
Childhood ADHD Symptoms: Association with Parental Social Networks and Mental Health Service Use during Adolescence

Abstract
:1. Introduction
2. Experimental Section
2.1. Participants and Procedures
2.2. Study Variable Construction
2.2.1. Sociodemographic Characteristics
2.2.2. Adolescent Clinical Characteristics
Psychopathology
Impairment
Emotional and Behavioral Functioning
2.2.3. Adolescent Perceived Stigma
2.2.4. Parental Social Network Characteristics
2.2.5. Caregiver Stress
2.2.6. Mental Health Service Use
2.3. Statistical Analyses
3. Results and Discussion
3.1. Parent Network Structure and Support Levels by Type of Support Source

{kind=link}
| Spouse | Parent | Other Family | Friends | Other | Healthcare | Teacher | |
| N a = 230 | N a = 196 | N a = 420 | N a = 356 | N a = 154 | N a = 67 | N a = 18 | |
| n b = 230 | n b = 165 | n b = 227 | n b = 195 | n b = 105 | n b = 54 | n b = 15 | |
| Network Structure | |||||||
| Contact Frequency c | 4.9 (0.5) | 4.5 (0.7) | 4.4 (0.7) | 4.4 (0.7) | 4.4 (0.7) | 2.6 (0.7) | 3.6 (0.7) |
| Relation Length d | 4.9 (0.3) | 5.0 (0.2) | 5.0 (0.1) | 4.8 (0.5) | 4.5 (0.9) | 3.6 (1.4) | 2.8 (1.3) |
| Geographical Distance e | 1.6 (1.3) | 4.7 (1.6) | 4.6 (1.6) | 4.3 (1.0) | 4.2 (0.8) | 4.1 (0.3) | 4.2 (0.6) |
| Emotional Closeness f | 1.2 (0.4) | 1.2 (0.5) | 1.1 (0.3) | 1.2 (0.4) | 1.5 (0.6) | 2.0 (0.7) | 2.1 (0.4) |
| Network Support | |||||||
| Affective g | 3.5 (0.8) | 3.6 (0.7) | 3.6 (0.5) | 3.6 (0.5) | 3.4 (0.7) | 3.0 (0.8) | 2.9 (1.0) |
| Affirmative g | 3.5 (0.6) | 3.6 (0.7) | 3.6 (0.5) | 3.6 (0.5) | 3.4 (0.7) | 3.0 (0.8) | 2.9 (1.0) |
| Instrumental g | 3.6 (0.8) | 2.8 (1.4) | 2.8 (1.2) | 2.7 (1.1) | 1.9 (1.3) | 0.5 (0.8) | 0.8 (1.3) |
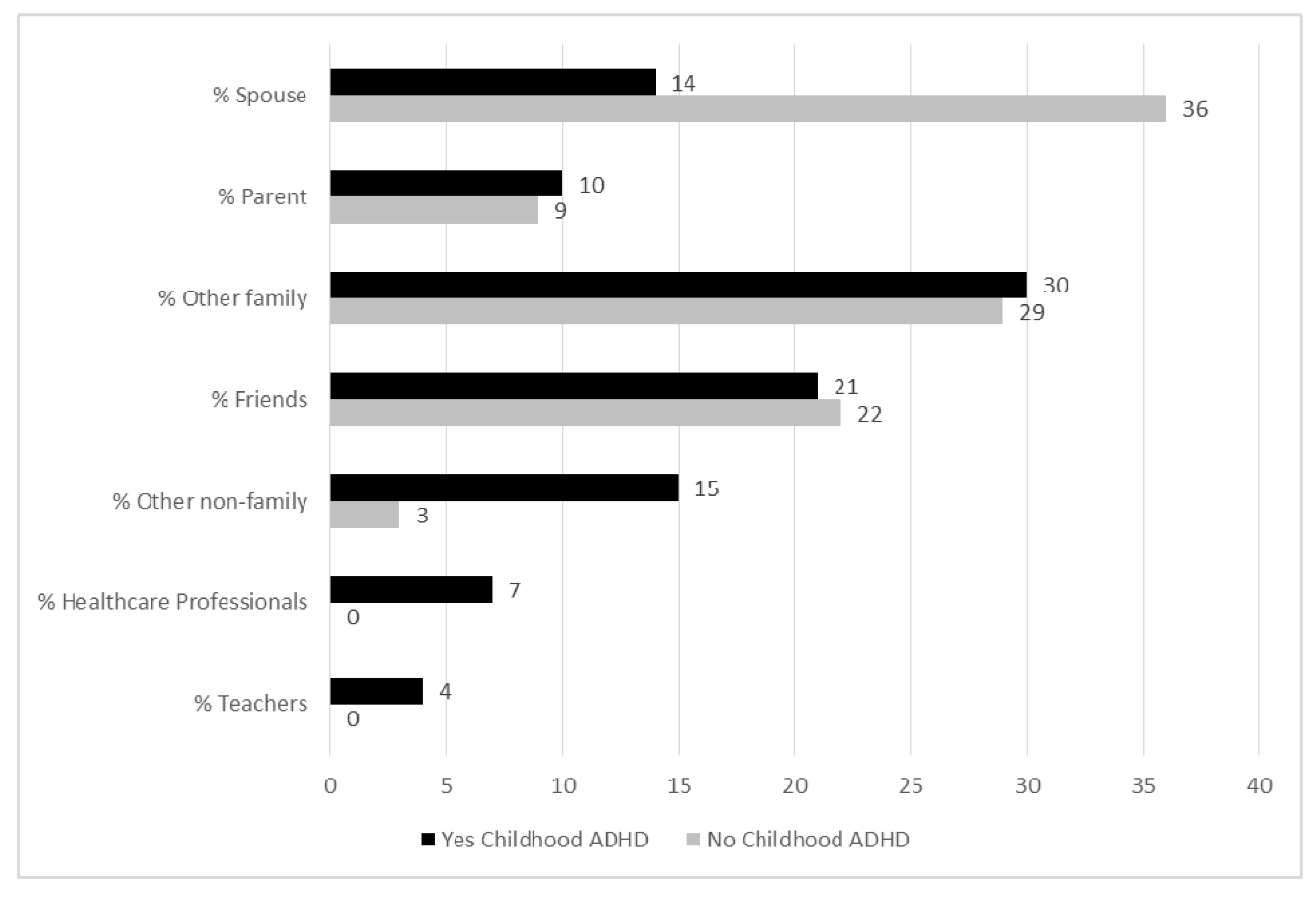
3.2. Parent Network Support Type Composition by ADHD Status

3.3. Parent Network Characteristics by ADHD Status, Poverty and Race
| Overall Mean (SD) | By ADHD Risk Status Mean (SD) | By Poverty a Mean (SD) | By Race b Mean (SD) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Low N = 167 | High N = 207 | p | Non-Poor N = 178 | Poor N = 196 | p | C N = 237 | AA N = 137 | p | ||
| Network Size | 3.9 (2.2) | 3.7 (2.2) | 3.9 (2.3) | 0.57 | 4.4 (2.3) | 3.4 (2.1) | <0.0001 | 4.2 (2.3) | 3.3 (2.1) | <0.001 |
| Network Structure | ||||||||||
| Contact Frequency c | 4.5 (0.6) | 4.5 (0.6) | 4.5 (0.7) | 0.34 | 4.4 (0.7) | 4.6 (0.6) | <0.0001 | 4.4 (0.7) | 4.6 (0.6) | <0.0001 |
| Relation Length d | 4.9 (0.4) | 5.0 (0.2) | 4.9 (0.5) | <0.01 | 4.9 (0.3) | 4.9 (0.4) | 0.42 | 4.9 (0.4) | 4.9 (0.3) | 0.81 |
| Closeness e | 1.2 (0.4) | 1.1 (0.3) | 1.2 (0.4) | <0.05 | 1.2 (0.4) | 1.1 (0.4) | 0.06 | 1.2 (0.4) | 1.1 (0.3) | <0.05 |
| Geographic Distance f | 4.0 (1.2) | 4.0 (1.3) | 4.1 (1.1) | 0.40 | 4.2 (1.2) | 3.8 (1.2) | <0.01 | 4.1 (1.2) | 3.8 (1.2) | <0.05 |
| Network Support | ||||||||||
| Affective g | 3.4 (0.8) | 3.6 (0.7) | 3.3 (0.8) | <0.0001 | 3.5 (0.6) | 3.4 (0.9) | 0.94 | 3.4 (0.6) | 3.5 (1.0) | 0.25 |
