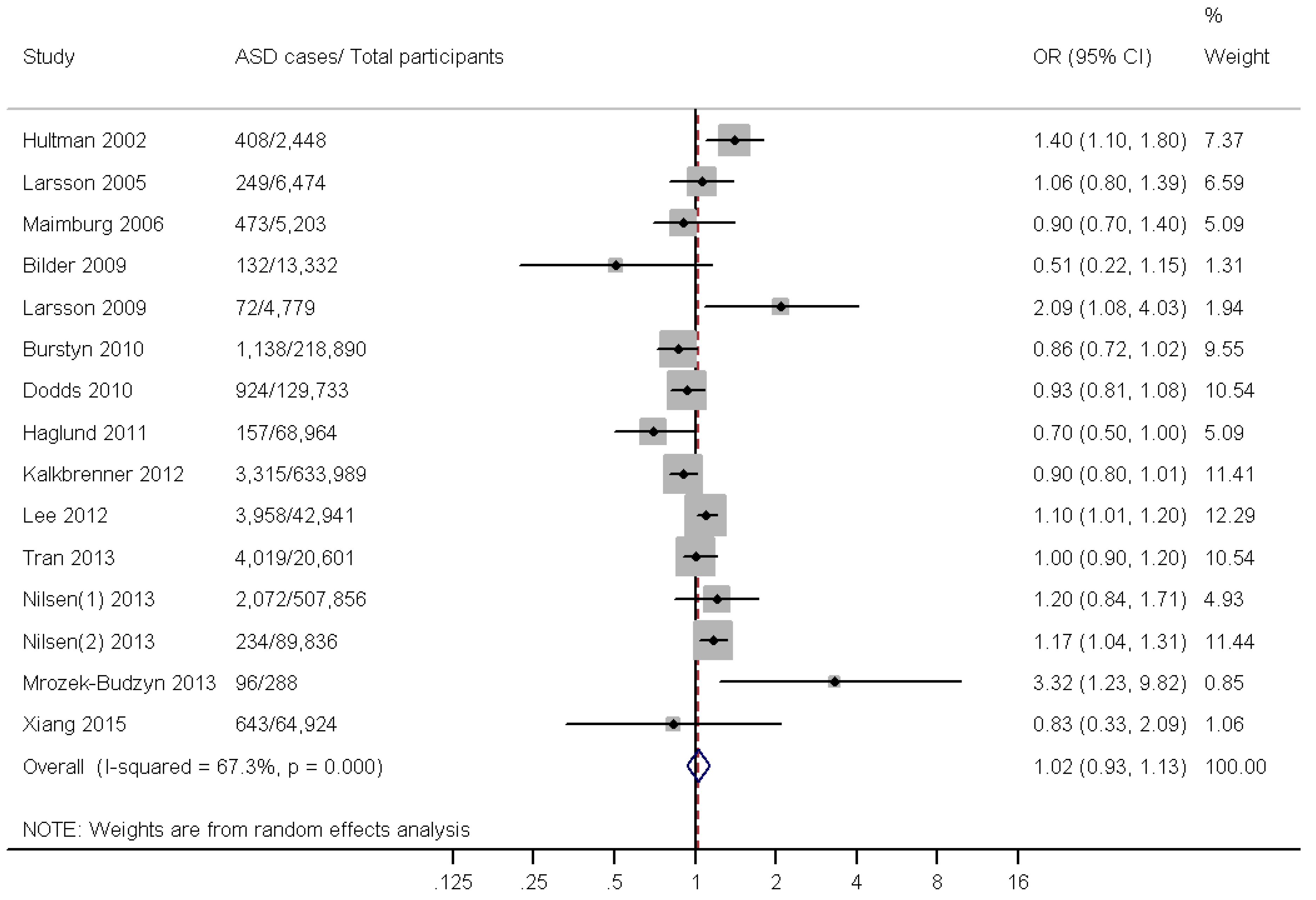
3.3. Main Analysis

3.4. Subgroup and Sensitivity Analysis
| Variables | No. of Studies | I2% | pheterogeneity | OR(95%CI) |
|---|---|---|---|---|
| All studies | 15 | 67.3 | <0.001 | 1.02(0.93,1.13) |
| Location | ||||
| Europe | 10 | 60.1 | 0.007 | 1.11(0.99,1.24) |
| America | 5 | 0.00 | 0.671 | 0.90(0.83,0.97) |
| Design | ||||
| Cohort | 6 | 68.9 | 0.007 | 1.05(0.88,1.25) |
| Case-control | 9 | 70.0 | 0.001 | 1.01(0.88,1.15) |
| Study quality | ||||
| High | 12 | 60.4 | 0.003 | 1.02(0.92, 1.12) |
| Moderate | 3 | 83.1 | 0.003 | 1.65(0.73, 3.73) |
| Adjustment for confounders | ||||
| Yes | 9 | 69.0 | 0.001 | 1.00(0.88,1.13) |
| No/NA * | 6 | 68.2 | 0.008 | 1.08(0.89,1.32) |
3.5. Publication Bias
4. Discussion
5. Conclusions
Supplemental Material
| Case-Control Study | Definition of Cases | Representativeness of the Cases | Selection of Controls | Definition of Controls | Comparability of Cases and Control * | Ascertainment of Exposure | Same Method of Ascertainment for Cases and Controls | Non-Response Rate | Total Score |
|---|---|---|---|---|---|---|---|---|---|
| Hultman 2002 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 0 | 8 |
| Larsson 2005 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 7 |
| Maimburg 2006 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
| Bilder 2009 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 7 |
| Haglund 2011 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8 |
| Kalkbrenner 2012 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 6 |
| Lee 2012 | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 0 | 7 |
| Tran 2013 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
| Mrozek-Budzyn 2013 | 1 | 1 | 0 | 0 | 2 | 1 | 1 | 0 | 6 |
| Cohor study | Representativeness of the exposed cohort | Selection of the non exposed cohort | Ascertainment of exposure | outcome of interest was not present at start of study | Comparability of cohorts * | Assessment of outcome | follow-up long enough for outcomes to occur | Adequacy of follow up of cohorts | |
| Larsson 2009 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 5 |
| Burstyn 2010 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 7 |
| Dodds 2010 | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
| Nilsen(1) 2013 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Nilsen(2) 2013 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 7 |
| Xiang 2015 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 7 |
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lai, M.C.; Lombardo, M.V.; Baron-Cohen, S. Autism. Lancet 2014, 383, 896–910. [Google Scholar] [CrossRef]
