
The Effect of a 12-Week Omega-3 Supplementation on Body Composition, Muscle Strength and Physical Performance in Elderly Individuals with Decreased Muscle Mass

 ,
,
Abstract
:1. Introduction
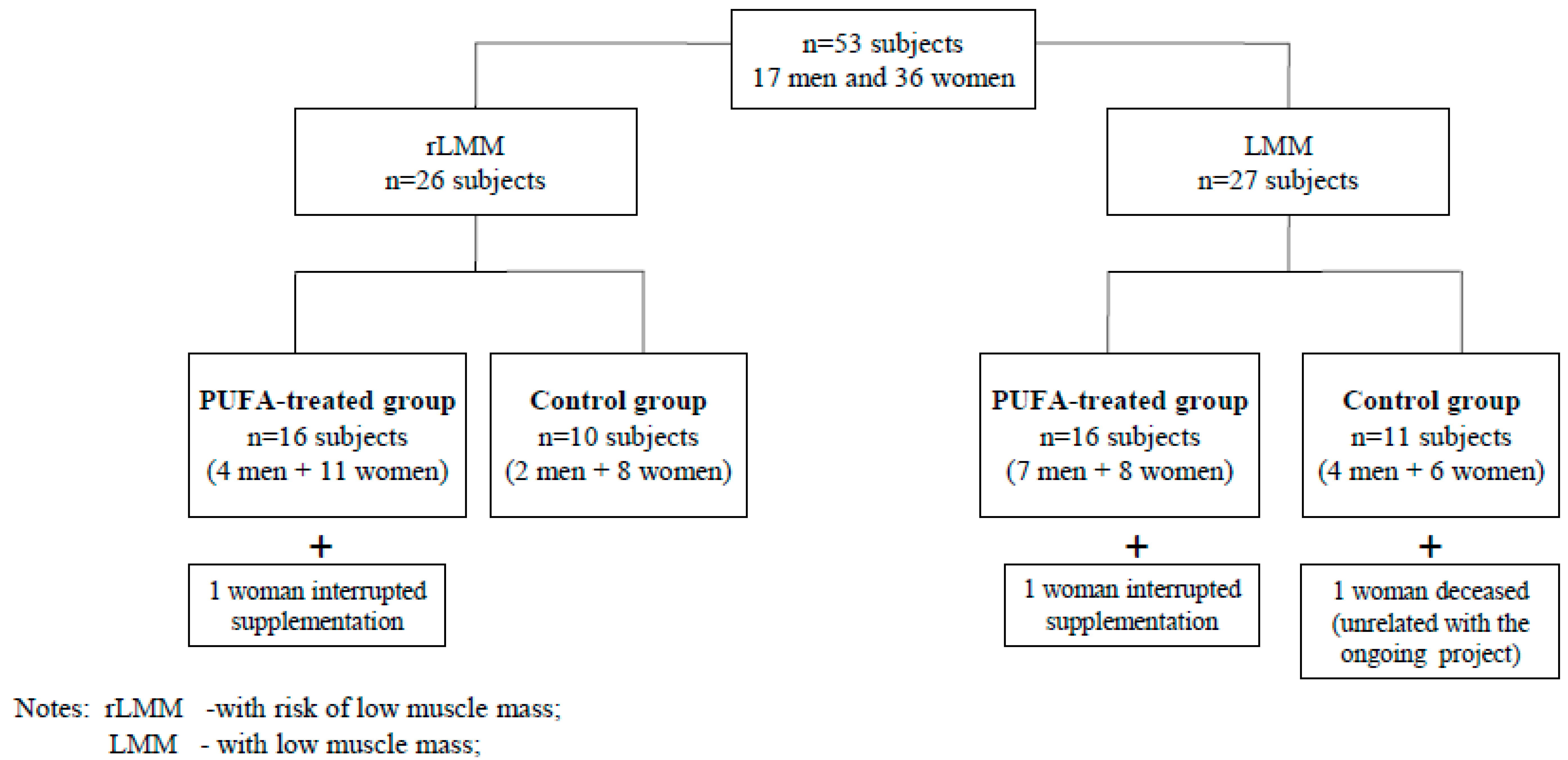
2. Material
Study Population
- low muscle mass or the risk of occurrence,
- lack of cognitive function disorders,
- ability to keep a vertical position, which was required for the performance of the body composition test by means of the bioimpedance analysis, due to the type of analyser used.