| Affirmative g | 3.3 (0.7) | 3.4 (0.7) | 3.2 (0.8) | <0.01 | 3.3 (0.6) | 3.3 (0.9) | 0.60 | 3.3 (0.6) | 3.3 (1.0) | 0.33 |
| Instrumental g | 2.7 (1.0) | 2.9 (0.9) | 2.4 (1.0) | <0.0001 | 2.6 (0.9) | 2.8 (1.1) | <0.05 | 2.5 (0.9) | 2.9 (1.1) | <0.001 |
3.4. Predictors of Caregiver Stress
3.5. Predicting Adolescent Mental Health Service Utilization
| Model 1 (Network) | Model 2 (Network, Parent Perspectives) | Model 3 (Network, Parent Perspectives, Adolescent Perspectives) | ||||
|---|---|---|---|---|---|---|
| OR | [95% CI] | OR | [95% CI] | OR | [95% CI] | |
| Network Characteristics | ||||||
| Network size | 1.07 | [0.97, 1.19] | 1.04 | [0.92, 1.17] | 1.05 | [0.92, 1.19] |
| Affective support | 0.68 | [0.36, 1.28] | 0.85 | [0.41, 1.75] | 0.73 | [0.34, 1.60] |
| Affirmation support | 1.92 | [1.03, 3.57] | 2.50 | [1.23, 5.06] | 2.60 | [1.23, 5.51] |
| Instrumental support | 0.69 | [0.52, 0.92] | 0.93 | [0.66, 1.30] | 0.91 | [0.63, 1.32] |
| Parent Perspectives | ||||||
| Anxiety/Depression a | 2.12 | [1.11, 4.08] | 1.62 | [0.78, 3.29] | ||
| ADHD a | 1.88 | [1.18, 3.01] | 1.97 | [1.18, 3.29] | ||
| CIS | 1.02 | [0.96, 1.08] | 0.98 | [0.92, 1.05] | ||
| Caregiver strain | 1.23 | [1.02, 1.50] | 1.29 | [1.03, 1.60] | ||
| Adolescent Perspectives | ||||||
| ESI | 1.02 | [0.97, 1.06] | ||||
| CIS | 1.05 | [0.99, 1.11] | ||||
| ADHD Stigma | 0.30 | [0.15, 0.59] | ||||
| 2 LOG L b | 419.2 | 347.8, (71.397,4), p < 0.0001 c | 307.1, (40.625,3), p < 0.0001 c | |||
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Merikangas, K.R.; He, J.P.; Burstein, M.; Swanson, S.A.; Avenevoli, S.; Cui, L.; Benjet, C.; Georgiades, K.; Swendsen, J. Lifetime prevalence of mental disorders in U.S. Adolescents: Results from the National Comorbidity Survey Replication—Adolescent Supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 980–989. [Google Scholar] [PubMed]
- Danckaerts, M.; Sonuga-Barke, E.J.; Banaschewski, T.; Buitelaar, J.; Dopfner, M.; Hollis, C.; Santosh, P.; Rothenberger, A.; Sergeant, J.; Steinhausen, H.C.; et al. The quality of life of children with attention deficit/hyperactivity disorder: A systematic review. Eur. Child Adolesc. Psychiatry 2010, 19, 83–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loe, I.M.; Feldman, H.M. Academic and educational outcomes of children with ADHD. Ambul. Pediatr. 2007, 7, 82–90. [Google Scholar] [CrossRef] [PubMed]
- Coghill, D.; Soutullo, C.; d’Aubuisson, C.; Preuss, U.; Lindback, T.; Silverberg, M.; Buitelaar, J. Impact of attention-deficit/hyperactivity disorder on the patient and family: Results from a European survey. Child Adolesc. Psychiatry Ment. Health 2008, 2. [Google Scholar] [CrossRef] [PubMed]
- Faraone, S.V.; Buitelaar, J. Comparing the efficacy of stimulants for ADHD in children and adolescents using meta-analysis. Eur. Child Adolesc. Psychiatry 2010, 19, 353–364. [Google Scholar] [CrossRef] [PubMed]