- Christensen, J.; Gronborg, T.K.; Sorensen, M.J.; Schendel, D.; Parner, E.T.; Pedersen, L.H.; Vestergaard, M. Prenatal valproate exposure and risk of autism spectrum disorders and childhood autism. JAMA 2013, 309, 1696–1703. [Google Scholar] [CrossRef] [PubMed]
- Baxter, A.J.; Brugha, T.S.; Erskine, H.E.; Scheurer, R.W.; Vos, T.; Scott, J.G. The epidemiology and global burden of autism spectrum disorders. Psychol. Med. 2014, 45, 601–613. [Google Scholar] [CrossRef] [PubMed]
- Levy, S.E.; Mandell, D.S.; Schultz, R.T. Autism. Lancet 2009, 374, 1627–1638. [Google Scholar] [CrossRef]
- Pineles, B.L.; Park, E.; Samet, J.M. Systematic review and meta-analysis of miscarriage and maternal exposure to tobacco smoke during pregnancy. Am. J. Epidemiol. 2014, 179, 807–823. [Google Scholar] [CrossRef] [PubMed]
- Tran, P.L.; Lehti, V.; Lampi, K.M.; Helenius, H.; Suominen, A.; Gissler, M.; Brown, A.S.; Sourander, A. Smoking during pregnancy and risk of autism spectrum disorder in a Finnish National Birth Cohort. Paediatr. Perinat. Epidemiol. 2013, 27, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Rosen, B.N.; Lee, B.K.; Lee, N.L.; Yang, Y.; Burstyn, I. Maternal Smoking and Autism Spectrum Disorder: A Meta-analysis. J. Autism Dev. Disord. 2015, 45, 1689–1698. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Ji, J.; Liu, Y.-J.; Deng, X.; He, Q.-Q. Passive Smoking and Risk of Type 2 Diabetes: A Meta-Analysis of Prospective Cohort Studies. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [PubMed]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Duan, G.; Yao, M.; Ma, Y.; Zhang, W. Perinatal and background risk factors for childhood autism in central China. Psychiatry Res. 2014, 220, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Ronald, A.; Happe, F.; Dworzynski, K.; Bolton, P.; Plomin, R. Exploring the relation between prenatal and neonatal complications and later autistic-like features in a representative community sample of twins. Child Dev. 2010, 81, 166–182. [Google Scholar] [CrossRef] [PubMed]
- Visser, J.C.; Rommelse, N.; Vink, L.; Schrieken, M.; Oosterling, I.J.; van der Gaag, R.J.; Buitelaar, J.K. Narrowly versus broadly defined autism spectrum disorders: Differences in pre- and perinatal risk factors. J. Autism Dev. Disord. 2013, 43, 1505–1516. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, R.M.; Suren, P.; Gunnes, N.; Alsaker, E.R.; Bresnahan, M.; Hirtz, D.; Hornig, M.; Lie, K.K.; Lipkin, W.I.; Reichborn-Kjennerud, T.; et al. Analysis of self-selection bias in a population-based cohort study of autism spectrum disorders. Paediatr. Perinat. Epidemiol. 2013, 27, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Bilder, D.; Pinborough-Zimmerman, J.; Miller, J.; McMahon, W. Prenatal, perinatal, and neonatal factors associated with autism spectrum disorders. Pediatrics 2009, 123, 1293–1300. [Google Scholar] [CrossRef] [PubMed]