- intake of any steroids,
- intake of anti-platelet and anti-thrombotic drugs, due to the anticoagulant activity of omega-3 fatty acids,
- intake of polyunsaturated omega-3 fatty acids supplements during the 3 months previous to the study,
- presence of metal implants, such as a knee or hip endoprosthesis, or a pacemaker, which is a contraindication for a study conducted by means of bioimpedance analysis.

3. Method
3.1. Assessment of Body Composition
3.2. Assessment of Cognitive Function
3.3. Nutritional Assessment
3.4. Assessment of Independence in Activities of Daily Living
3.5. Assessment of the Muscle Strength and Physical Performance
3.6. Statistical Analysis
4. Results

{kind=link}
| Variable | PUFA-Treated Groups: LMM + rLMM | Control Groups: LMM + rLMM | p |
|---|---|---|---|
| Sex | |||
| Women (n) | 19 | 14 | |
| Men (n) | 11 | 6 | |
| Age (years) | 74.97 ± 8.23 | 74.85 ± 7.49 | 0.96 |
| AMTS (points) | 9.00 ± 0.80 * | 8.95 ± 0.92 ** | 0.88 |
| Katz’ index (points) | 5.92 ± 0.30 | 5.70 ± 1.12 | 0.59 |
| Lawton scale (points) | 25.93 ± 2.18 | 24.45 ± 4.38 | 0.17 |
| MNA (points) | 24.76 ± 2.89 * | 23.39 ± 3.25 ** | 0.16 |
| Variable | LMM PUFA-Treated Group | LMM Control Group | p |
|---|---|---|---|
| Sex | |||
| Women (n) | 8 | 6 | |
| Men (n) | 7 | 4 | |
| Age (years) | 74.87 ± 8.99 | 77.20 ± 6.81 | 0.49 |
| AMTS (points) | 9.14 ± 0.95 * | 9.11 ± 0.93 ** | 0.92 |
| Katz’ index (points) | 5.90 ± 0.39 | 5.45 ± 1.57 | 0.35 |
| Lawton scale (points) | 25.33 ± 2.89 | 22.50 ± 5.50 | 0.08 |
| MNA (points) | 24.53 ± 2.77 | 21.60 ± 2.98 | 0.02 |
| Variable | rLMM PUFA-Treated Group | rLMM Control Group | p |
|---|---|---|---|
| Sex | |||
| Women (n) | 11 | 8 | |
| Men (n) | 4 | 2 | |
| Age (years) | 75.07 ± 7.71 | 72.50 ± 7.74 | 0.42 |
| AMTS (points) | 8.87 ± 0.64 | 8.80 ± 0.92 | 0.98 |
| Katz’ index (points) | 5.93 ± 0.18 | 5.95 ± 0.16 | 0.84 |
| Lawton scale (points) | 26.53 ± 0.83 | 26.40 ± 1.35 | 0.88 |
| MNA (points) | 25.00 ± 3.10 | 25.39 ± 2.29 | 0.75 |
5. Discussion
| Variable | PUFA-Treated Groups: LMM + rLMM | Control Groups: LMM + rLMM | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Post-Pre Difference | Pre | Post | Post-Pre Difference | p * | |
| Sex | |||||||
| Women (n) | 19 | 19 | 14 | 14 | |||
| Men (n) | 11 | 11 | 6 | 6 | |||
| Age (years) | 74.97 ± 8.23 | 74.85 ± 7.49 | |||||