- Watson, S.M.; Richels, C.; Michalek, A.P.; Raymer, A. Psychosocial treatments for ADHD: A systematic appraisal of the evidence. J. Atten. Disord. 2015, 19, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Wolraich, M.; Brown, L.; Brown, R.T.; DuPaul, G.; Earls, M.; Feldman, H.M.; Ganiats, T.G.; Kaplanek, B.; Meyer, B.; Perrin, J.; et al. ADHD: Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics 2011, 128, 1007–1022. [Google Scholar] [PubMed]
- Anastopoulos, A.D.; Shelton, T.L. Standardization of Assessment Procedures for ADHD; Kluwer Academic/Plenum: New York, NY, USA, 2001. [Google Scholar]
- Barkley, R.A.; Edwards, G. Diagnostic Interview, Behavior Rating Scales, and the Medical Examination, 2nd ed.; Guilford Press: New York, NY, USA, 1998. [Google Scholar]
- Garland, A.F.; Lau, A.S.; Yeh, M.; McCabe, K.M.; Hough, R.L.; Landsverk, J.A. Racial and ethnic differences in utilization of mental health services among high-risk youths. Am. J. Psychiatry 2005, 162, 1336–1343. [Google Scholar] [CrossRef] [PubMed]
- Merikangas, K.R.; He, J.P.; Burstein, M.; Swendsen, J.; Avenevoli, S.; Case, B.; Georgiades, K.; Heaton, L.; Swanson, S.; Olfson, M. Service utilization for lifetime mental disorders in U.S. Adolescents: Results of the National Comorbidity Survey—Adolescent Supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 2011, 50, 32–45. [Google Scholar] [CrossRef] [PubMed]
- Costello, E.J.; Pescosolido, B.A.; Angold, A.; Burns, B.J. A family network-based model of access to child mental health services. Res. Community Ment. Health 1998, 9, 165–190. [Google Scholar]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Pescosolido, B.A. Beyond rational choice: The social dynamics of how people seek help. Am. J. Sociol. 1992, 97, 1096–1138. [Google Scholar] [CrossRef]
- Bussing, R.; Zima, B.T.; Gary, F.A.; Mason, D.M.; Leon, C.E.; Sinha, K.; Garvan, C.W. Social networks, caregiver strain, and utilization of mental health services among elementary school students at high risk for ADHD. J. Am. Acad. Child Adolesc. Psychiatry 2003, 42, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Rini, C.; Manne, S.; DuHamel, K.; Austin, J.; Ostroff, J.; Boulad, F.; Parsons, S.K.; Martini, R.; Williams, S.E.; Mee, L.; et al. Social support from family and friends as a buffer of low spousal support among mothers of critically ill children: A multilevel modeling approach. Health Psychol. 2008, 27, 593–603. [Google Scholar] [CrossRef] [PubMed]
- Srebnik, D.; Cauce, A.M.; Baydar, N. Help-seeking pathways for children and adolescents. J. Emot. Behav. Disord. 1996, 4, 210–220. [Google Scholar] [CrossRef]
- Hammer, M. Influence of small social networks as factors on mental hospital admission. Hum. Organ. 1963, 22, 243–251. [Google Scholar] [CrossRef]
- McKinlay, J.B. Social networks, lay consultation, and help-seeking behavior. Soc. Forces 1973, 51, 275–292. [Google Scholar] [CrossRef]