- Burstyn, I.; Sithole, F.; Zwaigenbaum, L. Autism spectrum disorders, maternal characteristics and obstetric complications among singletons born in Alberta, Canada. Chronic Dis. Canada 2010, 30, 125–134. [Google Scholar]
- Dodds, L.; Fell, D.B.; Shea, S.; Armson, B.A.; Allen, A.C.; Bryson, S. The role of prenatal, obstetric and neonatal factors in the development of autism. J. Autism Dev. Disord. 2011, 41, 891–902. [Google Scholar] [CrossRef] [PubMed]
- Haglund, N.G.; Kallen, K.B. Risk factors for autism and Asperger syndrome. Perinatal factors and migration. Autism 2011, 15, 163–183. [Google Scholar] [CrossRef] [PubMed]
- Hultman, C.M.; Sparen, P.; Cnattingius, S. Perinatal risk factors for infantile autism. Epidemiology (Cambridge Mass.) 2002, 13, 417–423. [Google Scholar] [CrossRef]
- Kalkbrenner, A.E.; Braun, J.M.; Durkin, M.S.; Maenner, M.J.; Cunniff, C.; Lee, L.C.; Pettygrove, S.; Nicholas, J.S.; Daniels, J.L. Maternal smoking during pregnancy and the prevalence of autism spectrum disorders, using data from the autism and developmental disabilities monitoring network. Environ. Health Perspect. 2012, 120, 1042–1048. [Google Scholar] [CrossRef] [PubMed]
- Larsson, H.J.; Eaton, W.W.; Madsen, K.M.; Vestergaard, M.; Olesen, A.V.; Agerbo, E.; Schendel, D.; Thorsen, P.; Mortensen, P.B. Risk factors for autism: Perinatal factors, parental psychiatric history, and socioeconomic status. Am. J. Epidemiol. 2005, 161, 916–925; discussion 926–928. [Google Scholar] [CrossRef] [PubMed]
- Larsson, M.; Weiss, B.; Janson, S.; Sundell, J.; Bornehag, C.G. Associations between indoor environmental factors and parental-reported autistic spectrum disorders in children 6–8 years of age. Neurotoxicology 2009, 30, 822–831. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.K.; Gardner, R.M.; Dal, H.; Svensson, A.; Galanti, M.R.; Rai, D.; Dalman, C.; Magnusson, C. Brief report: Maternal smoking during pregnancy and autism spectrum disorders. J. Autism Dev. Disord. 2012, 42, 2000–2005. [Google Scholar] [CrossRef] [PubMed]
- Maimburg, R.D.; Vaeth, M. Perinatal risk factors and infantile autism. Acta Psychiatr. Scand. 2006, 114, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Mrozek-Budzyn, D.; Majewska, R.; Kieltyka, A. Prenatal, perinatal and neonatal risk factors for autism—Study in Poland. Cent. Eur. J. Med. 2013, 8, 424–430. [Google Scholar] [CrossRef]
- Xiang, A.H.; Wang, X.; Martinez, M.P.; Walthall, J.C.; Curry, E.S.; Page, K.; Buchanan, T.A.; Coleman, K.J.; Getahun, D. Association of maternal diabetes with autism in offspring. JAMA 2015, 313, 1425–1434. [Google Scholar] [CrossRef] [PubMed]