| Height (m) | 1.57 ± 0.08 | 1.59 ± 0.09 | |||||
| Weight (kg) | 57.56 ± 8.43 | 57.66 ± 8.94 | 0.10 ± 1.71 | 57.96 ± 11.50 | 58.33 ± 11.68 | 0.37 ± 1.68 | 0.99 |
| Body Mass Index (kg/m2) | 23.41 ± 3.14 | 23.44 ± 3.36 | 0.03 ± 0.72 | 22.93 ± 3.39 | 23.06 ± 3.38 | 0.13 ± 0.66 | 0.97 |
| Skeletal Muscle Mass (kg) | 21.46 ± 3.89 | 21.54 ± 4.17 | 0.08 ± 1.09 | 21.41 ± 4.19 | 21.47 ± 4.62 | 0.06 ± 1.00 | 0.99 |
| Fat (kg) | 17.20 ± 6.79 | 17.48 ± 7.36 | 0.28 ± 1.64 | 17.75 ± 6.44 | 18.08 ± 6.52 | 0.33 ± 2.03 | 0.94 |
| Percent Body Fat (%) | 29.48 ± 9.08 | 29.81 ± 9.47 | 0.33 ± 2.33 | 30.11 ± 6.74 | 30.60 ± 7.25 | 0.49 ± 2.87 | 0.92 |
| Total Body Water (l) | 29.68 ± 5.09 | 29.53 ± 5.27 | −0.15 ± 1.15 | 29.56 ± 5.27 | 29.58 ± 5.84 | 0.02 ± 1.29 | 0.98 |
| Fat-Free Mass (kg) | 40.36 ± 6.78 | 40.19 ± 7.06 | −0.18 ± 1.55 | 40.21 ± 7.10 | 40.25 ± 7.91 | 0.04 ± 1.78 | 0.98 |
| Segmental Lean-Right Arm (kg) | 2.11 ± 0.53 | 2.09 ± 0.57 | −0.01 ± 0.16 | 2.01 ± 0.57 | 2.03 ± 0.58 | 0.02 ± 0.11 | 0.98 |
| Segmental Lean-Left Arm (kg) | 2.08 ± 0.54 | 2.06 ± 0.57 | −0.02 ± 0.17 | 1.97 ± 0.55 | 2.02 ± 0.59 | 0.05 ± 0.12 | 0.95 |
| Segmental Lean-Right Leg (kg) | 5.62 ± 1.29 | 5.64 ± 1.26 | 0.02 ± 0.20 | 5.68 ± 1.40 | 5.62 ± 1.43 | −0.05 ± 0.29 | 0.98 |
| Segmental Lean-Left Leg(kg) | 5.63 ± 1.24 | 5.63 ± 1.21 | 0.00 ± 0.20 | 5.67 ± 1.28 | 5.65 ± 1.37 | −0.02 ± 0.32 | 0.99 |
| Appendicular Lean Mass (kg) | 15.43 ± 3.48 | 15.42 ± 3.49 | −0.01 ± 0.63 | 15.33 ± 3.66 | 15.33 ± 3.86 | 0.00 ± 0.72 | 0.99 |
| ALM index (kg/m2) | 6.19 ± 0.82 | 6.19 ± 0.82 | 0.00 ± 0.26 | 6.01 ± 0.92 | 6.01 ± 1.00 | 0.00 ± 0.29 | 0.80 |
| Average Muscle Strength (kg) | 25.70 ± 7.20 | 25.53 ± 7.18 | −0.17 ± 1.91 | 21.66 ± 8.16 ** | 22.51 ± 7.12 ** | 0.85 ± 3.14 ** | 0.17 |
| Timed Up and Go Test (s) | 6.97 ± 2.66 ** | 7.15 ± 1.86 * | 0.17 ± 1.17 * | 7.82 ± 2.66 ** | 7.95 ± 2.84 ** | 0.13 ± 1.13 ** | 0.62 |
| 4-meter Walking Test (s) | 1.43 ± 0.37 *** | 1.57 ± 0.47 *** | 0.14 ± 0.39 *** | 1.32 ± 0.38 ** | 1.51 ± 0.59 ** | 0.19 ± 0.49 ** | 0.32 |
| Variable | LMM PUFA-Treated Group | LMM Control Group | p * | ||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Post-Pre Difference | Pre | Post | Post-Pre Difference | ||
| Sex | |||||||
| Women (n) | 8 | 8 | 6 | 6 | |||
| Men (n) | 7 | 7 | 4 | 4 | |||