- Kadushin, C. The friends and supporters of psychotherapy: On social circles in urban life. Am. Sociol. Rev. 1966, 31, 786–802. [Google Scholar] [CrossRef] [PubMed]
- Podolski, C.L.; Nigg, J.T. Parent stress and coping in relation to child ADHD severity and associated child disruptive behavior problems. J. Clin. Child Psychol. 2001, 30, 503–513. [Google Scholar] [CrossRef] [PubMed]
- DeWolfe, N.; Byrne, J.M.; Bawden, H.N. ADHD in preschool children: Parent-rated psychosocial correlates. Dev. Med. Child Neurol. 2000, 42, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Graziano, P.A.; McNamara, J.P.; Geffken, G.R.; Reid, A. Severity of children’s ADHD symptoms and parenting stress: A multiple mediation model of self-regulation. J. Abnorm. Child Psychol. 2011, 39, 1073–1083. [Google Scholar] [CrossRef] [PubMed]
- Lovell, B.; Moss, M.; Wetherell, M. The psychosocial, endocrine and immune consequences of caring for a child with autism or ADHD. Psychoneuroendocrinology 2012, 37, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Tessler, R.; Mechanic, D. Factors affecting children’s use of physician services in a prepaid group practice. Med. Care 1978, 16, 33–46. [Google Scholar] [CrossRef] [PubMed]
- Janicke, D.M.; Finney, J.W.; Riley, A.W. Children’s health care use: A prospective investigation of factors related to care-seeking. Med. Care 2001, 39, 990–1001. [Google Scholar] [CrossRef] [PubMed]
- Janicke, D.M.; Finney, J.W. Children’s primary health care services: A social-cognitive model of sustained high use. Clin. Psychol. Sci. Pract. 2001, 8, 228–241. [Google Scholar] [CrossRef]
- Janicke, D.M.; Finney, J.W. Children’s primary health care services: Social-cognitive factors related to utilization. J. Pediatr. Psychol. 2003, 28, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Schor, E.L.; Starfield, B.; Stidley, C.; Hankin, J. Family health: Utilization and effects of family membership. Med. Care 1987, 25, 616–626. [Google Scholar] [CrossRef] [PubMed]
- Raphael, J.L.; Zhang, Y.; Liu, H.; Giardino, A.P. Parenting stress in US families: Implications for paediatric healthcare utilization. Child Care Health Dev. 2010, 36, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Angold, A.; Messer, S.C.; Stangl, D.; Farmer, E.M.; Costello, E.J.; Burns, B.J. Perceived parental burden and service use for child and adolescent psychiatric disorders. Am. J. Public Health 1998, 88, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Hinojosa, M.S.; Hinojosa, R.; Fernandez-Baca, D.; Knapp, C.; Thompson, L.A. Parental strain, parental health, and community characteristics among children with attention deficit-hyperactivity disorder. Acad. Pediatr. 2012, 12, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Hinojosa, M.S.; Hinojosa, R.; Fernandez-Baca, D.; Knapp, C.; Thompson, L.A.; Christou, A. Racial and ethnic variation in ADHD, comorbid illnesses, and parental strain. J. Health Care Poor Underserved 2012, 23, 273–289. [Google Scholar] [CrossRef] [PubMed]