- Tiesler, C.M.; Heinrich, J. Prenatal nicotine exposure and child behavioural problems. Eur. Child Adolesc. Psychiatry 2014, 23, 913–929. [Google Scholar] [CrossRef] [PubMed]
- Dwyer, J.B.; McQuown, S.C.; Leslie, F.M. The dynamic effects of nicotine on the developing brain. Pharmacol. Ther. 2009, 122, 125–139. [Google Scholar] [CrossRef] [PubMed]
- Ekblad, M.; Gissler, M.; Korkeila, J.; Lehtonen, L. Trends and risk groups for smoking during pregnancy in Finland and other Nordic countries. Eur. J. Public Health 2014, 24, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Raisanen, S.; Kramer, M.R.; Gissler, M.; Saari, J.; Hakulinen-Viitanen, T.; Heinonen, S. Smoking during pregnancy was up to 70% more common in the most deprived municipalities—A multilevel analysis of all singleton births during 2005–2010 in Finland. Prev. Med. 2014, 67, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Rai, D.; Lewis, G.; Lundberg, M.; Araya, R.; Svensson, A.; Dalman, C.; Carpenter, P.; Magnusson, C. Parental socioeconomic status and risk of offspring autism spectrum disorders in a Swedish population-based study. J. Am. Acad. Child Adolesc. Psychiat. 2012, 51, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Scherrer, J.F.; Grant, J.D.; Sartor, C.E.; Pergadia, M.L.; Duncan, A.E.; Madden, P.A.; Haber, J.R.; Jacob, T.; Bucholz, K.K.; et al. The effects of maternal smoking during pregnancy on offspring outcomes. Prev. Med. 2010, 50, 13–18. [Google Scholar] [CrossRef] [PubMed]
- James, W.H. Potential explanation of the reported association between maternal smoking and autism. Environ. Health Perspect. 2013, 121. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, S.; Wang, Y.; Gong, X.; Wang, G. A Meta-Analysis of Maternal Smoking during Pregnancy and Autism Spectrum Disorder Risk in Offspring. Int. J. Environ. Res. Public Health 2015, 12, 10418-10431. https://doi.org/10.3390/ijerph120910418
Tang S, Wang Y, Gong X, Wang G. A Meta-Analysis of Maternal Smoking during Pregnancy and Autism Spectrum Disorder Risk in Offspring. International Journal of Environmental Research and Public Health. 2015; 12(9):10418-10431. https://doi.org/10.3390/ijerph120910418
Chicago/Turabian StyleTang, Shiming, Ying Wang, Xuan Gong, and Gaohua Wang. 2015. "A Meta-Analysis of Maternal Smoking during Pregnancy and Autism Spectrum Disorder Risk in Offspring" International Journal of Environmental Research and Public Health 12, no. 9: 10418-10431. https://doi.org/10.3390/ijerph120910418
APA StyleTang, S., Wang, Y., Gong, X., & Wang, G. (2015). A Meta-Analysis of Maternal Smoking during Pregnancy and Autism Spectrum Disorder Risk in Offspring. International Journal of Environmental Research and Public Health, 12(9), 10418-10431. https://doi.org/10.3390/ijerph120910418