| Age (years) | 74.87 ± 8.99 | 77.20 ± 6.81 | |||||
| Height (m) | 1.57 ± 0.07 | 1.58 ± 0.10 | |||||
| Weight (kg) | 57.23 ± 9.41 | 57.07 ± 9.81 | –0.17 ± 1.54 | 55.52 ± 12.47 | 56.03 ± 12.33 | 0.51 ± 1.66 | 0.83 |
| Body Mass Index (kg/m2) | 23.08 ± 3.30 | 22.97 ± 3.33 | –0.11 ± 0.64 | 22.10 ± 3.59 | 22.30 ± 3.54 | 0.20 ± 0.67 | 0.69 |
| Skeletal Muscle Mass (kg) | 21.74 ± 3.99 | 21.50 ± 4.18 | –0.24 ± 0.96 | 20.70 ± 4.48 | 20.86 ± 5.13 | 0.16 ± 1.22 | 0.80 |
| Fat (kg) | 16.63 ± 6.15 | 16.99 ± 6.50 | 0.35 ± 0.99 | 16.32 ± 6.60 | 16.58 ± 6.02 | 0.26 ± 2.46 | 0.95 |
| Percent Body Fat (%) | 28.72 ± 7.43 | 29.39 ± 7.70 | 0.67 ± 1.80 | 28.84 ± 6.97 | 29.39 ± 6.84 | 0.55 ± 3.54 | 0.98 |
| Total Body Water (l) | 29.85 ± 5.10 | 29.47 ± 5.32 | –0.38 ± 1.20 | 28.83 ± 5.61 | 29.00 ± 6.51 | 0.17 ± 1.62 | 0.93 |
| Fat-Free Mass (kg) | 40.60 ± 6.77 | 40.08 ± 7.09 | –0.52 ± 1.60 | 39.20 ± 7.60 | 39.45 ± 8.84 | 0.25 ± 2.22 | 0.89 |
| Segmental Lean-Right Arm (kg) | 2.15 ± 0.58 | 2.15 ± 0.62 | –0.01 ± 0.18 | 1.90 ± 0.57 | 1.93 ± 0.61 | 0.03 ± 0.12 | 0.49 |
| Segmental Lean-Left Arm (kg) | 2.13 ± 0.57 | 2.12 ± 0.60 | –0.01 ± 0.20 | 1.87 ± 0.53 | 1.91 ± 0.58 | 0.04 ± 0.15 | 0.49 |
| Segmental Lean-Right Leg (kg) | 5.54 ± 1.12 | 5.55 ± 1.12 | 0.02 ± 0.23 | 5.46 ± 1.51 | 5.44 ± 1.64 | –0.02 ± 0.35 | 0.94 |
| Segmental Lean-Left Leg(kg) | 5.51 ± 1.13 | 5.52 ± 1.13 | 0.01 ± 0.22 | 5.48 ± 1.42 | 5.49 ± 1.59 | 0.02 ± 0.42 | 0.98 |
| Appendicular Lean Mass (kg) | 15.33 ± 3.32 | 15.33 ± 3.41 | 0.01 ± 0.75 | 14.70 ± 3.95 | 14.77 ± 4.35 | 0.07 ± 0.92 | 0.88 |
| ALM index (kg/m2) | 6.12 ± 0.89 | 6.12 ± 0.90 | 0.00 ± 0.30 | 5.77 ± 0.98 | 5.80 ± 1.14 | 0.03 ± 0.36 | 0.53 |
| Average Muscle Strength (kg) | 26.19 ± 7.13 | 26.87 ± 6.65 | 0.68 ± 1.43 | 21.09 ± 7.70 ** | 21.63 ± 6.41 ** | 0.54 ± 2.77 ** | 0.12 |
| Timed Up and Go Test (s) | 7.06 ± 3.51 * | 7.11 ± 2.24 * | 0.05 ± 1.50 * | 8.93 ± 3.12 ** | 9.35 ± 3.46 ** | 0.42 ± 1.18 ** | 0.11 |
| 4-meter Walking Test (s) | 1.46 ± 0.42 *** | 1.57 ± 0.44 *** | 0.11 ± 0.26 *** | 1.16 ± 0.27 ** | 1.25 ± 0.23 ** | 0.09 ± 0.13 ** | 0.06 |
| Variable | rLMM PUFA-Treated Group | rLMM Control Group | p * | ||||
|---|---|---|---|---|---|---|---|
| Pre | Post | Post-Pre Difference | Pre | Post | Post-Pre Difference | ||
| Sex | |||||||
| Women (n) | 11 | 11 | 8 | 8 | |||
| Men (n) | 4 | 4 | 2 | 2 | |||