- Theule, J.; Wiener, J.; Rogers, M.; Marton, I. Predicting parenting stress in families of children with ADHD: Parent and contextual factors. J. Child Fam. Stud. 2011, 20, 640–647. [Google Scholar] [CrossRef]
- Finzi-Dottan, R.; Triwitz, Y.S.; Golubchik, P. Predictors of stress-related growth in parents of children with ADHD. Res. Dev. Disabil. 2011, 32, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Lovell, B.; Moss, M.; Wetherell, M.A. With a little help from my friends: Psychological, endocrine and health corollaries of social support in parental caregivers of children with autism or ADHD. Res. Dev. Disabil. 2012, 33, 682–687. [Google Scholar] [CrossRef] [PubMed]
- Bussing, R.; Zima, B.T.; Mason, D.M.; Porter, P.C.; Garvan, C.W. Receiving treatment for attention-deficit hyperactivity disorder: Do the perspectives of adolescents matter? J. Adolesc. Health 2011, 49, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.W.; Sibley, M.; Serpell, Z.N. Changes in caregiver strain over time in young adolescents with ADHD: The role of oppositional and delinquent behavior. J. Atten. Disord. 2009, 12, 516–524. [Google Scholar] [CrossRef] [PubMed]
- DosReis, S.; Barksdale, C.L.; Sherman, A.; Maloney, K.; Charach, A. Stigmatizing experiences of parents of children with a new diagnosis of ADHD. Psychiatr. Serv. 2010, 61, 811–816. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.K.; Pescosolido, B.A.; Olafsdottir, S.; McLeod, J.D. The construction of fear: Americans’ preferences for social distance from children and adolescents with mental health problems. J. Health Soc. Behav. 2007, 48, 50–67. [Google Scholar] [CrossRef] [PubMed]
- Wolraich, M.L.; Lambert, W.; Doffing, M.A.; Bickman, L.; Simmons, T.; Worley, K. Psychometric properties of the vanderbilt ADHD diagnostic parent rating scale in a referred population. J. Pediatr. Psychol. 2003, 28, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Bird, H.R.; Shaffer, D.; Fisher, P.; Gould, M.S. The columbia impairment scale (CIS): Pilot findings on a measure of global impairment for children and adolescents. Int. J. Methods Psychiatr. Res. 1993, 3, 167–176. [Google Scholar]
- Reynolds, C.R.; Kamphaus, R.W. The Clinician’s Guide to the Behavior Assessment System for Children (BASC); Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- Kellison, I.; Bussing, R.; Bell, L.; Garvan, C. Assessment of stigma associated with attention-deficit hyperactivity disorder: Psychometric evaluation of the ADHD stigma questionnaire. Psychiatry Res. 2010, 178, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Norbeck, J.S.; Lindsey, A.M.; Carrieri, V.L. The development of an instrument to measure social support. Nurs. Res. 1981, 30, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Norbeck, J.S.; Lindsey, A.M.; Carrieri, V.L. Further development of the norbeck social support questionnaire: Normative data and validity testing. Nurs. Res. 1983, 32, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Auslander, G.K.; Litwin, H. Social support networks and formal help seeking: Differences between applicants to social services and a nonapplicant sample. J. Gerontol. 1990, 45, S112–S119. [Google Scholar] [CrossRef] [PubMed]