| Age (years) | 75.07 ± 7.71 | 72.50 ± 7.74 | |||||
| Height (m) | 1.56 ± 0.09 | 1.59 ± 0.08 | |||||
| Weight (kg) | 57.89 ± 7.65 | 58.26 ± 8.29 | 0.37 ± 1.88 | 60.39 ± 10.51 | 60.62 ± 11.14 | 0.23 ± 1.79 | 0.93 |
| Body Mass Index (kg/m2) | 23.74 ± 3.05 | 23.92 ± 3.43 | 0.17 ± 0.80 | 23.76 ± 3.15 | 23.83 ± 3.22 | 0.06 ± 0.68 | 0.97 |
| Skeletal Muscle Mass (kg) | 21.17 ± 3.89 | 21.57 ± 4.31 | 0.40 ± 1.14 | 22.12 ± 3.99 | 22.07 ± 4.24 | −0.05 ± 0.77 | 0.55 |
| Fat (kg) | 17.76 ± 7.55 | 17.97 ± 8.33 | 0.21 ± 2.14 | 19.17 ± 6.28 | 19.57 ± 6.97 | 0.40 ± 1.62 | 0.83 |
| Percent Body Fat (%) | 30.24 ± 10.70 | 30.24 ± 11.23 | 0.00 ± 2.79 | 31.37 ± 6.63 | 31.80 ± 7.80 | 0.43 ± 2.19 | 0.92 |
| Total Body Water (l) | 29.51 ± 5.25 | 29.59 ± 5.41 | 0.09 ± 1.10 | 30.28 ± 5.09 | 30.15 ± 5.38 | −0.13 ± 0.92 | 0.62 |
| Fat-Free Mass (kg) | 40.13 ± 7.01 | 40.29 ± 7.28 | 0.17 ± 1.47 | 41.22 ± 6.81 | 41.05 ± 7.25 | −0.17 ± 1.29 | 0.64 |
| Segmental Lean-Right Arm (kg) | 2.06 ± 0.49 | 2.04 ± 0.53 | −0.02 ± 0.13 | 2.13 ± 0.58 | 2.13 ± 0.56 | 0.00 ± 0.11 | 0.82 |
| Segmental Lean-Left Arm (kg) | 2.03 ± 0.53 | 2.00 ± 0.55 | −0.03 ± 0.14 | 2.08 ± 0.58 | 2.13 ± 0.62 | 0.05 ± 0.10 | 0.66 |
| Segmental Lean-Right Leg (kg) | 5.70 ± 1.48 | 5.73 ± 1.43 | 0.03 ± 0.18 | 5.89 ± 1.32 | 5.81 ± 1.24 | −0.08 ± 0.22 | 0.82 |
| Segmental Lean-Left Leg(kg) | 5.75 ± 1.37 | 5.74 ± 1.32 | −0.01 ± 0.18 | 5.87 ± 1.15 | 5.81 ± 1.17 | −0.06 ± 0.19 | 0.87 |
| Appendicular Lean Mass (kg) | 15.54 ± 3.75 | 15.51 ± 3.68 | −0.03 ± 0.53 | 15.97 ± 3.45 | 15.89 ± 3.46 | −0.08 ± 0.50 | 0.72 |
| ALM index (kg/m2) | 6.26 ± 0.76 | 6.26 ± 0.76 | 0.00 ± 0.22 | 6.25 ± 0.84 | 6.21 ± 0.85 | −0.03 ± 0.20 | 0.98 |
| Average Muscle Strength (kg) | 25.21 ± 7.50 | 24.18 ± 7.66 | −1.03 ± 1.99 | 22.18 ± 8.94 | 23.30 ± 7.96 | 1.12 ± 3.56 | 0.80 |
| Timed Up and Go Test (s) | 6.90 ± 1.79 * | 7.18 ± 1.55 * | 0.28 ± 0.84 * | 6.83 ± 1.77 | 6.69 ± 1.35 | −0.14 ± 1.07 | 0.76 |
| 4-meter Walking Test (s) | 1.40 ± 0.33 | 1.58 ± 0.51 | 0.18 ± 0.49 | 1.47 ± 0.41 | 1.74 ± 0.72 | 0.28 ± 0.66 | 0.76 |
Study Limitations
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Eurostat 2014: Population Structure and Ageing. Available online: http://epp.eurostat.ec.europa.eu/statistics_explained/index.php/Population_structure_and_ageing (accessed on 10 April 2015).
- Rosenberg, I.H. Sarcopenia: Origins and clinical relevance. J. Nutr. 1997, 127, 990–991. [Google Scholar] [CrossRef] [PubMed]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Amer. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef]
- Janssen, I.; Shepard, D.S.; Kaczmarzyk, P.T.; Roubenoff, R. The healthcare costs of sarcopenia in the United States. J. Amer Geriatr. Soc. 2004, 52, 80–85. [Google Scholar] [CrossRef]
- Bauer, J.M.; Sieber, C.C. Sarcopenia and frailty: A clinician’s controversial point of view. Exp. Gerontol. 2008, 43, 674–678. [Google Scholar] [CrossRef] [PubMed]
- Rolland, Y.; Czerwiński, S.; Abellan van Kan, G.; Morley, J.E.; Cesari, M.; Onder, G.; Woo, J.; Baumgartner, R.; Pillard, F.; Boirie, Y.; et al. Sarcopenia: Its assessment, etiology, pathogenesis, consequences and future perspectives. J. Nutr. Health Aging 2008, 12, 433–450. [Google Scholar] [CrossRef] [PubMed]
- Walrand, S.; Guillet, C.; Salles, J.; Cano, N.; Boirie, Y. Physiopathological mechanism of sarcopenia. Clin. Geriatr. Med. 2011, 27, 365–385. [Google Scholar] [CrossRef] [PubMed]
- Drey, M. Sarcopenia—Pathophysiology and clinical relevance. Wien. Med. Wochenschr. 2011, 161, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.; Cooper, C.; Sayer, A.A. Nutrition and sarcopenia: A review of the evidence and implications for preventive strategies. J. Aging Res. 2012, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Millward, D.J. Muscle wasting with age: A new challenge in nutritional care; part 2—management; nutrition and sarcopenia: Evidence for an interaction. Proc. Nutr. Soc. 2012, 1–10. [Google Scholar]
- Volkert, D. The role of nutrition in the prevention of sarcopenia. Wien. Med. Wochenschr. 2011, 161, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Smith, G.I.; Atherton, P.; Reeds, D.N.; Mohammed, B.S.; Rankin, D.; Rennie, M.J.; Mittendorfer, B. Dietary omega-3 fatty acid supplementation increases the rate of muscle protein synthesis in older adults: A randomized controlled trial. Amer. J. Clin. Nutr. 2011, 93, 402–412. [Google Scholar] [CrossRef] [PubMed]
- Noreen, E.E.; Sass, M.J.; Crowe, M.L.; Pabon, V.A.; Brandauer, J.; Averill, L.K. Effects of supplemental fish oil on resting metabolic rate, body composition, and salivary cortisol in healthy adults. J. Int. Soc. Sport. Nutr. 2010. [Google Scholar] [CrossRef] [PubMed]
- Couet, C.; Delarue, J.; Ritz, P. Effect of dietary fish oil on body fat mass and basal fat oxidation in healthy adults. Int. J. Obes. Relat. Metab. Disord. 1997, 21, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Rodacki, C.L.; Rodacki, A.L.; Pereira, G.; Naliwaiko, K.; Coelho, I.; Pequito, D.; Fernandes, L.C. Fish-oil supplementation enhances the effects of strength training in elderly women. Amer. J. Clin. Nutr. 2012, 95, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Cornish, S.M.; Chilibeck, P.D. Alpha-linolenic acid supplementation and resistance training in older adults. Appl. Physiol. Nutr. Metab. 2009, 34, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Krzymińska-Siemaszko, R.; Czepulis, N.; Suwalska, A.; Dworak, L.B.; Fryzowicz, A.; Madej-Dziechciarow, B.; Wieczorowska-Tobis, K. The Significance of body mass index in calculating the cut-off points for low muscle mass in the elderly: Methodological issues. Biomed. Res. 2014. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; Heymsfield, B.; Ross, R. Low relative skeletal muscle mass (sarcopenia) in older person is associated with functional impairment and physical disability. J. Amer. Geriatr. Soc. 2002, 50, 889–896. [Google Scholar] [CrossRef]