- Brannan, A.M.; Heflinger, C.A.; Bickman, L. The caregiver strain questionnaire: Measuring the impact on the family of living with a child with serious emotional disturbance. J. Emot. Behav. Disord. 1997, 5, 212–222. [Google Scholar] [CrossRef]
- Kang, E.J.; Brannan, A.M.; Heflinger, C.A. Racial differences in reports of caregiver strain among caregivers of children with emotional and behavioral problems. J. Child Fam. Stud. 2005, 14, 43–56. [Google Scholar] [CrossRef]
- Burns, B.J.; Angold, A.; Magruder-Habib, K.; Costello, E.J.; Patrick, M.K.S. The Child and Adolescent Services Assessment (CASA); Duke University Medical Center: Durham, NC, USA, 1992. [Google Scholar]
- Ascher, B.H.; Farmer, E.M.Z.; Burns, B.J.; Angold, A. The child and adolescent services assessment (CASA): Description and psychometrics. J. Emot. Behav. Disord. 1996, 4, 12–20. [Google Scholar] [CrossRef]
- Bussing, R.; Mason, D.M.; Leon, C.E.; Sinha, K. Agreement between casa parent reports and provider records of children’s ADHD services. J. Behav. Health Serv. Res. 2003, 30, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Barkley, R.A.; Fischer, M.; Edelbrock, C.; Smallish, L. The adolescent outcome of hyperactive children diagnosed by research criteria—iii. Mother-child interactions, family conflicts and maternal psychopathology. J. Child Psychol. Psychiatry 1991, 32, 233–255. [Google Scholar] [CrossRef] [PubMed]
- Wymbs, B.T.; Pelham, W.E., Jr.; Molina, B.S.; Gnagy, E.M.; Wilson, T.K.; Greenhouse, J.B. Rate and predictors of divorce among parents of youths with ADHD. J. Consult. Clin. Psychol. 2008, 76, 735–744. [Google Scholar] [CrossRef] [PubMed]
- Kvist, A.P.; Nielsen, H.S.; Simonsen, M. The importance of children’s ADHD for parents’ relationship stability and labor supply. Soc. Sci. Med. 2013, 88, 30–38. [Google Scholar] [CrossRef] [PubMed]
- Koro-Ljungberg, M.; Bussing, R. The management of courtesy stigma in the lives of families with teenagers with ADHD. J. Fam. Issues 2009, 30, 1175–1200. [Google Scholar] [CrossRef]
- Bussing, R.; Mehta, A.S. Stigmatization and self-perception of youth with attention deficit/hyperactivity disorder. Patient Intell. 2013, 5, 15–27. [Google Scholar] [CrossRef]
- Cadman, T.; Eklund, H.; Howley, D.; Hayward, H.; Clarke, H.; Findon, J.; Xenitidis, K.; Murphy, D.; Asherson, P.; Glaser, K. Caregiver burden as people with autism spectrum disorder and attention-deficit/hyperactivity disorder transition into adolescence and adulthood in the united kingdom. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 879–888. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S. Social relationships and health. Am. Psychol. 2004, 59, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Singh, I. Boys will be boys: Fathers’ perspectives on ADHD symptoms, diagnosis, and drug treatment. Harv. Rev. Psychiatry 2003, 11, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Hampton, K.N.; Goulet, L.S.; Rainie, L.; Purcell, K. Social Networking Sites and Our Lives; Pew Research Center’s Internet & American Life Project: Washington, DC, USA, 2011. [Google Scholar]
- Hampton, K.N.; Sessions, L.F.; Her, E.J.; Rainie, L. Social Isolation and New Technology; Pew Internet & American Life Project: Washington, DC, USA, 2009. [Google Scholar]
- Ellison, N.B.; Steinfield, C.; Lampe, C. The benefits of facebook “friends:” Social capital and college students’ use of online social network sites. J. Comput. Mediat. Commun. 2007, 12, 1143–1168. [Google Scholar] [CrossRef]
- Valkenburg, P.M.; Peter, J.; Schouten, A.P. Friend networking sites and their relationship to adolescents’ well-being and social self-esteem. Cyberpsychol. Behav. 2006, 9, 584–590. [Google Scholar] [CrossRef] [PubMed]
- Valkenburg, P.M.; Peter, J. Internet communication and its relation to well-being: Identifying some underlying mechanisms. Media Psychol. 2007, 9, 43–58. [Google Scholar] [CrossRef]
- Valkenburg, P.M.; Peter, J. Social consequences of the internet for adolescents: A decade of research. Curr. Dir. Psychol. Sci. 2009, 18, 1–5. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bussing, R.; Meyer, J.; Zima, B.T.; Mason, D.M.; Gary, F.A.; Garvan, C.W. Childhood ADHD Symptoms: Association with Parental Social Networks and Mental Health Service Use during Adolescence. Int. J. Environ. Res. Public Health 2015, 12, 11893-11909. https://doi.org/10.3390/ijerph120911893
Bussing R, Meyer J, Zima BT, Mason DM, Gary FA, Garvan CW. Childhood ADHD Symptoms: Association with Parental Social Networks and Mental Health Service Use during Adolescence. International Journal of Environmental Research and Public Health. 2015; 12(9):11893-11909. https://doi.org/10.3390/ijerph120911893
Chicago/Turabian StyleBussing, Regina, Johanna Meyer, Bonnie T. Zima, Dana M. Mason, Faye A. Gary, and Cynthia Wilson Garvan. 2015. "Childhood ADHD Symptoms: Association with Parental Social Networks and Mental Health Service Use during Adolescence" International Journal of Environmental Research and Public Health 12, no. 9: 11893-11909. https://doi.org/10.3390/ijerph120911893
APA StyleBussing, R., Meyer, J., Zima, B. T., Mason, D. M., Gary, F. A., & Garvan, C. W. (2015). Childhood ADHD Symptoms: Association with Parental Social Networks and Mental Health Service Use during Adolescence. International Journal of Environmental Research and Public Health, 12(9), 11893-11909. https://doi.org/10.3390/ijerph120911893