- Jitapunkul, S.; Pillay, I.; Ebrahim, S. The abbreviated mental test: Its use and validity. Age Ageing 1991, 20, 332–336. [Google Scholar] [CrossRef] [PubMed]
- MNA Polish Form. Available online: http://www.mna-elderly.com/forms/MNA_polish.pdf (accessed on 10 April 2015).
- Shelkey, M.; Wallace, M. Katz index of independence in activities of daily living (ADL). Available online: http://consultgerirn.org/uploads/File/trythis/try_this_2.pdf (accessed on 10 April 2015).
- Graf, C. The Lawton instrumental activities of daily living (IADL) scale. Available online: http://consultgerirn.org/uploads/File/trythis/try_this_23.pdf (accessed on 10 April 2015).
- Bohannon, R.W. Reference values for the timed up and go test: a descriptive meta-analysis. J Geriatr. Psychiatr. Neurol. 2006, 29, 64–68. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the probability for falls in community-dwelling older adults using the timed “Up & Go” test. Phys. Ther. 2000, 80, 896–903. [Google Scholar] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European working group on Sarcopenia in older people. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Welch, A.A.; MacGregor, A.J.; Minihane, A.M. Dietary fat and fatty acid profile are associated with indices of skeletal muscle mass in women aged 18–79 years. J. Nutr. 2014, 144, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Clark, B.C.; Manini, T.M. Sarcopenia ≠ dynapenia. J. Gerontol. Ser. A-Biol. Sci. Med. 2008, 63, 829–834. [Google Scholar] [CrossRef]
- Manini, T.M.; Clark, B.C. Dynapenia and aging: An update. J. Gerontol. Ser. A-Biol. Sci. Med. 2012, 67, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.M.; Jameson, K.A.; Batelaan, S.F.; Martin, H.J.; Syddall, H.E.; Dennison, E.M.; Cooper, C.; Sayer, A.A. Diet and its relationship with grip strength in community-dwelling older men and women: The Hertfordshire Cohort Study. J. Amer. Geriatr. Soc. 2008, 56, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, J.H.; Kleppinger, A.; Kenny, A.M. Self-reported dietary intake of omega-3 fatty acids and association with bone and lower extremity function. J. Amer. Geriatr. Soc. 2009, 57, 1781–1788. [Google Scholar] [CrossRef] [PubMed]
- Takayama, M.; Arai, Y.; Sasaki, S. Association of marine-origin n-3 polyunsaturated fatty acids consumption and functional mobility in the community-dwelling oldest old. J. Nutr. Health Aging 2013, 17, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Abbatecola, A.M.; Cherubini, A.; Guralnik, J.M.; Andres Lacueva, C.; Ruggiero, C.; Maggio, M.; Bandinelli, S.; Paolisso, G.; Ferrucci, L. Plasma polyunsaturated fatty acids and age-related physical performance decline. Rejuv. Res. 2009, 12, 25–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutchins-Wiese, H.L.; Kleppinger, A.; Annis, K.; Liva, E.; Lammi-Keefe, C.J.; Durham, H.A.; Kenny, A.M. The impact of supplemental n-3 long chain polyunsaturated fatty acids and dietary antioxidants on physical performance in postmenopausal women. J. Nutr. Health Aging 2013, 17, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Ferrucci, L.; Simonsick, E.M.; Salive, M.E.; Wallace, R.B. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N. Engl. J. Med. 1995, 332, 556–561. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, J.; Miyachi, M.; Moreau, K.L.; Dinenno, F.A.; DeSouza, C.A.; Tanaka, H. Age-related reductions in appendicular skeletal muscle mass: Association with habitual aerobic exercise status. Clin. Physiol. Funct. Imaging 2002, 22, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Ling, C.H.; de Craen, A.J.; Slagboom, P.E.; Gunn, D.A.; Stokkel, M.P.; Westendorp, R.G.; Maier, A.B. Accuracy of direct segmental multi-frequency bioimpedance analysis in the assessment of total body and segmental body composition in middle-aged adult population. Clin. Nutr. 2011, 30, 610–615. [Google Scholar] [CrossRef] [PubMed]
- Kaido, T.; Uemoto, S. Direct segmental multi-frequency bioelectrical impedance analysis is useful to evaluate sarcopenia. Amer. J. Transplant. 2013, 13, 2506–2507. [Google Scholar] [CrossRef] [PubMed]
- Karelis, A.D.; Chamberland, G.; Aubertin-Leheudre, M.; Duval, C. Validation of a portable bioelectrical impedance analyzer for the assessment of body composition. Appl. Physiol. Nutr. Metab. 2013, 38, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Naruszewicz, M.; Kozłowska-Wojciechowska, M.; Kornacewicz-Jach, Z.; Członkowska, A.; Januszewicz, A.; Steciwko, A. Expert Group recommendations on dietary consumption and supplementation with omega−3 fatty acids in adults. Family Med. Primary Care. Rev. 2007, 9, 175–176. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krzymińska-Siemaszko, R.; Czepulis, N.; Lewandowicz, M.; Zasadzka, E.; Suwalska, A.; Witowski, J.; Wieczorowska-Tobis, K. The Effect of a 12-Week Omega-3 Supplementation on Body Composition, Muscle Strength and Physical Performance in Elderly Individuals with Decreased Muscle Mass. Int. J. Environ. Res. Public Health 2015, 12, 10558-10574. https://doi.org/10.3390/ijerph120910558
Krzymińska-Siemaszko R, Czepulis N, Lewandowicz M, Zasadzka E, Suwalska A, Witowski J, Wieczorowska-Tobis K. The Effect of a 12-Week Omega-3 Supplementation on Body Composition, Muscle Strength and Physical Performance in Elderly Individuals with Decreased Muscle Mass. International Journal of Environmental Research and Public Health. 2015; 12(9):10558-10574. https://doi.org/10.3390/ijerph120910558
Chicago/Turabian StyleKrzymińska-Siemaszko, Roma, Natasza Czepulis, Marta Lewandowicz, Ewa Zasadzka, Aleksandra Suwalska, Janusz Witowski, and Katarzyna Wieczorowska-Tobis. 2015. "The Effect of a 12-Week Omega-3 Supplementation on Body Composition, Muscle Strength and Physical Performance in Elderly Individuals with Decreased Muscle Mass" International Journal of Environmental Research and Public Health 12, no. 9: 10558-10574. https://doi.org/10.3390/ijerph120910558
APA StyleKrzymińska-Siemaszko, R., Czepulis, N., Lewandowicz, M., Zasadzka, E., Suwalska, A., Witowski, J., & Wieczorowska-Tobis, K. (2015). The Effect of a 12-Week Omega-3 Supplementation on Body Composition, Muscle Strength and Physical Performance in Elderly Individuals with Decreased Muscle Mass. International Journal of Environmental Research and Public Health, 12(9), 10558-10574. https://doi.org/10.3390/ijerph120910558